There follows a guest post by ‘Amanuensis’, an ex-academic and senior Government researcher/scientist with experience in the field, who has undertaken a re-analysis of ONS data on deaths by vaccination status and concluded that vaccine effectiveness against death has been significantly overestimated owing to a failure to take into account the delay between infection and death. His analysis also uncovers an alarming spike in Covid deaths following vaccination during a Covid surge which, he says, needs urgent investigation. This post is also available on his Substack page.
Recently a blog post was brought to my attention. This was a very interesting piece of work that is directly related to a previous post of mine analysing the deaths by vaccination status figures published by the Office for National Statistics.
In Norman Fenton’s excellent analysis he considers the impact of a delay in the reporting of a death on the shape of the deaths curve; he finds that such a delay during a vaccination campaign will naturally result in the creation of a spike in unvaccinated deaths and an under-estimation of deaths in the vaccinated – indeed, he notes that you would see that spike in deaths even if the vaccines do nothing. If you want to read more about his analysis his site can be found here – and I recommend at least a quick skim of his work because I’ll be building on the fundamentals of data analysis that he considers.
However, there is a small but significant flaw in his argument; that there was a delay in reporting deaths which has then resulted in the spike in cases that we see in the data. Unfortunately, a check of the data source reveals that the deaths data were given by the date at which the death occurred, not the date at which it was reported. Thus there is little scope to introduce a delay in the data using this mechanism.
This then seems like a conundrum – we have a mechanism that might explain the spike in deaths in the unvaccinated apparent in the deaths data for last spring, but we can’t explain how the necessary delay might have occurred. But there is a potential explanation.
To understand what might have occurred, we first need to explore the timescales of the progression of Covid disease.
We know that Covid disease follows three broad stages, as illustrated by this figure (from Oudkirk et al, 2020):
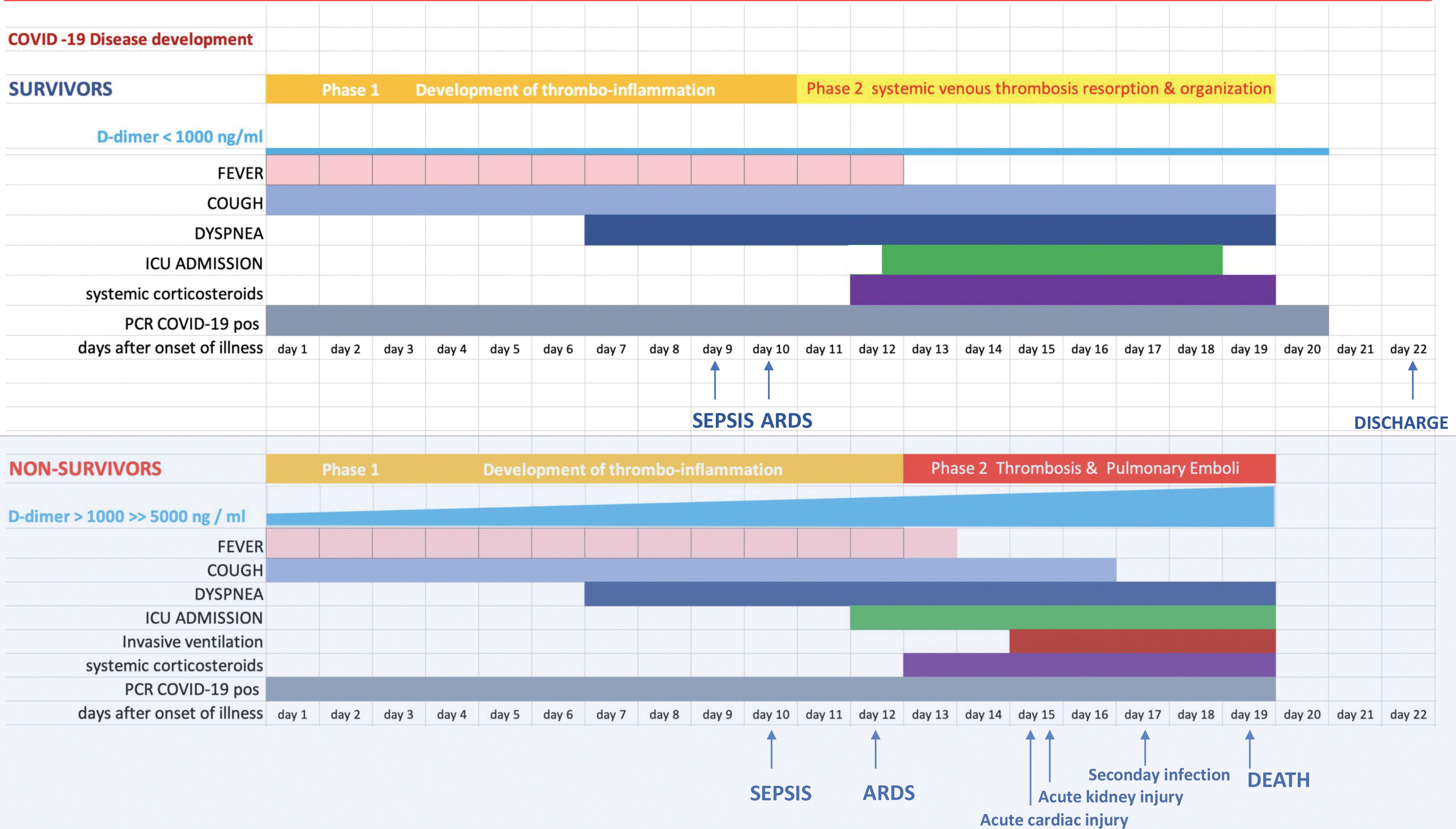
As can be seen in the lower half of the figure, first comes a mild symptomatic period lasting approximately seven days. Most individuals recover at this point, but in a minority there next comes a period where there is a significant shortage of breath (dyspnea – this is when medical assistance is often sought), and in a subset of those individuals this is followed by a period of significant illness and, potentially, death. The time period between symptom onset and death, if it occurs, has a median value of approximately 19 days.
On top of that, there is a short incubation period of three to four days between the point of infection and the onset of symptoms. Adding this period on gives a median duration between the point of infection and death of approximately 23 days, or three and a bit weeks.
The important point in this analysis is that it is not correct to compare weekly death statistics with the vaccinated population at the week of death; for this analysis the important point of the disease progression was the point of infection, not the point of death. Thus we should be comparing each week’s deaths with the vaccination numbers three and a bit weeks prior, i.e., the point in time when the infection that led to the death will have likely occurred.
It is important to point out that this isn’t a nuance that is ‘worth a try’, like the potential for the deaths to be reported a week after they occurred. This is the only correct way to interpret these data, and to use the vaccination numbers for the week of death is incorrect. Alas, I have realised this too late, and can only apologise for the misleading statistics I discussed in my earlier post – you can be sure that I’ll punish myself with a glass of wine later.
I shall discuss how this new factor affects my past analysis on the non-Covid deaths in a later post, but for now – how does the use of the vaccination numbers at the likely point of infection, rather than the point of death, affect the analysis of deaths with Covid?
In this post I’ll show data from week four to week 20 – week four because those dying in week four will have caught Covid in week one of 2021 and we don’t have relevant data prior to week one, and week 20 because the primary impact of this delay will be to affect data during the vaccine rollout – I’ll cover later data in a separate post. I’ll be showing data for unvaccinated and for those with a single jab, and will show the data for no delay and a three week delay. Note that I’ll be discussing deaths per week per 100,000 individuals, not simply ‘deaths’.
Just to explain briefly how the following graphs will be laid out, I have plotted the adjusted deaths per week per 100,000 individuals against the week of the year. I note that the periods during which vaccinations were given are not shown; they will be earlier for the older age groups (indeed, many of these were vaccinated in December 2020) and later for the younger age groups. The data for the unvaccinated is given in red, with open circles for no delay and filled circles for the data with the three week delay. Similarly, the data for those given their first dose of vaccinate is given in blue, with open circles (no delay) and filled circles (with delay).
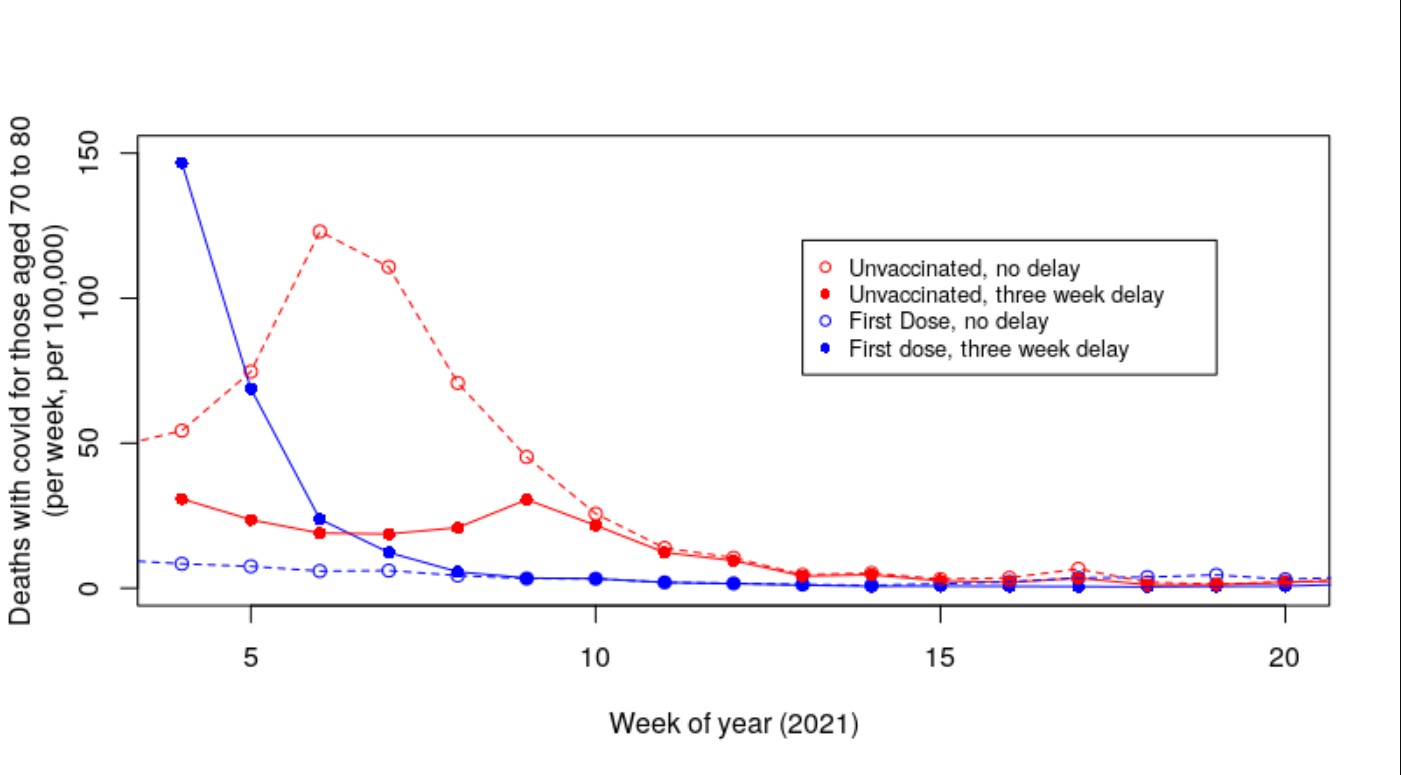
Let’s start with the updated graph for deaths per week per 100,000 in those aged over 80:

It can be seen immediately that the introduction of a delay to compensate for the time between infection and death has had a significant impact on the shape of the curves in the graph. First consider deaths per week per 100,000 individuals in the unvaccinated (red data points). The introduction of the delay has reduced deaths in the unvaccinated at week four from approximately 800 per day to approximately 200 per day. We have also increased deaths in those single-jabbed from approximately 80 per day to approximately 200 per day. In the original data the deaths in the unvaccinated fell rapidly to approximately week 10, but in our new data with the delay the data for deaths in the unvaccinated is rather flat with a small peak at week seven.
It is worthy of note that there is still a net excess of deaths per week in the unvaccinated compared with those that received a single dose of vaccine, but that the difference is substantially reduced. Also noteworthy is that at week four the data for those having received a first dose isn’t flat – perhaps deaths from Covid in the vaccinated at earlier time points were higher? Hmm – what about the data for those aged 70-80 who were vaccinated just that little bit later?
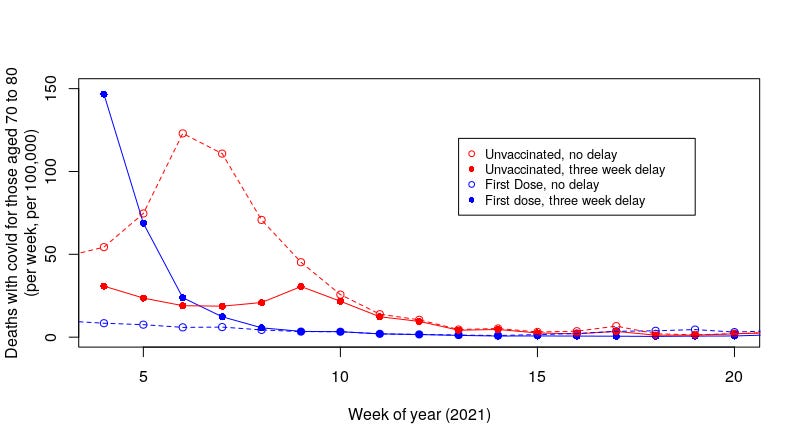
That’s a pretty scary graph. With the introduction of a delay to compensate for the time between infection and death we’ve eliminated the majority of the peak in deaths per week per 100,000 that we saw with the uncompensated data. What’s more, there is now a pronounced increase in the deaths of those with a single dose of the vaccine at the far left of the graph. It should be noted that these individuals were vaccinated after those aged over 80; thus we are getting closer to the point of vaccination in this graph.
And the data for those aged 60-70?
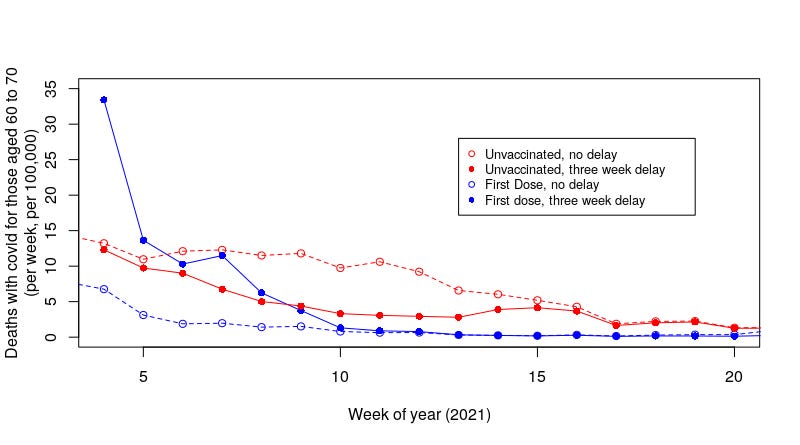
That’s a little less impressive, but we still see a substantial decrease in deaths per week per 100,000 in the unvaccinated and a substantial increase in deaths in the weeks after the vaccinated had their first dose.
I note that we’re still seeing a peak in deaths at the start of the study period, whereas the main roll-out of the vaccines in those aged between 60 and 70 was later in July, when the Covid wave was receding rapidly. The peak in cases in the UK was around January 8th, and as testing was usually instigated by symptomatic disease which starts three to four days after infection; it is likely that the point of peak infections was in the first week of the year. Thus it is likely that what we’re seeing in the graph for deaths in those aged 60 to 70 reflects vaccinations before the main roll-out of the vaccine. This is probably also true for the data for those aged between 70 and 80. This suggests that the main risks came with vaccination during the peak of that infectious wave, and that risks were lower after it. Of course, this aspect will equally affect the unvaccinated, and thus the comparison between the two groups holds.
To summarise what we’ve found in this new approach to the analysis: it appears that introducing a shift in the data (the delay) to try to work with the date of infection rather than the date of death significantly reduces the number of deaths seen in the unvaccinated over a sustained period of time and identifies a period of increased risk of death for a shorter period after vaccination.
Because we have shifted deaths per week per 100,000 lower in the unvaccinated and higher in the vaccinated the obvious question is – what is the net position? This is rather difficult to calculate given the data we have, however, we can gain an indication of the net position through a comparison of the sum of all the individual data points over the study period (weeks four to 20, 2021):

It should be stressed that this isn’t a prediction of the number of actual deaths per 100,000 during the study period; it is merely an attempt to compare the impact of our analysis on the vaccinated vs unvaccinated. Nevertheless, the two pairs of summed-deaths per week per 100,000 highlighted in green suggest that the vaccines’ impact on deaths was not as high as has been suggested. I’d note that although the data suggest that the vaccines made things worse, I think that might be an over-interpretation of the data – certainly, there is a significant shift in the unvaccinated versus vaccinated population during this period that doesn’t support a simple interpretation of ‘deaths in the vaccinated were higher’). Moreover, the impact of a proportion of the deaths being with-but-not-of-Covid will likely remove at least some of this effect (I’ll come back to this point). Also, the analysis is sensitive to the delay between infection and death – a shift in timescale could have been introduced by the Alpha variant prevalent during this time, changes in treatments for the vaccinated and/or changes in disease progression introduced by the vaccines themselves.
I note that the summed death data for those over 80 (highlighted in yellow) still shows a net benefit of the vaccine – I suggest that this is because those individuals aged over 80 were vaccinated before the study period. Thus it is likely that they did have a similar peak in deaths but during weeks one to three of 2021 and the peak is not seen in our analysis; if this is the case then it is likely that those aged over 80 also saw a lower net benefit from vaccination.
The observant amongst my readers will note that I have not addressed the data for those aged between 10 and 59 found in the U.K. ONS release. As I discussed in a previous post, this is a very wide age range and the variation in death rates in this group is too great to be able to perform a meaningful analysis. It would be nice if the UK ONS could release future data with more granularity in the 10 to 59 yrs age range, but for now these data cannot be considered useful for analysis.
The introduction of a shift in the data to compensate for the delay between infection and death has had a significant impact on the data for deaths with Covid. But is it correct?
I am a little concerned about one aspect of these data – the problem being the usual one of ‘deaths with Covid’. The compensation mechanism I have used is only valid for people dying from Covid – those people dying of something else while infected with Covid should not have the compensation applied to them – well, they shouldn’t be included in the data at all, but once the with-but-not-of data are mixed up with the with Covid deaths application of our delay compensation mechanism will introduce artefacts into our data that will increase the risk that we’re now underestimating the benefits of the vaccines. Unfortunately, of course, we don’t have separate data for with and from Covid deaths.
As it stands I believe that the truth lies somewhere in between the original analysis and this analysis with a compensatory delay, but where in between? Actually, I’m not sure it matters that much:
- If there are many with-but-not-of Covid deaths then this compensatory mechanism shouldn’t be used and thus we have to go back to our original analysis by the date of death. However, if most deaths were with-but-not-of Covid then really the vaccines aren’t particularly necessary;
- If there aren’t many with-but-not-of Covid deaths then the application of the necessary compensatory delay results in the vaccines looking rather ineffective.
No matter which way you look at it the vaccines don’t come out well.
For what it is worth, I believe that approximately one third of all with Covid deaths were actually from some other cause and the individual just happened to be Covid infected. If this is the case then the strength of the effect identified in this post will be lower than I have found. Nevertheless, it appears that there would still be a significant effect even with the removal of the with-but-not-of deaths; the vaccines are likely to offer some limited protection against death, however, the increased risk of death during the period immediately after vaccination is likely to remain.
I believe that this approach to the analysis of the U.K. ONS deaths data for early 2021 strongly suggest that there were fewer deaths in the unvaccinated group than has been considered to be the case. Also, importantly, there were likely to have been more deaths in those given their first dose of vaccine during this period, particularly in the first few weeks after vaccination and particularly during an infectious Covid wave.
This latter point is important. It suggests that in general there appears to be a an increased risk of death immediately after receipt of the first dose of Covid vaccine. If this is the case then vaccination during last winter’s Covid wave will have increased the risk of death in those vaccinated. This work is only a preliminary investigation into incomplete data; however, it reveals a very concerning result – more data and analysis must be undertaken into the risks suffered by the vaccinated in the period immediately after vaccination. Until such analysis shows the vaccines to have low risk in this period, it must be recommended that:
- Individuals being given their first dose of Covid vaccine should be warned that they may have a period of significantly increased risk from Covid over the weeks following vaccination and that they should take additional precautions to protect themselves from disease, including partial self-isolation.
- Mass vaccination during an infectious wave should be discouraged; there are increased numbers of infected individuals and thus increased risk in the crucial few weeks post vaccination.
In addition, further investigatory work must be undertaken to identify the real-world benefits of the Covid vaccines – to introduce risk without benefit is foolhardy.










To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
These vaccines are killing people – lots of them. It’s all over social media, it’s all over Telegram where there are thousands of first hand accounts, it’s even all over ‘serious’ business sites like LinkedIn where I am seeing more and more testimonies daily about vaccine injury and deaths in my feed (although these are quickly deleted – Gates owns LI like everything else). I refuse to believe this story is beyond the wit, intelligence or curiosity of journalists at the BBC, Guardian etc in terms of joining the dots here and writing about this. The only conclusion one can therefore draw is that this is a massive coordinated cover-up and that senior execs at these and other media outlets are being leaned on. By whom, specifically, is the only question.
A cover-up is when something is officially admitted to have happened, and then pressure is put on witnesses afterwards (during an investigation or at least when an investigation is being considered) to keep their mouths shut, make false statements, “lose” documents, change what they said originally, etc. There are many examples.
We are nowhere near the stage of a cover-up yet.
As for the Guardian, I’m boycotting it because the day after the Austrian cops started demanding people’s papers in supermarkets, in order to deny access to the unvaccinated, the Guardian said the checks were “routine”. Those who do PR work for fascism shouldn’t expect the rest of us to pay attention to their scribblings.
Speaking of Austria, the “UK-Austrian Parliamentary Friendship Group” consists of Peter Bottomley, “Lord” Anderson, “Lord” Tyler, “Lord” Dubs, “Viscount” Waverley, and Tim Loughton.
A brief look at some of their registered interests didn’t unearth any Austrian business connections, but “Viscount” Waverley has received state decorations from Kazakhstan, Kyrgyzstan, and Colombia, and he advises a company called Smarter Contracts Ltd which is involved in the blockchain, so one might hazard the guess that there are no flies on him where making money is concerned. Funnily enough he’s asked questions about blockchain-related matters in the Lords too.
Gates owns the Guardian and the BBC. They both take millions off the Great Depopulator.
“The important point in this analysis is that it is not correct to compare weekly death statistics with the vaccinated population at the week of death; for this analysis the important point of the disease progression was the point of infection, not the point of death. Thus we should be comparing each week’s deaths with the vaccination numbers three and a bit weeks prior, i.e., the point in time when the infection that led to the death will have likely occurred.”
exactly – probably 4 weeks
I agree with the argument that vax effectiveness against infection should be calculated by the vaxed/unvaxed ratios at the time of infection rather than at the later time of detection. However, I am less clear on why the effectiveness against death should be calculated from the ratios at the time of infection rather than the time of death. I guess the argument is that the percentage of vaxed could dramatically increase during the 3 week course of the illness – so it is invalid to base the calculation on the somewhat arbitrary ratios at the time of death – rather than the clearly defined ratios at the time the deadly infection occurred. But I thought this point could have be made more clearly in the article. It’s a subtle point which needs careful explanation rather than just stating it as an obvious fact.
and also have to remember that the unvaccinated and vaccinated are different groups apart from the vaccination.
vaccinated are worried well – unvaxxed will have a lot of people on the edges of society
if the Austrians are mandating it, its got to be bad for you
“For what it is worth, I believe that approximately one third of all with Covid deaths were actually from some other cause and the individual just happened to be Covid infected.”
It’s likely it’s even higher than a third which allied to the obvious fact that the jab is causing morbidity and mortality makes the experimental jab dangerous and totally unnecessary.
95% in my opinion were from other causes – mainly old age
200,000 people die each year ‘of’/’with’ a cold that knocks them over the edge
covid is the same but we decided to call it a covid death but we dont call them ‘cold deaths’ every other year
covid is a nasty cold. dying of old age is often dying of something you would have shaken off when younger
Quite agree.
Quite. Covid has taken over from influenza as the end-of-life disease. Really we should be presented with Quality-Adjusted-Life-Years lots (QALY), not simply deaths. This would have adjusted both for the risks to the most elderly, but also the very vulnerable in all age groups. If we’d presented ‘death’ statistics in this way it would have shown covid to be a non-threatening disease. I suggest that it would also show the risks from the vaccines to be greater than has been suggested officially (ie, the life of a healthy youngster is worth more than an elderly person on their death-bed).
Excellent point and overall analysis. Thank you for all your work.
100%
many of us having been talking about QALYs all the way through but its been ignored by everyone because its doesnt fit the narrative
Bartram, your piece on HI was splendid!
And the link to the Roy Anderson study very instructive. They seem to be following his recommendations to a T! Many thanks and keep it up please. We need people like you and Eugyppius very much.
I’ve been trying hard to not be too sensationalist in my analysis. It is rather difficult, though, because there’s just so many problems with the official data that we’re being presented with.
A post on the many problems with the official data would be welcomed by me!
Thanks for your post.
You may find this useful….
https://www.youtube.com/watch?v=SoV-PxTSi0E
I’ve seen this before, and yes, the ONS presentation of the data is so misleading as to reasonably be called a lie.
ONS has thoroughly discredited itself.
Hi @amanuensis, great work here. With the data that you have looked at, is there anyway to up pick the relationship between testing figures and “cases” please? When ever there is an increase in reported infection, there has been a corresponding increase in test volumes and also the mix of test types. There is also variation in testing capacity and higher utilisation could mean higher errors or something else. My instincts tell me that there are some patterns to unpick here?
Thank you for your efforts, on behalf of science, truth …… and us. X
You cannot be Covid infected. Covid is a disease.
Will, using vax data 3 weeks before would make the error bigger, not smaller because fewer people were vaccinated. The ONS data is faulty but that isn’t the reason. In fact, it’s the complete opposite. I’m trying to contact you. An old friend.
But what matters is the relative numbers vaccinated at the point of infection.
As a way to think about this — what would happen if the delay from infection was 6 weeks? What about if people were kept alive in ICU for six months before eventual death? To analyse by proportion vaccinated at point of death in incorrect and will lead to misleading conclusions.
I’m struggling with the logic of this at the moment.
I can see how a reporting delay of deaths during a vaccination campaign can affect the unvaccinated death rate because you are understating the unvaccinated population denominator that would be consistent with the unvaccinated death number numerator
So if we are talking about time in weeks you might with a death reporting delay of 3 weeks be calculating because the deaths reported at t+3 are actually the deaths that occurred at time t, say
unvaccinated deaths at (t)/unvaccinated number at (t+3)
And as the unvaccinated deaths at time t would be based on a higher population of unvaccinated than at t+3 because unvaccinated numbers are reducing as people get vaccinated, you get the ongoing overstatement. And when vaccination really ramps up to its faster rate you create an artificial death rate peak which then falls until vaccination ends and there is no overstatement of the mortality rate at all.
However here are we talking about calculating
unvaccinated deaths (t+3)/unvaccinated population (t+3)
to allow for the progression of genuine covid. So there isn’t a death/population mismatch so shouldn’t be the same issue.
So isn’t this argument reliant on those with ongoing genuine covid not being able to get vaccinated, which is a return to the original argument of those most sick not being able to get vaccinated? Not just the terminally ill but those with covid symptoms not being able to get vaccinated?
No. What matters is the vaccination numbers at the time of infection. At that point a series of events are set in motion that in the unlucky few results in death. What happens to vaccination numbers between infection and death doesn’t change the outcome for that individual.
Not related to this comment at all, but thought it worth pointing out that Norman Fenton does state “It is important to note that we are not claiming the death reporting is delayed in the ONS data”
Good point.
And Norman Fenton’s sole metric is all cause mortality in vaccinated vs unvaccinated and he’s trying to explain what causes the all cause (and non covid peak( in the unvaccinated. This post is talking about covid mortality.
That’s a fair point — I’ll apologise to Norman for suggesting that he’d said it was the case.
Sorry. Was getting a bit confused between all cause mortality and covid mortality.
I can see that in the theoretical scenario of all covid being real symptomatic covid disease, and disease progression to death being about 3 weeks, then you can strongly advocate for the 3 week lag and do this compare.
There’s an implied assumption that someone with covid symptoms doesn’t get vaccinated in the 3 weeks to death (otherwise you’d have a vaccinated death not consistent with the unvaccinated status). But not unreasonable to assume that.
Important to say Norman Fenton is talking about all cause mortality and with all cause mortality you need to keep the vaccination status and death statuses at the same point in time.
Yes — it is assumed that the infected / hospitalised don’t get vaccinated. I believe that it is advised that those with covid symptoms or a positive test should not be vaccinated until some time has passed.
It would, indeed, be a very bad idea to vaccinate someone who is already infected. Bad medically, that is. If your surgery or hospital was earning money for each vaccination it could be good financially….
The analysis uses time of infection which led to death.
From Yeadon’s telegram page https://t.me/s/robinmg
I am writing to you with great urgency over a grave matter which has not been highlighted anywhere I have seen. It looks like the MHRA are holding back on vast numbers of death and injury reports for the booster shots.
In their Yellow Card Summary, the MHRA have recently stated that the 9 million or so booster jabs have generated 5566 adverse drug reactions. This didn’t look right so ploughing into historical data, I went into the early figures of the initial rollout which would have included large numbers of the elderly and some health workers, so fairly like for like conditions. What I found was that the first 10.1 million jabs up to early February actually produced 102,000 ADR’s, a rate of ADR’s over 16 times higher that what we are seeing here. So what’s going on, are the vaccines safer this time around?
Well buried in the MHRA Yellow Card Summary are these paragraphs:
“As of 3 November 2021, an estimated 9,012,676 people had received their booster or third vaccination in the UK”
“However, due to ongoing work on the presentation of the latest data on numbers of vaccines administered, suspected adverse event reporting and incidence rates will be updated as soon as the vaccines administered dataset is available”
Because death reports have “only” risen by very roughly 200 or so in the last 7 weeks compared with a total of 1645 before, I’d assumed the booster rollout was going slowly but to my surprise 9 million have had the booster vaccine.
The UK Column graph data highlights this anomaly further, rises in death remain consistent with the rollout – except the rollout shown has zero data for the boosters.
https://yellowcard.ukcolumn.org/yellow-card-graphs
Subsequent vaccinations are expected in our camp to rise the severity of adverse reactions. With the statement by the MHRA this raises a troubling scenario. The substantial rises in death reports in the past couple of weeks may not be from the booster shots at all. And how many are really dying from the boosters? Why the redesign?
What could happen with these vaccines with no longer any feedback of death and injury?
I hope we can get to the bottom of it right away. Are you able to put something out there on this? Thanks
On the post-vaccination risk: there seems to be some evidence of widespread dormancy in SARS-Cov-2, ie the virus can remain harmlessly in the body until some trigger – such as winter cold and damp – predisposes to true infection.
If that were the case, then the post-vaccination vulnerability would not be due to exposure to infected people, but intrinsic risk. That might explain phenomena like multiple deaths in care homes after vaccination: residents might already have been carrying virus, and the vaccination sealed their fate.
I believe that this is an important factor — I intend to write a post on it in the near future.
But note that the time that symptoms appear is still the relevant date to take for ‘time zero’, not the date of death.
Not that data or evidence has mattered one bit since all this started, but as time wears on the number of variables affecting the data and the complexity of analysis required to make sense of the data grows and grows.
This means that the establishment will find it increasingly easier to blur any evidence it doesn’t like and the analysis required to demonstrate the futility of government actions will become increasingly impenetrable.
With third doses coming up comparisons between different population groups are going to be more complicated and harder to follow.
This serves the government very well as it will continue to offer simple messages that land better and are easier to understand.
Rather sadly, this is indeed the case.
Doesn’t the fact that infections are rampant, hospital admissions are high, mortality is high and lockdowns are back, including in countries with the highest vaxx rates in the world, demonstrate the futility of government actions?
That is what people in the street see in the end, which is one of the reasons why governments have been so desperate for the nassi pass, to get people vaxxed and having their green tick live life as normal. That fell apart real fast. Each new failure changes a few more minds, particularly among the younger people. Governments will run out of things on which to blame the failure to stop a respiratory virus in winter sooner or later.
I agree. Lockdowns is fairly obvious evidence that the vaccines don’t Work.
From the Daily Mail. This story was the main headline on their online site this morning and indeed it details the tragic loss, apparently from Covid, of a dedicated surgeon, RIP and all sympathies to the family etc. But now the story has been updated to include the facts that he caught the virus on the wards and had been double-jabbed. It has also led to a major piece on Covid, sad to say the editorial team at this rag that calls itself a paper must have been waiting for another ‘celebrity death’ to get their Covid train back on the tracks. It’s been somewhat derailed of late. More fear porn to encourage ‘boosters’.
EXCLUSIVE: Revealed – Hero surgeon killed by Covid was DOUBLE-JABBED: Heartbroken wife says ‘devoted’ father-of-four, 45, lost Covid battle nine weeks after catching virus on a ward, despite having his second vaccination in January
https://www.dailymail.co.uk/news/article-10220205/Hero-NHS-surgeon-dies-Covid-spending-months-away-family.html
Call me cynical but that was my immediate thought too.
Latest UKHSA Report proves this is a ‘Pandemic of the Fully Vaccinated’ and the data shows the Vaccinated are TWICE as likely to die and are about to overwhelm the NHS
https://dailyexpose.uk/2021/11/19/latest-ukhsa-report-proves-this-is-a-pandemic-of-the-fully-vaccinated/
The evidence for vaccination increasing the risks of catching (and spreading) covid is becoming overwhelming.
Do you mean ADE? Min. of health here has repeatedly said that if you’re vaxxed you barely spread it even if infected. The nonsense of asymptomatic spread aside, surely only a fool would believe that someone coughing and sniveling all over the place is not spreading virus, regardless of whether they are vaxxed or not. The mental gymnastics to keep this going is starting to look like the dead parrot routine.
I don’t think that this is ADE. It looks like the vaccines are mainly offering a protection for the body against a blood borne infection (ie, mainly IgG antibodies) but aren’t offering any protection against upper respiratory tract infections (the vaccines don’t stimulate production of the IgA antibodies that might offer protection in the upper respiratory tract). Thus there is no protection against infection, but some protection against serious symptomatic disease.
There have been suggestions that the presence of antibodies suppresses the ability of the body’s innate immune system to fight covid (this is Geert VdB’s theory) — this would explain an increase in susceptibility to covid while still having few with symptomatic disease (because of those IgG antibodies).
ADE is something else again — if we get post-vaccine ADE it will probably be seen as an increase in severe covid cases in the vaccinated, possibly with very fast disease progression once serious symptoms appear.
IMO this winter’s covid wave will be the high risk period to see if ADE will come. Up until now it has been too early to see the risks of ADE materialise (perhaps in those vaccinated in Dec/Jan, but no later — by next Jan the risks will be in all those vaccinated in the main spring rush for the jab). It is possible that we’ll see ADE after that (12 month’s time), but the peak risk period is probably now to Feb.
Agree, which is why the concept of ‘Vaccine Passports’ for the jabbed is ludicrous from a public health perspective. It’s just a method of control.
This all leans to prove the point that most sceptics and cautious individuals (not anti-vaxxers) had. That vaccination with these novel rushed out jabs should only be given to the over 70’s and those with serious underlying conditions AND with their full consent as to the risks vs benefits.
That is has been rolled out to all adults and teens now is looking like a huge mistake.
I have been hoping, against hope, that lockdown was going to remain the most stupid thing the human race has ever done. Unfortunately the insanity of vaccinating healthy people with a completely non sterilising vaccine is looking likely to supplant it and the human race is going to pay a bitter price for it.
You said it, a total catastrophe in the making!
Is it possible that the early, post vaccination, spike is winnowing out those very susceptible to Covid?
The residue (vaccinated population) would then be fitter/stronger/healthier.
That would mean that these early deaths should be included in any vaccine effectiveness calculations.
Has anyone done calculations of accumulated deaths rather than weekly figures; starting at day one of vaccination.
yougov.chat.
Do you support or oppose a lockdown for the unvaccinated?
You know what to do guys, let them know NOW.
https://t.co/ELxQO20Ber?amp=1
Have tried but can’t get past the first question, which goes something like this : How safe would you feel being in a room with unvaccinated people?
A classic case of trying to alienate the unjabbed. Despicable!
At the risk of attempting to predict the unpredictable, I believe the government is reaching an important moment in history. How do they push through passports, using a drug that is ineffective at dealing with a virus, falling in severity? Maybe they roll out boosters to everyone, then stop all testing, showing no (or little) COVID circulating in the UK….the boosters will clearly prevent transmission and everyone’s a winner. Obviously you must prove you have had your three shots with some sort of passport.
Just a guess…..
I can’t see him risking a vote on passports.
Will there be a vote?
There would have to be.
The key conclusions are supported by the observations that so many country’s observed a big spike in deaths following the start of their vaccination campaigns, including the UK.
An adaptation of an iconic poster.
A measure of how bad things have got is that persons involved with the government and medical establishment will be reading this, and will be saying to themselves:
“Probably very true. But we can’t say anything, because that will ruin vaccine take up.. ..”.
This analysis is also supported by this analyst who has called it the “two week worry window”.
https://boriquagato.substack.com/p/the-number-of-single-vaxxed-people
They are critical of the classification of such people as unvaccinated, making the analogy that to get to freedom you have to crawl over No Man’s Land
The ONS recently published a blog claiming only 9 people had died as a result of vaccination.
9.
https://mailchi.mp/tomwoods/ireland?e=9665758940
CNN recently summarized Robert F. Kennedy, Jr., as saying, “With so much yet to be learned about the virus, using vaccines as the main weapon against Covid-19 could lead to new variants.” “It has never been done before,” said Kennedy, “and it would really be an inappropriate public health strategy to do so.”
Wait, did I say that was Robert F. Kennedy, Jr.? My mistake. Those are the words, as reported by CNN, of Dr. David Nabarro, the World Health Organization’s special envoy for COVID-19.
MSM is trying to make fun of people wanting to protect themselves with cheap and proven drugs. Ivermectin has been FDA approved for human use since 1996. It also beats Pfizer’s new wonder drug hands down, and costs next to nothing. Ivermectin doesn’t make tons of money. So they know the Covid shot is on its final gasp, so they take it add something different to it, rebrand under another name and charge 20 times what they would for ivermectin. I cannot wrap my head around this nonsense. When I explain this to my relatives they label me as crazy and ask me if I know better than science. I don’t make up these information out of my ass. All this information is true and proven. For some people it is near impossible for them to wake up. They are comfortable in their clown world life. If you want to get Ivermectin you can visit https://ivmpharmacy.com
The graphics showing the time course of COVID-19 are revealing – certainly if the intervention of corticosteroids is the same now as then. Quite simply it is too late. It’s probably too late if started at the onset of dyspnoea (breathlessness) because this is a sign of serious decompensation; early on one has the “happy hypoxia “ stage. So what may still be killing people is that aggressive treatment is not given in time.
in the unfortunate event of me getting Covid-19 and being admitted I want systemic steroids at once. See my past blogs at https://bamjiinrye.wordpress.com.
Depopulation, going as planned. Just keep taking those boosters folks. Read Steve Kirsch, Rober Kennedy, Dr Pater McCullough, Del Bigtree if you would like to know how to stay alive
Very interesting analysis, thank you.
But doesn’t the fact that we don’t have any all-cause mortality figures add an additional wrinkle? If many extra vaccine-induced deaths which are missed by only looking at “COVID deaths,” then there will be fewer vaccinated people left alive to become positive COVID cases. Which will make the vaccines look better while all that’s happened is that there’s been disease substitution with increased mortality. I’m not sure it’s worth being saved from dying of COVID next month by being killed by a vaccine-induced heart attack or stroke tomorrow. Does that make sense?