A major update for this week’s analysis of the UKHSA Vaccine Surveillance report, with corrections to previous data. In our last post on week 5’s data we noted that it appeared the data for infections/hospitalisations/deaths for two doses of vaccine also included data for three doses of vaccine within two weeks of vaccination i.e., people were not counted as triple-dosed until 14 days post-jab. As a result we tried this week to obtain further data on infections/hospitalisations/deaths that might include the missing information. Unfortunately this was unsuccessful, but we did manage to get hold of the vaccination data used by UKHSA in its calculations (this differs from the official ‘vaccinations given’ figures because it only counts people that are still alive and resident in the country). This new data provides some surprising additional information that necessitates revisiting prior data.
The main issue is it transpires that the UKHSA has been using the number vaccinated at the end of the four week period to calculate its rates of infection/hospitalisation/death. As a result, its estimates of the boosted population have been excessively high; it’s been using a boosted population that is higher than the actual boosted population over the four-week data period.
To illustrate this, see the figure below.
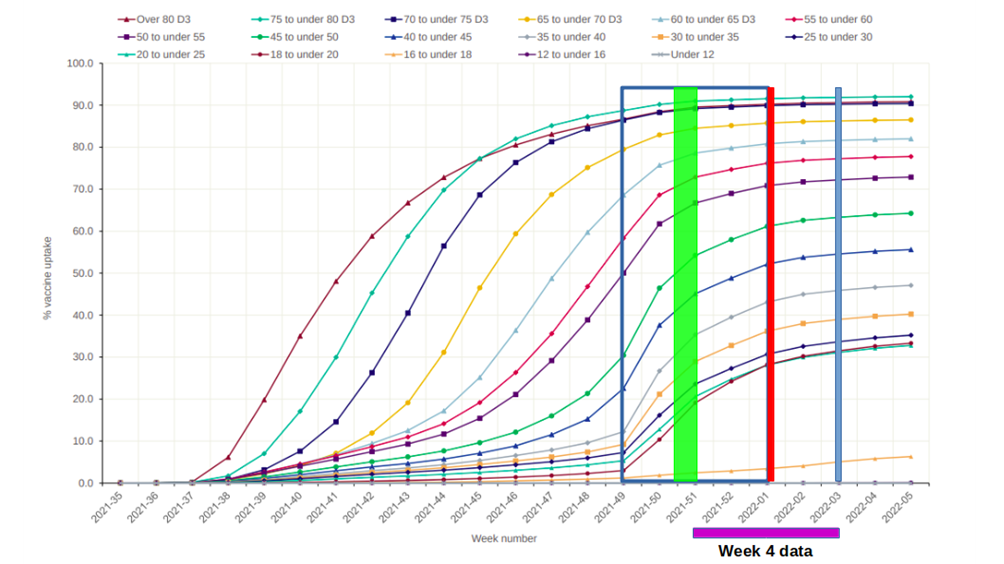
The data for the week 4 report is for up to week 3 (indicated by blue vertical line), as there is a delay of a week in their collation of the data. As the data is made up of four weeks’ worth of data, this covers the period between the end of week 51 2021 and the end of week 3 2022 (indicated by purple bar below the graph). However, the data is for 14 days after vaccination, so the relevant vaccination data should be taken from the blue square shown in the figure, from the end of week 49 2021 to the end of week 1 2022. Instead, the UKHSA took its vaccination data as that at the end of this period, shown by the red vertical line. As is apparent from the graph, because of the rush to boost the population during this period, the number vaccinated at the point of the red line is significantly greater than at the start of the period in question (considerably so for younger age groups). Really, the estimate of the population boosted during this period should be a weighted average across the study period; this will lie somewhere within the green rectangle (exactly where is dependent on the shape of the curve between over the period in question).
As a result of this error, the UKHSA rates of infection/hospitalisation/death will have been smaller than they were in reality, giving the impression the vaccines were performing better than they were. Whether this was done on purpose to exaggerate the benefits of the vaccines or was the result of a simple mistake is unclear.
Unfortunately, because our estimate of vaccine effectiveness of dose 2 alone was based on matching existing vaccination data to the UKHSA’s data which used its inflated population estimates, it resulted in our estimates being too pessimistic. So much for trusting official sources of information.
But, of course, if there is a mistake the right thing to do is to try to rectify it – so this week we’ve reanalysed the data for this year using a more appropriate estimate of the proportion of the population that has received two and three doses. As of today we’ve got data for the over-40s population, and next week we’ll aim to expand this.
There is an upside to all this, which is that in obtaining the same vaccinated population data as the UKHSA uses we can also estimate the vaccine effectiveness for those who only received one dose of vaccine.
So, on to the analysis. Vaccine effectiveness against infection first.
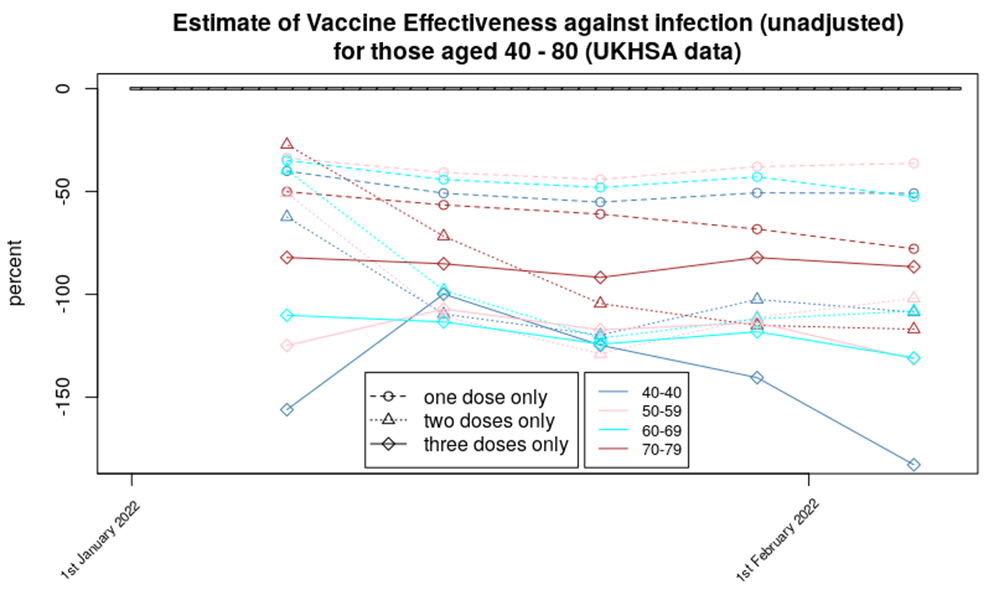
This is a busy graph, but it splits broadly into two sections:
- We now have the data for dose 1 – these are shown in the dashed lines near the top of the graph. Those having taken only one dose of the vaccine appear to have approximately 50% more chance of infection compared with the unvaccinated (note that all the values are negative, meaning the unvaccinated had lower infection rates than all the other vaccination categories).
- Data for dose 2 and dose 3 of the vaccines appear to show a somewhat similar level of protection, at around minus-100% – that is, the vaccinated appear to be approximately twice as likely to become infected with Covid as the unvaccinated. The pronounced downward trend in the data is likely a result of the vaccines’ protection being even worse for Omicron variant. There is a hint in the data that in the weeks following the booster (but after the 14 day post vaccine period) there is an increased risk of infection (indicated by the upward trend in the data between the first and second data point for those aged 40-49 and, to a lesser extent, those aged 50-59).
The finding that the vaccine effectiveness isn’t so negative for those with only one dose of vaccine offers some hope that the increased risk of infection might wane with time. Alternatively, the data might simply suggest that two doses ‘seals the deal’ with even more increased risk. It would be nice if there were official investigations into this effect, but, as with all potentially negative aspects of the vaccines, our authorities appear to prefer not to know. It’s worth mentioning that these are unadjusted vaccine effectiveness estimates of course.
The estimate for vaccine effectiveness against hospitalisation is shown below.
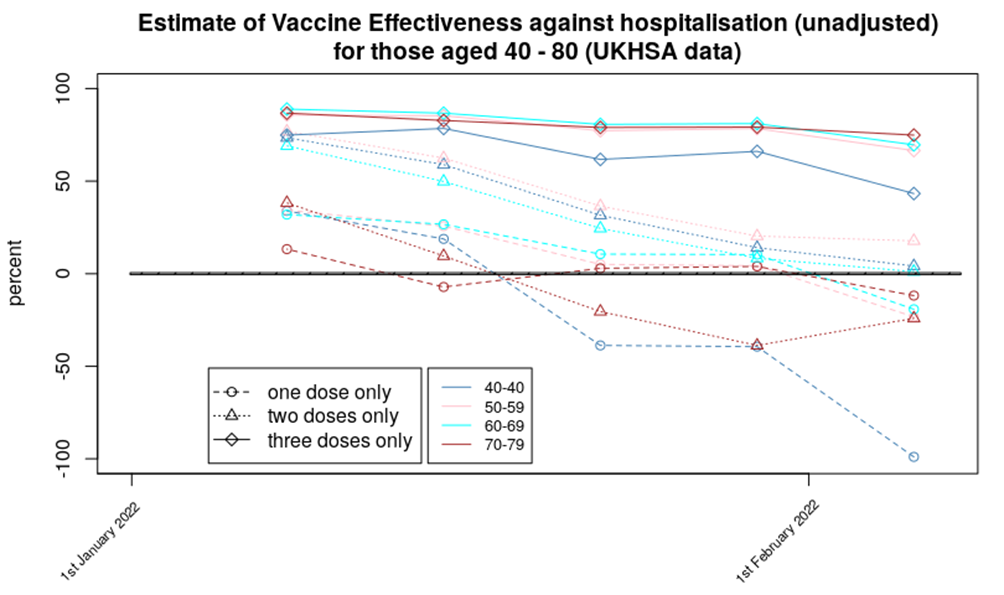
The data again can be split into two:
- Three doses of vaccine appear to have offered some protection against hospitalisation during the Omicron wave. Interestingly, the data suggest that those aged 40-49 obtained the least benefit. We hope to update this chart with data for those aged under 40 later in the week; it will be interesting to see if this trend is also followed by data for younger age groups.
- Two or one dose of vaccine appears to offer very little benefit against hospitalisation. All of the estimates of vaccine effectiveness for one dose of vaccine are slightly negative (with the data for those aged 40-49 at minus-100% possibly an outlier – we should find out more with this Thursday’s update); the estimates of vaccine effectiveness for two doses of vaccine are slightly positive.
Again, an interesting aspect of the graph is the pronounced downwards trend, possibly due to Omicron’s vaccine evasion.
On vaccine effectiveness against death, there is an important additional consideration. While the UKHSA data for infections and hospitalisations refer to ‘by specimen date’, the data for deaths refer to ‘by date of death’. Thus for the deaths data we also need to consider that people currently infected don’t get vaccinated, and that the time from infection to death is usually at least 14-21 days. As a result, it is necessary to consider the vaccination figures not at the point of death, but at a point some weeks earlier. We are undertaking a sensitivity analysis to work out the ‘right’ delay to use, but for now the data shown is for a delay between infection and death of two weeks – thus it has somewhat but not fully compensated for this effect and as a result the estimates given will likely be slightly too high.
With that in mind, data for the protection offered by the vaccines against death shows a similar trend as seen in the hospitalisation data:
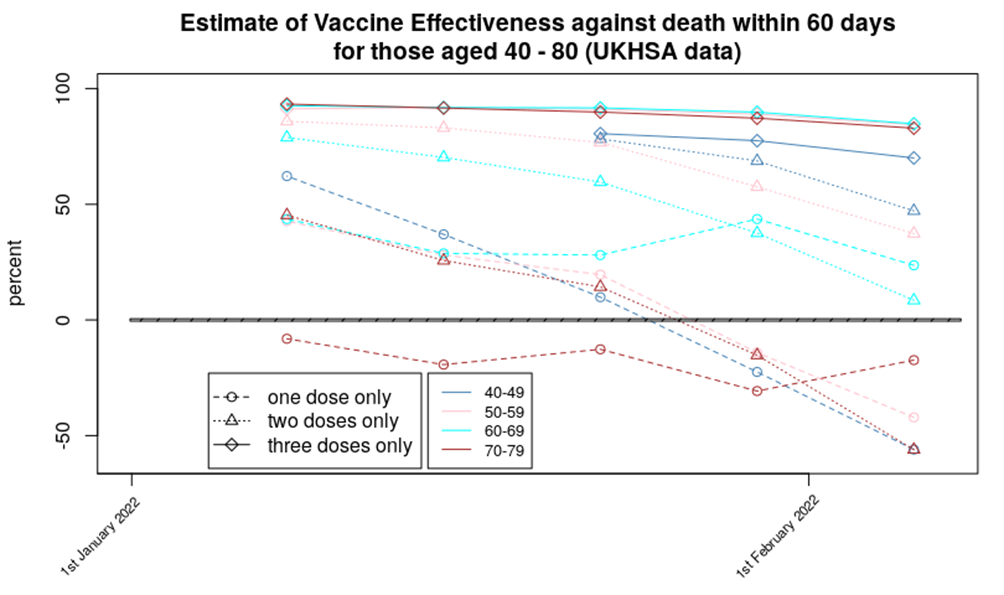
Three doses of vaccine appear to offer a reasonable protection against death, two doses show significantly reduced protection (especially for those aged 70-79 where it is negative), while a single dose appears to result in an increased risk of death, compared with the unvaccinated. Again, the downward trend in the data suggests that Omicron variant has made the vaccines’ job much more difficult.
I should explain why I concentrate on ‘deaths within 60 days’ rather than the more conventional ‘deaths within 28 days’. There is some evidence that the time course of infection in the vaccinated is more drawn out than in the unvaccinated. It isn’t clear whether this is a delay between infection and serious symptomatic Covid or between hospitalisation and eventual death, although data on hospital beds taken up by Covid patients suggests the former (there are fewer than you’d otherwise expect). Up until now the evidence has been limited to the deaths within 28 and 60 days of infection data in the UKHSA Vaccine Surveillance report. However, in recent weeks a new source of supporting evidence has emerged – the official deaths data published every day by the U.K. government:
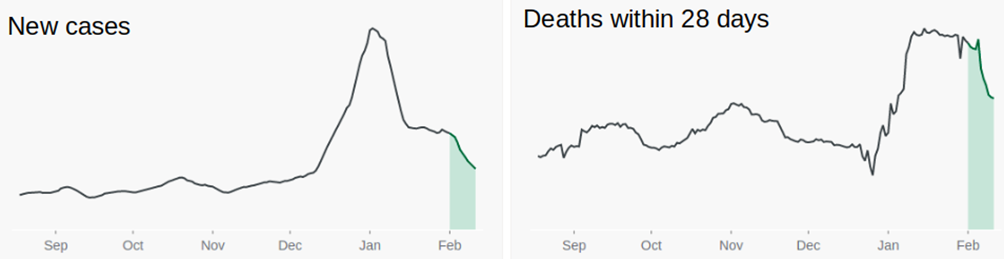
An aspect of the Omicron wave I found disturbing was how the deaths didn’t decline in synchrony with the case numbers; there was a clear lag of about two weeks before deaths started to rise, but they didn’t fall as might be expected and remained elevated. In the past week they have declined rather steeply, which has resulted in the exclamations of ‘vaccine success’ by the usual suspects, but note that the precipitous decline in deaths has tracked the decline in cases with a lag of around 28 days (it appears to be between 25 and 31 days; close enough). Is this, however, because Covid deaths in fact remain elevated, but they’re not counted as Covid deaths as they’re beyond 28 days after the original infection appeared? We should know more about this effect in the deaths data from the Vaccine Surveillance reports over the next few weeks, as they include data for deaths within 60 days of vaccination.
Amanuensis is an ex-academic and senior Government scientist. Find him on his Substack page, Bartram’s Folly.












To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
Very well said. Thank you.
I liked Mr Sunak’s bold decisiveness to go for an early election.
I changed from Reform to Conservative.
Then came the D Day debacle.
I too will now be voting for Reform and, yes, as an indirect vote for Kemi Badenoch.
Why on earth would you care about who did what at the D-Day circus, and how could you vote for the Lockdown Chancellor?
Badenoch seems vaguely OK in some respects but she also supported lockdowns. That’s a red line for me.
Anyone who had relatives serving, lost relatives, in the two world wars, takes the anniversary of D Day extremely seriously, as does much of continental Europe, including many Russians whose nation’s (ancestors, relatives) task on mainland Europe of defeating the Wehrmacht was made so much more straightforward; ultimate victory assured.
If you don’t get it, like, clearly, Mr Sunak, then you don’t get it, and you will not be alone in that, but tens of millions do and leaving the ceremony early…….for an ITV interview………is indicative to millions of someone who has either lost the plot or never clued into it in the first place, despite forthright and sincere apology.
I want decisive action in Westminster/Whitehall. I don’t know Mr Sunak but he seems a great deal more decisive, capable, honest, than Sir Keir Starmer and those two were the only two options.
It is now clear to me that neither candidate for PM is fit for that office.
Virtually the entire country supported the lockdowns. The entire cabinet supported lockdowns, only Jesse Norman requesting a cost/benefit analysis of the likely effect. In a perfect world, that should disqualify all except Mr Norman from high office.
Ms Badenoch was Equalities Minister 2020-2022 so by no means a key player. We all make errors of judgement. In my opinion, Ms Badenoch is the best candidate to lead the Conservative Party after the election.
That is only my own humble opinion and, no doubt, of little interest. I only comment on here to try and contain the still incandescent rage at the last four (actually 32) years. I have been hopelessly wrong before and will definitely be hopelessly wrong again……
Fair enough. I do wonder whether politicians should be involved at all in the D-Day stuff – I tend to think not.
Whether you are wrong or I am wrong or both sadly doesn’t matter – we are going to get a Labour government, probably for at least a decade, and I just see the proper role of the state so differently from most of my fellow citizens that I will not see any significant improvement in my lifetime.
Both Prime Minister and Monarch attended the original D-Day. It is an excellent tradition for their successors to follow, reminding the PM that his first duty is defence of the realm!
They ought to be reminded of that, but I think that anything a politician does will end up with them trying to score political points, which I feel debases the whole thing.
Well it has been an epic fail then!
I would be amazed if they get anywhere close to a second term. When people see that day to day life is still getting worse (it will) with taxes going up, Net Zero bankrupting the country the bitter infighting with the left wing Trots they will race back to a right of centre politician. That will be Reform ideally with Farage at the head.
Blair was re-elected twice, Cameron was also re-elected.
With two cast iron guarantees that Nigel kept him honest on the second.
He was pushed into a corner, for once
Proving how dumb people are
This is my view as well. Giving votes to 16 year olds will not help if you continue to screw them over in favour of mass immigration.
The government need to revert back to being administrators to the people, not handing them “rights”. Not sure Reform have the stones but they are well ahead of UKIP, Heritage & Reclaim. Though I do credit Reclaim for holding Nigel’s feet to the fire and getting him to stand after the Unite the Right rally a few weeks ago.
Those climbing the greasy pole are never the same person once they have got to the top. Badenoch will never be given the top job unless she has taken the Danegeld.
Firstly, I am a great admirer of Toby, most particularly for this site and the Free Speech Union but politically he is on another planet.
The Conservative Party is under controlled destruction and yet I see no articles from Toby questioning this. Why?
Over the last fourteen years the Conservative Party has effectively set to dismantling this country. Why?
The Conservative Party is no longer conservative and yet people like Toby seek to perpetuate the myth. Why?
A reset is being forced upon us and yet those in the bubble cling to cock-up theory:
C1984 – cock-up
Brino – cock-up
Immigration – cock-up (but we will sort it. Honest.)
Islamification – erm, best not go there
Increased lawlessness – ahh, not us. That’s your City Mayor”s job.
I could go on and on but I would be here all day.
So Toby is going to vote Reform on the basis of some convoluted logic by which over the next five years the suitably shrunken and chastised Con Party can address its utter failings and get itself back in to shape for 2029. Well that’s lost on me. Totally.
The Conservative Party is being wiped from history and for all the reasons I elucidated in a post two days ago. It’s over, it’s finished. Build Back Better don’t forget.
ALL the current political establishment need removing and permanently bar perhaps a dozen honourable exceptions. Why on earth should we allow failures, 600 plus men and women, to seek office once again? It should not be about voting them out more that we must not sanction treason.
Our whole political system is firked beyond repair and the only chance of recovering our country is to accept this fact and set about building from scratch.
On a positive note at least Toby is not voting for the Uniparty.
Yup I would agree with all of that
Thanks tof 👍
So do I, but, who do you vote for then?
Reform is the best of a bad bunch!
I will be voting for either the Heritage Party or Alliance for Democracy and Freedom, both of whom unequivocally and explicitly oppose lockdowns and medical fascism. I wrote to my Reform candidate to ask for his views on “Covid” and received no reply. Had I received a convincing response I may have considered voting for him.
Tof, bots can’t vote, Thank goodness!
Perhaps they can in the USA
My preference is Braverman.
I am also a fan. But, in my opinion, Ms Badenoch is a better performer in the H of C.
But both would be in our cabinet though
Totally agree though DDday is just representative that the billionaire Hindu and his class have no clue and no class.
BUT……
No one discusses the RONA MEDICAL NAZISM, LOCKDOWNS, STABS, EXCESS DEATHS AND THE DESCENT INTO TOTALITARIANISM.
And the Muzzie question is being addressed only by Reform – however very tendentiously.
I am voting Reform. I will not reward the Convicts for a half assed Brexit, ECHR still in our laws, open borders and the great English replacement, massive taxes, endless spending, the forever war in the Uketopia, Nutard Zero, Rona Fascism and all the attendant bribes, payoffs, grafting and 100% bullshit ‘science’. Rona forever destroyed my belief in the National Death Service, ‘Science’, Institutions, Pharma-ment, the Police….ad infinitum. FTA.
I’m not sure about WEFer Kemi. She paid Tata Steel £500m of taxpayers cash to close our strategic steel making blast furnace, losing 2000 jobs in the process and replacing it with an electric arc furnace that can only recycle used steel.
So it’s a thanks but no thanks from me #NetZeroSeats
Edit:- Jenrick might be the only one that could convince me.
Yes, I think Jenrick seems like a genuinely good man with principles, at least more principles than most of his colleagues. He should join Reform.
Yes, Jenrick seems the best option to me.
Badenoch, Braverman or Patel will not bring the voters back.
I can’t believe that anyone is still considering the Tory party as viable, either now or at some future date. They have shown themselves to be rotten to the core. They have presided over the most disastrous five years of any party ever. There is not one single issue on which they have had anything even resembling conservative policy. They are finished.
They are also ripe for a hostile takeover, like Trump did to the Republican Party. In fact, as they are likely to have so few MP’s it will be a much easier job for a new broom of leadership to clear out the rubbish.
There is one thing which comforts me as we stare into the abyss of a Labour administration for the next five years and that is the sight and sound of left-wing, Tory wet ar seholes fluttering like poppies in the breeze as they contemplate their futures without expenses. It is they – and no-one else – who are about to inflict Starmer and his unholy crew upon the nation and their collective terror is balm to my soul.
Good article in today’s Conservative Woman with a cogently argued case that Ratboy deliberately ‘threw’ the forthcoming election. Difficult to argue with when you see his actions delineated. Davos job done, CV burnished, “adios muchachos!”
I posted a link to the article BTL in the News Round-up with some suitably critical comments.
My own conspiracy theory about PM May was that she deliberately scuppered her majority so as to water down Brexit. She was, and her advisor, a Remainer that saw David Davis resign.
As I said under Ben Piles article today:
Looks like a reasonable analysis. But where do the proposed policies come from? A group of Permanent Secretaries and a club of professional organisations and one or two royalists perhaps? After all, whichever party provides the Ministers, they will have a job to change the minds of a department.
I wonder if anyone wants to gamble on the turnout, outside the constituencies that will make the headlines in the usual media, such as Clacton.
Toby, there is another good reason to vote Reform you didn’t mention. I can see the reasoning behind your thinking, and I presume you must be not too bad a chess player, as you have some neat manoeuvres in there but although I cannot see Reform winning an election, I think to myself that just as Farage kicked up the immigration stink that led to the Brexit vote so too might Reform cause the Tories to really wake up to the fact they need to be proper Conservatives again and stop playing the pretend to save the planet eco socialist game, and we may then have a choice at election times between phony planet savers (Labour, Lib Dems, Greens, and SNP) or Politicians who reveal to the public the true state of climate and that there really isn’t an emergency (Proper Conservatives)
Let them hang by their own petard, good riddance. They are the same cheek of the same arse as Labour, Galloway’s words.
Its all over bar the shouting. My focus is on 2029, which, assuming i’m still here, is what we should all be looking towards. What we have lacked for the last 14 years is effective opposition. God willing Farage will get his seat, with a handful of other Reform candidates, and be the ‘bloody nuisance’ he has already spoken of. Just as important is the orange mans victory in November, which should bring Globalism to a head. 5 years is an awful long time in politics. Labour are trying to play the even handed broker, but it will turn rabid as soon as Starmer is in No.10.
As an old socialist I’ll be voting for Workers Party of Britain.
What is their position on lockdowns and medical informed consent? I see they are suggesting something like nationalising Big Pharma. I am no fan of Big Pharma but I don’t think the answer is to bring Big Pharma under closer control of the state.
I doubt if any political party has mentioned “lockdowns” in their manifesto.
However, these 3 statements by WPB suggests they will be very libertarian as far as lockdowns and medical informed consent are concerned.
“Prevention will be central to our national health strategy which will be directed to the five key drivers of health outcomes – nutrition, exercise, sleep, stress and loneliness. We will declare war on ultra-processed food, improve the standard of school meals and invest in health education. Big Food and Big Pharma will be regulated to ensure positive outcomes at every level of national health.”
“The rebuilding of community goes alongside a commitment to find ways to alleviate loneliness while leaving those who want solitude to have their silences. Governments cannot legislate human relationships. Our ethos is one of respect and tolerance for individual lifestyle choices.”
“We are suspicious of the State’s accumulation of powers under past war conditions which appear to be more about the preservation of the State than the protection of the people. We will undertake a careful review of all emergency powers and related legislation in order to establish whether they represent a threat to civil liberties and of the conditions under which they might be invoked.”
Well I would prefer something more explicit.
Heritage, Freedom Alliance and Alliance for Democracy and Freedom all say “no more lockdowns”.
Your comment made me scan the manifestos of the Heritage Party which I agree with apart from banning abortions.
I also agree with the Freedom Alliance and Alliance for Democracy and Freedom.
However, these 3 parties and the WPB have no chance of government under FPTP until PR is made law.
Although not a wasted vote, a vote for either of these 4 parties would mean I had a clear conscience and exercised the right to vote won by the sacrifice of previous generations.
And Heritage want to stop Agenda 2030, they actually call it by the UN definition. If Heritage was on an equal level as Reform, I’d vote Heritage in a heartbeat. Tice went to Ukraine and is mates with Medazolam Mat.
Kurten appeared on some of the early anti lockdown protests
I’d vote for any party that will destroy these fake tories and at this time Reform with Farage at its head is favourite.
And a bigger bunch of skivers you couldn’t meet…
I will not be voting Reform. Weak on “covid”.
Also puzzled that TY would even consider voting Fake Conservative given they are Nut Zero Fanatics like the other Uniparty parties, as well as lockdown fanatics.
I’m not sure what you mean by that, this is Reform’s position on net zero:
“Net zero means reducing man made CO2 emissions to stop climate change. It can’t. Climate change has happened for millions of years, before man made CO2 emissions, and will always change. We are better to adapt to warming, rather than pretend we can stop it. Up to 10 times more people die of cold than warmth. In Roman Britain some 2,000 years ago, it was 2 degrees warmer than now. Grapes for wine were grown in Yorkshire.”
That doesn’t sound like net zero fanaticism to me, but perhaps I am misunderstanding you?
What I meant was it sounded like TY might have considered voting Tory but as they are going to lose anyway, he will vote Reform because that will force the Tory party into getting a more right wing leader. It sounds like he still believes the Tory party has a future.
Oh, OK I see. I misunderstood. Thanks for the clarification. It’s nuts that anyone can see a future for the Torys.
I tend not to talk politics with people I know, but would love any of the Tory voters among them (if there are any) to explain why they would choose the Tories over Reform. You’re either a conservative in which case vote Reform, or you’re not in which case just vote Lib Dem or Labour or Green.
“We are better to adapt to warming, rather than pretend we can stop it”
Adapt to warming you say? I’m still waiting for summer to begin – we are halfway through June – what happened to ‘Flaming June’?
They are Blairite Globalists, so no wonder they scuppered their manifesto.
A vote for Conservative is a vote to prolong Britain’s agony.
Labour will get a big majority or a huge majority. Huge may actually enable Starmer better to resist the worst extremists. The practical goal is to destroy the Conservatives and re-constitute a patriotic, freedom-oriented conservative party.
Reform is the only vessel for that ambition and its authority is likely to come from the number of its voters rather than the number of its MPs.
I’ll vote Reform.
Heaton-Harris, my MP, disdained the traditional family in favour of homosexual adoptions and gave Northern Ireland to the EU.
His replacement, parachuted in from Pudsey, is an active campaigner for LGBT.
Today’s ‘conservatives’ are further to the left than Clegg’s Libdems and globalist.
Time for them to die politically.
“Today’s ‘conservatives’ are further to the left than Clegg’s Libdems and globalist.
Time for them to die politically.”
I had started to believe I was on my own with this opinion.
I can assure you that you are not on your own.
The clue is in the name. It’s a “general” election. Whoever, or whatever, wins, we’ll have to fight them on the beaches when it comes to various details. Voting for someone does not necessarily mean that you agree to everything on the agenda, so it’s down to an assessment of which is the worst (if you’re a pessimist).
Tories switching to Reform might not stop a Labour win but narrow its majority. If the Red Wallers voted Reform too maybe a Reform majority, or hung Parliament and Labour/Reform coalition.
This wouldn’t last of course, but would limit Labour destruction, and allow Reform time to consolidate with a chance of winning the subsequent election.
Wishful thinking probably – but hope us all we have left.
Net Zero Elephant in the room
As far as I can see Net-Zero is the huge elephant in the room that is being totally ignored in this election. It seems to me that Net-Zero is going to be the huge issue over the next 5 years, the uni-party seems intent on pursuing the Net-Zero agenda which will start to have a huge impact on our lives. TPTB will give up on trying to persuade us and it will be imposed by force and legal action.
Net-Zero will have a huge, profound and increasingly immiserating effect on all our lives and yet it does not seem to be an issue in this election. And so will I vote Reform, yes I will, because of Net-Zero, they seem to be the only party to have any sort of policy to question this whole uni-party NET-Zero Agenda. Is their policy perfect? are they the best thing since sliced bread? is Nigel Farage the new Messiah? No, No And No. But either I spoil my ballot paper or I vote Reform, just to hopefully put a spoke in the Net-Zero wheel.
Yes, people have forgotten this:
UK 2035 petrol and diesel ban: what is it and what cars are affected? | Auto Express
The head of Toyota warned of this absurdity of putting all eggs in the EV basket. Toyota decided to accept environmental fines as it was cheaper for them than losing billions building cars that people do not want, and as the market for EV’s collapses we see Toyota were entirely justified and are now making huge profit on the Hybrids that they decided to push forward with.
Over the last couple of weeks I have been saying pretty much the same as you on Net Zero and over the longer term I have been warning of the devastation that is about to hit us and all the other countries trapped in this eco socialist Double Nelson.
The pubic really have no idea what is about to hit them with energy prices set to hit the stratosphere and once 95% of homes have the smart meters installed by hook or crook then will start the “dynamic pricing”. The unsuspecting public think the smart meter is there to save them money and stop them getting estimated bills. ——–Yes that is the selling point but if there ever was a latter day trojan horse then it is the smart meter, as customers will be paying prices based on demand and depending on whether the wind is blowing or not……..wakey wakey people.
The dynamic pricing in the trade is already live, via the APX spot market on wholesale pricing. More info here under ‘Price’: https://grid.iamkate.com/
The other possibility is remote load management for certain things, like trying to charge some kind of car, to keep within the capacity of the local distribution network; they won’t advertise that!
I’ve lost count of the number of letters from my energy supplier stating I need to have my meter change to smart meters. Every one goes into the wastebin.
“Kemi Badenoch is a very devoted Catholic. She gets together with church leaders in London to help Catholic Ukrainians.”
“Kemi, who is 42 years old, calls herself a “cultural Christian” and has many different religious traditions from which to draw. She was born in London, but grew up in the United States and Nigeria, deciding to go to the UK when she was 16.
Her grandfather on her father’s side was a Muslim who became a Christian, and her grandfather on her mother’s side was a Methodist minister.”
Like Candace Owens, she converted to Catholicism so that her white Catholic husband would marry her, as the Catholic church demands that children of Catholics must be baptised and raised as Catholics.
It is remarkable that all the Third World Ethnic women who have gained political power and fame in the West have refused to marry within their own ethnic group, always determined to marry an Ethnic European = White Man, which has helped their meteoric rise to fame. For example, Priti Patel, Suella Braverman, Ayaan Hirsi Ali, Candace Owen, Kemi Badenoch, Kamala Harris, Nikki Haley, that Wealthy Fake Kenyan Refugee installed as a Mayor in Northern Ireland, and countless others. These women never marry their own, but use White Men as a catapult to power, while sneering at White Men and the patriarchy.
As a Catholic, like Truss, Tugendhat, Rees-Mogg & others, Badenoch can only hold the post of Prime Minister ILLEGALLY, as Truss and Sunak have done, because the LAW OF THIS LAND states that no Catholic, Jewish, or anyone other than a PROTESTANT may hold the posts of Monarch or Monarch’s Prime Minister.
All of these ILLEGAL CANDIDATES, along with Mass Invasion from the Third World, are part of the Globalist/Communist/Vatican Battering Ram against the greatest nations of the West, which were all founded by Protestants.
Has anyone heard of Lee Martin Taylor? Neither had I until Sunak’s Dunkirk moment. Curious where he was seeking reelection, I discovered it was Richmond and Northallerton Constituency in Yorkshire, and the boundaries were changed last year to ensure reelection. I also discovered that the Reform candidate was Mr Taylor. But who is this unheard of person? He was born in Yorkshire, where he lives. He served in the British Army for more than twenty years until he retired early this year (heavily decorated after, among others, having served a tour of Iraq and two tours of Afghanistan). As I do not share Toby’s faith in Farage and Reform, I thought I’d put them to the test. I offered Reform HQ £1000 on condition that that they would give half of it to Mr Taylor’s campaign.
I’m still waiting for an answer, reenforcing my opinion that Mr Farage is more than meets the eye.
Of course, I will change my opinion if someone answers my question: Why does Reform wish to keep Sunak as an MP and do they not support the only person who can dislodge him?
Wow! Good sleuthing, Curio! There can be no question that Lee Martin Taylor is the best man for the job, but I thought gerrymandering was now illegal, especially when boundaries were changed by a sitting, though illegal, Prime Minister to ensure his own victory!!!?
The awkward thing about the Reform party financial funds is that they are in the charge of a Persian-Indian bloke, and one news item said that of the £11 million pounds in the original fund, only £1 million remained. I haven’t heard any more about that, but I hope they strongly support Lee Martin Taylor in his home county of Yorkshire.
Let’s remind ourselves and all true Yorkshiremen of his name, the one who will boot Smarmy Sunak out of Parliament:
Decorated war veteran LEE MARTIN TAYLOR.
Much obliged for the encouragement.
F&F disclosure. Some aeons back I worked in Darlington for a year, often visiting Richmond, an absolutely idyllic part of Yorkshire. Very fond memories.
Does anyone remember the Brexit Club that you had to pay for and in return you get some sort of vague exclusive invites. That was just after the election in 2019, a cushty picture of Farage & Tice sat in a posh room laughing and giving the impression that you would be some sort of exclusive guest. Just a last minute attempt to make some dosh I suspect.
Thanks for the post. Brilliant work.👍
Kemi a staggering disappointment in person. Pro NetZero, CBDCs, WHO landgrab. In short, a globalist. And hit a lowball in discussion. Unforgivable, and untrustworthy.
Sorry Toby you’re a good man but they’re all part of the same old same old brand. Also apart from anything else where the hell was Farage during the scamdemic? No I’ll be voting for an Independent if there is one otherwise it’s a spoilt paper from me – a plague on all their houses.
What the country needs is a constituency by constituency guide to tactical voting.
Who to vote for to keep party X, Y or Z out.
Or to reduce the disaster a massive Labour majority will cause.
I am with you. It has been “None of the above” for many elections. Voting for the main parties is like buying dinner for your jailer. I will vote for reform if I have the opportunity, next, any independent, next “None of the above”. This country has become corrupt to the core. The main parties will not address this because they are involved in it. Politicians on both sides have sold this country to the corrupt corporations and WEF via international agreements to out source decision making on arming groups around the world with no accountability, medical reactions to illness, corrupt banking practices that see our economy asset stripped, an education system that stifles debate. Etc etc
Toby assumes Nigel will want to join a weakened Tory party, I think not. He’ll want to swallow it in to a new right of centre party, and spit out the dead wood.
I will vote Reform because we need to move away from the deluded politics involving ever-increasing government and institutional capture that has become the norm. More of the electorate need to become politically active, ask questions and support wholesale change if we are to avoid economic chaos, anarchy and painful revolution. The writings of David McGrogan are excellent regarding our descent into political apathy and big state-cum-corporatist tyranny.
I refuse to use labels such as “left”, “right”, “conservative”, “progressive”, etc. We the people from all walks of life need to work together and make our voices heard to demand change. Reform may not be perfect but they are a start.
I’m voting Reform because I want the Treacherous Tories to be obliterated. It’s as simple as that.
Tories is a misnomer – they have been Social Democrats for years. Reform are also part of the system. We need to stop party politics and vote for whoever we think will serve our constituencies best.
Reform is a useful tool to despatch the tories into oblivion.
I note that your analysis ignores people like me, a long term natural conservative and conservative voter, not a red-wall or other 2019 newcomer that is consumed with a deep sense of betrayal and one I am convinced is and has been a long standing playbook for the Conservative Party. I also note that you have not referenced the leadership’s anti-conservative selection shenanigans.
It is impossible for me to believe the party leadership and maybe half the supposed firebrands to which you refer are not longer-term social democrat plants.
The ordinary British voting citizens have been and are being ripped-off. They are watching as their country is handed to foreigners invited in their millions over very short periods under ‘conservative’ leadership that has deliberately failed to deal with the deep rooted impact of Britain’s disastrous membership of the EU and its “freedom of movement” and “ever closer union”. FoM delivered a never ending stream of wage (and salary) depressing foreign labour that morphed business models so greatly that supposed conservatives have consciously fostered/managed a mass invasion to pleases BIG, predominantly foreign business with corporate welfare and related privatised profit and socialised costs.
The Conservative Party is dead to me and Boris surely cannot be seen as its saviour? He failed to grasp the Woke nettle and then ramped-up ‘legal’ (dear me this shows what state our judicial system has become) mass migration and on his way out, perhaps a bribe to show he too is one of the Wets.
I agree Kemi is impressive and believable but how can anyone feel sure she is not the most talented of the fakes.
Boris couldn’t run a tap and should be kept well away from politics as should his stablemate Camoron. Why are we plagued with people like them?
I will also be voting Reform – I want these fake tories destroyed. 14+ years in office and what have they done to this country? It makes me sick to think about it. Sunak has been a useful puppet for the WEF and his ineptitude has hastened the demise of the conservative party and for that I thank him – now he can clear off to bluidy Florida or wherever he has decided on settling next.
After 50 years of voting for the person and not party I will be voting Reform for the simple reason that they seem to be the only Party committing to getting rid of Net Zero madness. I consider that this is, or shortly will be, the most important issue in our day to day lives.
Delighted you’re going to be voting Reform, Toby.
But Nigel really is not a “right wing firebrand”.
Firebrand, maybe. But he is firmly in the centre right. Read Reform’s policies on their website.
Kemi is great but a non starter as Tory leader, not least because she has supported Sunak and spoken out against Reform.
Don’t forget: Nigel is never going to lead today’s Conservative Party. He will only become leader of the centre right after the demise of the Conservative Party, including the social democrats who lead it, and a complete realignment in the British centre-right.