
Does anyone still recall the excitement in late 2020 when the vaccines against COVID-19 were finally in sight? The trial results were excellent, promising an end to the pandemic in 2021. The main worry was the availability of the vaccines and of course equitable distribution between countries.
I believed in the narrative myself, even if scientists I know and trust had voiced doubts about the vaccines’ effectiveness against infection I saw no reason not to believe the trial results. In early 2021, when worries arose regarding vaccine sourcing for the Icelandic population, I even took part in an attempt to have one of the manufacturers arrange a population-wide trial in Iceland, similar to what Pfizer did in Israel. Today I’m very glad we didn’t succeed.
Soon it will be two years since the trial results were out. The virus still ravages the world, though it may have become less deadly. Data on infection, hospitalisation and mortality already show vaccination not only failing to prevent those, but in some cases being counterproductive. In short, the vaccines have failed to deliver what we were promised. And even worse, the skyrocketing rate of side effects may mean that for most people vaccination makes no or little sense.
Still, it is for the most part forbidden to discuss this fact. For example, LinkedIn, the world’s largest online professional community, explicitly forbids content that draws attention to potential harms from the vaccines or how they may be counterproductive. The policies of Facebook and Twitter seem to be largely consistent with this.
As an example, it is forbidden to say COVID-19 vaccines may cause death, even if a quick search on the internet shows confirmed cases where there is no doubt about the causality. It is forbidden also to share evidence showing higher infection rates among the vaccinated than the unvaccinated.
It will therefore be interesting to see how those platforms will react to those who share the results of a new research letter published on August 3rd in Jama Network Open. The letter describes the result of a study which monitored for reinfection all Icelanders previously infected, during the Omicron wave, between December 1st 2021 and February 22nd 2022. The study shows a probability of reinfection of up to 15.1% among 18-29 year-olds, declining with age. Reinfection is not surprising considering the reinfection rates seen around the world after the appearance of Omicron, though the authors expected a lower rate.
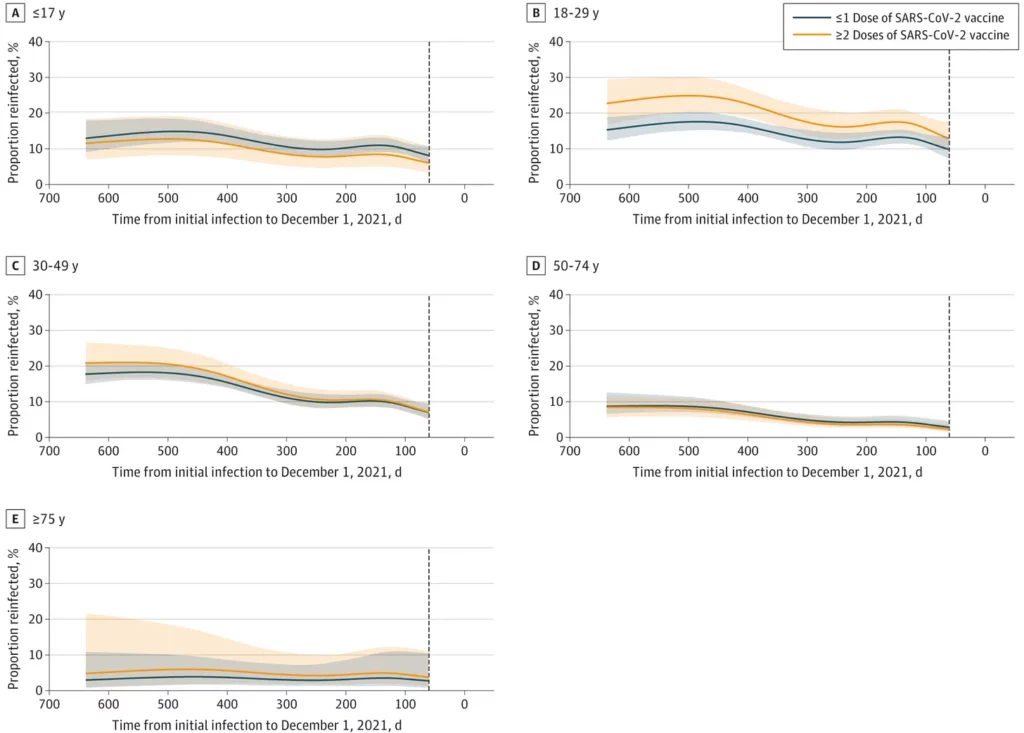
But the most interesting part is the comparison by vaccination status. It shows that for most age groups, those who have received two doses or more are more likely to become reinfected than those who have received no vaccination or one dose. The difference is small, but it is statistically significant. In the authors’ own words: “Surprisingly, two or more doses of vaccine were associated with a slightly higher probability of reinfection compared with one dose or less.”
This article was first published on Thorsteinn Siglaugsson’s Substack newsletter, From Symptoms to Causes. You can subscribe here.
Postscript: It has been pointed out that the authors of the study referred to in the above article have included the following health warning about their results which Thorsteinn Siglaugsson omitted: “This finding should be interpreted with caution because of limitations of our study, which include the inability to adjust for the complex relationships among prior infection, vaccine eligibility, and underlying conditions. Importantly, by December 1st, 2021, all persons aged 12 years and older were eligible for two or more vaccine doses free of charge, and 71.1% of the Icelandic population had been vaccinated, compared with only 25.5% of our cohort of previously infected persons.”
In Thorsteinn Siglaugsson’s defence, the significance of the facts referred to in the health warning is unclear. Why should the fact that the previously infected have a different vaccination rate to the general population make any difference to the finding that the reinfection rate is higher in the 2+ dose vaccinated compared to the one or less dose group? After all, all those in the study have been previously infected, so there is no need to control for previous infection rates.
The sentences are also somewhat misleading in that they draw attention to the overall Icelandic vaccination rate of 71.1% and compare it to the vaccination rate in the previously infected of 25.5%, without pointing out that those two groups are likely to differ considerably in age profile and other factors. There’s also the question of why the authors don’t provide the single-dosed rates separately to the unvaccinated rates, when they clearly had access to the data.
Note also that the study’s description of two or more doses of vaccine being associated with a “slightly” higher probability of reinfection compared with one dose or less is misleading as the study actually found it was 42% higher (CI 13-78%), which is hardly slight. The authors appear to be playing down their findings in relation to vaccination status (perhaps under pressure from the journal editors), so we would not necessarily want to repeat the misleading or confusing claims they make.












To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
I believe I am correct in saying that jabs going into arms today are still coded for the original spike protein from 2020? I think an updated version is on the way but is not in general rollout yet.
I don’t know enough about the rate of mutation in the actual ‘nucleus’ of the virus but if you’re only receiving the ‘outer shell’ which seems to have changed significantly in two years then that would go some way to explaining the failure to provide any significant protection in my mind.
You are over-thinking this issue.
The “vaccines” that are not vaccines are simply designed to maim and kill within the period of approximately five years. The data would suggest the snake oil injections are performing admirably in this respect.
I agree. The S1 spike protein is a patented bioweapon, and is designed to maim or kill in a multitude of different ways. This is one of many proteins that make up the ‘virus’, so you would have to be extremely naive to believe that all manufacturers just happened to choose this one. I agree with you, as ever, this was an attack.
Thanks CG, and good to hear from you.
Virus has no nucleus, it is just a parcel,of genetic material, in this case RNA which is an instruction for when the virus penetrates a Human cell, how the chemicals in that cell can make copies of the virus – up to about 100 000 per cell, at which point the cell membrane ruptures releasing the copies.
On entering the cell, the virus causes a ‘spike’ of part of its protein to form on the cell surface and which the immune system recognises as foreign and reacts accordingly.
The mRNA carry part of the viral RNA which allows it to enter body cells and reproduce copies which also means the ‘spike’ forms. This alerts the immune system.
RNA virus mutate and evolve rapidly, which means new virus with slightly altered RNA which will produce a modified ‘spike’ which the immune system does not recognise, and since it has not ‘seen’ the whole virus, it has no other clues.
Any new vaccine is always going to be obsolete by the time it gets into arms, because the mutant version upon which it was based, will have evolved further.
Colds & ‘Flu are caused by fast evolving virus which is why there are no safe effective vaccines against them… no not for ‘flu, that’s just a sales campaign each Autumn.
I think the flu vax is no more effective than a placebo, so may as well hang a rabbit’s foot around your neck and pin all your hopes on that. In fact, that would be a good experiment. But never ever has the flu jab been pushed on the global population anywhere near the extent of this crazy shit. What we’ve witnessed and lived through is something off the scale that I hope will not be repeated for a third year running, despite all of their best efforts.
What a surprise. Re bullet point 5, it gels with the reality that it is not a conventional “vaccine” under the old definition. Rather it is a mitigation drug for those that become infected, thus those who are suffering from it with reduced symptoms might be more likely to dish out their infection to others, unfortunately.
There is no reason why a vaccinated person with an infection will be more infectious than an unvaccinated person with an infection, the virus is the same, the symptoms the same.
infection of a third party is dependent on the viral load they receive and the state of their immune system – and that is not dependent on the vaccination status of others.
The ‘less serious’ claim is not backed by any data, there is no evidence that vaccination is capable of preventing serious symptoms any better than natural immunity.
Prior to the vaccines over 99.5% of infections were ‘less serious’.
In other words it’s a prophylactic, just like a condom – but a condom with holes in it.
I believed in the narrative myself, even if scientists I know and trust had voiced doubts about the vaccines’ effectiveness against infection I saw no reason not to believe the trial results.
??
When they announced the Pfizer trials results at 95% effective Mrs TJN and I looked at each other and said ‘WHAT?’ 95%?? – vaccines that have been around and have been tuned for decades have effectiveness rates much lower than that. And they hit 95% on first go? Alarm bells ringing everywhere.
And then there were the ominous levels of side effects. The one or two cases or transverse myelitis, and MS, looked worrying considering the low number of trial stabs. But there was also some massive percentage (don’t recall what now, but it was large) of headaches etc., which raised some very profound questions about what was going on (we now know this was probably clots).
The next paragraph is from my memory, haven’t got time to check now – please anyone correct or confirm from their own recollections:
And no one seems nowadays to talk about Astra Zeneca. Does anyone recall now that the initial AZ results for two doses gave an effectiveness level of circa 68%. But – apparently unnerved by the Pfizer results (i.e. lies) – and desperate to claim something similar, they said that by mistake they’d given only one shot to many trial participants, and that to their surprise these participants were getting circa 95% effectiveness. (!!!!????) So they were so desperate to keep up with the Pfizer lies they were prepared to admit the sort of gross trials mistakes that should have warranted an investigation and got them banned from ever doing trials again. And that’s supposed to inspire confidence??
So from the very outset Mrs TJN and I did not believe the claims – and neither did many BTL contributors on this site.
It’s amazing how many level-headed people were taken in at the time – I can’t work it out. Maybe to do with the level of hysteria which had dominated the previous months, and left even many lockdown sceptics desperate for a way out.
I was always highly sceptical that a vaccine would be the way out of covid (I never really thought looking for a way out was feasible or needed) but I was open-minded about having it. I decided to wait a while and monitor things before making a decision, because the whole thing seemed rushed. I can’t understand why anyone with an ounce of sense wouldn’t do the same. Nothing I’ve seen since has persuaded me that waiting was the wrong decision, and now it’s a definite NO – certainly the current covid “vaccine” is useless and on balance harmful, and I am not sure I would bother with any covid vaccine unless covid suddenly becomes a lot more dangerous, and I think I would be sceptical of any mRNA vaccine as the undue haste and lying puts me off. I would think very long and hard about getting any vaccine now, as I have lost confidence in the medical profession and the regulators.
It helps if you already were an “anti-vaxxer”. :-
http://vaccinepapers.org/
and for the mRNA jabs :-
https://www.sciencedirect.com/science/article/pii/S027869152200206X
In the very early days, knowing nothing about immunology as I did (still don’t know that much now), I assumed that a vaccine would be useful for vulnerable people – if it could be developed and implemented sufficiently, but that it might take a couple of years or more to get something ready. I didn’t understand then how difficult developing vaccines to these sorts of virus was.
Very quickly cottoned on to the fact that the Pfizer/AZ/others vaccines were likely to be very questionable that certainly no healthy person should risk taking.
I never for one nano-second had any thoughts of taking this shit.
There was also another screaming red flag: as they were implementing the first jabs in December 2020 there was absolutely no attempt to distinguish the covid-recovered. Every ‘vulnerable’ person was to have the jab. But it was already clear that the covid-recovered had effectively water-tight resistance against subsequent serious infection. So they didn’t need an experimental stab. As I say, alarm bells ringing everywhere.
Nope, no more vaccines for me, and I look forward to the day when the medical regulators responsible for authorising and pushing the covid stabs are in jail.
The fact they tried to downplay recovery from infection was indeed a big red flag in the scam. When they were talking about adding ‘recovered status’ to the nazty pass, the head of the Dutch OMT wanted it to be valid for a period of 18 months. EU politicians with no medical background (but quite probably lots of pharma stock) insisted that it be cut to 6 months! Disgusting, having people have poison pumped into their veins just to line their pockets. Would still love to see the details of the deal Ursula fond of Lying made with her buddy Bourla, purchasing enough poison for 2 doses for every EU citizen in April 2021, *after* enough poison had already been purchased to poke everyone twice. How did she know further doses would be necessary? And why did she agree to pay pfisser 25% more than for the preceding purchase?
I remember Didier Raoult, a well-known French infectious diseases expert, who was originally on the French OMT, saying around Feb/March 2021 that people should be treated with HCQ but that the treatment needed to start as soon as symptoms started, otherwise there was no point. He was ignored and vilified.
The fact that people still cannot choose for themselves whether or not they wish to try HCQ or ivermectin is a serious red flag. The safety profile is well-known, they still have to be prescribed by a doctor, so a doctor could determine whether it might be contra-indicated for some reason or another for a particular individual, so from a safety perspective there is zero reason not to let people make that decision for themselves. If it didn’t work, this would become clear quickly enough – took about 4 weeks to figure out that the only efficacy pfaxlovid has is in increasing profit. The only reason to not allow use of these drugs is because they are obviously terrified that it will then be proven that they are indeed effective treatments, cheap and truly ‘safe and effective’. They won’t be able to hide that forever either.
I agree with you, except I would categorically never get a Covid injection. A respiratory virus doesn’t suddenly mutate to become more pathogenic after evolving less and less so, as nature intended, so if we suddenly hear that it does with Covid then all of our BS detectors should be sounding the alarm. But the way this Omicron cold is affecting the multi-jabbed I’m not sure they’d need to manufacture another scarient.
I’m a person who doesn’t even take paracetamol unless absolutely necessary so taking this jab would be like using a sledgehammer to crack a walnut, especially regarding the alarming speed that it came to market. I remember the whole Swine flu fiasco from years ago you see, and being a nurse we all dutifully got our jabs, fit tested for respirators and awaited the tsunami of sickness and death that was forecast to come our way. And we all know how that went down! I’ve become a lot more savvy and sceptical since then so I wasn’t about to fall for this hyped up nonsense based on crummy modelling again.
Now I’m like you and won’t trust any vaccines ever again. Let’s just assume the depopulation theory is correct, and this is one of their aims, do you really think they’d limit their nefarious practices to just the Covid jabs? It’s perfectly possible they could manufacture regular vaccines in such a way that would have seriously harmful effects over a period of time. I’d find it an odd notion to distrust Big Pharma and the regulators with these specific injections but be completely compliant and accepting of safety for all other vaccines just because they’re the ‘traditional’ type. I’ve zero confidence in the industry now ( particularly the very lucrative vaccine manufacturing industry with Pharma enjoying immunity from liability and the consumer ‘enjoying’ all of the risk ) and zero tolerance for shady companies with chequered histories who put profit above safety and ethics.
I’m a person who doesn’t even take paracetamol unless absolutely necessary
Yep, same as me. Very rarely touch the stuff, and then invariably only in the form of lemsip.
So no way I was every going near the covid stabs.
Big regret: my children have had all the standard immunisations to age 3. They won’t be having any more. I feel very guilty about their having these jabs, and will apologies to them when they are old enough to understand – maybe write them a letter or something to be opened when they are adults.
You are getting there Mogs.
LOL! Well its my rule of thumb now to discount nothing and keep an open mind to all theories. What would once have been scoffed at now looks like an actual possibility, sadly.
Look at those tiny chips the Swedes have had injected under their skin for several years now. They don’t even need to use money or cards, just scan your hand against the machine and you’ve paid for whatever item, travel, access to areas within the workplace etc, no need to carry any I.D or even car keys. Now they’re on about getting all the individual’s health data put on these chips so everything’s to hand. Literally!
This would have sounded completely woo woo years ago but now look where we are. I guess this is some people’s idea of progress but it sure as hell ain’t mine! This vid covers it;
https://www.youtube.com/watch?v=M4y7youazpo&t=718s
https://www.conservativewoman.co.uk/needless-jabs-the-death-penalty-for-thousands/
Here you go!
‘I’d find it an odd notion to distrust Big Pharma and the regulators with these specific injections but be completely compliant and accepting of safety for all other vaccines just because they’re the ‘traditional’ type.’
Yes something very odd has happened. Similarly, I know quite a few left-wing types who would have been the first to criticise Big Pharma but queued for the jab when it arrived. This is where the mass formation side of things comes in..
The jab roll-out started in the UK in January 2021. I was already concerned by the speed with which they had been produced and the indemnity given to the Pharmaceutical companies: it was simply not credible that a process of authorisation which usually takes around 10 years could be safely condensed to 1 year by running various stages concurrently.
So I was trawling the net, looking for information. And I came across an early warning in Feb 2021 (in Zerohedge, I believe) that the Israelis were concerned about the Pfizer jab causing Myocarditis in some people.
So the Government KNEW from Feb 2021 at the very latest that the jabs weren’t safe. But they rolled them out anyway and coerced millions to have something they not only didn’t need, but were positively dangerous …… and they still are.
They are evil people.
So the Government KNEW from Feb 2021 at the very latest that the jabs weren’t safe.
Yes, and they should have been pulled at that point – February at the latest.
In fact, BTL on here (but not ATL) was full of stuff about the side-effect problems from the moment of the ‘roll-out’ (horrible term).
Yep, they are evil people.
Incidentally, I’m not sure death caused by the vaccine should be described as a ‘side effect’. Death is pretty fundamental.
After the Ocean Princess I knew the scam was on.
After the concerted effort to delegitimise alternative therapies, Ivermectin and HCQ, I knew the Vax was an agenda item not to be trusted.
Oh and natural immunity won’t work.
Sheite just got crazier and crazier and the retarded crowd around me kept accepting more snd more nonsense right up to the mandates.
Anyway we all know the painful story.
I guess the question is how the author is so late to the party.
Now that is a much more pithy response.
Unfortunately, the author has not yet got to the front door of the party. These injections have been designed and built to maim and kill. My repeated phrase is “made / built to a recipe” with maim and kill factors among the ingredients list. I have been repeating this for months.
There is little pleasure to be had in reporting that the esteemed Dr Mike Yeadon has recently posted similar statements. I think Burlington Bertie posted a link.
I’m still trying to get my head around the designed-to-kill idea of this recipe.
It certainly seems that way considering the toxicity of the various known ingredients and the way people are continuously dropping down like flies with cover-ups all over the place.
Somehow it just seems too blatant to be intentional. I guess my cock-up conspiracy line ends at that point. I prefer to think that the project was to normalize blindly injecting your population semi annually and then the formulas could be tinkered with to control the herd up to and including creating new illnesses dependencies and culling. I have difficulty imagining that they came straight out with the kill formula be it over 5 years or not. That just seems like a dumb plan. I mean surely that will eventually be figured out by the herd?
My view is that maiming and killing gradually via scammed illnesses and emergency ‘vaccines’ to deal with their latest brew is likely to wake up the whole planet, which will release a tsunami of destruction that even the Davos Deviants (DD’s)would not be able to avoid.
The last thing the DD’s need is millions awakening to the fact that they will be dead in five years.
The depopulation agenda needs to be largely complete by 2030 to meet its target.
https://www.conservativewoman.co.uk/needless-jabs-the-death-penalty-for-thousands/
Just the fact that these jabs went from being aimed at the elderly and ‘at risk’ people, with spokespeople even declaring early on that they wouldn’t be necessary for younger folk, then that quickly morphed ( and the previous targeted advice memory-holed ) into going down the age groups…then when pregnant women and kids ( and babies FFS! ) were included to be targeted, well, you’d have to extremely thick indeed not to at least smell a rat and question this “public health” message. The only interest they have in public health is to decimate it in a multi-pronged attack, as evidence a-plenty demonstrates these last 2.5 years.
There’s a lot of cognitive dissonance and much has to do with, I suspect, the sunk cost fallacy. I imagine this applies more to people such as doctors who were actively promoting the jabs and supporting the narrative all along. Many doctors are gonna look pretty silly and incompetent if they turn around and say, “Actually I was wrong the whole time because I followed the dogma instead of the data.” There’s a lot of ego involved with many healthcare professionals I’m sure.
Just look at how fervently they’ve all advocated mask wearing. Can you imagine them eating humble pie any time soon and admitting they were taken for fools? People who’ve dedicated many years of intensive training and work to all things health/medicine-related are suddenly going to admit they haven’t got a clue about health or science because they were so spellbound and taken up by the hysteria and propaganda that they forgot what “evidence-based medicine” is? Not likely. Their reputation is at stake and to admit they’re wrong takes some serious nerve because it reflects very poorly on them as professionals and the public trust will surely be negatively affected. The entire crappy NHS and their constant cheer-leading of the narrative is a case in point.
Of all the sectors its the healthcare sector which I find to be the biggest let down in all of this. We expect politicians and pharma companies to be bent, for example, but doctors and nurses are meant to stand for science, health-promotion, integrity and have patients’ best interests as a priority. They’re meant to be on our side and we should feel safe under their care and trust their judgement because its based on the best available evidence. And yet these charlatans have been the biggest back-stabbers of the lot as far as I’m concerned.
Top class Mogs
Not far to go now.

Anyway we all know the painful story.
We know the story so far, but heaven knows what’s coming down the line on medium- and long-term side effects.
Yep, anyone with an ounce of common sense should have realised from April 2020 that something was very, very wrong about what the authorities were telling us.
2 possible hypotheses are an underactive right cerebral hemisphere (see Iain McGilchrist) and Mass Formation (see Mattias Desmet).
Yes, just plain stupid in the vernacular.
Trouble is, stupidity comes at a price.
“And no one seems nowadays to talk about Astra Zeneca”
Journalist Oliver Wright wrote for the Independent some years ago on the subject of big pharma corruption, including from A.Z. (and Pfizer). Now working for the Times, he is apparently no longer asked to write on this subject (or any other Times journalist that I’ve heard of), let alone corruption relating to the experimental “covid” medication.
See here
Revealed: Big Pharma’s hidden links to NHS policy, with senior MPs saying medical industry uses ‘wealth to influence government’ | The Independent | The Independent
And here
Big Pharma lobbyists exploit patients and doctors | The Independent | The Independent
Times muppets.
“The virus still ravages the world..”
Huh?
Not even sure the virus hype still ravages the world.
I did a double-take at that bit too, lol..Unless its Icelandic sarcasm.
Hmmm. <strokes chin> It might well be Icelandic sarcasm Mogwai.
Can’t we finally bury this total nonsense? No vaccine (and – for that matter – no other kind of medication) protects against infection, as determined by doing a test for pathogen RNA or DNA incapable of distinguishing between live pathogens and fragments of dead pathogens. The immune system of the body is not some kind of biological AA artillery shooting down incoming germs before penetration of its own airspace.
I still find it surprising that people are saying that they believed the claim about the vaxx stopping infection.
What claim? When the trials started, the only thing being claimed was that the vaxx would help suppress symptoms. It was never claimed to stop infection or even to keep people out of hospital or prevent death – the latter two are a somewhat more logical conclusion in the sense that if symptoms such as severe respiratory distress could be mitigated, fewer hospital admissions and deaths would be an expected consequence.
Simply the fact that the producers peddling this poison initially did not claim it stopped infection should have been enough. If they could have claimed it, they absolutely would have, they weren’t being cautious, they knew it wouldn’t.
The only reason they could come up with studies indicating some reduction in infection was probably because 1) they started poking people right in the middle of a wave, so infections would be going down anyways (same trick they pulled with the lockdowns) and 2) by claiming that people who got infected in the first two weeks after the 1st poke or in the week after the 2nd, were not yet ‘protected’. This claim should never have been accepted or the weeks between injection and infection should have been included in the calculation of ‘efficacy’ in some way. This is particularly significant now we know that the vaxx intentionally suppresses the immune system in the first weeks after injection, making people more likely to become infected. We were told that people became infected because they unfortunately were exposed to the virus before the ‘protection’ kicked in. That was clearly an outright lie, one they still peddle and one a lot of people still believe. In fact, the claim of 1 week after the subsequent injections strikes me as mendacious – if the poke suppressess the immune system for 2 weeks after the 1st poke, it must surely do so for subsequent pokes as well. What a scam.
Gert van der Bosch (?) posted severe warnings about “vaccinating” during the middle of a wave did he not?
https://www.conservativewoman.co.uk/needless-jabs-the-death-penalty-for-thousands/
Let’s say this brings the subject up for tighter scrutiny.
Just seen in the Mail that Britain is the first country in the world to approve the new Moderna vaccine. Couldn’t be anything to do with the conract to build a new factory in the UK could it? My cynicism just gets worse each day. Anyway, going to my singing lesson now & hopefully put all the nonsense behind me for a while.
Ps I see that Valneva have cancelled their production due to lack of orders. I wonder why that might be?
“New Icelandic Study Shows Covid Reinfection Rates Rise With Number of Vaccine Doses”
Excuse the language but I am sure for many on here the reaction to this headline will be:
No Shit Sherlock
‘… though it may have become less deadly.’
Less deadly… compared to what? It wasn’t ‘deadly’ in the first place except in the same way as ‘flu, Common Cold or peanuts can be deadly.
‘I believed in the narrative myself, even if scientists I know and trust had voiced doubts about the vaccines’ effectiveness against infection I saw no reason not to believe the trial results.’
Clearly you hadn’t been paying attention to the climate doom ‘debate’ – a parallel and primer for the CoVid & vaccine ‘debate’ – where trusted, dissenting scientists are vilified, ignored, and silenced and ‘the ‘science’ is junk peddled by charlatans and liars.
I wonder if based on your recent experience with ‘the science’ and the approved ‘experts’ you would indicate whether you are still a climate change believer – I know I shouldn’t assume, but I assume you are, because anyone so easily taken in by the CoVid scam certainly is prey for that fraud too.
Great Post.