
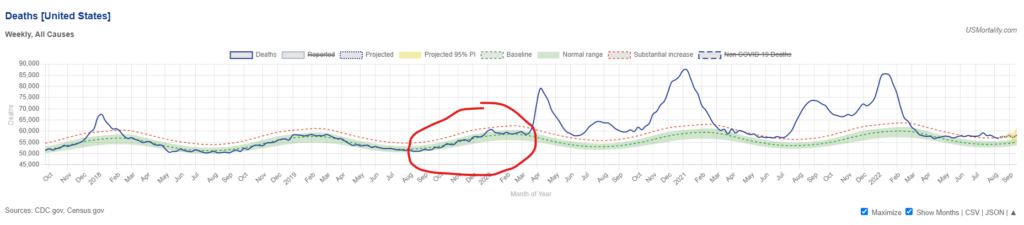
There is now no shortage of evidence that the coronavirus had begun spreading undetected all over the world by autumn 2019 at the latest. However, the 2019-20 flu season was mild in most places. For instance, here is U.S. mortality, with the 2019-20 flu season circled.
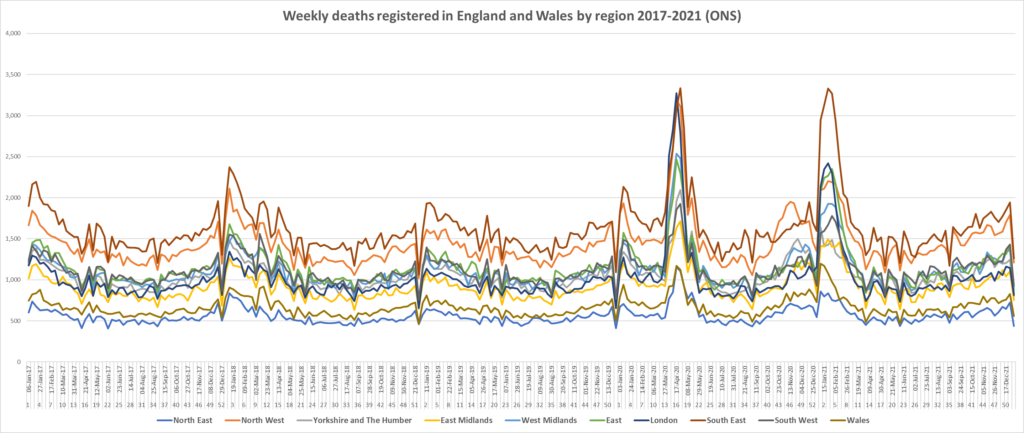
And here is England and Wales, with the unremarkable end of winter 2019-20 on the left hand side (before week 10). The contrast with the spring surge (and subsequent waves) is obvious.
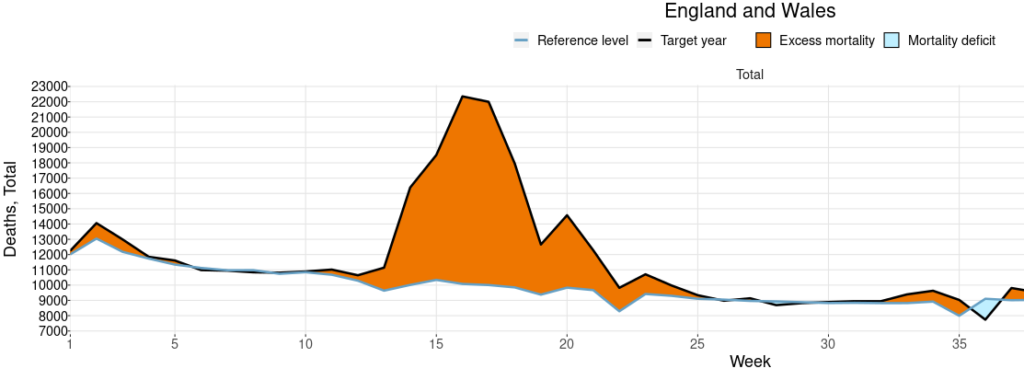
This leads to a mystery: why did COVID-19 only start killing lots of people come spring 2020 if it had been hanging around quietly all winter?
Some sceptics argue that it’s because Covid isn’t really a more severe virus than flu, but the excess deaths were all caused by how we started responding to it in February and March 2020. For example, the overuse of ventilators particularly in New York City and the surrounding states in the first wave has been suggested by some to account for tens of thousands of additional deaths. However, while a ventilator panic in and around NYC will explain some of the additional deaths that spring, it wouldn’t explain the deadly outbreaks elsewhere, or the deadly outbreaks that kept coming in subsequent waves even as the use of ventilators was scaled back.
The fact that deadly Covid outbreaks kept coming over the ensuing months and years (see the U.S. chart above) is a powerful objection to the idea that what was causing most of the deaths was anything peculiar about the treatments used in, say, New York in March 2020. After all, many states including Florida had deadly waves during summer 2021 as the Delta variant surged. But Florida had not had a large wave the previous winter (despite famously ending its statewide restrictions in autumn 2020). It’s clearly not the case that medics in Florida started going big on the ventilators again just as Delta appeared, and then stopped using them again afterwards. This is not an adequate explanation for the patterns of deaths we see. Early on there was a high level of variation in how many deaths occurred in different U.S. states, just as there was in different countries, for example, between Eastern and Western Europe. However, over time the number of excess deaths tended to converge, putting a limit on how much of the variation can be pinned on things specific to localities or time periods, such as poor treatment protocols early on in the north-eastern United States.
Below is the picture in the U.S. at the end of May 2020 – a real patchwork, though with clear concentrations of excess deaths around New York and around Michigan, Illinois and Indiana, plus Louisiana and one or two other states.
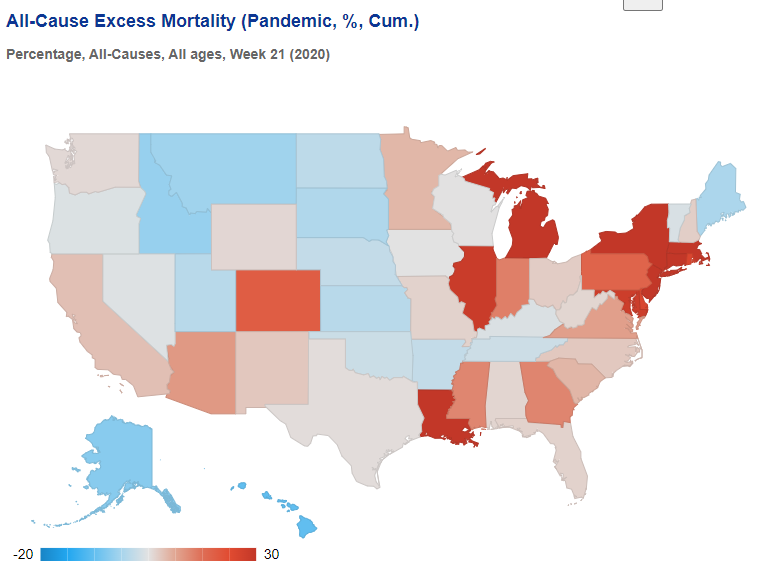
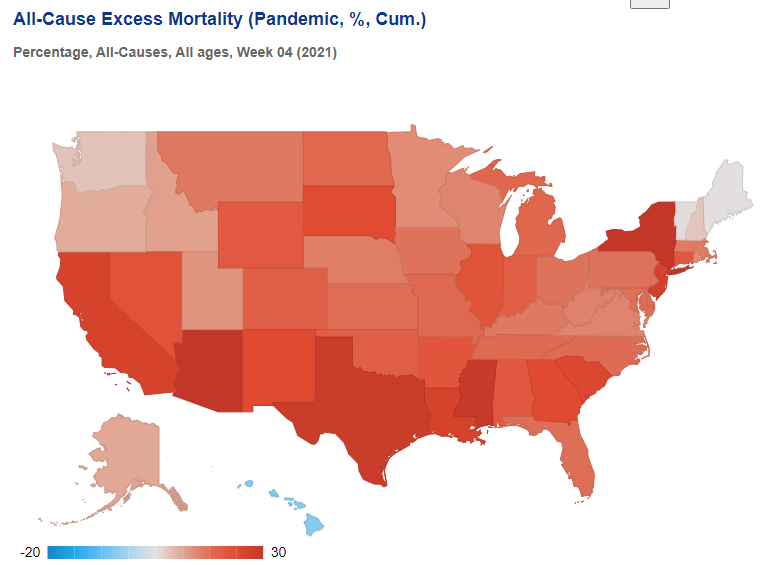
By the following winter, however, excess deaths were high almost everywhere, meaning specific local treatment protocols or policies cannot be blamed for bringing the deaths.
One suggestion is that the simultaneous surge of deaths across the regions of England in March 2020 is indicative of a cause other than an infectious virus. However, data from the ONS, displayed below, suggest that flu deaths typically surge across the country simultaneously, so this is not unusual or unexpected. While the data below are by registration date, which creates artificial synchronicity (e.g. from bank holidays – the sharp dips), nonetheless the regional patterns are so tight they leave no room to think the picture by date of occurrence would be vastly different.
In other words, the main driver of Covid deaths appears, in fact, to be COVID-19, a disease caused by a virus which Dr. John Ioannidis has estimated from antibody surveys to have an infection fatality rate (IFR) of around 0.3-0.4% in Europe and the Americas. This rate, he says, varies between and within countries and over time, and some of that variation will be due to poor treatment protocols. However, the consistency of the values across different contexts suggests this is the right ballpark, at least for those with no specific immunity to the virus and pre-Omicron. Dr. Ioannidis writes:
Even correcting inappropriate exclusions/inclusion of studies, errors and seroreversion, IFR still varies substantially across continents and countries. Overall average IFR may be ~0.3%- 0.4% in Europe and the Americas (~0.2% among community-dwelling non-institutionalised people) and ~0.05% in Africa and Asia (excluding Wuhan). Within Europe, IFR estimates were probably substantially higher in the first wave in countries like Spain, U.K. and Belgium and lower in countries such as Cyprus or Faroe Islands (~0.15%, even case fatality rate is very low), Finland (~0.15%) and Iceland (~0.3%)… Differences exist also within a country; for example within the USA, IFR differs markedly in disadvantaged New Orleans districts versus affluent Silicon Valley areas. Differences are driven by population age structure, nursing home populations, effective sheltering of vulnerable people, medical care, use of effective… treatments, host genetics, viral genetics and other factors.
But if a virus with an overall IFR of around 0.3% was spreading throughout the winter, why were deaths so low until March and April?
I had thought this may be due to a more deadly variant emerging in, say, Lombardy and spreading to New York and elsewhere. However, it is now clear to me that the main reason for the lack of deaths was the lack of spread, particularly in care homes. Yes, the virus had spread around the world, but it had not displaced flu and the other viruses, and did not have any explosive outbreaks. It just moved around at a low level alongside other viruses, infecting some people but not in huge numbers. This may seem strange given what has happened since spring 2020 and the series of large waves with explosive surges and no flu anywhere to be seen. But the evidence on this is completely clear, as summarised below. Winter 2019-20 was an ordinary winter, despite SARS-CoV-2 lurking and circulating incognito.
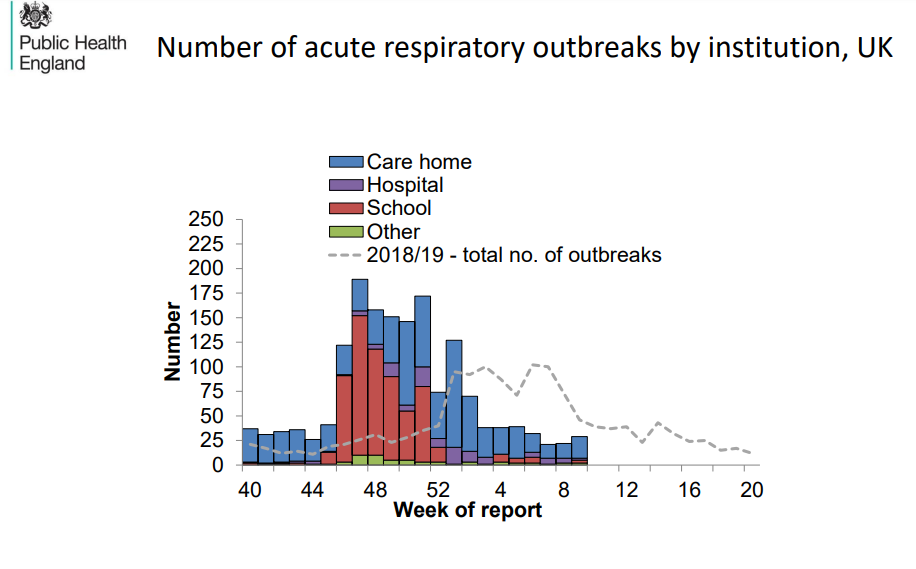
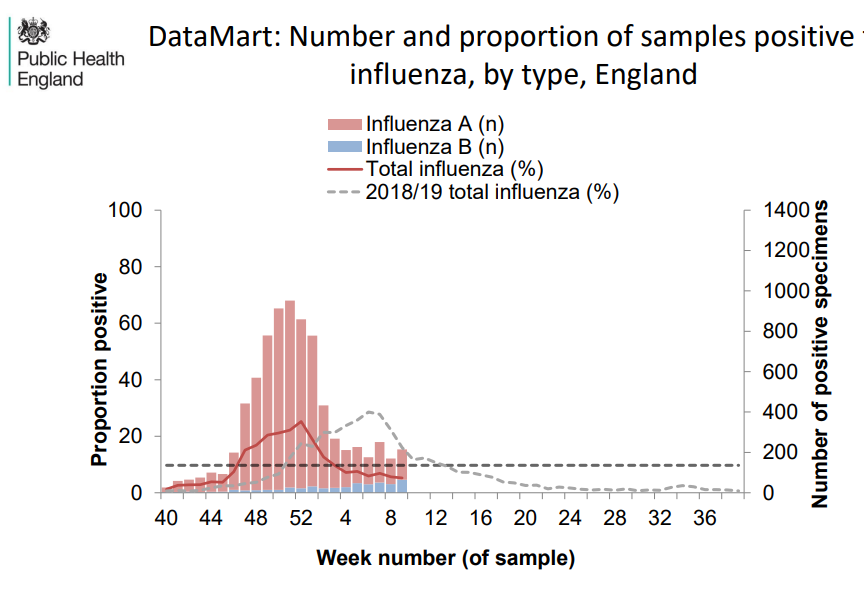
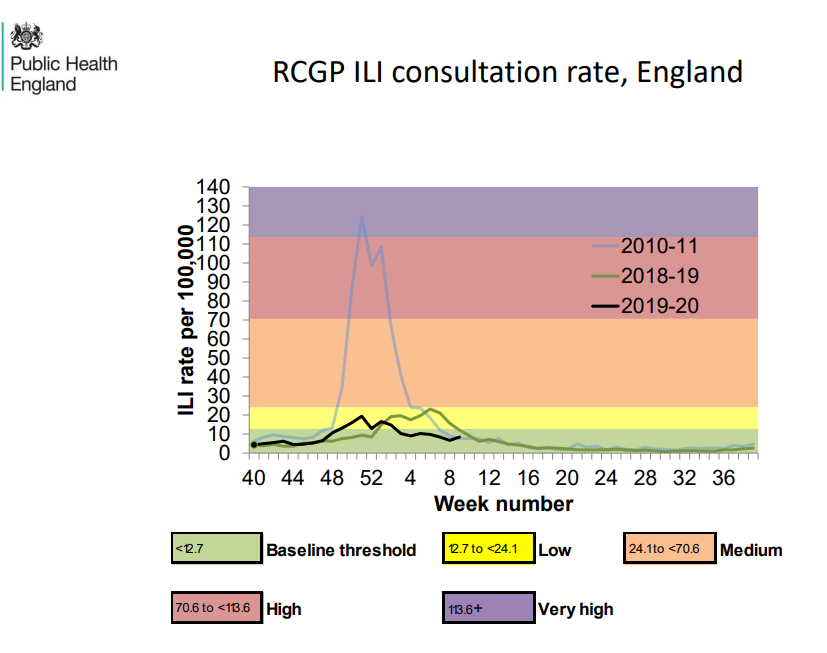
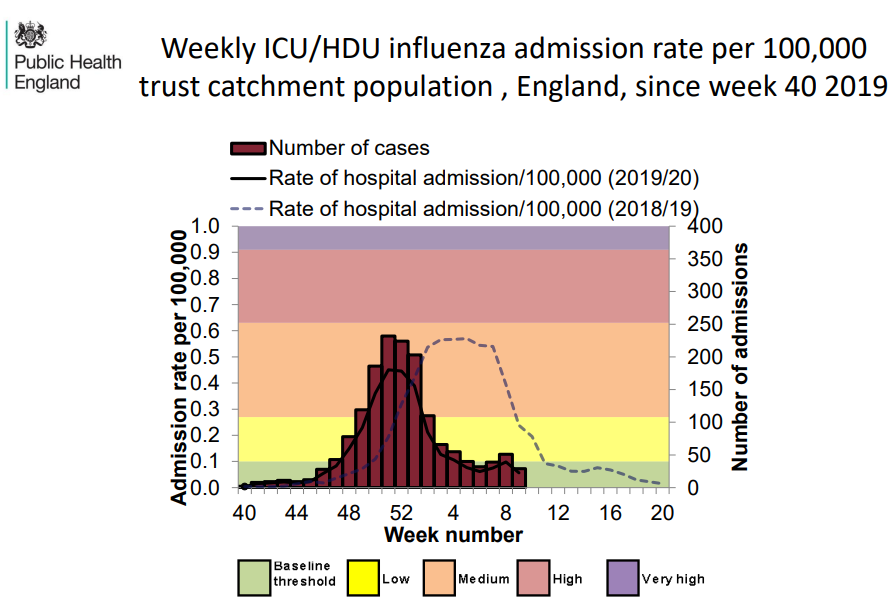
Take a look at these charts from the U.K. flu surveillance report in early March 2020. The flu season arrived early but it was not particularly severe.
The proportion of influenza-like illness testing positive for flu was normal, if early.
GP consultations for influenza-like illness were normal.
ICU admission rate for confirmed flu was also normal.
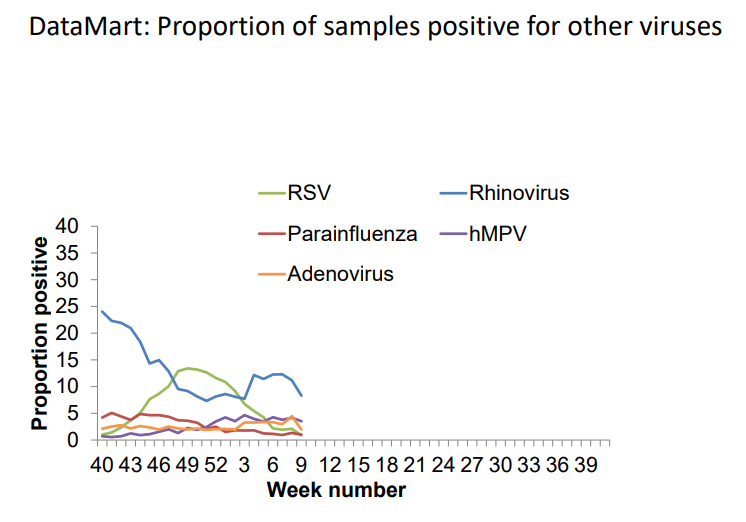
Other known causes of influenza-like illness were also at normal levels.
While many hospital tests for the cause of influenza-like illness came back, as usual, for an unknown pathogen – one of which would have been SARS-CoV-2, of course – the proportion for SARS-CoV-2 couldn’t have been that high as overall deaths were not, as we have seen, elevated as they would have been if SARS-CoV-2, which has a higher IFR than flu (~0.3% vs ~0.1%), was rife.
This limited spread of SARS-CoV-2 that winter is also confirmed by early antibody testing. Dr. Jay Bhattacharya’s antibody survey of Santa Clara County in California on April 4th-6th 2020 found 2.8% of the population with antibodies. This puts an upper limit on how many of the general U.S. population can have been infected during that winter.
Antibody evidence from England also shows a low level of spread throughout the winter before an explosive outbreak at the end of February. The following chart was created by researchers who asked those who tested positive for COVID-19 antibodies when their symptoms began (these were antibody tests, no PCR tests or LFTs were involved). The pattern of infections it gives is striking – and supports the picture above of a virus circulating at low level over the winter before suddenly going big.
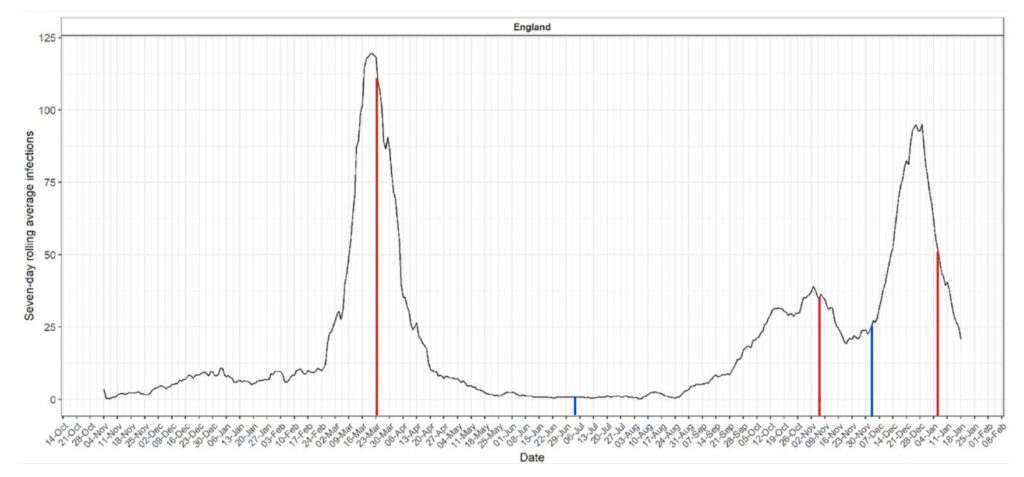
So the evidence all points to a picture of SARS-CoV-2 being widespread in the winter of 2019-20 but not being the dominant virus, circulating at a low level, before exploding into a large outbreak – and getting into the care homes – in the spring. It was thus this explosion in spread that primarily caused the explosion in deaths (though some were caused by poor treatment protocols of course, and a sizeable number of care home deaths were due to mistreatment of residents). The deadliness of the virus didn’t change a great deal; the IFR didn’t suddenly leap up; it’s just that suddenly many more people were catching it and spreading it, and it was getting into many more care homes. (Discharging hundreds of infectious hospital patients into care homes to free up beds won’t have helped with this of course.)
So why did the virus suddenly become much more infectious in February 2020; why did it go from circulating at a low level alongside flu and other viruses to displacing them and infecting a relatively large proportion of the population in a space of weeks? What’s more, it has stayed in this infectious mode, with successive variants driving new surges and waves. Though not everywhere, notably. In some countries, such as Japan, South Korea and other East Asian countries, it remained in its low-spread pre-2020 mode until Omicron came along (which has so many mutations it is a substantially different virus).
So why? This, I think, is one of the big outstanding mysteries of the virus. Why is its behaviour at different times and places so variable, so hard to predict? My feeling is still that this has a lot to do with the genetics of the virus and how it interacts with the genetics and other features of the populations it infects. Variants, in other words. Not more deadly variants necessarily (though Omicron is significantly less deadly than earlier variants). But variants that are more transmissible among certain populations, or certain sections of the population. After all, new waves are often caused by new variants, which seem to be able to infect (or re-infect) a different group of people to the previous ones. So why couldn’t the first big waves also be explained by a similar shift in variants?
Thus what may have happened in February 2020 is a new more transmissible variant emerged (or at least more transmissible among certain subgroups of people) which was then able to spread much more readily. But for some reason it wasn’t able to become dominant everywhere at once, or get into care homes everywhere, thus the early patchwork of deaths, the staggered start, and also the gradual convergence. Possible evidence in support of this is that one of the only interventions that some studies found to reduce deaths in the first wave was early border closures, which may be because it kept the new more transmissible variants out for longer.
Well, that’s my current best guess. You might have a better one (though please don’t try to pin it all on the treatment protocols in New York or wherever, that really doesn’t explain what we see). But whether my guess is right or wrong, the question of why a virus circulating over the winter at a low level suddenly started spreading fast and wide and causing successive waves of deaths is not yet resolved. The virus still keeps its secrets.











To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
Midazolam – look at the amount prescribed to the elderly who were barricaded in care homes and denied access to medical care during that same window of time.
^ This 100%
I’ve seen a covid treatment protocol document from the NHS dated early March 2020 for patients suffering respiratory distress. It comprises of two drugs: midazolam & morphine. The dosage is TWICE the usual dose. If you check side effects of those drugs, particularly in the elderly (which in pharmacy speak means anyone over the age of 55 years) suppression of respiratory function is a common side effect.
The question is, why further suppress the respiratory function of an individual with respiratory distress? This is the ‘just following orders’ part to push the blame downwards onto the medics & nurses (who should have known better) from the ones who made the decision that this was the correct protocol for treatment.
The other thing to remember is that once a patient arrived in hospital, NO CPR was to be carried out.
An acquaintance has these documents. NHS documents. Instructions passed down from the DoH & we know who was in charge then. GPs also prescribed the midazolam/morphine protocol to Nursing Home inmates without sight of the patients. I know of a few NH managers & staff who resigned in protest as they knew what that combination of drugs would do to a frail, elderly person.
The instruction to bypass GPs, call 111, take paracetamol & only go to hospital when you can’t breathe was the means of ramping up the numbers who would die.
The above actions contributed to the very real distress of NHS staff dealing with lots of deaths & terrifying them into becoming part of the baying mob calling for harder, faster restrictions & ‘vaccine’ pushers. They really were brainwashed into the covid cult.
Very effective psychops.
Or manslaughter, depending on your point of view?
The protocols were designed with murderous intent & only very few medics/nurses were able to perceive the danger of the protocols. Fear & heightened stress helped to ensure that the vast majority wouldn’t be able to engage the cortex in critical thinking but use the primal brain response via the amygdala which has no connection to the cortex.
Fear does dreadful things to the ability to think critically. This doesn’t absolve the actions of those medics & nurses but points to the true perpetrators of this crime, those in power.
They took the oath and they knew they needed to give informed consent. With every person they injected, they knew they could not possibly give informed consent.
The charge is surely greater than manslaughter.
Yep, they were all condemned to a deliberately cruel slow suffocating death.
Evil.
You know that nagging feeling you get when the answer is there for everyone to see, but instead, they choose to write a huge article with graphs and stats to argue about the renamed flu/common cold?
This video of Hancock’s boastful admission of guilt has been freely available long enough for Daily Sceptics to pick it up. There are plenty stats and graphs for the purchase and administration of Midazolam out there too.
Reading the latest of eugyppius’ analyses, I think that anything that the virus does, it has been planned that way by its creators…
Not quite.
The planning has gone in to the injections.
The injections have been brewed to a recipe. We are yet to see its full impact.
Will has highlighted an important and, to date, little-considered riddle: If this virus was spreading widely around the world beginning in the autumn of 2019, where were all the “Covid”deaths one might expect to see during those months?
There’s two reasons I believe “early spread” was also “wide” spread:
2) The vast number of at least Americans who were “sick” with something in the months before “official” Covid. Will presents data that suggests there was no wide-spread outbreak of flu in many places in the world. However, I’ve saved scores of files from December 2019-March 2020 from state health departments that report that ILI was “widespread” and “severe” in most states in America in the flu season of 2019-2020. (It should be noted that the CDC later down-graded (significantly) its “estimates” of ILI in this flu season. Still, all those contemporaneous ILI surveillance reports still exist; I saved many of them).
Here’s a Time magazine story from December 9, 2019 that states in the headline: Flu Season Is Off to an Earlier-than-Normal Start, Raising Fears of a Severe Year”
“Influenza activity has been higher than normal for four weeks in a row, which many experts consider the official mark of flu season. As of the week ending Nov. 30, 3.5% of visits to health care providers nationwide were related to influenza-like illness, according to the U.S. Centers for Disease Control and Prevention (CDC). Already, the country has seen about 1.7 million cases of the flu, 16,000 flu-related hospitalizations and 910 flu-related deaths, the CDC says. Six children have died so far.
… The last time the flu arrived this early was the 2003-2004 season, which turned into a fairly severe one; at its peak, 10% of U.S. deaths were flu-related.”
Here’s a randomly-selected excerpt from Ohio’s Department of Health in Week 4 of that flu season (January 19th-25th, 2020):
“During week 4 (January 19th – January 25th, 2020), the majority of the U.S. reported High influenza activity. The proportion of outpatient visits for ILI was 5.7%, which is above the national baseline of 2.4%.”
The Time article and the Ohio Department of Health info gibe with my personal observations in my hometown of Troy, Alabama where it seemed like half the town had some flu bug in December 2019 and January 2020 (myself and my two children included). I’ve also saved about 30 articles from around the country, reporting school closures for “flu” outbreaks. I can’t recall another year where so many schools closed for the “flu.”
In my latest Substack article, I summarized the responses of approximately 150 people who contacted me, expressing their opinion that they had Covid before it was supposed to exist.
One thought is that the virus was less “nasty” early on. However, if you read these responses, it’s clear that these people were very sick in October 2019, November, December and January.
My citizen correspondents also mention that many other people got sick at the same time they did, suggesting “community spread.” It seems to me that there were “outbreaks of something” all over America. Perhaps significantly, most of these people report they tested negative for flu and many report they never had Covid after that (suggesting they had natural immunity). Seven of these respondents say they later tested positive for antibodies (the story says six but I miscounted).
Again, all of this points to a question that warrant more REAL investigations. Some bright people must have possible explanations.
Please could you consider whether covid was actually a side effect of the newly introduced QIVc flu vaccine in 2019?
https://www.facebook.com/239013323479861/posts/pfbid0EijT5eK219yfjMVRXyrvM28kFaF896kBUJe8Zq4s5PRenYQVkJ3CQ9zBag1DSVkdl/?d=n
I’ve never seen that – thanks. I’ve long wondered if the big spike of deaths in the winter of 2020-2021 might have had something to do with so many people getting their flu shots during and before those big spikes in deaths. This possibility has never been investigated either.
I recall some early work on Covid reporting that T cell immunity (rather than antibodies) was produced, meaning that not many people’s immune system needed to go as far as to produce antibodies.
All part of the smoke and mirrors of the plandemic? Perhaps March was not actually very different from February, January and December; and all winter the government were actively hushing up the virus, just like they’ve actively hushed up many other elephants in the room over the last two years, playing the card of “it’s nothing to worry about”, until it was time to “release the hounds” in March, and twist their figures to make it look as if it was wreaking havoc, shifting the odd zero here and there? Remember how the “deaths by Covid” suddenly dropped by a few thousand, as Saint Boris and his merry men decided to count them using the seven fingers on each hand that they have (because they’re not human) instead of five? Lockdown would not have had the same painfully isolating effect in the January and February post-Christmas hibernation that it did in late March, as the weather turned nice, and people wanted to be out and about.
I myself certainly caught some sort of virus in late 2019. I don’t know if it was Covid, but I was ill like I’d never been before, with many of the symptoms similar to the “official” ones (checks year, as the government moves the goalposts of official symptoms all the time). As has often been stated, if the virus (if it existed) had happened before the age of social media and 24-hour news, handpicked by the government, we might not even have known anything was amiss; people get ill in winter, people die all year round. And the government suddenly told us “People will die”. (Which they are doing in droves now, thanks to Saint Boris’s lockdowns.)
“I was ill like I’ve never been ill before” (in late 2019). This same sentiment is expressed over and over by people who think they might have had Covid in 2019 or early 2020. That’s one reason I put so much weight on these claims and don’t immediately discount them. Millions of people think they had Covid and most of them say this illness was unlike other illnesses they had experienced in their lives. When so many people report this virus was different in obvious ways, why shouldn’t we take note of this? Officials haven’t done this, but they should have.
Recently I posed the question of how things would’ve gone if political polarities (Republican vs Democrat, right vs left) were reversed in the USA in regards to the pandemic. Then I realized that such polarities WERE reversed until that fateful day when Governor Cuomo of New York panicked and, the rest was history. Suddenly the virus went from “no big deal” to “OMG it’s the plague!” almost overnight.
If the theory about the lack of spread among those most vulnerable is correct, it strongly supports the thrust of the Great Barrington Declaration
Community spread among the healthy was never the problem, but we knew that would be the case from the Diamond Princess data
Two thoughts.
“We really know very little but go about as if we knew a lot.” That is why covid was such a prime candidate for weaponisation by politicians. It is in essence the same as the Great Global Warming Swindle around 2004, and any number of Mencken Imaginary Hobgoblins in the centuries before that. Bartholomew and Evans’s original book “Panic Attacks” gives a highly-readable account of similar scares since around 1700, and studies the role of government-media collusion in maintaining them. We know more about Didymos 65803 than we do about Covid 19!
First they create the narrative, which is often false, and then they protect it by censoring and cancelling voices that would challenge it. And, yes, they clearly do this for a reason. They are exploiting or benefitting from bogus narratives.
The Nocebo Effect; it’s as real as the Placebo Effect. It’s how witch doctors/shamans in some ancient tribes/cultures can literally kill people by “merely” putting a curse on them.
Huge numbers of people may quite possibly have been frightened to death.
… as in, the IFR/CFR of an illness may be increased significantly by PR/govt and media messaging which indicates/persuades people that it is super deadly.
The IFR /CFR of Covid was *actually* lower before people had been “told” that there was a novel, dangerous etc virus on the loose.
NB. Apparently about 30-35% of the population tend to be very susceptible to the placebo/nocebo effect.
Just one of the couple of articles that I found and bookmarked back in March/April 2020 when I first thought that this might be a factor. I can’t find the other article.
https://gizmodo.com/how-the-nocebo-effect-can-trick-us-into-actually-dyin-1681746203
Found the other one; 🙂
https://theconversation.com/coronavirus-could-reading-about-the-pandemic-cause-harm-135585
Thanks for finding these links. I’ve saved them. I think this could provide some percentage, maybe small, of the post March-15 spike in deaths. Some people might have scared themselves to death. Or when they got scared and panic this influenced how they were treated by doctors and nurses, who thought they were much sicker than they really were?
I think you are right. I think there were more cases (far more “sick” people) in the early winter of 2019-2020 and far fewer deaths. By April 2020 (a warmer weather month and usually the end of the flu or virus season), this virus was on the down side of the slope. Still, this is when the death numbers went hyperbolic – at least in some places. Still, most communities didn’t have these huge spikes in deaths* – another mystery that hasn’t been satisfactorily resolved.
*For example, in my county in Alabama, it wasn’t until December 2020 that I personally knew one person who died from Covid. Even to this day, I only personally knew three people who died from Covid. They all died in the winter of 2020-2021. Two were in their early 80s and one was 70. I still wonder if the flu shot roll-out – in combination with Covid – might have had something to do with these deaths.
I also think people were dying of Covid in 2019 and early 2020. These deaths were just “Missed” or attributed to something else. The vast majority would have been in the elderly and infirm. I did a story on 39-year-old Tim McCain of Sylacauga, Alabama. He definitely had Covid in December 2019 (proven by his medical records and a positive antibody test) and he almost died several times the first week of January 2020. He is lucky to be alive, but there’s no doubt others weren’t so lucky.
Strongly agree with this. There is a wealth of research indicating that psychosocial factors play a key role in respiratory illness. For example, this study found “Factors we found to be associated with greater risk of respiratory illnesses after virus exposure included smoking, ingesting an inadequate level of vitamin C, and chronic psychological stress. Those associated with decreased risk included social integration, social support, physical activity, adequate and efficient sleep, and moderate alcohol intake.
If you consider that much of the population, particularly the elderly, who were most vulnerable, were terrified by the media and government propaganda, isolated from their social support networks, deprived of physical activity and possibly drinking more than usual, then it is hardly surprising that many of them succumbed to serious illness.
Absolutely this! ^^^^ 🙂
I can’t insert a graphic but if you go to the WHO flu net system and look at flu in England from say 2010 to 2022 there are large flu peaks in the years leading up to 2020. Then no flu at all, none, zero. It was the same in all countries from exactly the same day. ‘I am John Cullen’ has been flagging this up and has put together some excellent graphics. On Twitter and online.
This is the link to the chart for England https://app.powerbi.com/view?r=eyJrIjoiZTkyODcyOTEtZjA5YS00ZmI0LWFkZGUtODIxNGI5OTE3YjM0IiwidCI6ImY2MTBjMGI3LWJkMjQtNGIzOS04MTBiLTNkYzI4MGFmYjU5MCIsImMiOjh9
This is the link to the whole world chart, flu numbers growing since 2012.
https://app.powerbi.com/view?r=eyJrIjoiZTkyODcyOTEtZjA5YS00ZmI0LWFkZGUtODIxNGI5OTE3YjM0IiwidCI6ImY2MTBjMGI3LWJkMjQtNGIzOS04MTBiLTNkYzI4MGFmYjU5MCIsImMiOjh9
Again flu disappeared in 2020 then miraculously came back again in 2022.
I am not sure where the USA flu data came from in the article above but the WHO system indicates that there were much larger numbers. In 2018 at the peak there were over 25,000 cases, 17,000 in 2019 and then over 25,000 again in 2020. But ZERO in 2021.
USA – https://app.powerbi.com/view?r=eyJrIjoiZTkyODcyOTEtZjA5YS00ZmI0LWFkZGUtODIxNGI5OTE3YjM0IiwidCI6ImY2MTBjMGI3LWJkMjQtNGIzOS04MTBiLTNkYzI4MGFmYjU5MCIsImMiOjh9
Please refer to ‘I am John Cullen’ for a more thorough explanation. Credit to John Cullen for his investigation and reporting on this (on You Tube/Rumble/Twitter).
In the USA flu tests were not covered by insurance but covid tests were, so patients were tested for covid not flu. We know now, that the pcr tests couldn’t differentiate between flu and covid. The New York Post reported that around 48% of results were false positives. In the USA, hospitals were paid large sums of money to treat covid patients. If that patient went to ICU and was classed as a complex case it was worth up to $400k to the hospital with a further 10% bonus if the patient died. It was financially beneficial to have covid patients rather than flu patients. Also if patients had flu but were not treated for that there was more chance they would become ill and possibly die. Protocols that were used did not include early treatment and even now people are still being put onto ventilators when they should not be.
It looks highly likely that flu cases were called covid cases to inflate the covid numbers, then incorrect treatment, use of midazolam and lack of early treatment increased the deaths. Given that flu disappeared in every country in 2021 it would appear that a similar scam was operated in those countries also.
What was the motive?
There are a few possibilities.
1.’I Am John Cullen’ suggests that an earlier flu leak was being covered up.
2. Financial reasons
2.1 ‘Big pharma’ revenues have been on cliff edge for years following patent expiries and introduction of generics. New medicines tend to have poor risk benefit profiles and many have black box warnings or are aimed at a niche market so limited markets. The only hope they have of sustaining long term or growing revenues is through the routine /annual injection of healthy individuals. They knew that to get people to accept a novel injection they would have to make it more scary than flu (so they included flu numbers and added covid to make it look worse than flu). There is even a video of this conversation I can’t recall who was in it, Gates I think). Deaths were inflated by counting with covid cases not from covid and people with flu were counted as covid.
2.2 To prop up the western economy for a bit longer money with billions spent on all the covid measures.
3.To cover up a lab leak of the covid virus.
Being able to implement lockdowns, mask wearing to test our compliance, and force through digital ID in pursuit of the 2030 agenda was just the icing on the globalist cake.
Or maybe I am just imagining things.
Why did COVID deaths suddently goes so BIG after reporting about deaths of people after they had a positive PCR test result went so BIG? A mystery Will Jones certainly isn’t ever going to solve.
Exactly this!☝️ People were always coming to the hospital sick and dying. We just suddenly started testing for a ubiquitous virus and all their symptoms were automatically blamed on the virus.
Because it’s not the same virus. The PCR test is highly suspect.
Surely Midazolam and Remdesivir had a lot to do with it, not to mention early discharge of sick people from hospitals into care homes.
Perhaps the inconsistencies and mysteries could be better understood with an entirely different perpective on ‘viruses’. Please consider Dr Mark Bailey’s recent ‘A Farewell to Virology’ here..
https://drsambailey.com/a-farewell-to-virology-expert-edition/
The follow-up to that would be digging into ‘The Invisible Rainbow’ by Arthur Firstenberg as well as Piotr Garyaev’s ‘Wave Genetics’.
‘Virology’ itself is but a theory that may well be misleading…kind of like physicists basing their whole conceptual reality around ‘big bang’ theory 😉
Will asks lots of pertinent questions here.
My guess is that there is no single or over-riding answer – that there are a whole lot of things going on.
First of all though I’d question the base data. If something doesn’t appear to make sense, is that because the data is wrong? One of the problems we’ve had with analysing covid is that we just can’t get to bedrock data. From that point, everything’s a struggle.
Will asks why it might be that SARS-COV-2 suddenly became much more transmissible in spring 2020, when it had almost certainly been around since autumn 2019.
As I and many others have written here and elsewhere, there was clearly a covid-type bug going around in late 2019. At Christmas the TJN had what were later to be recognised as the absolute classic covid symptoms. Knowing nothing about SARS-COV-2 at that point, we just remarked on what a miserable and odd bug it had been, and moved on. Looking back, it seems to me it was almost certainly covid.
Thing is though, absolutely loads of people around us (in SW Devon) had the same bug at the same time.
Whatever it was – and it probably was SARS-COV-2 – it was certainly highly transmissible.
As I say, Will asks lots of pertinent questions about the virus and the effect of societal responses. But my instinct is first of all to question the data. I don’t think we’re on bedrock.
Yes, already highly transmissable; what changed is how people viewed it, and how lethal it became to many people as a result of that frightening new presentation/perception of it, the very real and powerful nocebo effect.
Virology itself might be unable to explain the inconsistencies and mysteries of the Covid scenario…
https://drsambailey.com/a-farewell-to-virology-expert-edition/
When looking at excess deaths over the years, it appears that the last couple of years were not extremely unusual (see some of Clare Craig’s data).
Just some thoughts on a few variables which may have played a role. I know not all these variables lead to excess deaths, some have more to do with attribution of deaths to SARS-CoV.
Please could you consider whether covid was actually a side effect of the newly introduced QIVc flu vaccine in 2019?
https://www.facebook.com/239013323479861/posts/pfbid0EijT5eK219yfjMVRXyrvM28kFaF896kBUJe8Zq4s5PRenYQVkJ3CQ9zBag1DSVkdl/?d=n
“The virus still keeps its secrets.” And guess who does the same; no shortage of the ones that screwed it up and caused a lot of damage to us all.
Since when have we been testing for flu?
I thought the criminal, fraudulent and spurious testing was brought in specifically for “Covid” to a) frighten us and b) keep the nonsense going for however long they wanted (which it stupidly still is).
You are also assuming all these deaths are from Covid when in fact very few are – 5% Covid only 95% with 2 or more comorbidities.
It’s the “testing” what does it! Simples.
John Dee’s Almanack on substack has been crunching the numbers and describing it as a testdemic for a while now – see his testing testing thread. https://jdee.substack.com/p/testing-testing-part-1
It is unlikely in the extreme that we will ever have a proper answer to this fundamental question simply because we reached the limits of our understanding of the complexities of the immune system a long time ago. No money in it you see.
The same alarming lack of knowledge also applies to virus. Do they spread/cause disease in the generally accepted sense or are they merely an artifact of electron microscopy/blast genetics/exosome expression?
There are supposedly 40 million virus (just random bits of nucleotides?) in a cubic metre of air. How does the immune system deal with that lot – why are some apparently harmful whereas the rest aren’t.
Anyway it seems not to matter, purely because there is money to be made and control to be had if one can persuade people that the only way to salvation is elimination of disease by manipulation of your genes aka mRNA jabs.
All hail our wonderful genetic engineers. They have no clue as to the harm their product will cause.
GATTACA for all.
In my view, this is not complicated.
The common cold, coronavirus or other, is lethal to the elderly with co-morbidities or a history of previous respiratory infections.
Where are most of those to be found? In big cities or areas of heavy air pollution, also care homes.
Where were the worst mortalities for covid: Lima, Wuhan, New York, Northern Italy etc. and care homes.
Britain’s covid 19 mortality spike simply coincided with hospital clearances that, by spreading the disease quickly, replicated the effect of high density housing occupied by the most vulnerable as had been the case in Lima, Peru.
‘Patients with prior respiratory diseases were globally less likely to be hospitalised for COVID-19 than for influenza but were at higher risk of developing severe COVID-19 and had a higher mortality rate compared to influenza patients and patients without a history of respiratory illness.’
Chronic respiratory diseases are predictors of severe outcome in COVID-19 hospitalised patients: a nationwide study
European Respiratory Journal 2021
I got the mystery illness (now believed to be Covid) in late December 2019.
My mother was in a care home.
The care home policy was that relatives should not visit when they were ill. I understand that most care homes operate this policy in the UK.
I waited until I was symptom free for a few days before I went to visit.
Perhaps this type of care home policy delayed many elderly and vulnerable people getting Covid-19.
Very logical point, John. Thanks. Perhaps …. Bingo. I think this is important and has been overlooked. Why didn’t folks in nursing homes start dying earlier? Because they didn’t get the virus on a large scale earlier – because their visitors who might have been sick didn’t visit them. Nor would employees who were sick be working. Theory: They got it when they started going to the hospitals and then coming back to the nursing homes.
‘This leads to a mystery: why did COVID-19 only start killing lots of people come spring 2020.’
No mystery: when every hospital death has CoVid on the death certificate, because death by Covid is assumed or ‘confirmed’ by a test that will produce viral fragments from dandruff.
I thought this was clearly understood by now given we know during 2020 there were only 6 000 deaths in UK CAUSED by CoVid, much less than a mild ‘flu season.
The ever-insightful Michael P. Senger and Emma Woodhouse pointed this out for the USA just the other day, especially in the first big epicenter, NYC.
Very important article by Michael IMO.
My theory: the virus was originally much milder, that is, UNTIL the lockdowns put selective pressure on the virus, selecting for both nastier AND more contagious strains than would otherwise have occurred. That is in ADDITION to the direct iatrogenic effects of the lockdowns, restrictions, and panic themselves (and midazolam, vents, etc.)
It elegantly explains the excess deaths in subsequent waves (but before the jabs) as well, and also the excess deaths that occurred in countries and states that largely ignored the virus (Sweden, Belarus, Nicaragua, Tanzania, South Dakota, and also the Amish in the USA), albeit similar to or lower than their neighbors. And in the places that largely ignored the virus, except for Sweden, they did not experience excess deaths at all until months later, when they got the secondhand spillover from the rest of the world.
Maybe something to that, but it seems like there were a lot of people in November, December and January who were very sick. That’s what many people report. They also report whatever they had, other people around them were getting it at the same time. So if was not that mild a virus and it was spreading. It just hadn’t spread widely in nursing homes yet – probably for the reasons outlined by John Dempster above.