
There follows a guest post by the Daily Sceptic’s in-house doctor, a former NHS consultant now in private practice. He’s looked at the latest NHS England data and points out that there are fewer than half as many Covid patients in English hospitals than there were this time last year, not 14 times as many, as was claimed recently.
On Friday November 26th, the South African Institute for Communicable Disease released a statement in relation to the Covid variant now referred to as Omicron.
The variant had been first detected on November 12th from specimens collected in Gauteng Province and the molecular structure was characterised by November 22nd. The statement from the South African Institute on November 26th considered that the Omicron variant did not meet the WHO criteria for being either a ‘variant of interest’ (VOI) or a ‘variant of concern’ (VOC). Yet less than 24 hours later, the WHO had classified the Omicron variant as a ‘variant of concern’.
The definitions of variant classification are clearly laid out by the WHO. Classification of a ‘variant’ usually proceeds stepwise, from VOI to VOC. Classification of a VOI requires data collection to verify different effects of the specific variant and upgrading it to a VOC requires evidence that the variant is definitely evading prior immunity or making humans more severely unwell than previously.
I cannot find any evidence in the open sources to date that shows infection with the Omicron variant carries any greater risk of hospitalisation or death than the currently dominant Delta variant. One obvious possible reason for this absence of evidence is that the variant was only identified very recently. Given the known time lag between infection, the development of severe disease and hospitalisation, there has not been sufficient time to assess whether this particular new strain is clinically significant or not. It might be, but we just don’t know.
Simply put, it is not yet clear whether this new variant is a bad one (more infectious and more lethal) or a good one (more infectious but less severe). Opinion is clearly divided on how this situation will develop. Dr. Angelique Coetzee, the Chair of the South African Medical Association, speaking on Marr on Sunday 28th said that so far all the known patients infected with Omicron had very mild symptoms and none of them had been admitted to hospital.
Looking at the ‘charts that matter’ this week, we see a continual reduction in Covid admissions to hospitals (graph one). It’s important to note that all of these admissions are likely to be the Delta variant rather than the Omicron variant.

Graph two shows that the total number of Covid positive patients in hospitals also continues to fall – from this we can reasonably infer daily discharges are higher than daily admissions.
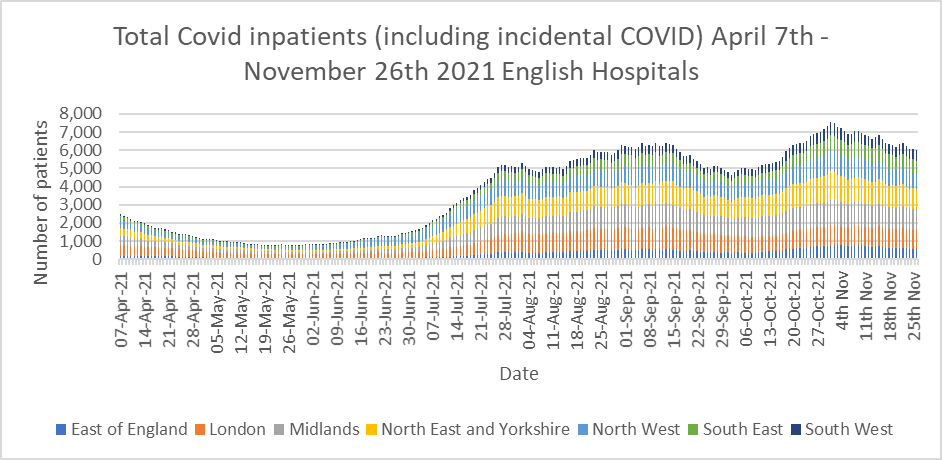
The Pritchard ratio (the number of patients in hospital with Covid divided by the number at the same date in 2020) is approximately 0.43 – so there are currently fewer than half the number of Covid inpatients compared to this time last year – not 14 times as many. Covid positive patients occupy approximately 4% of NHS hospital beds.
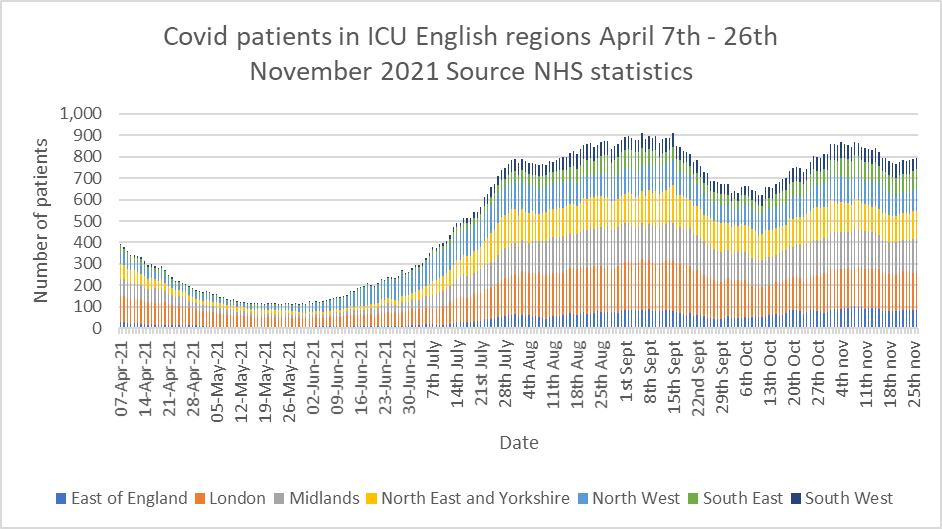
ICU numbers show a similar pattern (graph three).
I was encouraged to see in last week’s report from the Intensive Care National Audit and Research Centre (ICNARC) that vaccination status has now been included in the data. The absence of this important information from such a reliable and credible audit has puzzled me for months.
Table 16 of the report shows that overall, 75% of patients in ICU with severe Covid are unvaccinated and there is a gradient of incidence with increasing age – 90% of admissions in the youngest age group (18-29 years-old) were unvaccinated compared to 39.3% in the over 70s.
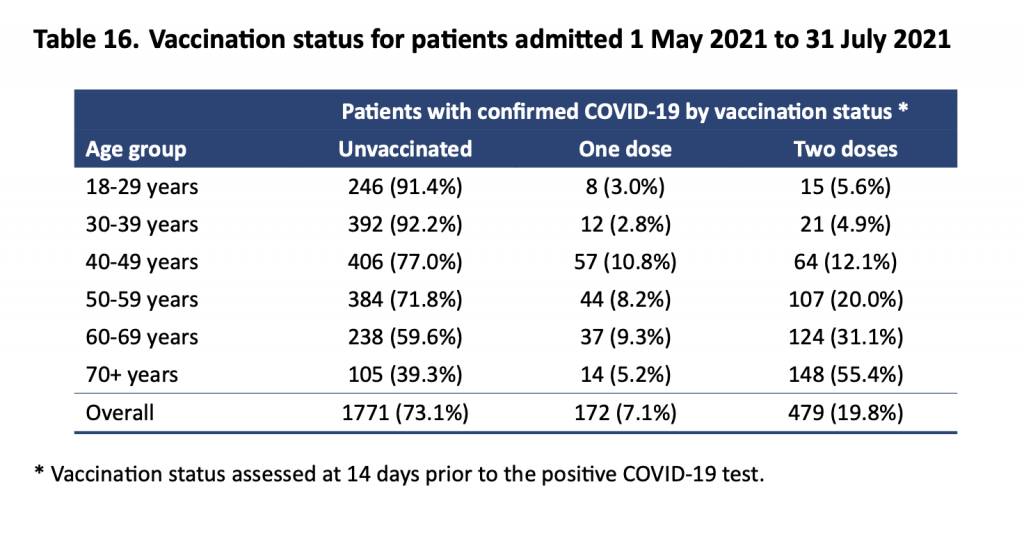
Nevertheless, the data presented only refers to the period from May 1st to July 31st. I find it surprising that there isn’t more up to date information available. Clearly, the proportion of the population double vaccinated at the end of November is likely to be higher than it was at the beginning of May and that may have a significant bearing on the ICU admission figures. Further, a casual glance at graph three above shows that the incidence of ICU cases between May 1st and July 31st is very different to the period from September 1st to November 26th. Surely, there must be more up to date information about vaccination status of ICU patients available? Why not publish it, unless it tells a different story to the one the NHS wants to tell?
Overall, the trends as we go into winter are fairly stable or on a gradual downslope. The numbers are substantially better than this time last year. Professor Chris Whitty acknowledged as much at the Downing Street press conference on November 27th. The widely predicted resurgence of influenza has so far failed to materialise. The National Influenza and Covid Surveillance report shows extremely low levels of both flu and Respiratory Syncitial Virus (a common winter respiratory infection in children) – both far lower than at this stage in prior years.
In politics, as increasingly in clinical medicine, decision makers are fixated on blame – as in who gets it when things go wrong.
The reimposition of travel restrictions and mask mandates in England in response to the identification of the Omicron variant marks the crossing of a new threshold in ‘non pharmaceutical interventions’. At the start of the pandemic, the WHO stated that societal restrictions should be regarded as a last resort – mainly because of the known economic and wider adverse public health consequences.
We have now come to a situation where societal restrictions are imposed on the basis of fear about what might happen, rather than a rational analysis of what has happened and is currently happening. Patrick Vallance acknowledged in the Downing Street press conference that, as yet, there is still no clear data suggesting Omicron is more dangerous than the Delta variant.
Simply put, the Government now reaches for societal interventions as the first resort to a perceived public health threat, rather than as a last resort. This is a worrying precedent as it opens the door to arbitrary restrictions by the executive on the population based on opinion rather than quantifiable facts. I’m sure the implications of that shift are obvious to readers.
Stop Press: According to the Telegraph, backbench Conservative MPs who are sceptical about the effectiveness of NPIs are asking for a House of Commons vote about the new restrictions on Tuesday. Read more on that story here.










To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
Has it occurred to anyone that the reason they are going to war against the moronic variant may be precisely because it may be as serious as a mild cold and may outcompete the other variants? Perhaps if this became dominant it would be game over for the scam.
They aren’t going to war against a virus.
They are going to war against the population
The goal is to enslave the population.
“Stop Press: According to the Telegraph, backbench Conservative MPs who are sceptical about the effectiveness of NPIs are asking for a House of Commons vote about the new restrictions on Tuesday. Read more on that story here.”
Yawn! I think we all know how that will go by now, and how utterly useless MPs have,been. collectively, throughout this episode.
I emailed my MP yesterday requesting that he ask for all current research on the efficacy and risks to physical and mental health of mask wearing before he votes. I also supplied some details of latest findings.
Of course he won’t, he’s a complete brown noser but he’s had the email and I’m getting quite a collection of the data he has ignored, all of which will be sent to any inquiry panel or prosecution team, I’m hoping for the latter.
Name and shame. My MP is Greg Clark, Tunbridge Wells.
Mine is Kevin Foster, Torbay.
Alex Cuntingham, Stockton North….unashamedly pro-mask, pro-lockdown and pro-immigration.
Depends how you want to define it, but i’d class myself as pro-immigration as believe there are logical, economical and ethical reasons to be so.
Masks and lockdowns however have no reasonable justification so not sure why you’ve conflated them with immigration.
I expect he’s done it because if the agenda is globalist, they go together.
Though I understand your view.
We will lose the vote, if there is one, and MPs have been close to useless, but I think asking for a vote and getting a debate is still worthwhile and important because it makes the evil cabal in charge realise, even if briefly, that someone is watching, and it goes some way towards pushing the sceptic POV back into the mainstream where it belongs, and gives wavering MPs a small opportunity to come over to our side. A tiny benefit, but still a benefit.
But there’ll probably only be one MP who shares the truth in the debate. Like every time before.
And also helps the awake man on the street – “See, they don’t even debate it.”
It forces them to show a loathing of open, democratic discussion.
That’s worth doing.
They are snakes. Below is an exchange I had with my MP. He didn’t bother to answer my final question. Rearranged into chronological order. He appears to think I’m stupid.
From: Redacted
Sent: 23 October 2021 22:14
To: GIRVAN, Paul
Subject: Covid Pass
Dear Mr Girvan,
I am writing as your constituent to express my concerns and objections to the proposed Covid Pass and to ask you to vote against mandatory Covid Passes in the forthcoming Parliamentary vote…(letter of about 10 paragraphs continues to explain my concerns, name and postal address included)
Yours sincerely,
Redacted
On 26 Oct 2021, at 14:57, Paul Girvan wrote:
Dear Redacted
Many thanks for your email. I can confirm that I am not in support of government legislation to introduce a mandatory covid passport.
I trust this is acceptable and answers your concerns.
Kind regards,
Paul
From: Redacted
Sent: 26 October 2021 15:32
To: GIRVAN, Paul
Subject: Re: Covid Pass (Case Ref: Redacted)
Dear Mr Girvan
Thank you for your response. You didn’t address my central question. Let me rephrase it. Will you vote against Covid Passes in any upcoming Parliamentary vote? And if not, why not, given your view stated below.
Kind regards,
Redacted
On 26 Oct 2021, at 16:05, Paul Girvan <paul.girvan.mp@parliament.uk> wrote:
Hi Redacted
I am not in favour of the government legislating in relation to this issue and will therefore not support any government vote to implement covid passes.
I hope this clarifies.
Best wishes
Paul
Dear Mr Girvan,
Thank you for your response. Let me spell it out for you. Will you abstain in a vote, or will you vote against the government? Us little people have grown accustomed to political nuance. Perhaps you can give me a straight answer this time, you know exactly what I am asking.
Very sincerely,
Redacted
Very good.
Girvan gave a fine example of the use of the verb “to palter” there.
“Simply put, the Government now reaches for societal interventions as the first resort to a perceived public health threat, rather than as a last resort. This is a worrying precedent as it opens the door to arbitrary restrictions by the executive on the population based on opinion rather than quantifiable facts. I’m sure the implications of that shift are obvious to readers.“
How is this any different to what they did in March 2020?
We didn’t know the full risks of the virus in March. A short precautionary lockdown made sense.
We’ve known that the virus isn’t particularly dangerous to the non-vulnerable since late April — the universal biocontrol measures since then don’t make sense; since then only targeted measures should have been used.
The craziness of the whole situation is that they’ve actually locked down vulnerable and non-vulnerable in step. This has led to the bonkers situation of having a universal lockdown one month with vulnerable octogenarians allowed to go and have a coffee in town the next month while at the same time completely non-vulnerable children’s education continued to be disrupted. The whole response has been driven by stupidity, not science or logic.
I disagree, we knew before the first lockdown that it was not the deadly disease they were making out due to it being removed from the HCID list, and the data coming from the Diamond Princess.
The response is not driven by stupidity it’s driven by the need to bring in vax passports.
The Diamond Princess is the one single item of data needed to understand this virus in terms of what the man in the street needs to do about it. That is, absolutely nothing he didn’t already do for any other respiratory virus.
Every other graph and list of numbers is pointless fluff. It just distracts from the lesson of the Diamond Princess.
And yet it appears to have been memory holed. I read something else by I think an American military doctor who said the Taiwanese had done a deep dive into covid mortality early on and discovered a consistent occurrence of Vitamin D deficiency. She was advocating for vitamin D3 with K2, zinc, selenium, N acetylcysteine, IVM, HQC etc and was therefore also memory holed.
One effect of removing covid from the HCID list was that it is no longer possible to get emergency use authorisation for repurposed drugs such as Hydroxychloroquine or Ivermectin.
Unintended side effect, or part of a sinister conspiracy?
“We’ve known that the virus isn’t particularly dangerous to the non-vulnerable since late April —”
W knew that in March.
How do you determine the severity of any new variant if everyone in the ‘control’ group has already received a covid jab and those jabs are working as claimed?
And how do you determine the ‘efficacy’ of any new jabs against variants without a proportion of the population un-jabbed for comparison? If we’d all ‘done a Gibraltar‘ we’d have seriously compromised the ability of scientists to do science.
The vaccine programme could be read as a modern day inquisition. It’s an ingenious way of establishing who is prepared to accept the new false ideology and who isn’t. Not dissimilar to the purges seen in 20th century totalitarian systems. We have identified ourselves as fifth columnists. The question is how do the present day tyrants deal with us without appearing like tyrants?
This is true.
You demonstrate your acquiescence by believing their lies.
As the lies become more and more unbelievable, you signal your further obedience by believing them.
This is total satanic control.
Whatever the dominant partner demands, however absurd, it is complied with by the faithful.
You’re right, but also the scammed save face by daring not admit to the scammer they know they’ve been scammed, like this guy.
“I don’t understand how people can be so gullible and naive.” (comment)
Yes indeed, quite remarkable isn’t it? I wonder if that comment was made by someone who took a certain injection this year…..
Omicron. Love it. It’s sexier than Delta. It’s deadlier than Delta.
next ‘variant’?
Captor.
There’s a third analysis on this variation that the good doctor misses. It might be worse, it might be better, or it might as I suspect by entirely fabricated for use a prop in fear porn.
Given that it takes some considerable time, and a lot of money, to work out what “variant” someone has, it strikes me that there are many, many porkies being told here.
I think it should be pretty clear to everyone now:
Admissions/cases/deaths/ICU going up = unvaxxed/new variant
Admissions/cases/deaths/ICU going down = vaccines/boosters/NPIs/our wonderful NHS
Hospitals in USA and in first world countries are refusing life-saving Ivermectin treatment even with court orders. Big Pharma doing everything they can to jab us no matter what, while alternative COVID cures EXIST! There happens to be heavy censorship who are looking for these treatments. The Research Is Clear: Ivermectin Is a Safe, Effective Treatment for COVID. Get your Ivermectin today while you still can! https://ivmpharmacy.com
THE WHO declared a global health pandemic on January 30, 2020
666 days later
The WHO classified the Omicron variant as a VOC on November 26, 2021
Correction :
That should have read :
( The WHO declared a pandemic on March 11, 2021 )
Good spot if that’s correct ModeRNA I may have to use that.
Great piece. Thank you, Dr DS.
Incidentally, I like “incidental Covid”. Great phrase. We should all use that as much as possible in speech and writing: “But so many of the hospital deaths they’re talking about are just incidental Covid aren’t they? Like Captain Tom.”
It puts “with Covid” deaths back in their rightful box.
I fear someone noticed their PPE (mask) profits starting to dip a teeny bit and sensed an air of freedom/liberty creeping back into the mostly cowed and terrified populace. I also sense concern from the evil bastards pulling the strings.
This feels a bit like desperation coming from them. Way Over the top lies and repeat freedom grabbing. It’s as if they know even the ‘moronic’ are becoming a wee bit immune to their by now standard filth and lies. They’ve had to ramp it up a notch or two to get the same effect. You know, a bit like alcohol or drugs.
Ironically, we the awake seem to be getting more and more sensitive to the tsunami of 100% proof Bullshit we are being waterboarded with. The more we have to swallow, the less tolerant we become.
Whatever will they come up with next, eh?
Bandstand in Blake Park – Bridgwater – Somerset. Every Sunday 10 am meet like-minded people who can see the bleedin’ obvious.
Telegram: Connecting Warriors. MeWe group Connecting Warriors
Other venues are available all over the country, but you won’t find their details on MSM.
If unsure A good start would be Telegram groups for your area. “A Stand in the Park – Bracknell & Wokingham”. Via posts from our very own ‘Lockdown Sceptic’ A regular here on DS
”…whether this new variant is a bad one (more infectious and more lethal) or a good one (more infectious but less severe)…”
So what happened to the very definitive statements we’ve been hearing all through this ”pandemic” that viruses mutate but become more transmissible but less deadly? Shall we assume that was all tripe then?