We’re publishing a guest post by a blogger calling himself “eugyppius” about the frantic attempts by the UKHSA to renounce its own data showing infection rates are higher in the vaccinated than they are in the unvaccinated. This post was originally published on eugyppius’s Substack account, which you can subscribe to here. Highly recommended.
Vaccinated vs. unvaccinated case rates in the United Kingdom, from the latest U.K. Health Security Agency vaccine surveillance report:
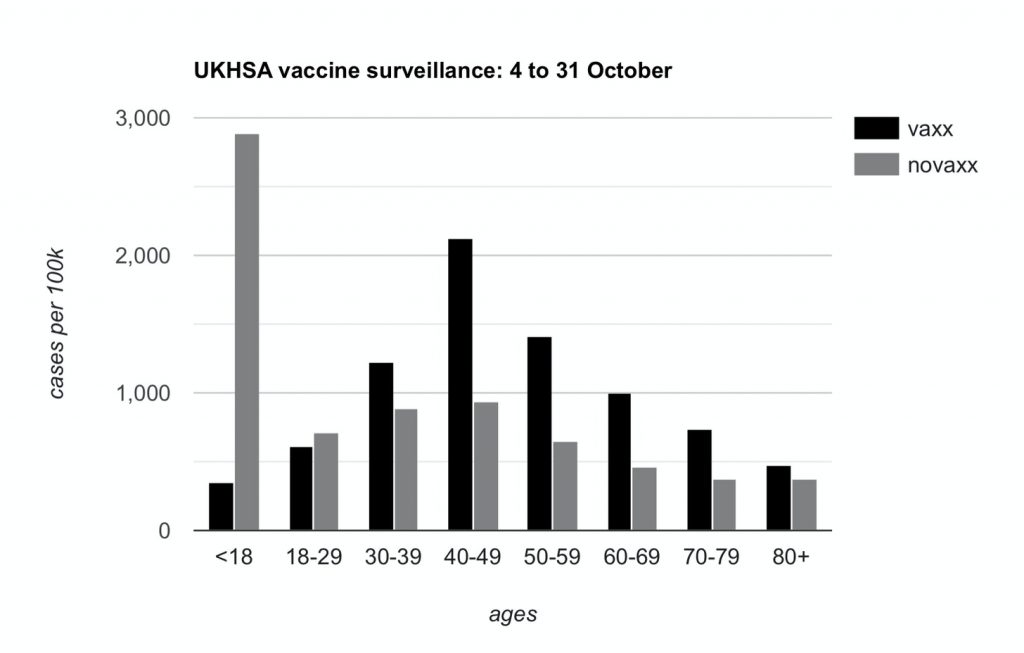
Yet again I had to draw this graph myself, and yet again, the U.K. Health Security Agency wants you to know that these rates are extremely, totally, absolutely unadjusted. They just don’t know precisely why or how.
As I noted on Twitter, it’s emerged that UKHSA inserted all of their ill-advised disclaimers after coming under fire from the Office of Statistics Regulation, a regulatory body which periodically complains about statistics published by the British Government.
OSR director Ed Humpherson met with UKHSA hours before they published their Week 43 report, demanding they do something about these awkward graphs. They responded by ditching the graphs altogether and calling every last number unadjusted. This failed to satisfy him, so in the days afterwards he issued this unbelievable open letter.
Dear Jenny,
COVID-19 vaccine surveillance statistics
Thank you for the constructive meeting on Thursday October 28th to discuss the UK Health Security Agency’s (UKHSA) COVID-19 vaccine surveillance statistics. We focused on the risk that the data presented on rates of positive cases for those who are vaccinated and those who are unvaccinated have the potential to mislead – and indeed we noted that these data have been used to argue that vaccines are ineffective.
We welcome the changes you have made to the Week 43 surveillance report, published on October 28th. It is also very good that you are working closely with my team and with the relevant teams in the Office for National Statistics (ONS).
The U.K. has backed itself into publishing some less-than-useful numbers. Now the office responsible for this publishing will have to work closely with a gaggle of political commissars, responsible for cleansing official discourse of anything that might be “used to argue that vaccines are ineffective”.
Because he appears to be a genuinely stupid man, Humpherson spells this point out explicitly:
It remains the case that the surveillance report includes rates per 100,000 which can be used to argue that vaccines are not effective. I know that this is not the intention of the surveillance report, but the potential for misuse remains. In publishing these data, you need to address more comprehensively the risk that it misleads people into thinking that it says something about vaccine effectiveness.
Emphasis mine. The next time somebody tells you that UKHSA reports show substantial protection against severe outcomes, draw their attention to Ed Humpherson’s letter. He thinks these numbers don’t tell you anything about anything. This is the first step towards not publishing them at all.
This is not just about the choice of denominator. It is about recognising that the comparison of case rates for vaccinated and unvaccinated groups is comparing datasets with known differences – including, potentially, the greater propensity of people who are vaccinated to come forward for tests. So the data reflect a behavioural phenomenon, not just a feature of how well vaccines work. I do not think your surveillance report goes far enough in explaining this crucial point.
Emphasis mine again. Humpherson has no idea what behavioural factors might be at issue. He is just throwing random ideas at the wall here. And notice how he slithers from what is “potentially” true to totally unqualified and unsupported assertions about is true (“the data reflect a behavioural phenomenon”). Maybe the higher unvaccinated death rates also “reflect a behavioural phenomenon“ and are “not just a feature of how well vaccines work”. As long as we are allowed to speculate baselessly, let’s do it in both directions.
He goes on to voice the old and tired complaint about the NIMS data. He wants UKHSA to use ONS population estimates instead. While the former might well understate the case rate among the unvaccinated, the latter is sure to overstate it, but Humpherson doesn’t care.
One possibility would be to only publish rates in the vaccinated population, which are known accurately, but I recognise your concern that you are already publishing rates for both groups.
Confirmation yet again of the obvious: They are only publishing these numbers because they locked themselves into doing so early on, when they looked good.
The alternative would be to use the ONS population estimates, which are used in the main coronavirus dashboard but which may be flawed for some age groups, as you have pointed out. … In the meantime, you should consider setting out these uncertainties more clearly, including by publishing the rates per 100,000 using both denominators, and making clear in the table, perhaps through formatting, that the column showing case rates in unvaccinated people is of particular concern.
That column is of particular concern because Humpherson doesn’t like the numbers in that column. He doesn’t care about the other columns because those numbers are neutral or pleasing to him.
And he closes with this:
I recognise that you want to maintain transparency and consistency, but these qualities should not be at the expense of informing the public appropriately.
Remember, always, that all Corona statistics are propaganda.
The UKHSA have issued a separate set of disclaimers on their website. Every line is fairly hilarious. And the Office of Statistical Regulation provides their own wall of text, where they show that if you understate the unvaccinated population with ONS numbers, indeed you can get the unvaccinated case rate to go up. Humpherson and his crack team of statistics regulators just love the ONS numbers, but UKHSA don’t like them so much. This is because UKHSA actually have to compile minimally plausible tables and for this they are unworkable. From p.15 of the Week 44 report:
When using ONS, vaccine coverage exceeds 100% of the population in some age groups, which would in turn lead to a negative denominator when calculating the size of the unvaccinated population.











To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
If I was a practicing Christian I’d by shrugging my shoulders and leaving the church for good!
I agree..what the heck is the point of it? If you keep chopping the salami, eventually there’s nothing left!
Although I suspect within the Church itself there are many who don’t agree, and hopefully carry on regardless….
Sadly we just see the stuff the media wants to exaggerate and promote….and I’m hoping it’s a bit like the ‘Rona Con’, make people think they are isolated, wrong and alone..when really they are not…..and again it’s some ‘high-ups’, just like our own Government, who are making crack-pot decisions, that the majority would never agree to if asked….
It seems to be the way with everything now!?
Sandi Toksvig moaning about lack of progress towards CofE recognising same-sex marriage:
“In a video, she said it was clear the “Church of England and the society it purports to represent are not remotely in step”.”
Sandi Toksvig says archbishop told her progress on same-sex marriage in Church of England will be ‘glacial’ (yahoo.com)
What on earth makes her think it’s the church’s role to “represent society”? Isn’t it supposed to represent the Word of God?
https://m.youtube.com/watch?v=aQe4vHuXGXQ
great speech in Dutch parliament criticising the Dutch Covid inquiry.
I am not always in agreement with Baudet, but this one is good, despite the fact he does get a bit too shouty towards the end.
I really enjoyed this…and of course he is just speaking the truth…
I had really quick search to see who he was…..apparently, he’s far-right, associated with Russia, and a conspiracy theorist…I could have bet money that is what I would have found…LOL!
He will have to join Mark Steyn, Neil Oliver and all the others in the sin-bin, where all the factual truth speakers have to go!! LOL!
…another one of the good guys…Croatian MEP MIslav Kolakusic….
“The misinformation about COVID-19 spread by officials and public health workers around the world was not just harmful lies but a complete betrayal of citizens. Those lies have severely damaged the credibility of the public health systems, and the consequences will be permanent.”
https://twitter.com/mislavkolakusic/status/1623266467264319488
“Jewish group and MPs urge GB News to stop indulging conspiracy theories” Well, we all knew that this was coming, didn’t we? I mean you can’t have some wild haired presenters speaking their minds, can you? So the powers that be have been looking closely at the content and – oh, hang on, isn’t that anti-semitic? We’ll just go and check with our pet Jewish groups who sounds important and representative but really are there to get the ‘idea’ into the mainstream press and then we’ll call up our buddies at the Guardian and say ‘could you get that journalist, McFidget, to write a piece introducing the ‘idea’ that GB News is anti-semitic and we’ll make sure our chums at Ofcom are notified and …’ Barstewards! This is what those cowardly little people do when faced with unrelenting probing into their plans. They resort to underhand tactics that worked so well with others such as Jeremy Corbyn etc. So Neil Oliver, who is about as antisemitic as Ben Gurion, is the latest focus now that the wonderful Mark Steyn has effectively been neutralised. And they have the gall to say ‘conspiracy theories’ which torpedoes any rational, logical argument below the waterline so it hasn’t got a chance, among the sleeping masses, of gaining more traction. It’s all a well-worn script but how do you fight back? Mark Steyn was actually quite scathing of his former boss, Frangopolous or whatever his name is, calling him a habitual liar. So what we have is the demolition of free speech in plain sight and we all knew it would happen at some point.
Well, we are taking the fight local because this is where the battles will be fought, not in the pages of the Guardian or on the BBC, but in the council chambers, local meeting halls and in the streets of local council districts. First off, the 15 min city plans which councils are rolling out regardless of people’s objections. We clearly live in a totalitarian regime and the people bringing in these plans are going against the rule of law, the common law of this land. We are bringing back jural assemblies, the true indication of real democracy, and we will bend every sinew and nerve towards exposing this treason. They are not going to win this.
Just like Andrew Brigden, I think we will find strong Jewish voices coming out in support over the next few days…
I’m reminded that many millions more people have watched the Project Veritas Pfizer video, than have watched the ‘satanic’ Sam Smith Grammy video…I saw the numbers online yesterday….but we know which was the only one shown in the MSM….!!
I can smell their fear…LOL!
my annual synagogue subscription currently due includes an extra amount for the Board of Deputies which has been cancelled
Good man.
Neil Oliver
@thecoastguy
Anyone worried about me – don’t be. I’ve seen and had it all before. Onwards. X.
The guy is a legend..and I agree with you Ath, they are not going to win….
“Moon dust fired into space could help stop global warming” Lunacy at its most literal. Why give these clearly insane ideas column inches? Even I, with a severely limited appreciation or knowledge of astrophysics, can see how utterly stupid such a plan is. It reminds me of the totally preposterous plots I’ve seen in some Hollywood movies – the idea to restart the sun by sending nuclear missiles into its heart, or landing on an asteroid to divert its course. Do you remember Klaus Schwab’s plan to send huge mirrors into space to deflect sunlight? Are there no critically thinking journalists left at the Telegraph? And I seem to remember, but of course I could be wrong, that we are actually about to enter a period of global cooling. I mean how cold are they planning for us to be? Cold enough to be able to do away with fridges? And have they though that this might be permanent and interfere with ALL life and not only our miserable human ones? Bonkers! I hope their plans, if at all put into being, perish in the Van Allen belt.
…don’t tell anyone, but it’s not just Moon Dust, it’s moon dust mixed with Unicorn Farts, which apparently is the highly secret ingredient….!
Although the question could be moot as there could also be a shortage of actual Moon Dust….. due to China…..who else…?? LOL!
https://www.dailymail.co.uk/news/article-11590249/NASA-boss-China-claim-moon-territory-BAN-astronauts-touching-down.html
A chief at NASA is raising red flags over China’s ambitions to get to the moon.
In a new interview, NASA Administrator Bill Nelson says he and others within the scientific agency are growing increasingly concerned over what the country plans to do when they make it to the moon.
Nelson believes China could attempt to corner the market on resource-rich locations on the moon’s surface and try to block out the U.S. and other countries looking to make it to the lunar object.
‘There is potentially mischief China can do on the moon,’ said one other official monitoring the ‘space race.’
‘And it is true that we better watch out that they don’t get to a place on the moon under the guise of scientific research. And it is not beyond the realm of possibility that they say, “Keep out, we’re here, this is our territory,”‘ Nelson continued.
The NASA boss said he fears China will mimic their strategy when it came to claiming land- and water- in the South China Sea.”
LOL!
I’ll try not to buy it.
The madness of Khant’s net zero. I know it’s not him but he is the poxy proxy. We have to hope that all London Borough’s fight back because “first they came for…
https://www.conservativewoman.co.uk/khans-carbon-cult-is-tearing-london-apart/
…reality….! And just think if it was your baby or child for instance…
Low Traffic Neighbourhoods delay paramedics on 999 calls, says ex London ambulance chief…
Traffic-management schemes and other road changes that could delay life-saving treatments are being monitored, according to London Ambulance Service (LAS).
LAS confirmed it was working with traffic teams across the capital to avoid using physical barriers such as bollards on schemes designed to manage the flow of vehicles. It comes after a series of social media posts showed ambulance crews’ access to streets newly blocked by bollards in Palmers Green…..
Apparently the leader of Harrow Council sent a tetchy letter to Khan saying that the people came first and ignoring Khan’s bullying, HP. Worth a watch: https://www.youtube.com/watch?v=BrjSkkxiiFw&t=364s
Thanks Aethelred I watched the video last night.
I hope the defiant councils are genuinely defiant and not putting on a show.
The article by Berenson in the round-up is worth a read..he ends with
…Fauci is 82 it will be up to the rest of us to deal with what he’s done.
But I’m reminded that this isn’t Fauci’s first rodeo….if you want to sit for an hour with a cuppa I can’t recommend this Substack highly enough….I read it when it came out, but it’s so pertinent to many of the things that have happened with Fauci/Covid….….and taken as an overview of the AIDS ‘scandal’ it’s really informative..
(Currently Dallas Buyers Club is showing on Sky movies, and I’m going to re-watch this weekend….)
https://filiperafaeli.substack.com/p/dont-watch-dallas-buyers-club
I was really impressed when I read the substack article a few weeks ago and subsequently bought the dvd. I’d not seen or heard of the film before that.
https://www.conservativewoman.co.uk/are-king-and-country-worth-fighting-for/
A subject that has bothered me all my adult life. Would I stand and fight for King and Country? Sadly no.
First and foremost I would fight for my family, that is and will be ALWAYS my overriding priority.
I would fight for England, or England as it should be – honest, decent, proud, virtuous – but for the current establishment and the Windsor traitors, never.
I doubt I am on my own and I suspect many couldn’t care less.
I’d fight for the nation of which I’m part but not for the state that clearly hates everything about me other than the taxes I pay.
…it’s an interesting article….
….I think most people faced with a real enemy, that they felt had to be totally overcome, would fight…but I agree with you….not for King and Country, but for family, friends, the life they want to live..and leave for their children…
…..but I don’t think those things aren’t threatened externally..but internally…
I don’t think many would want to fight for our out of touch, WEF member, and fully Woke King, I certainly wouldn’t…..I also wouldn’t fight to fill the coffers of the military industrial complex…..which most people see through now, and are utterly cynical about…..
As you say honesty, pride, virtue and decency, the nuclear family….have all but disappeared from any thoughts or actions of the ‘elites’….so why would anyone want to die, or send their children to die on their behalf?…in the main I despise them…
We have a very different relationship with Government and Monarchy than our forbears did….
At the rate we are giving our military capabilites away to the Ukraine, I am more and more concerned by the threat of War being declared by the Isle of Man. We would surely have to capitulate and sue for peace.
The proudest of military traditions, to not being able to defend ourselves, in a single generation. All while no-one noticed…
Or, yea Gods, what if the wee screecher attacked over Hadrians Wall??
I have a distinct feeling that leaving the country so ill defended in a time of great turmoil and war is actually a treasonous act. I would have to check but it must be written somewhere about this.
Sadly yes Neil. 😔
Agree with all you say, HP. I think I might have done way back but I ain’t fighting for no WEF puppets. I would fight for England, for my fellow countrymen but definitely not the government or, indeed, the King if he continues to go along with the WEF stance.
Thanks Aethelred. 👍
I’m with you Hux me old fruit ! Used to think I might if The Queen asked but now it’s a no from me !
Cheers Freddy.
More dubious use of taxpayers money…
https://declassifieduk.org/uk-spends-over-80m-on-media-in-20-countries-around-russia/
Yet people in this country have to go cold and hungry while an illegitimate government pisses taxpayers money away in foreign lands and for which we have no legitimate interest.
Our government is treasonous but for how many years has this been so?
All the way back to Major I reckon.
I reckon that it goes back even further, early to mid 20th Century at least.
https://youtu.be/q1_5VrUunqI
The MET now admitting to recruiting coloured people who can’t write or speak English. I’ve posted on this previously.
Quel surprise!
I refer to the Guardian article about Neil Oliver’s broadcast. There was nothing anti-Semitic in it and if the Jewish community is ramping up its sensitivity to crazy levels that restrict free speech then they must be told to stop, or risk being ignored even when actual anti-Semitism occurs.
On the subject of “Hypocrisy from MPs regarding regulators”, New Scientist in November 2019 (just before the “pandemic”), had a front page article “Why the Medicine You Take Could Actually be Bad for Your Health”.
ISSUE 3258 | MAGAZINE COVER DATE: 30 November 2019 | New Scientist
The article was drawing attention to the increasing phenomenon of new drugs being rushed to market with insufficient testing, and of regulatory capture by the pharmaceutical industry.
It included this observation:
“Drugs are approved based on preliminary findings, or authorised for a particular use, then widely prescribed for something else. And hanging over the process is a worrying question: are these agencies working to protect the public or to further the interests of drug companies?”