
The COVID-19 vaccines have been in use among the public for over a year now, having first been approved and rolled out in December 2020 in the U.K. and Israel. The trials reported them to be safe, but the time period was short and the study population relatively small, and there are concerns that a trial run by the company trying to bring the vaccine to market may not always be run to the highest standards of honesty and transparency. Subsequent revelations about the trials have suggested some adverse events may have been overlooked or worse.
What do we know now about the safety of the vaccines?
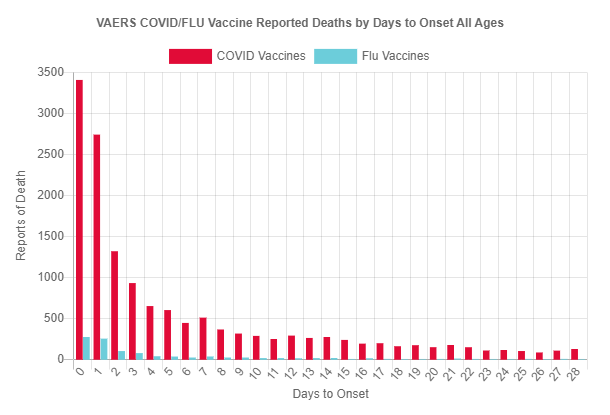
First, let’s distinguish two types of vaccine injury, short term and longer term. Short term injuries occur within 28 days of receiving the vaccine. They are what are typically reported to adverse event reporting systems like VAERS and Yellow Card, and data from VAERS show reports of them cluster in the first few days after the jab (see below). We would expect any signals of them in mortality data to correlate with the vaccine rollout. Longer term injuries, on the other hand, we would not expect to have any correlation with vaccine rollout, meaning it may be harder to spot the signals or associate them with the vaccines.
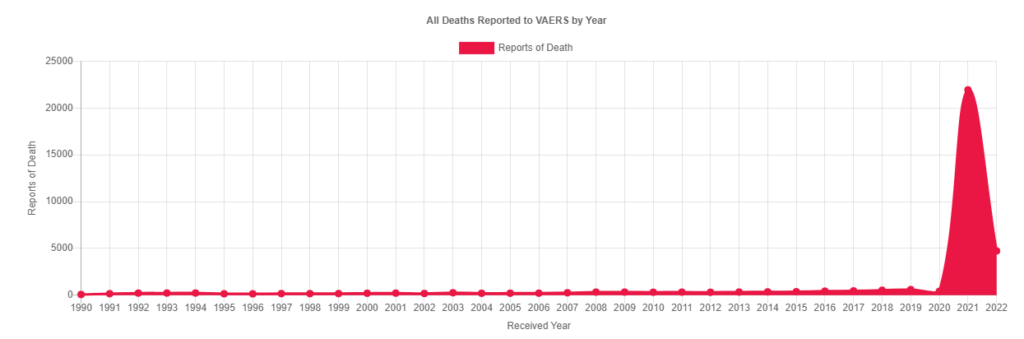
Looking at short-term injuries first, up to March 18th 2022, 26,059 deaths have been reported to VAERS, including 11,943 Americans. As the graph below shows, this is vastly more than have been reported in previous years, which is due of course to the Covid vaccines. In 2021, 21,940 deaths were reported, compared to 605 in 2019, the next highest year, a more than 36-fold increase. Other adverse events show similar levels of increase on previous years. In the U.K., 2,061 deaths have been reported to the Yellow Card system since the start of the pandemic up to March 9th 2022.
Passive reporting systems like VAERS and Yellow Card are not designed to establish rates of adverse effects (though such comparisons can be informative if their limitations are understood). They are designed to pick up signals of potential adverse effects which can then be properly investigated. Unfortunately, this allows regulatory authorities to dismiss even large numbers of reports by investigating them and concluding there is no link. While high numbers of reports of adverse events were stacking up already in January 2021, it wasn’t until mid-March that the problem with blood clots from the AstraZeneca vaccine was acknowledged by regulatory authorities, and then only because it was brought to their attention by scientists in Norway and Denmark, not because the regulatory agencies in most countries were doing their jobs in monitoring safety. We shouldn’t assume that if there are strong signals then governments will necessarily pick up on them and follow them up.
Some of the adverse event reports will of course be incidental. A far larger number of adverse effects will go unreported. One analysis of early Covid reports to VAERS concluded that up to 86% of deaths to that point (almost all in the elderly and high risk as this was early in the rollout) were linked to the vaccines. A pre-Covid 2006 meta-study found that reporting systems of drug adverse events typically picked up about 5% to 20% of events, suggesting an under-reporting factor (URF) of between five and 20, i.e. the real number of adverse events is five to 20 times greater than the number reported. The MHRA has previously estimated that the Yellow Card reporting rate may be approximately 10% of actual figures, suggesting a URF of 10.
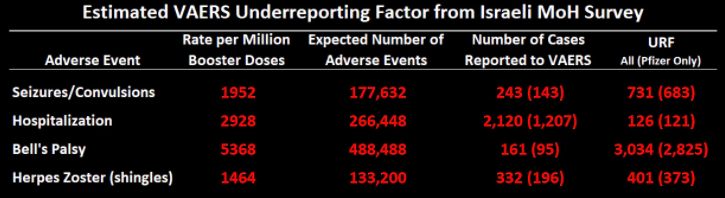
It might be thought that with the higher numbers of adverse events being reported with the Covid vaccines, and with the higher profile of vaccine safety systems in the pandemic, under-reporting rates would drop. However, that isn’t necessarily the case. The Israeli Government undertook what is, unfortunately, a very rare exercise in vaccine safety – a proactive survey where it asked a representative sample of 2,049 third dose recipients their experience of adverse events.
Dr. Josh Guetzkow, a senior lecturer at Hebrew University of Jerusalem, analysed and summarised the results:
- Two thirds of the respondents (66%) reported at least one side effect within three to four weeks after the jab (75% of women).
- Close to one third of respondents (29%) reported that they had “difficulty performing daily activities” due to the booster side effects (51% of women).
- One in three hundred respondents (0.3%) reported hospitalisation (not just medical care) as a result of the side-effects.
- Nearly 10% of women under the age of 54 reported disruptions to their menstrual cycle after the injection. Half of these women reported ongoing menstrual symptoms in a follow-up survey two to three months later.
- Around 5.5% of the respondents reported chest pain (7% of women), and 4.2% reported enlarged lymph nodes (6% of women).
- Close to 5% reported neurological problems (6.9% of women), including Bell’s palsy (facial paralysis; 0.5%), eye disorders (0.5%), memory issues (0.4%), hearing issues (0.4%), convulsions (0.2%) and loss of consciousness (0.2%).
- Around 4% reported allergic reactions (5.3% of women).
- About 25% of people with pre-existing auto-immune disorders, depression or anxiety reported a worsening of their symptoms following the injection.
- Around 5% to 10% of people with diabetes, hypertension, and lung and heart disease also reported a worsening of their condition.
Comparing these rates (which are shockingly high) with VAERS reports, Dr. Guetzkow estimated under-reporting factors for different events on VAERS (assuming that Israeli and American populations are broadly comparable). He found an under-reporting factor of about 120 for hospitalisations, 700 for convulsions or seizures, 3,000 for Bell’s palsy and 6,000 for enlarged lymph nodes – meaning the real number of these adverse effects is hundreds or even thousands of times higher than the reported figures. For obvious reasons, the survey didn’t include deaths, but it’s hard to see how deaths would be much less under-reported than these adverse events.
These values, while extremely high, are generally consistent with other data. The Pfizer booster trial found enlarged lymph nodes in 5% of recipients, compared to the survey’s 4.2%. The CDC V-Safe survey found that 0.9% of recipients of a Pfizer booster sought medical care, similar to the Israeli data. A whistleblower board member of a German insurance company revealed that his company’s data suggested around 4% of Germans had sought medical care following vaccination. A British survey found 20% of women reported menstrual changes after vaccination with AstraZeneca, compared to the survey’s 10% (with Pfizer).
This suggests that the number of deaths reported, like the number of injuries, is likely to be a fraction of the real number. Exactly what fraction is hard to say, but it’s difficult to see it being more than 10%, and possibly lower, meaning the real number of deaths may be ten times higher or more than the number reported.
This is not a small number (around 20,000 in the U.K. and 120,000 in America on current figures). So should we expect to see a clear signal for this in the overall mortality data, correlating with vaccine rollout? The difficulty with this is that overall mortality data are heavily confounded. For instance, Covid has been causing waves of elevated mortality, particularly in the winter, and these waves then lead to subsequent troughs of mortality displacement, owing to people who would have died in the following weeks dying early in the Covid wave. These patterns can conceal deaths associated with vaccination. In the U.K., the oldest and most frail received their first doses in December 2020 and January 2021, right in the middle of the Alpha wave. Non-Covid deaths were below average that winter, meaning Covid deaths were displacing deaths from other causes, in many cases as a secondary cause (‘with’ not ‘of’ Covid). How many vaccine-related deaths in the old and frail were recorded as Covid deaths? It’s worth bearing in mind that Norway stopped vaccinating the frail in January 2021 because its scientists noticed they were dying from vaccine adverse effects, but the U.K. gave no indication it would follow suit.
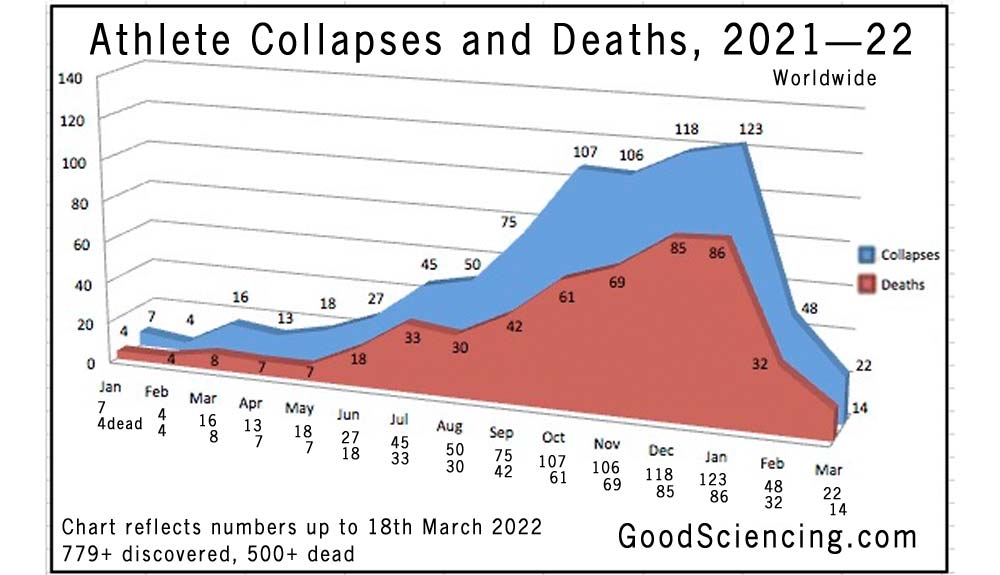
Following the winter, there was a period of low mortality due to mortality displacement, which can conceal a signal for vaccine-related deaths – plus vaccine deaths in the younger people then being vaccinated will not usually be in numbers that show up in overall mortality statistics, which are dominated by the old. Factors like these mean even a significant number of short-term vaccine injury deaths may not give a clear signal in excess mortality data. What can be said, however, is that the international excess mortality data in 2021 are certainly compatible with the levels of short-term vaccine injury that we are seeing reported. In addition, sometimes clearer signals do appear, as in Israel in spring 2021. An insurance company in Indiana, USA, also reported an alarmingly high number of deaths in working age people in 2021. In addition, among footballers and athletes, over 500 globally have so far been reported to have died following Covid vaccination (see below), mostly of heart attacks, apparently a considerable increase on previous years.
It is sometimes argued that any adverse effect of the vaccines will always (or almost always) be no worse than the symptoms and side-effects of having Covid. But this is a false binary, as vaccination does not prevent a person being infected, so the risks from vaccination are in addition to the risks from Covid. It is also not necessarily true. Scientists have noted that while the virus will usually remain confined largely to the respiratory tract, the vaccine, injected into muscle and moving from there into the blood, can cause spike proteins to be expressed throughout the body. Studies have shown that vaccine mRNA and spike protein persists in the body for months, whereas with infection the virus is cleared much more quickly and is not found so widely distributed. The vaccine mRNA and spike proteins, since they are not part of virus particles, behave differently, interacting and fusing with a wider variety of cells.
Of 15 autopsies conducted on vaccinated people, 14 showed “clear evidence of vaccine-induced autoimmune-like pathology in multiple organs”, with the heart and lungs affected in almost all cases. A study in mice found that the heart muscle absorbs the vaccine mRNA, causing it to produce spike protein, get attacked by the immune system and suffer inflammation and cell damage. Embalmers have reported strange clots in the vaccinated, while unusual large structures have been reported in the blood of the vaccinated.
The worry raised by these observations is not only that of short-term vaccine injury but also that the vaccines will, to quote Professor Sucharit Bhakdi, “give rise to lingering and slowly progressing inflammatory disease”. Supporting this, dose effects have been observed in some studies, suggesting problems may compound with additional doses.
In the second half of 2021, most of Western Europe and America saw a high number of non-Covid excess deaths (see below), due to a variety of causes, many cardiovascular, which remain unexplained. The pattern of deaths here mirrors that in the athletes in the graph above, rising from the summer into the autumn.
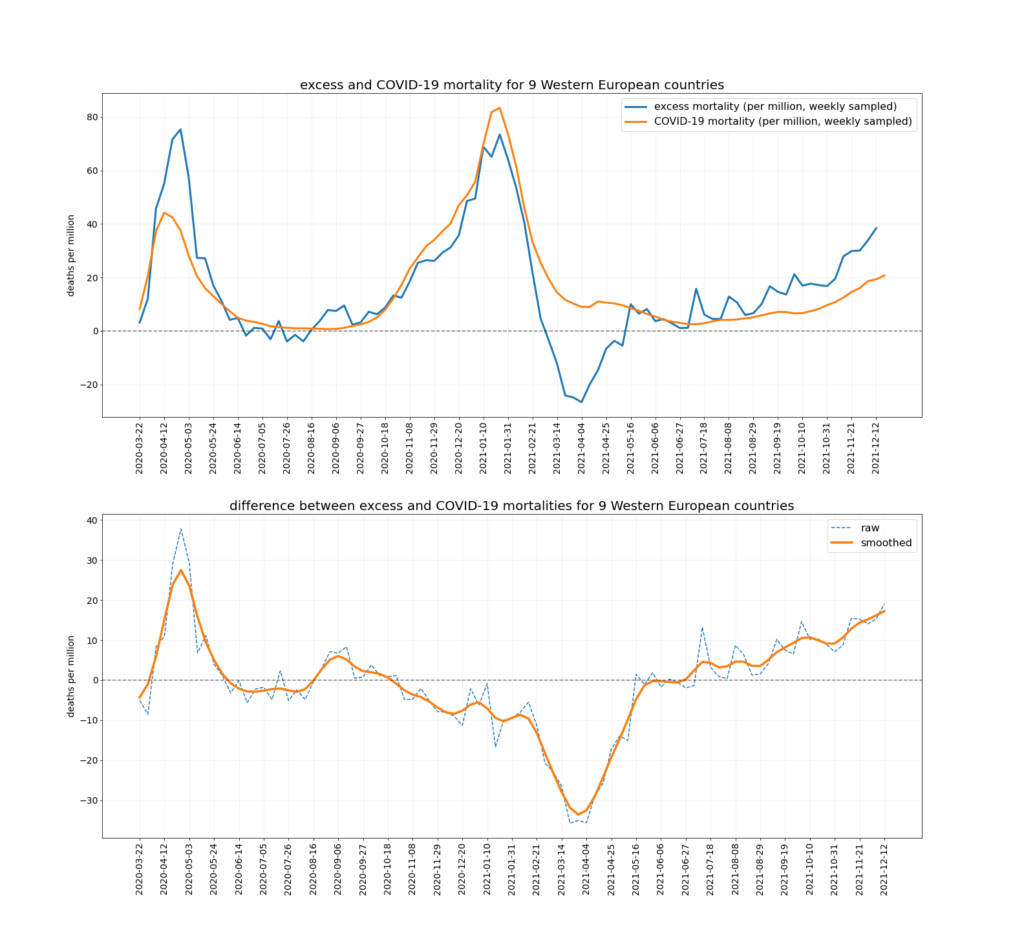
Why did this wave of non-Covid deaths only begin in the summer of 2021? Was it linked to second doses? Was it linked to the Delta wave with which it coincides (see graph above)? It appears to have ended with the Omicron wave, though recent excess deaths data may be confounded by the mildness of Omicron as a winter respiratory virus, as well as by mortality displacement. Did encountering the Delta Covid variant trigger further deterioration in the vaccinated, or was it unrelated to vaccines?
A further problem with the vaccines is that they cause temporary immune suppression in the days following the injection (an issue which Pfizer picked up in the trial, though didn’t reveal until recently), which can lead to increased risk of Covid infection particularly at times of high prevalence, adding fuel to an existing Covid wave and putting vaccinees at increased risk prior to any protection from the vaccines kicking in.
There’s a lot of smoke here rising from what appears to be a considerable amount of fire. While it’s not possible with the data publicly available to quantify precisely the number of people the vaccines are sending to an early grave, what data there are indicate the number is not small, and may be very large – in the tens of thousands in the U.K. Certainly more than enough to be ringing alarm bells that ought long ago to have triggered drug suspensions, urgent investigations, proper controlled studies and detailed reports. That very little of this appears to be happening – and that the authorities continue to repeat the mantra that the vaccines are safe as they roll them out to ever younger age groups – is disturbing, to say the least.











To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
On Tuesday Sir Christopher Chope, Conservative MP for Christchurch, told the House of Commons: ‘This Government’s approach seems to be to try to promote vaccine confidence by covering up the adverse consequences for some of having been vaccinated.’
https://www.conservativewoman.co.uk/betrayal-of-britain-mp-my-government-is-covering-up-covid-jab-injuries/
And he dismissed by the Speaker. Disgusting!
Perfectly reasonable from their point of view. Alternative views cannot be tolerated.
This Speaker is a massive disappointment – disgrace to the most basic principles of our ancient Parliament – he is in the pocket of the rule breaking Ruling Elites and has in effect colluded in he suppressing of a free Parliament and open debate.
Agreed. I had high hopes initially but the current Speaker is a very sorry excuse of a human being.
But I don’t think the previous Speaker would be any better on this subject.
probably why he got voted into the job – “safe pair of hands” “won’t rock boat” etc etc
I wonder how Bernard Weatherill or Betty Boothroyd would have handled the situation. Bernard enforced the rights of Parliament to be publicly told of government policies before telling the media before them. So Johnson would be in trouble. He was the last to uphold tradition by wearing a judges wig & since them standards have been a fast toboggan ride down hill
TPTB have made sure every Speaker is bent and does not allow anyone to “speak” against their shared interests. Makes me wonder what former Essex MP Amess did.
Pardon my ignorance but TPTB?
The Powers That Be.
His callous disregard for the victims really shocked me, even from a government we already know holds us in utter contempt. There was even a hint of amusement from this appalling man. Do they really think we’ll forget what they’ve done?
I’ve emailed him at chopec@parliament.uk to express support. He’s probably feeling pretty lonely right now.
I emailed him a while back thanking him for his support of us vaccine injured and he replied bless him!
likewise.
im with you.. i emailed him last night, to show my support.. bet his life is hell at the moment.. everyone should email their support.. show him how much he is appreciated.. lets out number the trolls..
I did yesterday.
One decent MP- a lone hero surrounded by……what would you call the rest?Are there any words adequate?
I could think of a few but I’d probably get banned from here and if that happened then it would be insanity central for me
I’m certainly not a Tory and, in fact, abhor almost all MPs. However, I have e-mailed in support of Sir Christopher Chope as he has, albeit a little belatedly, shown moral fortitude and backbone lacking among his peers who are nothing but WEF sycophants.
The terms thrown at Christopher Chope include “extremist”, “misinformation”, “anti-science”, “conspiracy theory”, “ridiculous”, and “discredited” – and apparently his “comment” “doesn’t justify a comment”.
That last one is from Martin McKee of “the independent SAGE group”, a “man” who, it is safe to say, has been close to Big Pharma for decades, because otherwise he wouldn’t be a “professor of European public health” at the notorious “London $chool of Hygiene and Tropical Medicine”.
McKee seems to have a small vocabulary, to judge from how he uses “justify” to mean “merit” or “deserve”. He sounds like the headmaster of a dump school, or some c*** from a local council.
He also seems to spend a lot of his time on stupid websites, or at least to be habituated to thinking in terms of posts and comments to posts, because he calls Christopher Chope’s speech in the House of Commons a “comment”, upon which apparently (who knew?) there is a question as to whether McKee himself might or might not “comment”. Personally I couldn’t care less whether McKee responds or not, nor even whether he practises in front of a mirror. But never mind “F*rtin’ Martin”.
Christopher Chope’s words were in his speech as an elected representative, in support of a motion for leave to introduce proposed legislation (a “bill”), which is one of the things that elected representatives are sent to the national assembly to do – along with, if they are not members of the government, holding the administration to account. And, on extremely rare occasions, one of these characters actually speaks sound words, as Chope did.
Go back to your house, Martin McKee, or to some publicly-funded desk somewhere. Read an article about “speaking truth to power” and polish your view of yourself as an “intellectual”, you fascist creep of a Heil Hitler boy.
Other MPs who’ve impressed me include Marcus Fysh. He was derided as a conspiracy theorist, as I assume were Steve Baker and Desmond Swayne.
Swayne let the side down a bit, just like the Queen telling us all to ‘get the jab’. Major fuck up.
https://www.youtube.com/watch?v=ZZf5iBWQlWw
He was talking to an almost empty room, once he brought the subject of vaccines up, two people walked out. They looked like they were almost trying to escape. Shameful.
Shows us what we are up against.
There is no place for being in denial now. That is a luxury we can no longer afford.
What we are up against doesn’t look pretty but we have to face up to it and start working out what to do to try to fight back against it.
I’m in – I’m sick to death of my near death experience being belittled and dismissed as collateral damage by the powers that be. See this poor lady – this is exactly what happened to me but I luckily didn’t have a clot in my head so survived https://mol.im/a/10627157
As with the Australian MP, video featured on this site yesterday. These people have an OBLIGATION to listen to alternative views, even if they contradict their own personal ones. They forget (if they ever knew) that they’re in that place to SERVE and work for us, not to throw tantrums because they find other’s views unacceptable, for their own reasons.
Only 1 MP speaks up out of several hundred and they will know what is going on. It’s absolutely disgusting. The only thing that will save the people is the people that much is clear. Sadly the majority seem to be brainwashed and lack common sense. At this point in time some due diligence for yourself and others you know who are incapable is likely to save many lives.
If they were innocent as to what’s going on, they’d have turned up and stayed to listen to him. It shows that they know full well that all is not as it should be. If even a few stayed to listen, we’d know that they were willing to hear all sides, and relay it to their constituents. The fact that they don’t makes them culpable and wish to keep us in the dark for as long as possible.
Let’s all write to our MPs and ask WHY they didn’t turn up to hear him out.
There is no confirmation but yet another super fit young Gaelic footballer in Ireland has died suddenly.
No idea how many have he had but, we should look at Matt Letiseur(?) who is up to speed on athletes deaths.
Matt Le Tissier
One of the many silenced voices that is now posting to gettr regularly.
I will have to look out for him. One commentator I follow is Calvin Robinson.
Star and hero (Saints fan, so I’m biased, but still. . . )
Chris no need to apologise. He was an outstanding player and now even a bigger hero.
RFK Jr. Discusses Fauci, Vaccines and Big Pharma’s Power
https://articles.mercola.com/sites/articles/archive/2022/04/02/rfk-on-fauci-vaccines-big-pharma.aspx
Analysis by Dr. Joseph Mercola
Stand for freedom with our Yellow Boards
Tuesday 5th April 2022 4pm to 5pm
Yellow Boards By the Road
A3095 Maidenhead Road/B3034 Forest Road
Three Legged Cross, Forest Rd, Warfield,
Bracknell RG42 6AE
Thursday 7th April 5.30pm to 6.30pm
Yellow Boards By the Road
The Meadows, (A321) Marshall Rd,
College Town,
Camberley GU47 0FD
Stand in the Park Sundays from 10am – make friends & keep sane
Wokingham Howard Palmer Gardens
(Cockpit Path car park free on Sunday)
Sturges Rd RG40 2HD
Bracknell
South Hill Park, Rear Lawn, RG12 7PA
Telegram http://t.me/astandintheparkbracknell
The truth is already out there for those who can be bothered to find it!
Having read RFK jnr’s book I fail to understand why Fauci isn’t already behind bars. Perhaps he will need protective custody soon.
That fact that he is not sueing RFK jnr already speaks volumes.
This is just one small example of the activist takeover of government, and the disconnect between them and the truth.
Activists and single-issue fanatics believe that their ideas are right, and when they start to fail they prefer to reject reality rather than give up their beliefs.
So we get politicians lying to themselves and the rest of us about the need for wind power, the advantages of regime change, the usefulness of vaccines and the lack of difference between men and women….
If it walks like a cult, talks like a cult, with rules like a cult, then it’s most probably a cult
I’m increasingly of this view myself. Difficult to accept as it is well presented. Parliamentary debates, pomp and ceremony; people on TV all saying the same thing. But the decisions, from net zero to injecting children with these dangerous drugs, speak for themselves.
We have to assume the government has access to much better data than us. Yet day after day this website publishes pieces by scientists and others providing damning evidence and inconvenient facts that challenge the narrative. Why proceed?
The answer increasingly is they behave like a cult. Our challenges, including those based on observable facts, act to reinforce the cult’s belief systems. When ordinary people claim the climate announcements seem extreme because the weather isn’t changing, the cult takes this as proof of their superiority; climate isn’t weather, you don’t understand the longterm trends signaled within the data; we see further than you and every appeal to observation demonstrates our superior ability to grasp the deep structures that elude you.
That statue of David Livingstone represents the horrors of our evil past even though Livingstone was an abolitionist. Your pathetic attempts to use the facts of his actual life – campaigning to end exploitation of Africans – misses the point. He was successful because the whole thing was based on exploitation. All of it must be condemned. Abolishing even the abolitionists themselves demonstrates a deeper, better grasp of how much we must atone.
Reason has failed. Cults cannot be reformed only stopped, preferably eradicated.
Sadly, almost no-one cares about finding out.
The people ‘in charge’ don’t care as they would then be wholly culpable in misleading the public and causing the deaths and harms.
The people who took them also don’t seem to care. Why I don’t know, but given that they have all gone on to swallow the hastily invented lie that these vaccines were never meant to stop you getting ‘Covid’, merely mitigate the symptoms, I feel there is no hope for them,
Also fair play to Will Jones for continuing to analyse these stats as if the vaccines weren’t total junk.
The apparent lack of interest from the jabbed is entirely understandable. It’s too late now. They’ve taken it. To question it now would be to admit their mistake and people are very reluctant to do admit even to themselves that they screwed up big time. Especially when there is little remedy.
Where you really see how they feel about it is in the declining proportion of jabbed with each additional dose.
Indeed. My cousin in the US simply will not discuss it. Previously she would have been, well, militant (and rightly so!) about bodily autonomy, freedom of choice, so I can only guess that she’s sh*t scared.
I too have a relative like that. It is difficult to say the least.
Or gene mutated
Correct. Two acquaintances of mine have had serious adverse effect:
Ditto…my brother with liver cancer and a good friend with pancreas problems. Hard to prove it was definitely the vaccines but somehow I just have a strong feeling it was.
Though, some people have ‘strong feelings’ that masks of any type are effective… I live with one. Drives me nuts!
Challenge them to go in the bathroom with their mask on after you have dropped one.
Explain that the particles of poo that they can smell are massive compared to the claimed virus, if the mask can’t stop the aerosolised poo going up their nose how does it stop virus?
:-))))))))))))))))))))
Yes indeed, a mask stops the virus as much as pants stops farts.
If the person in question has been jabbed be careful with this.
Their immune systems may have been so compromised, that a really evil smelling one might push them over the edge.
But but —- early on one of the cast iron symptoms of Wu Flu was a lack of smell.
I’ve had the coof. It’s true that one of its benefits is the inability to smell farts, or indeed anything much.
Other benefits were a week at home, working half speed, and an excuse to loaf about a lot, not having to speak with anyone. Lovely.
Yup, I know one with thyroid disfynction, one with gangrene-like symptoms, one stroke and one heart attack (fatal). Ages 58-70, no way of proving any jab-related (though may pass Bradford-Hill), so probably all councidences.
Coincidences. . .
I hear cases like this nearly every day now from a limited range of friends and acquaintances!
Same story every time.
Good point. Actions speak louder than words. I have family members who succumbed. They clearly regret it but cannot quite bring themselves to say so. It is therefore avoided. Inevitably each positive take on it is grasped to salve their conscience. The mental goal is to at least assume it is harmless, it does nothing. The adverse events challenge that view so must be rejected or at least ignored.
Your comment also very comprehensively describes the underlying reason for politicians , medics and the rest of “cultists” to be so against any admission of fault, error etc. They just can’t face doing it, perhaps because they themselves (or some of them) are shot full of the “vaccine”, but also because of the losses any backing down would incur; employment, status, earnings, kudos etc.
If they are in government they are bound by contract to defend and indemnify the drug suppliers
Yes – I can understand that – they have taken it. But surely they could use the information now coming out and analyse it to inform their decision about whether they should have any more of the jabs which might have harmed them. Would that not be the common sense and logical thing to to?
Went to a rally for the freedom friendly minor parties today (I’ve joined the Liberal Democrats) and met a fellow vax-resister who is still in employment. His hold on his job is tenuous, but a significant number in his workplace have had two or three shots and are not willing to take any more. Some are suffering adverse events. Management is ‘flexible’ on the time between shots, meaning that they’re stretching the three months out to six for some workers. They can’t do much else; staff shortages are biting hard and hitting the bottom line. Probably praying that McClown does a Daniel Andrews and meets an unfriendly flight of stairs.
They tried to do a Dan Andrews in Scotland with the emergency Bill that can be brought into action on a whim. Fortunately it was rejected.
So Australians are now officially more stupid than both the Kiwis and the Scots. That’s a great start to my Sunday.
It is not that they don’t care – it is that they are taking orders ‘from above’ on a very specific and detailed agenda .
They are no longer serving the interests of the people of this country in any respect- if they ever did!
In fact they now see the people themselves as the “problem”.
The next front after Medical, food and energy is Financial -see the Agenda of the World Government Summit in Abu Dhabi, March 30th 2022, for their advanced plans to crash the Global economy and introduce the digital currency based on blockchain any time soon.
The attack on Russia’s economy is just the start- the real target is the Western Financial System – and taking control of our money and eveything we buy!
https://m.youtube.com/shorts/bkNh4MNw_MI
Digital currency
And it won’t stop there.
what do you think they tell you (or do with you) if you click on the “learn more” button?
It is now 3 April 2022 – what happened at the WGS then?
You mean apart from at least one person dying during the trials?
The pfizer trial in the US showed 21 all causes deaths in the treatment arm vs 15 in the control arm. plus piss poor efficacy. These jabs should never have been approved, even for emergency use, cus there was no emergency.
Irrespective of whether there was an “emergency” they shouldn’t have been approved for emergency use because they were not working and there were extremely concerning harmful effects. The (lack of) benefit, could not justify even the known harm, let alone the long term and therefore unknown harm.
We need to get beyond the ‘injections’ and consider the bigger picture and as they do not stop Covid transmission what they are really for – ever heard of the Great Reset?
Well, it is currently underway and covid and the vaccines were very much part of it!
Heard of the US multiple biowarfare labs in the Ukraine ? Ever heard of Peter Daszak?
Fully documented exposure is out there! (Not seen on the BBC)
And also there were other treatments available, That may be part of their downfall. We can all live in hope.
Hence the need for the control group to be dispensed with.
3 kids with adverse vaccine reactions through breastfeeding out of 133! Criminal!
Again, Dame Sarah thingy thinks they were too cautious and didn’t get enough jabs into enough pregnant women
The “trials” were a fraud.
Trials shcmials old boy – Dame Sarah thingy who created the AZ vaxx thinks future vaccines should be produced within 100 days. Trials are so last century and as for safety?
It will never be known how many people died, or were injured, from the ‘Covid vaccines’.
The data is almost impossible to interpret.
And the Government and their henchmen will only claim that injuries & deaths were from ‘Covid’ itself. And that they had ‘no choice’ but to introduce the ‘vaccines’ to try and save as many lives as possible.
Neil Ferguson himself declared that everyone would die, including Mrs Miggins’ cat. When you add on the story that ‘Covid’ is a very mysterious disease, unlike no other seen before, and that it could be a ‘bioweapon’ made in a Secret Laboratory in China, then 90% of the nation got frightened out of their skins and then the Government knew they could strike and remove freedoms and put their hands deep into the pockets of the public.
My basic outlook is that no dead bodies everywhere = no pandemic. No dead bodies everywhere = the ‘vaccines’ can’t be that deadly.
We know lots of people who have had 3 jabs (Pfizer/Moderna/Astra-Zeneca/combinations) and we know of none who have been injured or have died.
Waiting for them to die of ‘ADE’ or ‘VAIDS’ from the ‘vaccines’ is a bit like waiting for Reiner Fuellmich’s lawyers to come and lock up all the baddies.
We have to decide for ourselves where the boundary of reality ends and that of fantasy begins. My bottom line is that there is no need at all to take these ‘vaccines’ as there has not been no ‘pandemic’ in the first place. It’s all been one gigantic con. Which continues to this day with the 4th & 5th jabs being ‘rolled out’ during 2022, and an even younger age group, the 5-11 year olds, now being roped into the clutches of those who profit from this scam.
Two years of this farce gone by and the UK Health ‘Security’ Agency (sinister name) wants it to continue for at least another two years.
This is exactly my view, EF.
But I would add that, given a choice between death at the hands of a flu virus in my declining years, and death on a football pitch from myocarditis as a young man with a life ahead of me, I would prefer the former.
Ivermectin could have saved many thousands of lives as it has done in India – they banned its use in the UK.
( See devastating interview with Dr Tess Laurie and Andrew Hill for the shocking truth!)
Yes. We are in a war. That is one of the enemy’s strengths, they dictate the terms. The antidote is to remove that power from them. We must decide our own terms for medical care.
Indeed, that’s a shocker – and very revealing.
As long as people are offered information so they can make an informed choice, and as long as no one is coerced, then it’s all fine. That is where the problem lies.
I personally know no one who has died of OR with covid. I know one person who has been left with heart problems after infection (though they had had 3 jabs, make of it what you will) and one person who has still, 1.5 yrs after a scary respiratory infection, got lung damage and exhaustion.
I also know two people in their 50s with no prior history of heart problems who had heart attacks, a student who was off school for nearly 3 weeks after her second jab and another who had a whole body hive-like response.
As long as I’m allowed to choose, I shall continue to choose to try to avoid getting ill, rather than risk the injection. My concern is whether I shall be forced.
It’s NOT “all fine.” These injections should be removed immediately. They should never have been released.
If they had not been released then the public would not have had to make informed decisions. They would not have been responsible for making their own assessments.
The government knows these things are dangerous gunk and yet they persist in promoting them.
The government is guilty of mass murder at least. Every MP not speaking out is equally guilty. Every shill “scientist” is equally guilty. So too complicit medics and civil servants. The charge sheet is a long one.
Never forget, never forgive.
I know I know. I DO know. But right now RIGHT NOW I just want them to NOT force it on people, on me, on MY CHILD. Aside from my parents and my child, EVERYONE I KNOW and LOVE has been JABBED and the past is the past, I want the future to not hold forced medical procedures of any kind. It is too late for them, for those who chose with inadequate information because they were scared and lied to. The Jabs WERE released, the damage is DONE, what should have happened is NO USE TO ME RIGHT NOW.
If the information is now freely available, then going forward it will be perfectly fine if people see and understand the risks and do it anyway, because my world has shrunk to a tiny tiny group of people I can protect and if they go to coercion then I can’t protect them so don’t even think your ‘never forgive’ thing is more than a slogan. I will be thrilled when they are arrested, tried, found guilty and punished but until that happy day arrives, I will continue to try to protect my own, which I can’t do if they take away choices.
I understand fully where you are coming from – I too am trying desperately, like the little boy with his finger in the dyke, to protect the people I love, who unfortunately are damned hard to protect as they seem ever more determined to take the bloody jabs the more I try to tell them that they are harmful. They just cannot get their heads around the fact that their government might be actively trying to harm them. (That is what happens if you are addicted to the BBC ‘News’)
Unfortunately, I think the days of bodily autonomy are over, unless we put our heels in the sand and fight back against that. I see a scenario now (after the pandemic summit which TCW reported on yesterday) where this is just the beginning, and there will be a trolley load of even more unsafe jabs for any and every ailment the government decides everyone has to have whether they want them or not, with safety no longer a consideration – just mass jabbing.
Whether we like to accept it or not, this is what we now face, and this is what I mean when I say above that the time for denial is over and we need to oppose what is coming.
1) Fraud (on a global scale)
2) Psychological abuse (on a glibal scale)
3) Mass extortion
4) Mass murder
These people are criminals on an historic scale.
I agree entirely – you beat me to the ‘No, its not all fine’ line, and I would take it a step further, as I would say that as it is ALL manufactured manipulation, the “pandemic” the Net Zero panic, the Ukraine ‘war’ which Biden has provoked (and now see Pakistan for the next arena of instability) the supply chain chaos, the looming energy and food shortage crises, NONE of it is fine.
And we don’t even KNOW what the full damage from the jabs is going to be yet – I personally DO know people harmed by the jabs, the jabs they continue to sign up to take despite not knowing what is in them.
It is not “all fine” by any means!
I would stick something sharp in their neck!
Last night I watched the first part of Hotel Terminus, the Max Ophuls documentary about Nazi Klaus Barbie. As you’d expect, a lot of elderly Germans hiding their faces from the camera and whining ‘It was forty years ago! Who cares now?’
Easy to see that history repeating itself with The Dreaded C.
I watched The Stanford Prison Experiment last night. Yeah, pretty disturbing and enlightening in equal measure.
Was it you that mentioned it, EF?
Hotel Terminus next on ze leest.
One by One sounds good but not seen it.
I started to watch it but wasn’t impressed. The acting was wooden and the film boring.
They are still being injured and dying as we write -they are still injecting our children and threatening mandated jabs for life( however long that willl last)!
https://www.birpublications.org/doi/10.1259/bjrcr.20210139
Bilateral adrenal haemorrhage with renal infarction after ChAdOx1 nCoV-19 AstraZeneca vaccination
Friend of mine. Blood clots in her kidneys, lungs, and adrenal glands, the latter of which were destroyed and she now has permanent health problems because of the AZ vaccine. She’s very lucky not to have died.
A neighbour recently suffered from serious haemorrhaging, and had been due to fly out of the country the following day. Had he been on a plane at the time, it’s guaranteed that he’d have died.
The trials didn’t show them to be safe. The trials were poorly conducted and over too short a time; results were manipulated; inconvenient data was ignored or suppressed.
And there is still no medium to long-term safety data.
This is the largest human medical experiment in history …. and the vast majority of trusting sheeple didn’t know they were participating in it.
This is not an experiment. An experiment would imply that they want to learn something from it and would change or adapt the experiment depending on results. They are getting the result they want and are therefore continuing with the campaign. They are all earning a fortune, increasing their own power and removing democracy. Whether long term health damage – increase in frequency and malignancy of cancers, reduction of fertility and increase in other illnesses – are part of this will only show up in time to come.
A member of my family participates regularly in clinical trials (the proper ones, with scientific control, placebo arms, etc). She is on one now.
The trial company couldn’t care less about whether their test subjects have been “jabbed” or not. Everyone should find that to be a very interesting fact. They enquire about whether they have had the “COVID vaccine”, but only because there are rules about how much time must be left after many medical procedures before a person can be admitted to a trial.
Of the 12 currently participating in the trial, 4 have not been “jabbed” at all (including my family member) and 2 said they didn’t want to be, but felt coerced, but now won’t be having any more.
The other 6 didn’t want to talk about it.
And bear in mind that this population of 12 is one which is NOT squeamish about needles, medical industry, pharma etc.
Thank you. That is interesting intelligence.
Pleasure. Kinda.
It is an eye opener and something I hadn’t thought of until now, but considering the number of people globally, with even just a single jab, it means that the bulk of future drug testing will be done in jabbed people.
Which means that medicines developed from this point onwards will have very little idea of what they will do to someone who is never jabbed.
It was an experiment & the unsuspecting, lied to & manipulated public were the test subjects. There is a great deal of variability within batches due to how the product is manufactured & the vials are filled. There is also a rapid degrading of the product over time. In Europe Pfizer manufacture in Belgium, higher rates of reporting of adverse events there than elsewhere. Coincidence? Accident? Consistency of product is not achieved at all, leading to some vials being more toxic than others & the birth of http://www.howbadismybatch.com
For a further explanation of this variability, how it occurs & the methodology used to determine this fraud can be viewed on this presentation here: Sasha and Craig presentation 220308 (rumble.com)
The “experiment” is by no means over!
Quiet before the next even bigger storm!
In my ‘umble opinon I reckon that in 2025/2026 we will see a massive increase in deaths of the jabbed.
These will be medium term side effects. Just based on intuition with all of the current adverse events noted,
These gunk injections are designed to kill. Depopulation is the aim.
Unproven but it seems likely, yes.
McCullough, Bhakdi, Malone et al have changed their minds and agree with Yeadon that the drug pushers seem to be malign, not just trying to make some $$.
Just say no to drugs …
And this is only the start of it.
Good point – and now that they have got away with it they plan to continue it, with worse coming down the line.
Also, imagine Ford releasing a new car but withholding performance test results for 75 years.
Not just performance test results, but braking and steering efficiency and fuel tank leakage reports.
The withholding of any results always shows there is something to hide. You never withhold anything that shows how good you are. Why would you?
That is incidental. An experiment’s motivation is to discover something. The driver behind the covid injection project is profit, with totalitarianism a useful co-pilot.
That the results were manipulated & the true data hidden means that fraud was committed. No pharma is exempt from liability for fraud.
Most likely Edward Dowd will try to establish this – as at least one pillar of his investigation.
Dowd thinks that the scandal will soon be breaking into the mainstream:
https://www.financialsense.com/podcast/20225/edward-dowd-greatest-scandal-our-times-about-break
Listen from 36:45.
And yet if you try to explain that to them they still either don’t understand or believe you.
I have read the reports of the Pfizer whistleblower describing the way the trials were conducted and the myriad ways in which they erred.
I would imagine there are more clinically run school canteens than the Pfizer trials.
Why is it that the structures that where in place to keep us safe have been overridden?
this needs fully investigating and exposing, yet it seems that everyone who could is too scared to raise their hands and expose this travesty, from scientists to doctors to medics to the journalists all are too scared to seriously challenge the consensus propaganda that has been indoctrinated into everyone over the last 2 years.
im just sorry I had 2 AZ jabs, I was feeling amazing before my 1st jab and I’ve felt crap ever since. I should have known better.
Well, as someone who doesn’t give a damn about what you choose to do with your own body, here is a hearty handshake for being able to talk so candidly about all this!
Sarah Gilbert Barbie dolls may still be available for fans of Astra Zeneca!
What a joke this woman is. Uses a vector that is linked with blood clots and thrombocytopenia to express a protein that does much the same
Agreed, I kinda want to meet her so I can ask her 1) why she thought this might be a good idea 2) does she have any guilt?
I’d like to ask her has she been jabbed with her own gunk or that of a competitor? (prob only saline – but still)
Who will “investigate it? Johnson? Javid, Hancock, Whitty, Raine? the fearless London Met Police? Judge Whitewash?
Laugh out loud!
You might want to look at Option 4 on this page:
https://covid19criticalcare.com/covid-19-protocols/i-recover-protocol/
Brilliant post and suggestion – you beat me to it.
sorry to hear that.
And me
More news continues to trickle out about Shane Warne’s untimely death in Thailand (which, in the official cover-story, is from ‘natural causes’ of heart attack brought on by lifestyle factors) suggesting that the deadly vaxx can’t be written off as the initiating cause of death.
Blood clots in the lung manifest symptomatically as chest pains and excessive sweating and the Thai Police autopsy report on Warne notes that between his 14th January booster (making him triple-jabbed, which he boasted about on Twitter) and his departure for Thailand, he consulted his Australian doctor for precisely these symptoms. Lung blood clots also cause coughing up of blood and the Thai Police report also noted the presence of blood on Warne’s pillow, sheet, carpet and towels. Heart attacks do not cause blood discharge from the lungs. Everything is suggestive of a pulmonary embolism (blood clot in lung) taking Warne’s life.
The Defense Medical Epidemiological Database (DMED), operated by the DoD in the US (which logs all medical events, including vaccine adverse events, amongst serving US military, as determined by DoD doctors), records a three-to-four-fold increase in PE amongst service personnel in 2021 following the compulsory Covid vaxx requirement in the US military. PE was running at fewer that 1,000 PE events per year until the vaxx year when it ballooned to 3,500 cases (https://stevekirsch.substack.com/p/this-medical-data-from-the-us-dod?s=r).
Yet, amongst all the eulogies and state funerals for Warne (and that ‘ball of the century’ which got Gatting will truly never be seen again) there was no hint that his jab-status had anything to do with his death. The authorities don’t want to know because they have a narrative of ‘safe and effective’ to preserve at all costs, even at the cost of dead legendary leg-spinners and countless lesser mortals.
With ongoing symptoms of possible blood clots the last thing he should’ve done was fly.
That’s interesting Phil – didn’t know that about Shane W’ and it does change the picture for me such that I’m now more open minded to the idea that Warne’s death is indeed vaccine related. I’ve been sceptical about that hitherto for the following reasons . . .
Whilst I’m completely on board with Will’s article and the comments by members btl, I’m wary of jumping on every heart attack death and attributing it to the vaccines. I had a heart attack myself back in 2011 aged 50 and the medics struggled to attribute any reason for it. I’m not overweight, eat healthily and don’t smoke etc. The point being that plenty of people do (sadly) have fatal heart attacks for reasons that have nothing to do with the vaccines. Distinguishing between those that are vaccine related from those that aren’t is the devil’s own job. DS members will always be a tempted to attribute a death to the vaccines just as, conversely, the mainstream medics will stick to their line of there being no correlation.
Who any longer believes anything “the authorities” say about the sudden death of so many sport’s personalities?
Surely no-one with any discernible brain activity?
The crushing of warning voices on the “vaccines” is the result of the fear of public rage when people discover that they have been cruelly duped.
How many more will learn, as we have here, that “the authorities” are outrageous liars who can’t be trusted; even when it comes to life-and-death issues such as public health?
So far, many have gone along because they believe that their governments must know the right thing to do on something so vital, and would not deliberately withhold or distort information about it.
Our numbers can only grow.
Here’s hoping AE.
Quite a disappointing article. How many people have died from the vaccines? Answer: no one knows. But we’ve all known that.
I think it is very misleading to show charts of the absolute number of deaths after COVID vaccines. We all know the number of COVID vaccine recipients is bigger than any other vaccine. So we need to see the *rate*, not the absolute number.
The questions I’d like answers to are
Is it possible to differentiate a COVID vaccine-induced event from COVID itself, and if so, how in particular?
Can scientists differentiate COVID vaccine spike protiens from SARS-CoV-2 spike protiens?
I have heard Dr Peter McCollough say that for any other medicine/vaccine, once 50 deaths are reported the product is pulled off the market. Does he mean 50 deaths after taking the medicine, or 50 deaths that have been attributed to the medicine? And is this 50 deaths limit written in an official health document protocol anywhere? If so, it would be great to see it.
So I had an adverse reaction to AZ and ended up in hospital. I hadn’t had covid so they couldn’t blame that. I had had the AZ two weeks before. It was one of the first questions the doctor asked me was when he showed my blood screen and told me it was the vax. I spent 10 horrible frightening days in hospital wondering if I was ever going to get better. The hospitals know and never said it was anything but. I guess you don’t have to be Sherlock Holmes to work out if someone who has got to nearly 50 without any form of weird clotting shows up at A&E with a bunch of other people around the country within a couple of weeks of an experimental jab then that is your cause. Plus there is a test for VITT
He actually told you it was the vax!
One in a million then! Did he fill in the Yellow Card?
Yes he did. Couldn’t really deny it – four others in the hospital at the same time so slightly more than one in a million. One covid patients in the whole trust of 4 hospitals and not in icu. The day I went in was the day the AZ was pulled for the under 40s. Yes think he did fill out the yellow card.
Certain articles with charts that I’ve seen do take into account the number of vaccines given, because without that it is meaningless, so it’s quite easy to do this as flu vaccines have been given to a large proportion of the population and over many years. The covid ones do not compare favourably.
In the US they use the Bradford Hill criteria to judge whether an event is likely to be associated with having been vaccinated. There are 10 criteria (which you can look up, as the system is used by the WHO, I believe); for a likely causation 5 of these criteria need to be met. Dr Jessica Rose did a substack article on this towards the end of last year.
Why are we even discussing this ?
In the previous ‘normal’ moral and ethical, medical world, with honest Medical Protection Institutions, if there had been just a couple pf vaccine deaths the experimental product would have been withdrawn – that tells us all we need to know about the evil intentions behind this project, saturated with lies!
Why would you subvert and stand down Organisations designed to protect the public unless you intended that the public should have no protection just as the vaccines had no meaningful trials and the Pharma had protection from legal action against them?
Money of course ….but why else?
Think dark and you cannot go wrong!
In the previous ‘normal’ moral and ethical, medical world, with honest Medical Protection Institutions, if there had been just a couple pf vaccine deaths the experimental product would have been withdrawn
This is one of the most important points to stress. Plenty of people will shrug their shoulders about adverse events, because they have no idea of standard practice with regard to such matters.
They need to understand that their governments have been driving through red lights, and that they and their families and friends are or could be amongst the casualties.
Think dark and you cannot go wrong!
Most of us are afraid of the dark. Many really don’t want to go there. We will need to offer genuine hope that there’s light; that there’s at least the possibility of something better than this.
I’m not talking of offering utopian ideals, but of sets of standards that cannot be crossed. Those standards should include guidelines concerning free and informed consent; what constitutes the violation of this; and precisely how it is to be protected.
If we speak about returning to what was normal, we’ll have to consider how ill-protected that normality actually was.
“They need to understand that their governments have been driving through red lights, and that they and their families and friends are or could be amongst the casualties.”
Brilliant way of expressing it AE.
I know I am repeating myself but the reason for the injections is depopulation.
Yep: nothing else makes any sense.
Yes – especially when you consider the TCW reports of the pandemic summit or whatever it was where the likes of Sarah Gilbert think that jabs should be developed within 100 days and to hell with concerns about safety and efficacy.
We need autopsies.
In the US fluvaccine is given almost 200 million doses per year.Very relevant to compare with VAERS report for flu and covid vaccines
https://www.frontiersin.org/articles/10.3389/fpubh.2021.756633/full#T1
“Quite a disappointing article. How many people have died from the vaccines? Answer: no one knows.”
Really? No one knows? I think you are missing 2 things:
And my last comment on what you said above, however many people have died after being jabbed with these “vaccines” – they are TOO MANY
From having never known anyone personally hospitalised with serious heart problems, I knew 3 people with life threatening heart conditions in the first 6 months of 2021. Two in their fifties, one a fit man of 70+. One person with (thankfully temporary) kidney failure which the hospital admitted was vaccine-induced.
I foolishly had one AZ injection, have not been right since with a bout of more worrying heart palpitations in 2021. Now much better (no thanks to the NHS, which was not interested). My 81 year old mother had 3 Pfizer vaccines the last of which nearly killed her. The NHS 111 gp she saw recently after a second chest infection (she believes due to the weakening effect of the vaccine) said that she has seen a lot of people having difficulties after the booster.
Which makes me wonder – they are doing the 4th injection after the winter, at a time of year when deaths often reduce, will the effects be a bit more obvious thus time, with the “pandemic” on the wane?
My parents are the same. Similar age. My mother had robust health her whole life. Literally never been in hospital except to give birth. Then she contracted pneumonia out of nowhere after her fourth jab. Never been right since.
It is all around us – everyone has the same experiences – this tells us the real numbers – and they are going up.
And come autumn and next winter it will I fear be worse.
Quite obviously there is and never has been a satisfactory system of recording “vaccine damage/death cases.
The longer it takes for adverse effects to manifest themselves the harder it becomes. The adverse effects simply get lost in the general noise of disease/death. Just look at how long it took to nail Vioxx as being responsible for anything between 50,000 – half a million premature heart related deaths in the USA – and that was without any MSM/bigpharma campaign to whitewash it.
We are stuck with the system we have. All we can really do is to publicise it – and amongst the medics as well.
But, in addition to that, real scientists and those of any influence must show any and all causal links between adverse events and the jabs.
There are known bio molecular mechanisms, courtesy of GVB., which prove how these events take place ie how the erstwhile properly functioning immune system is disrupted :-
https://uploads-ssl.webflow.com/616004c52e87ed08692f5692/6244c3b09ad5701f3ec17765_GVB_s%2Banalysis%2Bof%2BC-19%2Bevolutionary%2Bdynamics.pdf
This facilitates the ability of the virus to mutate.
In addition, parts of the immune system have to be trashed in order to enable the mrna to enter and infect your cells – leading to a plethora of future auto immune disease.
But, never mind, the jabs are useless and dangerous, so it is essential everyone is jabbed.
Oh, and they STILL encourage kids, now 2- 5 year olds, to persuade their parents to jab them.
Could we add, as a legal requirement, a proactive survey such as that outlined in the article?
Perhaps we should let governments know that such surveys must be mandatory.
Personally, I know no one who has had covid with anything other than mild cold symptoms. That number is quite large and includes someone aged 83 at the time. It also includes people in their 70s with various health issues including a coronary by pass. In contrast, three members of my close family have had adverse reactions to the vaccines. A super fit 38year old male (chest pains) late 60s female (stroke/speech symptoms, stroke ruled out by hospital) and male, late 60s, phlebitis. Although I am not of this view, I can understand why people want to put their heads in the sand… If they look and see, what can they do?
These are the kind of ‘testimonials’ and communities being censored on Twitter and of course Facebook by Zuckerberg and our own Clegg!
For the short term the Yellow Card system has its faults, but as regards the long term it is useless.
The Yellow Card system is there to provide an early warning of vaccines that are dangerous – it actually succeeded wonderfully well, but the authorities have chosen to ignore it!
But the MHRA don’t seem to be doing anything with the data, no follow up checks on people regarding adverse effects.
Yes, that was the point I made, ‘the authorities have chosen to ignore it!’.
Last chance!
https://togetherdeclaration.org/covid-19-public-enquiry-survey
There’s a link to the survey
Faulty link.
Yes, it should be ‘inquiry’ not ‘enquiry’ i.e. https://togetherdeclaration.org/covid-19-public-inquiry-survey/
Thank you for correcting my error. The more people who can contribute, the more, albeit slim, chance that justice will be done.
No probs: I imagine you Ctrl-C (or equivalent if you are an Apple user) copied the link, so maybe someone decided to change the spelling used!?
Cheers. Gave ’em a right kicking.
Yes do and encourage everyone else too. I filled out the one (which was very hidden) on compulsory jabs for NHS workers. Not sure if anyone can verify but sure I heard that 87% of people were against them following that consultation
Posted by someone else a couple of days ago, but I think this is worth watching to make people aware of what is actually happening. ‘Vaccination of 5-11 year old children’.
(2 minutes long advert for the Health Service Executive):
https://www.youtube.com/watch?v=1w5FZ-WxMnU
I found this very sinister. ‘We will look after you, just walk this way. Look we’re all friendly. Now, just put your valuables here for us to look after and step into these lovely hot showers…’ Okay, I made the last bit up, but that’s how it comes over to me.
How about “Too damned many, and a lot of people should face real consequences for this perversion of medical science”?
Agreed, but as we know the establishment and their spouses are a protected species to whom the normal societal norms, like the rule of law, democracy and fair treatment for everyone, do not apply.
All I know is that the vaxxed at my work are constantly ill. Sickness rates have gone from 0.5% to better than 3%, The jab seems to convert people into public sector workers.
I was reading a general forum the other day where people were saying that they didn’t understand why they kept getting ‘Covid’ (and some being very poorly) when they had been fully jabbed. The general answer seemed to be, after some discussion, that those who had been very ill would have, but for the vaccine, ended up on a ventilator, and the not so ill had had a lucky escape, but were saved from worse by the wonderful jabs. One person mildly questioned the actual efficacy of the jabs and was immediately shouted down and labelled ‘one of those anti vaxxers’. The total unquestioning faith in their received information that the vaccine is safe, it works and the more the better (many were bemoaning that only the over 75s were having a fourth jab, because they wanted one too) was quite frightening. However, this is the consensus among the majority, it seems to me. I have a friend who has faithfully believed and followed everything the government has said, and was extremely shocked when I sent her various links (like the Pfizer released documents). I may actually have turned her, but generally, I think we are fighting a losing battle.
Do you think they will dare give the Queen a fourth jab?
“Do you think they will care give the Queen a fourth jab?”
Only if they want to bump her off early.
I’d like them to give Charles 7 or 8 maybe.
Do you really believe she or any of TPTB have had the clot shot? At most they’ve had saline.
Look on the bright side … they might have exposed themselves to serious health issues by their choice of “news”, but clearly a huge number of people resisted the brainwashing news and took the right decision. Clearly good quality alternative information sources are now really having an impact.Yes, they might still only be informing a minority of people, but I doubt those who were misled into taking the jab will ever have quite the same faith in their former sources of “information”. That does suggest that those sources pushing the jab are on the way out, and the high quality information sources will do better and better in the future.
The Queen hasn’t had one jab! It’s naive to think that the elite inject this stuff into themselves.
Or perhaps she is being fed prophylactic ivermectin.
Is it true that the head of Pfizer hasn’t had it?
Bourla (?). He’s on record as saying he hasn’t had it. He didn’t want to jump the queue.
Decent of him.
Was the first one real though!
I have had a conversation today with a friend I’ve known for over 50years. She completely believes all that she has been told. Her fully jabbed daughter has had “covid” twice, once being really poorly, but “it would have been so much worse without”. I suggested that that was a bit like walking down the road with your fingers crossed and being pleased that it you stopped you being run over, but she wasn’t having it! She was totally shocked that I haven’t been jabbed. This followed her talking about “those dangerous people” and me saying “that’s me”! My “choices are misplaced”…
Perhaps send her this link from last October in which Boris Johnson admits the jabs don’t stop people catching or transmitting the virus:
https://youtu.be/fL00v2YjWKI
Ergo why would you bother getting one.
Apparently they have done studies of milk.
Yes – Milk!
It contains a protein which prevents you getting covid.
I’m upping my consumption.
You won’t hear that on the BBC, but oddly enough it was reported in the Daily Fail.
I think you have nailed it.
I had to listen to an idiot friend of my Mum’s complaining that she was jealous because my Mum was getting her booster sooner than she was and she was going to have to wait until January and inside I was thinking to myself “I don’t want my mum to have any kind of booster, you can have her bleeding booster any time you want it”
This was at a time when I was trying, and failing, to explain to my Mum how harmful the jabs are, and this idiot friend was talking about them like they were the latest “must have” commodity.
I think it was Norman Fenton who drew attention to a regular and repeated spike in deaths which followed the roll out of the jab in each age cohort.
This means that even the unjabbed experienced a correspondingly increased death rate.
This means that either the unjabbed must be dying in sympathy with the jabbed – or it’s just an artefact of not counting the jabbed as jabbed. The 28 day rule perhaps.
Not daft are you bigpharma.
Their approach is superb. It is working. Even now we still live with spectre of compulsory vaccination in the future. Quite the business model.
And how strange that noone, not even the Labour Party, has called for a windfall tax on Big Pharma!
That’s because Big Pharma was paid with the Magic Money Tree, iane!
Most of the profits will land in the US of A.
“This means that even the unjabbed experienced a correspondingly increased death rate”.
Without a breakdown of figures of vaccinated vs unvaccinated, I don’t think you can assume that.
Professor Fenton shows this with the data.
With each age cohort being vaccinated there was a spike in deaths amongst the unvaccinated in the same age group.
This was because those vaccinated are not classed as being vaccinated until 14 days after vaccination.
So people were having the muck squirted into them, then if they died within two weeks of the injection they went down as an unvaccinated death (probably a covid death).
This was very clever by pharma, as the vaccines killed people it was claimed the deaths were part of a new wave of covid which was spun as being more reason for other people to get vaccinated.
Thanks Mr. Tea.
I forgot it was 14, not 28 days.
There is also a spike in deaths in the 50 & above age groups ~6 months post jab which is discussed here Sasha and Craig presentation 220308 (rumble.com) giving a much more complicated picture of post jab deaths & raises an uncomfortable question of what mechanism is causing this? Post mortems are reporting that it isn’t the toxic injection, obviously!
Ample evidence that spike shedding by the jabbed can harm the unjabbed.
What a vaccine!
It’s fine really, the government and their ‘science’ advisory henchmen can do what they did with the Great Barrington Declaration, which was to feign ignorance and carry on regardless. And now they have the newly approved demographic of primary school aged children, who are at more risk from the flu, to experiment on.
Excellent work.
The point about the reporting systems (not meant to be used to identify side effect rates) is valid. An excellent example of this is the side effects related to menstrual cycles — the authorities swore that they didn’t exist (‘rare’) up until the point in April when there was a report on the UK’s women’s hour that asked listeners to report anything unusual to Yellow Card — the next week’s Yellow Card report had a doubling of reports related to menstrual cycles. Not a doubling of the rate — there were more reports in that one week than had been reported since vaccination began. The yellow card system isn’t good at identifying new problems, because medics generally only report on side effects that are already known to exist.
The other problem is that the authorities have consistently denied the existence (or ‘rare’) of any serious side effect/complication until the evidence becomes overwhelming — currently the two that are recognised are thrombosis/throbocytopenia and myocarditis/pericarditis. I imagine that there are other serious side effects that have so far managed to remain suppressed; the most likely candidates are those that take longer than 3-4 weeks to emerge, as there’s an assumption that side effects will occur within a 3-4 week window (and thus experiments seldom look beyond this point).
What is the prognosis for improvements in understanding among the public? How likely is it we will get to the bottom of this?
I know of several family members who have suffered I’ll health since their jabs. Even they do not associate their decline with the injections. Any suggestion of this is dismissed by them, the recipients of these biological agents.
I’d merely point out that they didn’t have those health problems before the vaccination. Let them put two and two together.
Anecdotal I know but 2 members of the local bowling club, average age around 72 years, membership approx 250 suffered severe eye problems a couple of months after the second dose, both been seen and no obvious cause found both been referred to neurology…neither reported to the yellow card scheme…. Replicate that around the country it’s alot of eye problems.
Is there a fertility time bomb ticking?
Quite possibly. But don’t fret, our replacement “New Britons” are being shipped in as we speak. No supply line issues there funnily enough.
Yes.
I look at pregnant ladies now and wonder if they have been jabbed (likely) what kind of Franken babies they will produce – which is a hideous indictment of something which should be a happy and joyous event.
And I look at couples struggling to conceive (both jabbed) and going through cycles of IVF and wonder – is there any point? wouldn’t they be better off just spending the money on a brilliant holiday?
It’s more than merely disturbing. At this point, it starts to look deliberate.
During the last swine flu scare the government rushed out a vaccine and indemnified the manufacturers. That scam didn’t run as well because the public had been insufficiently terrified to roll up there sleeve en mass, they rectified that this time around with lockown.
Regardless many took that vaccine and a significant minority had their lives destroyed by it, of course the government fought tooth and nail in the courts to avoid paying out any compensation.
Indeed the government will happily spend far more in legal fees denying the injured compensation than the compensation would cost.
So if you or a loved one were foolish enough to trust our government and got injured (or killed) as your reward good luck going against the State when seeking compensation.
[Note that legal aid has been slashed to nothing since the last swine flu pandemic hoax so you will will be paying for your own legal team and if you lose you will pay the State’s costs as well].
Please note that it is time for your booster.
Ministers lose fight to stop payouts over swine flu jab narcolepsy caseshttps://www.theguardian.com/science/2017/feb/09/ministers-lose-fight-to-stop-payouts-in-swine-flu-jab-narcolepsy-cases
By 2020, compared to 2009, social media had become sufficiently intense to magnify hysteria manifold within a short period of time.
This hysteria flattened the fledgling resistance very quickly in February and March of 2020.
No doubt. But why didn’t it affect us? That’s what I’ve been pondering these last few months.
I’m not an immunologist or doctor, yet I understood immediately the need for caution. All the propaganda did at that point was reinforce my initial instinct; this is not right, something is afoot.
I also know borderline dopes who employed the same cautious approach. Yet the most enthusiastic jabbees in my circle, the ones who question nothing, are the “educated professionals.” Even now they make casual comments about scheduling their young kids for jabs if they decide to book a holiday.
Social media played it’s part, but the propaganda clearly found a receptive audience.
I can’t figure it out. I have never been frightened by the virus, so that hasn’t addled my brain like so many others.
But then I know others who were not frightened of the virus, but still got the jabs. Because they weren’t frightened of the side effects either.
I am frightened of the vaccines. And of what the hell it is that has turned the majority of people around me into zombies.
And the more zombified they are the more they are likely to not do their own thinking and keep rocking up to be re-jabbed.
The hysteria feedback loop has two components: one which is positive and amplifies the hysteria, and, the loop to which we belong which is the sceptical “do you have any evidence for that view?” loop. What happened about five years ago, starting on climate, is that the big Internet companies started repressing the sceptics. The result is that sceptical voices are only seen a faction of the time of the hysterics … and it doesn’t take a genius to work out what will happen. Hysteria will now tend to grow out of nothing until it dominates everything …until we stop the internet mafia repressing sceptics.
During the last swine flu scare the government rushed out a vaccine and indemnified the manufacturers. That scam didn’t run as well because the public had been insufficiently terrified to roll up there sleeve en mass, they rectified that this time around with lockown.
What a brilliant device the lockdowns were. Firstly, they encouraged people to believe that something so unprecedented must surely mean that “this COVID virus” was going to kill enormous numbers of people.
Secondly, they provided experiences so distressing and disorientating that the vast majority never wanted to repeat them, and would accept any offer of a way out.
Whatever the preparatory mass formation events, the lockdowns themselves immensely accelerated the process: creating anxiety and providing a solution.
Swine flu was the covid trial run and they learned their lessons from that try out.
Covid vaccines are like Jimmy Savile. Your dont need all the evidence, you just know they are dodgy as f***.
This is very true. Though we do have an awful lot of evidence, thought there was in Savile too if you cared to look.
And in both cases it was the same people – those in authority and positions of influence, the BBC, Royal Family, who chose not to look or actively looked the other way.
Thank you Will Jones for sharing this .. it is a ‘brave journalist’ to do so! in this climate of suppressing detail, as your investigation seems to evidentially prove that it is a dangerous pharmaceutical product.
Superb summary. Well done Will for striking the balance.
There is so much smoke that ignorance at this stage is inexcusable from anyone in a public position to do something about it.
Pfizer were supposed to have phase 3 trials running for 3 years.
They terminated those trials at 6 months because the the all cause mortality was increasing in the vaccine group over placebo.
21 were dead in the vaccine group, 16 in placebo.
This obviously indicated something was seriously wrong with the vaccine.
There was supposed to be this super deadly virus stalking the land, the deaths in placebo should have been noticeably higher than in the saviour vaccine group because all things being equal the vaccine was supposed to be the only thing stopping folk from dying prematurely.
This is why Pfizer ended the trial early, they couldn’t risk the death rate being seen to get worse and worse in the vaccine group?
You don’t need negative stats like this when you have a block buster vaccine to get to market.
I suspect that is just standard practice … if at first it doesn’t give the right result … run the trial again (I presume finding excuses to remove the “problem” people).
It doesn’t matter if the number was only 1. If there is a risk of death there must be a choice and that risk should be openly discussed.
It’s funny how those with pre-existing conditions who catch the virus and die, it’s the virus that killed them.
But anybody susceptible to death from taking the vaccine that dies, it was their pre-existing condition that killed them.
And what happened to the emphasis being put on pharma to prove these deaths and adverse events were definitively not caused by the vaccine, rather then vice versa.
Like all the other statutory safety rules to protect human life and welfare we have lived by for the last 70 years – it was bi-passed and ditched by the crazed Globalists at the WEF and their allies in pursuit of their real dystopian agenda for the world!
The crime is manslaughter.
The crime is Genocide.
What an excellent question! Given the massive efforts to conceal the fact that many more deaths than admitted have probably been caused by the vaccines how can we know? What we must assume is that the number is far far greater than the figure admitted by Governments on flawed reporting systems as they are determined to conceal the facts through censorship and deflection.
What we must also assume is that the number of deaths wil increase steadily especially with promise of endless spike protein boosters being pushed to ensure the the body cannot clean them up recover or sustain its own immune system.
We face a society blighted by vaccine induced diseases, sickness, cancers and VAIDS which will leave individuals wide open to a whole range of infections and conditions that would otherwise have been non-life threatening.
Surely, this much, although concealed by a censored MSM, is already in the ‘well-informed’ public domain.
Yet still they are jabbing our children.
The question is, at what point do we make our baseline assumption become – this is deliberate, an assault on us that must be stopped, investigated then punished?
The point has already been passed – but the sheep are still sleeping and the Media are still censored by Ofcom.
This could not have happened in the UK before Blair arrived o te scene with his ‘orders’ and began dismantling out Institutions!
“Yet still they are jabbing our children.”
In more ways than one!
https://www.bbc.com/news/uk-england-oxfordshire-51467518
Far more than were killed by Covid, that’s for sure.
https://www.ons.gov.uk/aboutus/transparencyandgovernance/freedomofinformationfoi/covid19deathsandautopsiesfeb2020todec2021
<10K dead FROM Covid, Feb 2020 to Dec 2021
And given govt figures suggest lockdown killer over 200k, official government figures demonstrate what a total disaster has been inflicted on us by the corrupt bastards.
https://www.telegraph.co.uk/news/2020/07/19/lockdown-may-cost-200k-lives-government-report-shows/
MHRA reports just over 2k deaths attributed to the death shots. They also note publicly that they believe at most 10% of fatalities are recorded. So maybe 10k killed by the jabs add to that the lockdown figures and we are close on one quarter of a million slaughtered unnecessarily BY OUR GOVERNMENT.
Yes and people are still dying and will continue to die – as predicted by those brave virologists who tried to stop the evil madness – and were cancelled by the UK Media on our Government’s orders to Ofcom !
Still they jab our children and demand we have their spike protein ‘boosters’ forever!
Wait for the return of their ‘Vax Pass’ to access your own digital money!!
https://drmalcolmkendrick.org/2022/03/21/pfizer-and-me-best-buddies/
Good as usual and … er, the situation he describes seems to have been 30 years ago and was pretty brief.
I’ve rarely agreed with Chris Chope MP in the past but I deeply appreciate anyone in parliament who shows that they have a moral compass, regardless of ‘party’.
I’d support political changes that would lead to more independent-minded MPs being chosen, possibly a non-‘list’ PR system. I fear that things are heading in the other direction.
Quite. I know Chope winds many up, but that’s largely as he continually complains – and rightly – that parliament are not doing their job when assessing various bills. This can make him very unpopular, depending on the legislation – but he has a very strong point; Palriament no longer serves us and it has been all downhill since the expenses scandal and the House’s blatant attempt to scupper Brexit.
It no longer does what we elect its members to do.
Stop voting. It really IS a waste of time
The only way I can cope with the utter insanity of people who continue to take the jab, is to keep repeating: “It’s only natural selection”. Indeed, I am wondering whether it’s all part of a huge cycle: the idiots being idiots, breed like rabbits, the idiots take over, then the idiots do something really stupid, leaving only the sceptics behind, and then the cycle repeats. It does have a potential to explain a lot of human history.
It wouldn’t be so bad if the suicidal vaxxers didn’t want to force it on the sane people.
Exactly. Did you watch Fight Club?
I pray that one of our MPs follows the example of this man with integrity and backbone: WE’RE COMING FOR YOU: Aussie Senator Malcolm Roberts Throws Down Against Government Covid-Criminals (bitchute.com) In fact, having read other posts, plaudits to Sir Christopher Chope, and hope that the link can give others the strength to speak out.
When you listen to the establishment – doctors, MP’s, health specialists, they always manage to trot out the line ‘safe and effective vaccines…’ and ‘huge success of the vaccine rollout.’ It’s as though they continually have to affirm it to themselves, despite the fact that it has been an unmitigated failure.
One is too many
We need to expose Pfizer’s cover up of the clinical trial data which showed 21 deaths in the vaccine arm and 17 in the placebo. That alone, as Ed Dowd has pointed out, should have been enough to sink the vaccine.
Join Naomi Wolf’s campaign asking volunteers to read the Pfizer data dump ordered by a court after the company wanted it kept secret for 75 years. Any damning information is referred to teams of lawyers. https://campaigns.dailyclout.io/campaign/brand/cc3b3e5a-6536-4738-8ed6-5ee368c67240
Please spread the word, we need to act otherwise this nightmare will never end.
Basically this!
Just focus here all the time as it’s the most wobbly card of the medico-fascist house of cards.
I sure it was all worth it. The house imprisonment, the mental health issues, the suicides (especially amongst the young), the debt, the mass hysteria, the useless masks, the untested injections, the bullying, the coercion, the propaganda, the mind games etc etc.
But the best thing is that granny was saved, unfortunately her grandchildren won’t.
Granny is only saved – for now – if she keeps on getting jabbed it isn’t likely she is going to last that long.
Our societies in the West have begun to exhibit yet another hallmark of totalitarianism — a lack of good statistics. The Soviets covered up (or were incapable of recording) many vital statistics that made the regime look bad. That’s the world we live in today.
We’ll never know definitively how many people died from the vaccines or what their net benefit was. The that we needed was not recorded. Similarly for the blocking of ivermectin and HCQ.
But only a cursory inspection of the numbers tells you it is easily 1M who died unnecessarily, and directly, because of the corruption of the regime in the past 2 years.
I suppose you could even say this about every C19 death, considering it was made with US funding.
https://nakedemperor.substack.com/p/the-missing-number-in-the-pfizer?s=r
Good article Will.
Is there anyone here who has had more than one ‘vaccine’? If so, would you be so kind as to share any adverse experiences you’ve had since?
Also does anyone know friends/relatives who are suddenly becoming ill with headaches/ear ache and pain behind the eyes?
Members of my family are ill with all the above and have had three jabs.
My partner has had 3 jabs of Pfizer (who knows what’s in the vial? – it says Pfizer Comirnaty on the label)… no noticeable side effects at all. Sorry to disappoint.
Has anyone considered that all the bad batches get sent to the UK? The manufacturers know that all that happens is that the Brits tut-tut and say “Mustn’t grumble!”.
Onthe contrary, this is one subject I want to be wrong on. Still will never have the jab myself though.
The sad thing is we will almost certainly never know the real numbers. Yes, i know people who have had adverse experiences from the jab but nothing life-changing. On the other hand, 3 members of my family have died from cancer in the last year. One had a small lump show up during 2020 but ‘didn’t want to bother the doctor’; when it was finally checked out, she was at stage 4 and died a few months later. Another was diagnosed with lung cancer last summer, she never smoked but i gather that lung cancer is not uncommon whether you smoke or not. She was doing well after chemo but had a big relapse a few weeks ago and died this week (don’t know when she had a booster but i’ll bet she did) My BIL, a fit man who was playing golf once a week all last year was diagnosed with a tumour in the pancreas around new year and died in March, also fully jabbed.
It will of course be said that all these were elderly folk (70s, early 80s) and it was perfectly understandable that they should all get cancer at this time and certainly pancreatic cancer can cause death very quickly. However, i will never be convinced that the jabs didn’t have some effect on their immune system which could have brought on the cancers, or that an existing one wasn’t made worse by jabs and boosters.
I am sorry to hear of all your losses Maggie May. I would imagine that you are right to be suspicious and I fear that you are probably on the money when you speculate that the jabs impacted their immune systems which then left them vulnerable to cancer. The US pathologist Ryan Cole has seen this in biopsied tissue he has examined and in blood samples, where after jabbing, the markers which represent effective protection against the development of cancer are substantially reduced.
Admitting to vaccine injuries and death will promote vaccine refusal.
You don’t need to promote confidence when you have propaganda and coercion in your tool kit.
Have a listen to the fat fascist Gaunty!
https://www.youtube.com/watch?v=249uM_cvl9c&t=161s
Dear Will Jones, thank you.
Once again. 37656 people dead only in the UK, 21 days after their dose (1st,2nd or 3rd).
Plus ~5000 dead ‘with’ covid, in the same time span.
It’s official.
https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/datasets/deathsbyvaccinationstatusengland
And remember, as of a few months ago (not checked NHS data for a while) Covid had killed around 9000 people in England without comorbidities.
9000 deaths for covid. 38,000 deaths for the vax, and counting.
Given the colossal operation to suppress vax deaths by the regime, I would argue now, sadly, that we will never know how many were killed by them, or the many more who were maimed and injured in some way. Medium and long-term effects are still entirely unknown but are likely to involve autoimmune diseases and also problems with fertility.
The vax mandates of 2021/2022 were indisputable crimes against humanity and everyone involved in forcing them on people in anyway are criminals who should be tried at the Hague. Until this happens, the West is dangerous, irrelevant and to be ignored.
Great article, Will. Thanks for the level headed look at this important topic.
I wish to add a few comments on the rate of deaths. Will suggests that VAERS may be signalling 120k deaths in the USA. Since 250 million Americans have been jabbed, that means possibly 1 in 2083 people died. My estimate by early 2021 (from multiple other sources) was that it might be as high as 1 in 1000. Sure enough, when the jab was rolled out in my small town (population 3k), 4 people died unexpectedly within days of their injection. All 4 were in good health previously, 2 of whom I had talked to just prior to their sudden passing. None of the deaths were recorded as a vaccine event. While it is true that people routinely drop dead, it is highly improbable that 4 should do so in one month in one town and all immediately after taking an injection. So I blame the covid shot for at least 3 deaths.
Conversely, I know of no one that died of covid. Furthermore, the local funeral director (a friend of a friend) confirmed only 1 deceased person in 2 years time had covid on their death certificate, but deaths since the covid shot was rolled out have increased noticeably. This suggests the death rate is worse than 1 in 1000.
Interesting and vital article, treading cautiously and even courageously into what is a very difficult area. Thanks Will.
Hopefully Will, or someone with his measured approach and analysis, will continue to analyse this subject over the coming weeks, months and even years, as new evidence and new interpretations arise.
This human tragedy cannot be allowed to be dismissed and conveniently forgotten.
Good wrap up article of the ongoing very sorry situation.
Just adding to the others.Great article,Will,and thanks for all great work you have done.
With all this evidence that the so called vaccines actually kill people and cause serious and life changing injuries to many hundreds of thousands more, it’s unbelievably lucky for the governments of the world who inflicted this on their people that WWIII is kicking off and diverting everyone’s attention. COVID and vaccines are so last year.
Er, don’t you think that’s why the war kicked off when it did, just as the COVID narrative is unravelling?
Apologies if you’re American, I’m a sarcastic Brit.
My take is that WWIII kicked off in March 2020 and we are already 2 years in to a war of what might be a very lengthy duration. The war of the governments of the world against their own peoples.
And doubtless all this was already known. I’m sure there isn’t much that’s a surprise to ‘them’.
Drs. Zev Zelenko, Michael Yeadon, Peter McCullough, Harvey Risch, Pierre Kory, Paul Alexander, Robert Malone, Geert Vanden Bossche, sucharit Bhakdi, Ryan Cole, along with thousands of other doctors have advised the use of early treatments for covid with repurposed drugs and to avoid the repetitive injecting of experimental biologicals as this drives the virus to mutate, possibly into a more lethal variant.
Norway stopped vaccinating the frail in January 2021. The first to be injected with boosters are the frail elderly along with other “vulnerable” over 50’s.
Steve Kirsch believes the cdc VAERS numbers to be underreported by a factor of 41. The big question is why is such a dangerous chemical still available for human consumption? All of us know friends and family damaged by a covid vaxx and yet the silence is deafening. I can only imagine what GP’s and other doctors and practice nurses are witnessing.
To describe as “disturbing” the continuing government and mainstream media claims that the vaccines are “safe” in the face of this number of vaccine related deaths and adverse events is surely a massive, massive understatement, particularly in the context of the almost obsessive continued roll-out to young children. The continued roll-out of these jabs goes against ALL the long established medical and health care ethics of “do no harm” and cannot IN ANY WAY be justified by the risks presented by covid. The data and analysis set out in your article has been known for months now and for everyone involved in their continued roll-out from government to advisers to doctors to schools despite all the KNOWN damage can only be described as criminal. It’s high time it’s called out as such, before many, many more die unnecessarily, including children.
As ever, nature has us covered. For all those who believe the vaccines are safe it’s looking very likely that either they can no longer contribute to the gene pool or their contributions will be so weak and fragile that the blood line won’t last many more generations. Every cloud and all that…
Really, is “disturbing” the best you can do? The author must have ice in his veins. How about “criminally negligent” or “intentionally genocidal”?
Good, well-cited summary as usual Will.
Another data point worth mentioning is Alberta Canada, who up until February 2022 displayed cases, hospitalisations and deaths from day 1 post-vaccine.
https://web.archive.org/web/20220108064918/https://www.alberta.ca/stats/covid-19-alberta-statistics.htm#vaccine-outcomes
The data echo others in showing a huge jump in cases, hospitalisations and deaths within the few days post-jab, and throughout the initial 14 day period since vacciantion is given that drug makers and authorities insist be considered no vaccination has been given.