
COVID-19 is much less deadly in the non-elderly population than previously thought, a major new study of antibody prevalence surveys has concluded.
The study was led by Dr. John Ioannidis, Professor of Medicine and Epidemiology at Stanford University, who famously sounded an early warning on March 17th 2020 with a widely-read article in Stat News, presciently arguing that “we are making decisions without reliable data” and “with lockdowns of months, if not years, life largely stops, short-term and long-term consequences are entirely unknown, and billions, not just millions, of lives may be eventually at stake”.
In the new study, which is currently undergoing peer-review, Prof. Ioannidis and colleagues found that across 31 national seroprevalence studies in the pre-vaccination era, the average (median) infection fatality rate of COVID-19 was estimated to be just 0.035% for people aged 0-59 years and 0.095% for those aged 0-69 years. A further breakdown by age group found that the average IFR was 0.0003% at 0-19 years, 0.003% at 20-29 years, 0.011% at 30-39 years, 0.035% at 40-49 years, 0.129% at 50-59 years, and 0.501% at 60-69 years.
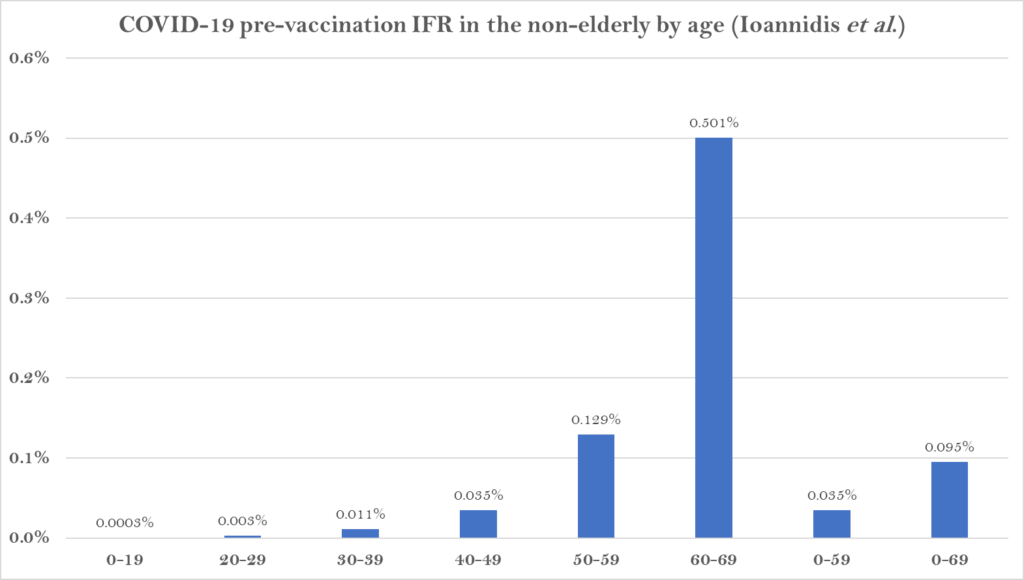
The study states that it shows a “much lower pre-vaccination IFR in non-elderly populations than previously suggested”.
A breakdown by country reveals the wide range of IFR values across different populations.
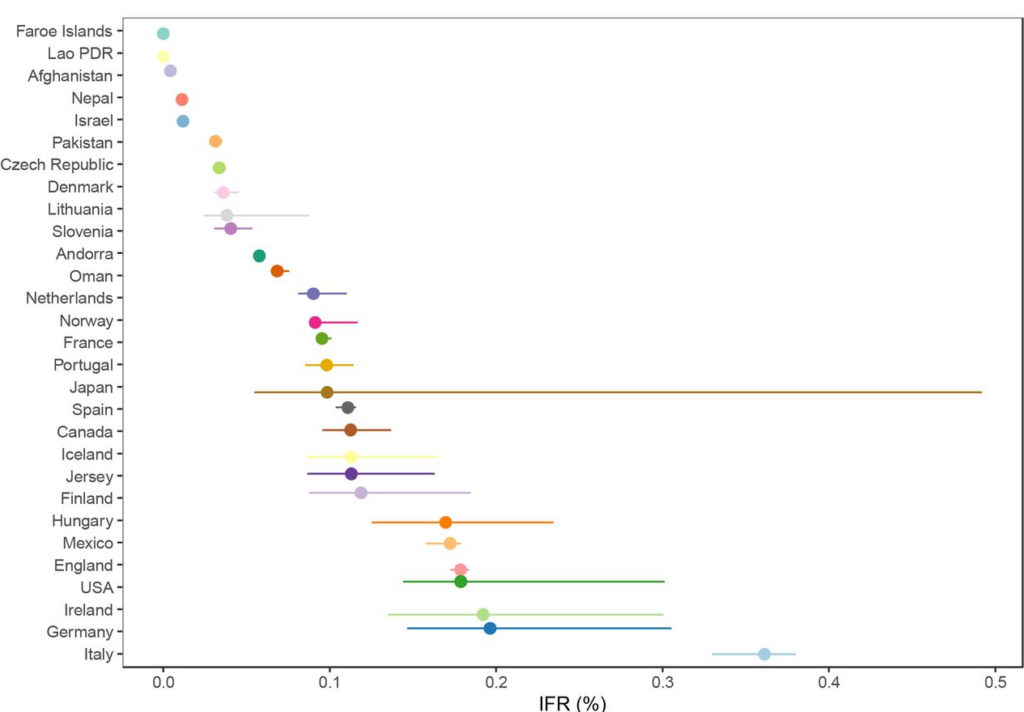
The significantly higher values for the top seven suggest some of the difference may be an artefact of, for example, the way Covid deaths are counted, particularly where excess death levels are similar. Note also that the antibody studies date from various points during the first year of the pandemic, most of them prior to the large winter wave of 2020-21, when levels of spread and numbers of deaths were more varied than later in the pandemic as subsequent waves caused countries to converge.
The reason some countries had much lower values and some much higher is not completely clear. The authors suggest that “much of the diversity in IFR across countries is explained by differences in age structure”, as per the plot below.
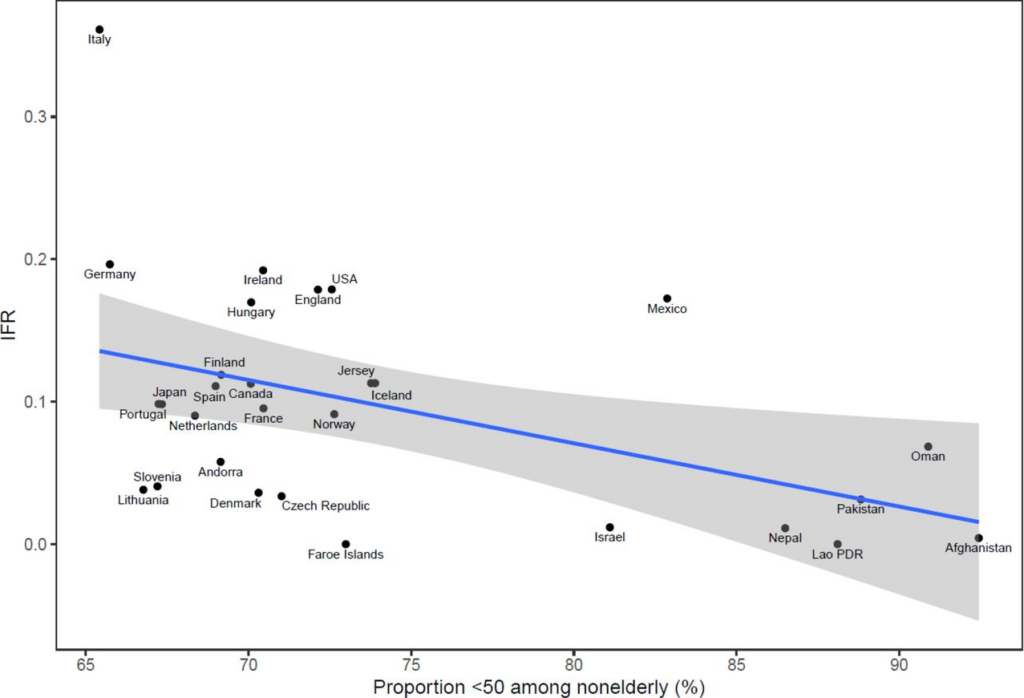
However, the age breakdown by country suggests that the IFR differed for each age group in each country, casting doubt on that suggestion. (In the chart below, note the logarithmic scale, and ignore the zig-zag lines, which are due to small countries having low numbers of deaths.)

Why are countries seeing differing IFRs even for the same age groups? The authors suggest a number of explanations, including data artefacts (e.g. if the number of deaths or seroprevalence are not accurately measured), presence and severity of comorbidities (for example, obesity affects 42% of the U.S. population, but the proportion of obese adults is only 2% in Vietnam, 4% in India and under 10% in most African countries, though it affects almost 40% of South African women), the presence of frail individuals in nursing homes and differences in management, healthcare, overall societal support and levels of drug problems.
Prof. Ioannidis has previously published a number of papers estimating COVID-19’s IFR using seroprevalence surveys. He and his team conclude that their new estimates provide a baseline from which to assess further IFR declines following the widespread use of vaccination, prior infections and evolution of new variants such as Omicron.












To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
“COVID-19 Much Less Deadly Than Previously Thought, Major Study Finds”
I would suggest a better headline would be “COVID-19 Much Less Deadly Than We Were Told/Lied To About, As Predicted/Pointed Out By Nutjob Conspiracy Theorists in March 2020, Major Study Finds”
Absolutely. All that was needed was to extrapolate the results from the Diamond Princess and then to monitor closely to ensure it wasn’t anomalous. Job done bar shielding the vulnerable.
We’re shaping up for another autumn panic again and with Mr “CCP did it best” in a major post it doesn’t look good for those of us who hoped for a restriction free life.
See my posts elsewhere on this thread. The fatalities (one) on the USS Roosevelt (4,850 crew members) show that Covid is/was not lethal to anyone under the age of 44.
Extrapolate and monitor? Wouldn’t that have been much less profitable for the government’s valued funders though?
“ He and his team conclude that their new estimates provide a baseline from which to assess further IFR declines following the widespread use of vaccination…”
*Sigh*
I think you will find the IFR goes up following the jabs.
“COVID-19 Much Less Deadly Than Previously Thought, Major Study Finds.”
I thought the C1984 was only really deadly to those already seriously ill and knocking on Heaven’s door. Or so I have been led to believe by those mad conspiracy theorists.
Can I suggest a lower IFR in some African countries might be the result of prior widespread use of Ivermectin to treat other illnesses?
…or the fact that they don’t have much of an elderly population or care homes?
And they don’t tend to be massively overweight.
Aren’t, according to the article: obesity US 42% most African countries 10%.
“Can I suggest a …”
Yes.
Ivermectin for river blindness and HCQ for malaria, both cheap and out of patent so of no interest to Dr Fauxi apart from working out how to ban them to keep the money rolling in.
BINGO
Yup – dr, fauci got his way. Bought up all the available stocks of ivermectin and got it removed from the WHO essential medicine list.
See Senator RF Kennedy book ‘The real dr, fauci’, The lower case letters are inentional as I totally despise this murderer and apology of a human being
Much less deadly than previously thought by whom? Certainly not anyone who read the report on the Diamond Princess cruise ship, or looked around and noticed the absence of corpses, or read about survival rates and that the true high risk was in those over 80 with comorbidity.
Absolutely. Back in 2020, the ONS used to publish data of C19 death numbers by local geography at quite a fine level, similar to local authority wards. That was quite revealing, when one knows the location of care home etc.
A few months on, they stopped doing that, and I queried to the ONS about why it did not continue, and I did get a reply from someone in the ONS which more or less said that the outbreak was almost over, so not required. That was in late summer (I don’t know if he’s still got a job there!).
The experts should have known one month into the official pandemic that almost all of the deaths were among people 80 or older with multiple co-morbidities. They should have also known the mortality risk for healthy young people was zero. Still, they cancelled sports in many leagues, states and countries.
Wait this is EXACTLY WHAT WE HAVE BEEN SAYING SINCE, OOO, I DON’T KNOW, FEBRUARY 2020!
But no, ignore us, we’re all just conspiracy theorists, granny-killers, right-wing fascist Trump and Putin lovers.
My blood boiled dry in the first six months of this scam/panic/fraud and I have been running on caffeine and alcohol ever since.
One of the best sources to calculate IFR or CFR would be an analysis of crew members serving on the USS Roosevelt aircraft carrier, which suffered a major Covid outbreak in March-April 2020. The CDC and Navy later did an antibody study of the approximately 4,850 crew members to see what percentage of this crew had antibody evidence of prior infection. The study found that approximately 60 percent of crew members did test positive for Covid antibodies in late April 2020. (For some unexplained reason, the CDC only tested 385 of the 4,850 crew members for antibodies).
Still, from this study we can extrapolate that approximately 2,910 crew members had been infected between late January 2020 and late April. Of this number, only one crew member died from Covid … and this crew member was much older (44) than most of the young Navy crew.
So the IFR/CFR on the Roosevelt was approximately 1-in-2900 (which is 0.0343 percent). The IFR for crew members under the age of 44 would have been 0.00000 percent.
A Navy ship where everyone is living in tight quarters for weeks on end would have to be the worse-possible environment for virus spread … and still nobody under the age of 40 died from this “deadly” virus.
FWIW, I personally think the novel coronavirus came on board that ship … when it left port from San Diego on January 17, 2020 – three days before the first “confirmed” case in America. Data included in the CDC/Navy antibody study actually supports this hypothesis. For example, two crew members self-reported (in a questionnaire) experiencing symptoms 98 and 99 days before they got their blood tested for this antibody study around April 20, 2020. This would mean these two crew members could have been symptomatic from Covid on or around January 17, 2020. Ten other crew members tested positive for antibodies and self-reported experiencing symptoms around or before the time the ship made its first port-of-call (in Vietnam) around mid-March. I also think there would have been much more “early spread” evidence if the CDC had actually tested the entire crew for antibodies (instead of about 8 percent of the crew).
I also find it interesting/revealing that the Navy never interviewed these 12 possible/likely “early spread” sailors.
I’m going to write a story on this hypothesis – outline the reasons why I think I could be right – in the near future at my Substack. I think every reporter in the world who read this study missed a possible blockbuster story. They didn’t “bury the lede,” they didn’t even mention it.
To further explain why I think my story (“finding”) is significant … I think it could prove two things:
1) That there was even more (possible ) evidence of “early spread” in America … from this antibody study performed by the CDC and U.S. Navy.
2) I would say this also provides evidence officials might have concealed this evidence from the public. Or, if nothing else, it provides more evidence these officials didn’t follow-up with potentially important evidence. For example, they didn’t question these 12 sailors about the symptoms they self-reported on the questionnaires they filled out.
However, I can’t say the CDC/Navy covered up this evidence as they actually presented it in this study. Text in the study (and indeed one graph) tells readers how many sailors had antibody evidence that could pre-date the ship’s first port-of-call (evidence that would suggest the virus that ultimately spread through most of the crew actually came on board the ship).
All I can think in way of possible explanation is that the Navy had already said they were going to do an antibody study of crew members (which is a common-sense thing to do). So they probably felt like they had to follow-up and do such a study. It is interesting that the larger study they had previously said they were going to do was down-sized significantly. I mean, why test only 385 sailors for antibodies? Why not test them all, or at least half of crew members?
Furthermore, I suspect they must have been confident that even if they did publish the results I’ve highlighted, officials were probably supremely confident that no mainstream media journalist would make a big deal out of the details I’ve made a big deal out of. (“Hey, doesn’t this mean this virus was spreading on this ship probably in late January?!”). No member of the mainstream press ever mentioned this detail/possibility.
Two weeks ago I even wrote a Substack piece where I listed future taboo Covid articles I’m going to write. No. 1 on that list is my story on the Roosevelt antibody study. I put it on this list to prove that nobody in the mainstream press is going to “scoop” me on this story. I know these “journalists” aren’t going to investigate this possibility. This, in fact, is the more sinister part of a larger story. All of the potentially narrative-changing Covid stories are off limits to serious mainstream inquiry.
I’m going to try to “prove” this as well.
For those who might be interested in researching this hypothesis, I’ve included link to a PDF version of the “Roosevelt Antibody Study.”
Please note Figure 3 and Page 720 in particular.
I’d welcome any thoughts and feedback on my hypothesis. Namely, I wonder if there are other people who reach the same conclusion from this data/information that I have?
https://www.cdc.gov/mmwr/volumes/69/wr/pdfs/mm6923e4-H.pdf
FIGURE 3. Days from symptom onset* to specimen collection (A) among a convenience sample of participants who had positive real-time
My comment: Note: 98 to 99 days from April 20 to April 24 (date blood was drawn for antibody tests) = “onset of symptoms” on or around January 17 – the date ship left San Diego.
Among 12 participants with positive ELISA.results >40 days after symptom onset, eight maintained positive microneutralization test results, including two participants who were tested >3 months after symptom onset.
Nearly two thirds of persons in this sample had positive
ELISA test results, which indicate previous exposure to
SARS-CoV-2
I also note that this study says that a positive ELISA antibody result is considered a “confirmed” Covid case for purposes of this CDC study (as well as a positive PCR test).
If the same standard was applied to two people in Washington State (identified by The Seattle Times) who were sick in December 2019 and later received a positive ELISA antibody result, they should also now be considered “confirmed” Covid cases. But despite this, the first “official” or confirmed case in America is still listed as January 20, 2020 – a man who returned to Washington State from Wuhan. Tim and Brandie McCain of Alabama, also sick in December, also later got positive ELISA antibody results.
Anyway, the official timeline of the origins of Covid spread is clearly wrong even to this day.
How a “case” is “confirmed” or not confirmed by the CDC is very interesting and important in my view.
Anyone with thoughts on the possible significance of the Roosevelt study (or early spread info) can contact me at my Substack.
https://billricejr.substack.com/p/covid-was-spreading-across-us-in
As the so-called Swiss doctor has repeatedly written: COVID is a very strange disease because its mortality profile is almost exactly identical to a natural mortality profile, or, in other words, people dying from COVID are people who’d have died soon, anyway, just because of another superficial cause. This makes it absolutely no different from comparable diseases which also thin out the rows of those who are already pretty weak so that an in itself very small additional shove will cause them to die. This may sound brutal, but that’s life: Very sick and/or very old people eventually die.
I think this story also could be used in my efforts to answer the other trillion-dollar question: Why didn’t more people die before March 15th, 2020 if “early spread” was, in fact, occurring?
The bulk of my answer will be that the vast majority of later “Covid deaths” were actually caused by iatrogenic faulty medical protocols (like vents, etc). Also, it’s pretty clear that the “Covid deaths” numbers were widely inflated. But another part of my effort to answer this question will be that Covid is really not lethal to the vast majority of people who contract the virus. This is what Ioannadis has been saying all along. This is what the results of the U.S.S. Roosevelt antibody study tell us as well (see post below).
This is actually a shocking finding/area of inquiry as it prompts this question: If Covid wasn’t and isn’t killing most of these official Covid fatalities, what was/is?
Hmm … climate change? Or whitness perhaps? Or maybe Prince Harry’s conversion from a dunderhead flying in helicopter gunships over Afghanistan who boasted the he was always good at shoot ’em up video games to an entirely charmless Prince Social Justice?
Sometimes (most of the times, actually) the best answer to a question whose answer we don’t know is We don’t know this.
That’s pretty much what I’ve said regarding the “where are all the early deaths” question – or “why didn’t we see a lot more deaths a lot earlier?” I don’t know. I have a strong hunch why they weren’t showing up earlier, but I probably can’t say definitively. That’s why better minds than my own need to be asking and thinking about this question. The answer(s) must be there … but first smart people at least need to ask the right question and go looking for the answer.
They weren’t showing up earlier because – COVID being pandemic, and very truly a pandemic of that, of extraordinary headlines about ordinary events – nothing out of the ordinary was happening, neither before nor after a pandemic was declared. I remember when the first panicky headlines about events in Italy rolled in. The only story the absolute numbers ever told was Negligible number of people infected with something. Throughout all of this miserable time, a COVID catasrophe was always said to be about three weeks away unless we now do … It never really materialized. On each and every occasion after measures started to be lifted, a catastrophe supposed to happen within at most two or three weeks if this was allowed to continue … ! was predicted but it never happened. This went on until January 2022 when the WHO special envoy for COVID came to London to have a bunch of media interviews. In a last ditch effort to save the mask mandate, he made ominous noises about him and his colleagues being such expertly COVID experts – We’ve been studying Sars-CoV2 since 2020. What do these people [who dare to lift COVID restrictions] know about the virus me and my colleagues don’t? – this obviously being a How dare you?!? style rethorical question – and confidently predicted the UK and even the world at large would see some (very bad) something happen within at most two weeks.
If he had meant him finally falling silent on the topic, he had been right about that. But not about anything else.
As to the question why all these people reported as COVID dead died, we’ll never know that. Someone would have needed to do autopsies to determine this. But it’s too late for that now and speculating about what could have been the cause isn’t helpful.
Oops
Maybe 5G. Maybe it disrupts the immune system.
I’ll get me coat on that one, but who knows
Maybe stress generated by the MSM…
On a more serious note, do some research on the effects of stress on WHAT IS KNOWN about how immunity actually works.
They don’t sedate patients who are told they’re being sent to ICU’s for nothing….
Well some of the “official covid fatalities” were just people dying who happened to test positive. There was a spike in “excess” deaths in the UK around April 2020 that possibly represents something fairly unusual in historical terms, but all-cause mortality in 2020 was not unusual – it was at 2008 levels. Mortality fluctuates a fair bit over time, though the general trend is down I suppose because of better diet/healthcare (not sure how true this will remain, looks like it won’t) but of course if you cherry pick data you can show a trend u or down if it suits your purpose. I guess my point is that in most (all?) countries, all-cause mortality was not exceptionally higher than a long term average and that the degree of fluctuation would not have been a reason to turn the world upside down, before covid.
What about my hypothesis? That Covid does not, and never has, actually existed.
After you’ve got back off the floor from laughing just remember that I’ve worked as a Paramedic for 21 years.
I also believed it was a new virus in early 2020 but after not seeing a single unequivocal Covid case I started to suspect that what we were actually witnessing was a Mass Psychosis outbreak with the Doctors and scientists the worst affected.
I said early on that the doctors, in their madness, were ventilating people with panic attacks. That’s because I saw people on TV who were ‘suffering’ from Covid and being ventilated. Believe me, I’ve seen plenty of people with serious breathing difficulties and these did NOT have serious breathing difficulties. A good rule of thumb is that people with serious breathing difficulties cannot speak in full sentences and yet these people were apparently chattering away under their oxygen masks.
To back me up have a look at “Underlying Medical Conditions and Severe Illness Among 540,667 Adults Hospitalized With COVID-19, March 2020–March 2021″The number 2 risk factor (after obesity) with a whopping 28% increase in risk from dying from Covid was errr……… Anxiety!
Of course this uncomfortable finding was immediately airbrushed and ignored. Why would a mental illness cause people to die from a respiratory virus? The short answer is, it doesn’t but there is a rational explanation.
The justification for ventilation was that Covid causes ARDS (Acute Respiratory Distress Syndrome) and that was why these patients were ventilated. But anxious people, when told by doctors in respirators and aprons, that they have a deadly virus inside them can have panic attacks and the main symptom of a panic attack is hyperventilation.
It is this that was being misdiagnosed as ARDS by doctors who were convinced that what they were actually seeing was the result of Covid infection when, in fact, they were anxious people, almost certainly testing positive, and coming to the hospital having panic attacks and then being ventilated by doctors, themselves suffering from Mass Psychosis and confirmation bias.
I believe that not a single person on earth has died of Covid 19 and that all the deaths have a completely rational explanation and are the result of the medical profession going, temporarily, insane.
I said this all way back in 2020 and yet still am apparently the only person on planet earth who believes this explanation but if thought about in this way, all the paradoxes. contradictions and bizarre behaviour actually start to make sense.
“just remember that I’ve worked as a Paramedic for 21 years.”
We didn’t know that.
I see you still haven’t done your Agenda 2030 homework. Naughty, Naughty.
https://www.youtube.com/watch?v=ojPcF-oLABE&t=16s
You are no longer alone on planet earth to believe this.
Looks like Covid wasn’t more dangerous than influenza after all.
That was obvious a very long time ago …… round about the time the Diamond Princess was quarantined and out of 2,600 passengers (+ 1,100 crew), there were around 700 cases and only around 7 highly vulnerable people died.
You don’t say…..
Misclassification, pure and simple. ‘With Covid’ not ‘From Covid’.
What was the predicted IFR from the Diamond Princess data? Two distinct groups, the mostly elderly passengers and the working age crew. They cannot say they didn’t know right back then.
Prof. Ioannidis once again confirms with complex statistical science what we all saw plainly with our own eyes. I.e not many elderly people dying of covid (in my case none whatsoever) It was a triumph of marketing, make-belief, suggestion and propaganda to make people believe the threat was greater than that they could actually see. They stopped listening to their own senses in favour of a constructed reality. Hats off to the manipulators..
I didn’t personally know anyone who died from Covid until around December 2020, when three elderly people I knew died “from” Covid. One was 70, and two were 80 or 81. That’s still the only people I personally knew who died from Covid. So that’s three deaths in more than 31 months – all elderly. I still wonder if the rash/spike in deaths in the winter of 2020 might somehow be related to all these people also getting their flu vaccines just before this. But that’s just a nagging question/possible hypothesis that has stuck with me.
However, I also know two people who almost died from Covid-like symptoms in December 2019/January 2020 – before Covid was even supposed to be in America. One of these men later tested positive for antibodies. The other never got an antibody test, but he had all the symptoms, hasn’t tested positive since and tested negative for the flu multiple times while in the hospital and ICU for several weeks. Assuming some people who were in critical condition with possible Covid DID die, I think some real “Covid deaths” from before March 2020 have been missed. But this wouldn’t be a great number of deaths and most would have been among people 80 and older with multiple co-morbid conditions.
I had one relative who died from it: male, aged around 58, significantly overweight. He was self-employed and his 30-year business was being destroyed by the lockdowns, so he was very stressed.
I don’t know anyone else who died from it.
But I knew several people who died of strokes post jab; a couple who have so far survived but one more will kill them. And an acquaintance who had a massive heart attack 3 weeks after his 3rd booster (2 x AZ and then 1 Pfizer).
Data and stats will never cut this! The whole shebang was a ‘kind of magic’ in the words of the late F. Mercury.
We’ve been conditioned to accept almost anything that is thrown at us.
The pandemic and the energy ‘crisis’ are large scale stress tests. What level of excrement can be thrown at us! This is all about calibration & fine tuning for Level 2.
We’ve been taking the conditioner into the shower with us for a long time now. How many sentient beings believed that the fragile wings of a jet plane could cut through steel like a knife through butter – and simply disappear? A lot. The work is done.
Dr Moreau is ready to leave the island for good.
How many people had really contracted this virus prior to March 15, 2020? It’s probably impossible to get a good estimate/answer at this point – as too many months have passed and too many variants and too many vaccines/boosters.
However, a great study would be to study the people who think they did have Covid before this virus was supposed to be spreading. Many of these people actually went to the doctor and at least got a flu test. I’d be interested in learning how many people in this study cohort – those who tested NEGATIVE for the flu (thus ruling the flu out as a reason for their illness) – later tested positive for Covid via a PCR test. Or at least got a positive PCR test result sometime in 2020 before the variants started to emerge. My hypothesis would be that members of my study group would have tested positive for Covid at a much lower percentage than the rest of the population (those who had not been sick in November 2019 through early March 2020). My hypothesis assumes the explanation for this possible finding would be that the people in my study group had already acquired natural immunity.
This would probably consitute evidence these people very well did have COVID much earlier than it’s thought the virus was spreading.
I’m pretty sure no such study will ever be performed because I think some officials KNOW this virus was already spreading before they said this was possible. My second hypothesis is that some officials want to conceal evidence of early spread. My main thought is this: Officials do not investigate that which they would prefer not to “confirm.” This also means they won’t do studies they could do.