
Infections are on the rise according to the ONS and, despite the vaccines (and the fact that fully-open U.S. states continue not to see a rise in infections let alone the prophesied mass hospitalisations and deaths), talk has once again turned to keeping restrictions going beyond June 21st. Portugal has been brutally struck from the green list, ruining the holidays of tens of thousands of Brits. Mark Drakeford, the First Minister of Wales, has suggested social distancing could continue for the rest of the year.
Driving the fear is the Delta (Indian) variant, which new data from Public Health England suggests could have more than double the risk of hospitalisation compared to the Alpha (British) variant. The Guardian reports:
An analysis of 38,805 sequenced cases in England revealed that the Delta [Indian] variant was associated with a 2.61 times higher risk of hospitalisation within 14 days of specimen date than the Alpha [British] variant. There was a 1.67 times higher risk of A&E care within 14 days. These figures take into account factors such as age, sex, ethnicity, area of residence and vaccination status.
It appears PHE has been up to its usual tricks again though. While the data adjusted for age, sex, ethnicity and so on might produce these alarming results, the raw data tells the opposite story. Here’s the relevant table with some key figures highlighted:
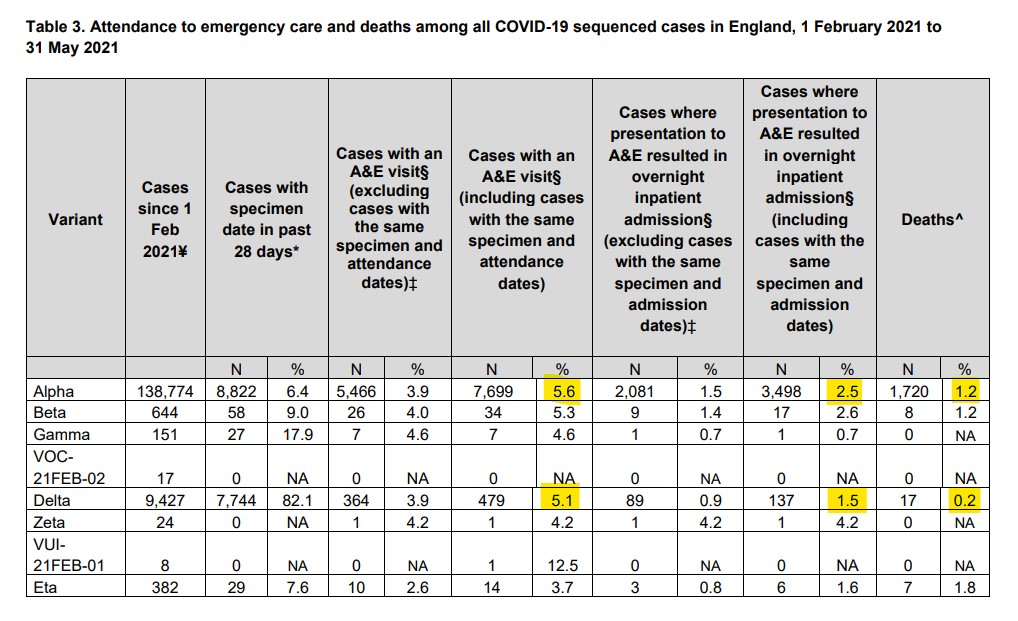
Far from showing double the risk of serious disease, in the raw figures a smaller percentage of Delta (Indian) cases versus Alpha (British) cases went to A&E (5.1% vs 5.6%), stayed in hospital (1.5% vs 2.5%) or died (0.2% vs 1.2%). The two groups are presumably very different demographically, which is why PHE’s adjustments were so radical. But the big question is, how reliable can findings really be when the reported results are adjusted so drastically from the raw data, bearing in mind the guesswork these adjustments involve?
Early Delta (Indian) variant hotspots also give reasons not to panic, with Bolton’s positive Covid tests and hospital patients already on the decline.
Is anyone else getting a wearying sense of déjà vu? As Ross Clark notes:
We have been here before. In January Sir Patrick Vallance, the Chief Scientific Adviser, held a press conference to announce, glumly, that the Kent variant appeared to have a mortality rate 30% higher than previous variants. That led news bulletins. Less noticed were two studies published in the Lancet and Lancet Infectious Diseases in April which analysed the data and concluded that, after all, the Kent variant was no more deadly than previous variants.
Who’d bet against a similarly quiet and belated admission happening here, once the panic has done its damage?











To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
My three year-old would do well under this regime. After lengthy preambles, we got to ‘What does C A T say?’ (sounding the letters). There was a thoughtful but confident pause, and she proudly returned with ‘Zebra!’. It’s a question of priorities, with imagination being the strongest. Sadly, she will lose this genius in the coming months.
I recall when my sister was three and she had trouble pronouncing the word “warm”. My dad said she could have a glass of cola if she could say it. So she thought for a second and blurted out the word “HOT”. —–She deserved the cola for that genius
🤣
My sister once asked dad for a drink of ‘nilk’. He tried to get her to say it correctly, and after a few failed attempts she gave up and asked for ‘zorange’ instead.
Wasn’t this a Calvin and Hobbes strip many years ago? Calvin wrote ‘I refuse to answer this question as it is against my religious principles’ or something, in a Maths test. I hope Watterson was cited.
No surprise. Cultural Relativity. No right answers including Maths, invented in the modern format by White men including Christians. Abominable isn’t it. But comports with a penis is a vagina and an x chromosome is the same as a y ‘science’.
I would say that in a world of Fake Science, Fake Maths is mandatory. What’s that? Can’t get Newton’s or Einstein’s equations for Big Banging theology to balance? Lorenz’s invariate not working? Galilean trickery failing? No big deal – just add the demi-urges of ‘dark matter’ and ‘dark energy’ as ‘constants’. There you go. Everything balances. Consensus. All hail. Don’t be an -ist.
Or the cat that can be dead or alive at the same time. But what about all the cats that existed before humans never looked at them because we were not a species yet?
I tried to get the views of our Lab-Pei (Labrador X Shar Pei) on this topic, but he was too busy doing the Times crossword puzzle and told me to foxtrot-oscar.
OMG
😀😀😀😀😀😀😀🙂😀🙂🙂😀😀😀😀😀
Class.
Not really hux’. He’s a rescue dog. Having said that, he had a splendid first two years of his life as a stud dog, then castrated and sent to the pound from whence we got him. Re “class,” in 1978 in my RAF days, I drove a fire-engine red Morgan +8. and was out front of the Mess checking the rad’ one morning, prior to an ‘assignation’ involving bubbly and the future Mrs 10navigator. Seeing the rad’ needed a top up, I used a champagne bucket to decant water into it.. A passing fellow officer looked, nodded and muttered, “class”.
“So, kids of different races may naturally ‘perform’ maths in different ways – the boring old traditional method of performing calculations in a logical, rational and systematic fashion is really just the way white, straight, males have long performed the subject.”
The pyramids were obviously designed to be traditional rectangular-shaped structures, but due to their race, their mathematical calculations ended up with pyramids.
Makes perfect sense to me /sarc.
Nah, they ran out of stone so had fewer to use for the upper layers.
An interesting article – from a ‘know your enemy’ perspective.
So essentially the suggestion is to allow certain students to fail and to make them feel less bad to drag others down too.
I don’t fancy using a bridge designed by these Mathematxcal (or should that be mathematiqal – to emphasise gender diversity?) geniuses.
By the way, my beans tell me I’m too late – I should have asked them for their fruit earlier. I must have lost count of days somehow.
Why do these people think adding an ‘x’ to the end of every word makes them edgy and cool?
Fux if I knowx !
😀😀😀👍
Good one.
In biblical times, wasn’t this known as the Tower of Babel?
Thanks Steven. It must have been harder than trying to solve Fermat’s last theorem using a decimated abacus deciphering this twaddle. Ever since the American Physicist Alan Sokal parodied this progressive drivel, its proponents have just turned up the ridiculous level. A serious point is that STEM skills will now become even more calcified in the white elite. In case this painfully stupid woman doesn’t know it the Chinese and Asians (who are often browner than her Latin compadres), and have just as many foundation myths, favour materialism. That’s why they come top of international league tables. Meanwhile the kids taught this mince will be further disadvantaged in a world where numbers as an abstract form of knowledge with really concrete applications rule. You could call it regression to the meaningless.
“Ma..? Fetch the net. No. the big one…”
So let’s see what happens when NAxA builds a space shuttle devised by Physxists and Mathematixns
After you… No, I insist.
5 out of 3 globalists can’t do fractions.
Did the author of this drivel pass it by her psychiatrist before publishing? I guess not.
Absolutely bonkers!
If a person can change gender just by believing it then 2+2 = 5 just by believing it.
Check her out in Google Images: I think that unhinged rictus probably never leaves her face. The Blair Stare – into fantasy world.
Extreme example of merging feelings with facts, so that there is no non-subjective reality.
The devouring mother indeed.