
The story on the front page of today’s Times is referring to the latest coronavirus data from the Office of National Statistics (ONS) for the week ending April 17th which showed a big jump in care home deaths compared to the previous week. The number of overall deaths in care homes for Week 16 (April 11th – 17th) was 7,316. That’s 2,389 higher than Week 15, almost double the number in Week 14 and almost triple the number in Week 13. However, deaths from COVID-19 in care homes in Week 16 was 2,131, less than the number of deaths in hospitals (4,766). So what is the Times basing its story on? Turns out, this is the view of David Spiegelhalter, the Cambridge statistician. Here’s the key sentence: “Professor Spiegelhalter said that it was possible that coronavirus deaths in the homes now exceeded those in hospitals, with both running at about 400 a day but heading in opposite directions.” In fact, the average number of deaths in care homes in Week 16 was 304, although it may be larger now.
The ONS data, which was published yesterday, seems to show we’re on track for a big rise in excess deaths this year. The provisional number of deaths registered in England and Wales in the week ending April 17th was 22,351, an increase of 3,835 compared with the previous week (Week 15) and 11,854 more than the five-year average for Week 16. That’s the highest weekly total recorded since comparable figures begin in 1993.
However, let’s contextualise those figures. By my calculations, that’s a total of 207,310 deaths from all causes in England and Wales for Weeks 1 through 16. (I couldn’t find this figure in the ONS data, so I added up the weekly totals.) That compares to a five-year average for the same period of 185,213, so a total excess of 22,097 for the year to date. Does that mean the total deaths for the whole of 2020 will be significantly higher than the five-year average? Not necessarily. Don’t forget that according to Professor Neil Ferguson up to two-thirds of those who’ve died of COVID-19 might have died anyway this year, so it’s possible that the virus is just pushing some of the deaths that would have been spread out over the course of 2020 into the first four months. At the end of Week 16 in 2018, after a bad bout of seasonal flu, the total deaths from all causes in England and Wales was 198,943, just 8,367 lower than it is this year. Yet the total number of deaths in England and Wales in 2018 was 541,589, compared to 533,253 in 2017, a difference of less than 10,000. According to the ONS: “Although 2018 saw the highest number of deaths since 1999, when taking the age and size of the population into account, death rates have remained more or less stable since 2011.”
These sorts of comparisons only tell us so much, of course. If the total number of deaths in 2020 is no higher than the five-year average, the lockdown zealots will attribute that to the extreme social distancing measures imposed on March 23rd. But here’s a curious thing about the latest ONS data: if lockdowns are effective at reducing mortality from COVID-19, why did England and Wales’s numbers go up in Week 16, the lion’s share of which (five days) fell more than three weeks after the UK lockdown was imposed? Given the three week lag between infection and death, you’d expect the numbers to go down between Week 15 and Week 16, but they haven’t. According to the ONS: “Of the deaths registered in Week 16, 8,758 mentioned ‘novel coronavirus (COVID-19)’, which is 39.2% of all deaths; this compares with 6,213 (33.6% of all deaths) in Week 15.”
Admittedly, this isn’t conclusive because the people dying in the first two days of Week 16 – the Easter weekend – might have caught the virus exactly three weeks earlier on the weekend of March 21st and 22nd, just before the lockdown was imposed. And it can take more than three weeks for someone to die after being exposed to the virus. However, if the ONS figures next week show a rise in deaths from COVID-19 in Week 17, that really will suggest the lockdown has been ineffective.
Okay, now for some light relief. Following the publication of yesterday’s ONS data, CNN ran a story headlined: ‘Coronavirus death toll 54% higher in England and Wales than daily stats showed.’ To get this 54% figure, CNN’s Simon Cullen and Zamira Rahim compared the ONS data for the number of deaths registered in England and Wales in the week ending April 17th (22,351) with the number of people the Government said had died of COVID-19 in England and Wales up to April 17th (14,451). “The 54% difference is caused by multiple factors,” the reporters solemnly intoned, and went on to list some of them: the Government’s figures only include people who’ve died in hospitals, not care homes, and the official figures “fail to account for a lag in reporting some deaths”. But there’s a simpler explanation. The ONS figure (22,351) relates to all-cause mortality in Week 16 (April 11th – 17th), while the Government figure (14,451) refers to the number of people who’ve died from COVID-19 in the year to date. Talk about comparing apples and oranges! I’ve posted a screen grab below as, hopefully, CNN will eventually get round to correcting this schoolboy error.
I’m not suggesting there isn’t a discrepancy between the ONS’s Covid data and the Government’s, mainly because the latter just refers to deaths in hospitals. According to the Reuters report, which unlike the CNN report is actually accurate: “The Office for National Statistics said it had recorded 21,284 fatalities that mentioned COVID-19 on the death certificate as of April 17, compared with 13,917 in the daily hospital death stats published by the government.” (Those are both cumulative, year-to-date totals.)
But before we conclude that the ONS figure is the more accurate of the two, it’s worth bearing in mind that it includes deaths outside hospitals recorded as being from COVID-19 when the doctors issuing the death certificates merely suspected the virus was the cause of death without having a test result to base that on. I’ve checked the guidance in the Coronavirus Act 2020 and it says any medical practitioner can sign the death certificate, even if they weren’t present during the patient’s final illness; they can record COVID-19 as the cause of death even if it’s the “underlying” and not the “direct” cause; and they don’t need “diagnostic proof” that COVID-19 was the cause of death provided they’re satisfied “to the best of their knowledge and belief”. Not exactly rigorous! The true number, therefore, is probably somewhere in between the Government figure and the ONS figure, although we’ll never know for sure without exhuming the bodies and carrying out autopsies.
Manhattan Contrarian has looked at the way Covid deaths are recorded in the US and concluded that they’ve almost certainly been over-reported, including in hospitals, not least because hospitals have a financial incentive for inflating the figures. Worth reading his post on this. Will we see a big uptick in the number of deceased NHS workers being recorded as having died from COVID-19 now that the Government has said it will compensate their families to the tune of £60,000?
This morning’s Telegraph leads with with the fact that the Government has changed the wording of its fifth test, watering it down considerably. It used to stipulate that the Government would only start easing the lockdown if it was “confident that any adjustments to the current measures will not risk a second peak of infections”. But at yesterday’s Downing Street briefing, the words “that overwhelm the NHS” had been added. That gives Boris considerably more wiggle room, particularly as the NHS’s critical care capacity has more than doubled since the lockdown was imposed. That capacity is now sufficient to accommodate the rise in infections associated with reopening schools and universities as estimated by no less an authority than Professor Ferguson and his team in their March 16th paper, a point I made in a blog post for the Critic yesterday.
If you can’t get beyond the Telegraph‘s paywall, the Mail also has the test tampering story. ‘Is the government preparing to ditch lockdown?’ it asks. We can but hope. (According to Christopher Snowdon, the whole story is fake news.)
Several papers report the fact that the NHS England issued an alert yesterday, warning of a “growing concern” that a coronavirus-related inflammatory syndrome might be affecting children. However, only 20 children, at most, have been hospitalised with the condition, the symptoms are remarkably similar to those of Kawasaki disease, a majority of the children affected have already been diagnosed with Kawasaki disease and some of the children affected have tested negative for COVID-19. Overall, the admission of children to hospital with Kawasaki disease is lower than normal this year, not higher.
At yesterday’s press briefing Matt Hancock announced that one of the six drugs currently undergoing clinical trials for treating COVID-19 is being tested on humans. He didn’t reveal whether this was hydroxychloroquine – or whether hydroxychloroquine is one of the six drugs being trialled – but the research evidence that it’s an effective treatment is growing. The Association of American Physicians and Surgeons (AAPS) has written to the Governor of Arizona claiming the drug helps 91% of patients recover. This contradicts the preprint published by the Veterans Health Administration that I referred to yesterday which found that Covid patients given hydroxychloroquine were more likely to die than those who weren’t. That study only involved 368 patients, whereas the AAPS’s involved 2,333. Incidentally, the woman whose husband died after ingesting chloroquine sulphate – a death that Donald Trump was widely blamed for in the mainstream media, following his praise for hydroxychloroquine – is now under investigation by the Mesa City Police Department’s homicide division. The Washington Free Beacon has the story. (Someone has pointed out in the comments that that AAPS is a conservative advocacy group.)
The ranks of lockdown sceptics received an unexpected addition yesterday: Theresa May. The ex-Prime Minister posted a video urging the Government to lift the lockdown. “The Government must also think about the impact of lockdown on our overall health and wellbeing as a nation,” she said. “That of course includes the economy, but it must also include the impact on domestic abuse and mental health. We cannot have a situation where the cure for the disease does more damage than the disease itself.”
Another unexpected recruit is Thomas Friedman, the Pulitzer Prize-winning New York times columnist. Speaking on Indian television, he said the sub-continent’s best hope is to go for herd immunity, sheltering the elderly but allowing the young and fit to return to work. “The trick is to get your people out to acquire immunity naturally but get only those out who may experience COVID-19 virus mildly or asymptomatically so that you don’t overwhelm the healthcare system,” he said. India Today has the story.
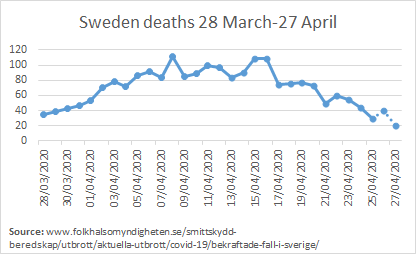
That strategy certainly seems to be working in Sweden, as the New York Times reported yesterday. Sweden’s death rate of 22 per 100,000 is about the same as Ireland’s and far better than in Britain or France. And the graph showing the daily death tolls up to April 27th shows the Swedes have flattened the curve:
In spite of mounting evidence that lockdowns are ineffective – see this new research by a group of Israeli professors, for instance – the British public remains passionately enthusiastic about them according to a new opinion poll. The FT writes:
Most British people would prefer to delay lifting lockdown measures until the virus is “fully contained”, and would feel worried about leaving their homes even once rules have been eased, according to a poll by Ipsos Mori. As many as 70% of UK residents said they were concerned about restarting the economy prematurely, while 71% expected they would be “nervous” about venturing outside once businesses had reopened. The results suggest that Britons are more cautious than other nations that took part in the survey of 28,000 people, conducted between April 16th – 19th. When asked if they would favour opening the economy before the coronavirus pandemic is fully under control, 65% of Mexicans were against, followed by 61% of Australians and 59% of Americans.
How to explain the British people’s supine acquiescence to being placed under house arrest? Could it be that our medical-industrial complex has completely terrified the public with its apocalyptic prognostications of doom? That’s the theory I come up with in an article in the latest issue of the Critic entitled ‘The return of Project Fear‘. Another possibility is that it’s due to the blob-like growth of ’elf-and-safety culture, particularly in the public sector. One reader thinks this is the reason:
The Covid thing has revealed the complete divide between the risk averse and risk takers and unfortunately that divide seems to fall in large part between the public sector and the private sector. Bureaucracies are not exactly the place to find people ready to jump – free fall or bungy or otherwise. I am in the latter category and I fear the long term consequences of the lockdown will be devastating. Look it’s complicated, I get that, but life is a risk and we have spent many decades hopelessly in thrall to reducing all forms of risk, in our parenting, our education, higher and lower, in government, nanny state, etc. People are far more fearful than they need/should be. Roosevelt’s quote is as pertinent today as it was then.
I’m reminded of another quote, this one by CS Lewis: “Of all tyrannies, a tyranny sincerely exercised for the good of its victims may be the most oppressive. It may be better to live under robber barons than under omnipotent busybodies.”
One consideration when assessing the effectiveness of lockdowns is understanding how coronavirus is passed from person to person. If large droplets and contaminated surfaces are the dominant mode of transmission, then washing your hands, wearing masks and social distancing may be sufficient to suppress infection. But if clouds of tiny aerosol droplets are found to be the dominant mode then ‘shelter-in-place’ orders make sense. My colleague Jonathan Kay, who like me works as an editor at the online magazine Quillette, has tried to answer this question by analysing what are referred to in the scientific literature as “superspreader events” (SSEs) – large COVID-19 infection clusters, such as the bartender who infected numerous people in an Austrian ski resort. Jonathan couldn’t find any comprehensive database of COVID-19 SSEs so he built his own, cataloguing 58 SSEs in 28 different countries (plus ships at sea). It’s worth reading the piece in full, but his conclusion is that virtually all SSEs feature forms of human behaviour that permit the direct ballistic delivery of a large payload of droplets from face A to face B. No aerosol transmission, in other words.
I should stress that Jonathan isn’t an out-and-out sceptic – he’s agnostic on whether lockdowns have had any positive effects and, being more scientifically-minded than me, won’t reach a conclusion until there’s more data available. But I like to think he’s on our side. I interviewed him for the latest Quillette podcast.

A reader has been in touch to complain about an article I linked to a couple of days ago:
I’ve been stewing over Andrew Sullivan’s column in which he quotes Damon Linker – “A life without forward momentum is to a considerable extent a life without purpose.” Sullivan, who identifies himself as a faithful Catholic, should know better. The Catholic church has a long, rich tradition of cloistered nuns and monks who surely are not engaged in “forward momentum” but are valued for their constant prayer and contemplative lives. And what about stay-at-home parents who homeschool their children and keep the household running? Are those lives without purpose? Just wanted to get that off my chest.
And finally, another reader has suggested a few more verboten phrases to add to the swear jar list that RDawg came up with yesterday:
- ‘The “R” number’
- ‘The “Lag”‘
- ‘NHS Heroes’
- ‘The Peak’
- ‘The five tests’
- ‘Test, track and trace’
As always, a big thanks to those who donated to pay for the upkeep of this site yesterday. Maintaining it – and doing these daily updates – is proving to be quite a bit of work, so if you feel like donating you can do so by clicking here. And if you want to flag up any stories or links I should include in the site, or have points you think I should make, you can email me here. See you tomorrow.
P.S. Congrats to Boris and Carrie on the birth of a son.













To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
Big news from Switzerland, which says grandchildren can hug theirnparents and claims: Young children are not infected and do not transmit the virus,” he said. “They just don’t have the receptors to catch the disease.”
Coronavirus: Switzerland says young children can hug grandparents https://www.bbc.co.uk/news/world-europe-52470838
…which was directly refuted by Hancock and Whitty:
“Advice in the UK remains that children should not have contact with grandparents.
At a daily news briefing this week, Health Secretary Matt Hancock was asked by a member of the public when she would be allowed to hug her grandchildren again.
Mr Hancock said he “fully accepts” the importance of getting together with family but that it was important that “people who are vulnerable continue to be protected”.
The UK’s chief medical adviser, Chris Whitty, has warned that for some vulnerable groups close contact with family may continue to be a risk for some time.”
So, who exactly, is following the science here?
We don’t know. The science and knowledge base is developing rapidly. As Toby points out the transmission modes are not properly understood yet – but must surely be improving rapidly. The Germans do not agree with the Swiss view which seems somewhat confused – hugging but no babysitting for example. The reporting might be incomplete.
My view is that we probably do not yet know. The Swiss might be right…. they might not.
It certainly supports a case that was report a while back on ‘Covid facts’
https://academic.oup.com/cid/advance-article/doi/10.1093/cid/ciaa424/5819060
*predictor for flu and influenza, not covid
Honestly I don’t know how, at this juncture, how someone who has been almost completely isolated for six weeks (whether they be young, old, whatever) visiting the home of someone else who has been almost completely isolated for those same six weeks, is really a risk to the other.
This is a very different situation from one of these people being a key worker who has been out of the house every day, around other key workers – possibly taking anything they catch into the home of the other.
The majority of people aren’t key workers and have as such been almost completely isolated within their households for at least a month.
Once again the position of the minority is being projected and subjected onto the majority.
This entire time, Switzerland has allowed group of children (up to 5 of them) to play together. They are also accelerating reopening of restaurants, starting May 11th, stating that we have to accept a certain amount of risk but be pragmatic.
Interesting guest post on my blog looking at the effect of latitude (a proxy for temperature) on Covid-19:
https://hectordrummond.com/2020/04/28/guest-post-simon-anthony-migration-of-infection/
CEBM have done this too. Great minds must think alike https://www.cebm.net/covid-19/effect-of-latitude-on-covid-19/.
There has been plenty of evidence this is a predictor (as a proxy for temperature and humidity). Link below. Does that meant he recent drop in Covid is due to the unseasonable warm weather we’ve had?
https://www.researchgate.net/figure/Influenza-peaks-and-climate-by-latitude-The-mean-monthly-rank-of-each-climate-variable_fig2_236057860
So just to summarize the situation with care homes. Something like half the grand total of Covid-19 deaths in the UK (depending whom you believe) are happening to about 0.6% of the population. Another 2% of the population are employed in adult social care looking after these people, and still working of course. The epidemic is still raging away happily among this 2.6% with plenty of new deaths since the lockdown. Meanwhile the other 97.4% are sitting at home watching the wall wondering if they still have a job.
In a nutshell, you nailed it.
Not sure it’s even raging among the 2% is it?
I was going by the chart here: https://www.bbc.co.uk/news/health-52284281 showing that deaths are still going up. They should start to drop off about 3 weeks after the lockdown if it was having an effect on them. I’m not really surprised if it isn’t.
Absolutely this. As an employee of BA I and my colleagues are at the head of that 97.4% queue. Still, at least Greta and the other water melons – green in the outside, red in the middle – will be happy to see the aviation and associated industries on their knees. Historically, this lockdown will be seen for what it is, the biggest unnecessary self inflicted wound in modern history.
Anyone who tries to use the lockdown as a model for how to reduce CO2 emissions is undermining the environmental cause. Anyone with sense knows that the only valid ways of reducing emissions are thsoe which preserve the luxuries and liberties of modern society but produce them in ways which emit less CO2. Climate change can be fixed through hydrogen cars, nuclear energy, renewebale energy, CO2 neutral biofuels for aviation, and cleaner fuels for shipping. Not by getting rid of the things which energy consumption enables.
Lol the TV lamestream are coming for Sweden now. Probably cause they’ve finally realised they’ve been peddling complete crap for six weeks.
The ONS figures relate to the day deaths are registered not when they occurred. The figures for this week are the peak, which occurred over 8 April. The important point about that is that this peak corresponds to a peak of infections on 18 March, 6 days before lockdown. The peak in London was 4 April so 14 March, 10 days before lockdown. They show that lockdown was not necessary to bring the epidemic under control. A similar result can be shown for New York (and lots of other places). This, along with Sweden’s experience, really destroys the case for lockdowns, but that government, its advisers and the media are closing their ears.
As a non believer who has a lively friendship with a Benedictine Nun, just wanted to comment on “A life without forward momentum is to a considerable extent a life without purpose.” Nuns actually have very active lives, unless they are cloistered for a particularly important part of the religious calendar, they travel, garden, hike, have visitors (benedictines in particular are very big on hospitality and have lots of friends visit, or receive guests who come on retreat), they go into schools, hang out with their monk mates, often have academic interests so are off visiting libraries, or researching their next book, and generally are not moping around the abbey.
Secondly even stay at home parents, or parents who home school go out, or go to the gym, or take their kids on trips, or have play dates and friendships and hobbies. My sis in law is a stay at home mum, she has a very active life, and is climbing the walls at the moment, as are her children.
Yes and although I electively home educated both my children, until they went to college to do A levels, “home” was a total misnomer for what I and hundreds of other home educators engaged in. For the most part we weren’t at home at all. We were out doing sports, theatre, walks, museums, group activities, technology centers, wildlife parks and anything else you can think of! I could not possibly have provided the education I did under house arrest.
Wow, I feel very special now. Mentioned twice in consecutive newsletters
Is there anything we can do to take collective action against locking down? This blog is brilliant journalism but feels wasted if it is only being read by the already converted. A reader mentioned yesterday the idea of publishing an open letter written by the various scientists who are against lockdown, of which there are many. If this is supported by powerful people in high places, this might be a goer.
I also feel an investigation needs to be undertaken examining the links between Neil Ferguson/Imperial College’s powerful and seemingly unchallenged influence in shaping government policy and the funding received from Mr Pro Vaccine himself, Bill Gates.
Could not agree more, I cannot understand why we are not taking some sort of action here! The letter sounds like a start, how can we start the process? Also, you are spot on with looking into Ferguson, I find it astonishing that a ‘vaccine’ department funded at least in part by the corrupt Gates Foundation is allowed to directly influence UK Government policy. Surely there is a conflict of interest here?
It is time for action now.
In my experience, when I have written in the past to eminent scientists / academics, I have had a response. Maybe all it takes is just writing to those we know are critical and see if they would join the action? They might also know some other people in high places who are dissenting?
http://inproportion2.talkigy.com/
https://swprs.org/a-swiss-doctor-on-covid-19/#latest
These links could be helpful in directing to researchers/doctors etc who could be worth getting in touch with.
I just checked, this was Willow’s idea.
Do we actually need a forum or wiki as well? Somewhere we can collaborate? Would Toby be willing to host it here perhaps?
I am glad people are bringing this up, finally – taking action rather than having this become a runaway train where we miss the point to change the trajectory and power up critical debate.
The lockdown will be eased at some point in the next 2 weeks, but the repercussions are just starting to show. I think so far many people have been treating this as an early paid summer holiday; caught up in the panic on one hand and cognitive dissonance on bigger agendas on the other.
The lockdown was just the beginning… we are now looking at months of being held in suspense over death rates, possible cures but most importantly the miracle cure – the vaccine, governments threatening a second lockdown and using the carrot and stick approach on the population, hefty fines for non-compliance in many countries, increased censorship of free speech, phone tracking devices being pushed, loss of privacy and data protection…. and on and on it goes.
IF one considered just for a moment, just for the sake of it, that the virus truly is on the level of a bad flu, easy for some, terrible for others, one is looking at one of the most far-reaching social experiments in totalitarianism in history – across the globe.
So yes we need to take action. Other citizens in other countries have been taking actions you just don’t see much of it in the media. There is only one petition floating about in the UK at this stage, but we need
1) openpetition / investigation into the true death rates of Covid-19 and proportionality of the response by the government and whether or not the lockdown was/is/would be justified in the future
2) openpetition / investigation into the Ferguson model, his involvement and sponsorship by the WHO/BG, and critical question as to why the government continues to rely on him despite disastrous results in the past
3) openpetition to challenge censorship of free speech and on social media platforms, especially that of professional people in the medical arena who are not complying with government agendas or views; accountability of the media in this epic hysteria, deliberate over and under reporting of issues as they see fit
4) Setting up a 2-3 page letter that can be used as a template by everyone as a summary to send to MPs, mayors, hand to friends, colleagues, etc, and challenge the medical and legal associations to speak out
Not one person can do this alone; so yes either a forum on this page would be great otherwise let’s host a zoom call and each can take on a bit.. it just all needs to be concise, clear, fact-driven, respectful, but to the point…
Thoughts?
We really need Ferguson’s non cleaned code to be examined. A support ticket has been raised with GitHub for it, but I doubt it will ever see the light of day. My son is a software engineer. He’s looked at the code that has been released and says it’s pretty appalling from a coding perspective. I’ve asked if he’ll write that up. Not sure how quickly he can do that though. And the model itself. Has that been peer reviewed now? I would have thought the Oxford team would be all over it. Anyone know if that’s happening?
At the risk of sounding harsh here we need to consider the clientele of care homes. These are not active, healthy individuals and in almost all circumstances have complex and medical and/or care needs, it’s why they are there in the first place. I would expect any infection brought in could be particularly “fatal” if easily transmittable.
So a maybe quick google will bring up evidence of that? And lo here’s an interesting piece about norovirus for example. In summary it suggests a norovirus outbreak sees increased mortality rates of 11% in care homes in the US states reviewed during outbreaks. Does norovirus go on the death certificates I wonder?
https://www.healio.com/infectious-disease/gastrointestinal-infections/news/print/infectious-disease-news/%7Ba5cbb876-72c0-49ed-a4e8-b41f15bfe387%7D/norovirus-in-nursing-homes-increased-mortality-hospitalizations
I suspect the scandal here of sending untested elderly back to care homes to deal with when untested for Covid to free up hospital space would be front page news but for the broader picture.
They are sending tested, positive patients back, and into hospices, and home to live with their also elderly spouse (and then a carer pops in once a day, and then spreads it to all the other houses)
Care homes have protocols if they have norovirus outbreaks. I think these are the basis for how they look at Covid. The question I have is how much life is being lost? We all know that moving to a care home is the end of life and that we don’t last long once this step is taken. This is why so many resist it. How do we weigh a suicidal 30-year old who loses 50 years of life against an 82 year old who gets cut short by 12 months?
BUPA have a study here on average stay lengths. The government doesn’t keep statistics.
https://eprints.lse.ac.uk/33895/1/dp2769.pdf
A tested, positive patient was ‘pushed out’ of the local hospital into the care home my wife works at, back when they were trying to empty the wards. I don’t suppose he was the only one they pushed out of the door. What staggers me even more than that is that the hospital did not make the home aware. I believe they only found out when he was already there, had a temp. and was coughing. They phoned the hospital and they then confirmed it. He infected someone else at the home during some nocturnal wanderings. Fortunately, just those two affected, and both have now recovered. One was 99!
A second point: an old chap (unconnected with the above) died. The home management called his GP to get a death certificate. The cause was put down as CoVid19. Home says ‘hang on, he didn’t have CV19’; GP: ‘he had a temperature last week’. Home: ‘Really? OK, so do we need to isolate anyone?’ ‘No, no need.’
Is there some points mean prizes thing going on with hospitals and GPs (as there is with everything else) for declaring a death? That’s shocking, and it’s happening near me too, friend of family is a hospice nurse, they’ve had to take 7 covid terminal patients, already terminal, then got covid, but she’s livid, as they have lots of vulnerable life limited people in there (and they’re a charity, rapidly going broke at the same time).
I sent these links to Toby the other day but he didn’t publish them, maybe they weren’t relevant enough at the time:
1. https://drmalcolmkendrick.org/2020/04/21/the-anti-lockdown-strategy/
Sending old people still with symptoms back into care homes is NHS policy at this time to keep hospital beds free… Dr MK has written a few superb blog posts on the whole lockdown disaster from the front line as a NHS worker / GP. Worth a look!
2. https://drmalcolmkendrick.org/?s=A+second+look&submit=Search
“A Second Look at Vaccine” from July 2019 is a blog post where he dissects the problems surrounding vaccines being touted as miracle cures in a one size fits all approach (he is generally pro vaccines), and illustrates the problems around no long term trials, general lack of engagement with side effects and big Pharma having complete indemnity for vaccines in general. A superb, fact-driven and brave look IMHO at one of the most divisive subjects on the planet from someone who DOES believe in science and the original thinking behind vaccines.
This is especially relevant as on 4 May the big Covid-19 vaccine summit will go down with Bill Gates at the front line telling us once again why the world needs to be in lockdown for 18 months until he can vaccinate us all…
This blog is one of the things that gives me hope every day! I was sadly disappointed when I came by this morning (East Coast USA) and saw yesterday’s column, and absurdly delighted when I revisited a bit later and Toby had posted a new column! Obviously I need more in my life, but the narrative has been so thoroughly overtaken by COVID that there is nothing. No variation in news stories. No hope for the future. The lockdown fan club will have us hide under our beds forever, because COVID is the only thing that matters.
It’s encouraging that there are so many skeptics here! Skeptics isn’t even the right word – how on earth did “COVID-is-a-deadly-plague-and-lockdown-the-only-possible-response” become the status quo, from which only the bold dare deviate? Absolute insanity.
Anyway, this blog by an Alabama doctor is really good (he uses an excellent American football metaphor to compare the infectiousness of influenza and Covid-19!): https://600wrec.iheart.com/content/2020-04-23-coronavirus-truths-and-lies/
I did read it. It is a political piece not a medical piece. The writer is a creationist and doesn’t believe in evolution. It’s in the interview at about 9 minutes. So one of this guy’s facts would be “Evolution is wrong”.
He has a few crackpot ideas at the end – the Chinese are loving this because they can buy real estate cheap. Right. And the total collpase of their largest export markets is OK for them? Then he lays in to the Democrats…..
It’s a good piece, well-argued and well supported by data. It is mostly medical. The politics comes at the end, and doesn’t affect any of the scientific arguments, though I agree with the author that at this point we need to look for explanations that go beyond epidemiology.
It’s not though. It’s not scientific and not that well argued. Covid is more lethal than flu. It just is. It’s not Ebola and it’s not a death sentence but it is worse than flu. That doesn’t mean “therefore let’s all lock down”. I am not saying that. I am saying this doctor is not being straight.
It might be more lethal than flu, by a factor of 2 maybe 3, but there’s still considerable uncertainty about this when you factor in how hyped Covid is and how we probably usually undercount flu deaths. We also have vaccines for flu.
I don’t agree that it is “hyped” – partly because I’m not entirely sure what that means. It is significantly worse than flu and that difference is enough to swamp the NHS if we don’t try to constrain the spread. We have seemingly slowed it. The big question is now what. We don’t have to trash the science to move forward. We need to look at the much wider picture. The lock down has a lot of very negative impacts that aren’t part of SAGE’s consideration.
The reason I got interested in the IFR was to try to estimate where different countries were in the courses of their epidemics by their reported deaths because this is more reliable than the reported number of cases, since in different places and at different times they have completely different ways of deciding whom to test.
Unless the IFR is ridiculously low like 0.001% or something, the strategy is going to be the same. Contain and eradicate early on if you can. If you miss the boat on that, try to make sure your health system isn’t overwhelmed.
We have missed the boat on eradication, and although some other countries (Iceland, Austria, NZ) have achieved that it’s still hard to see how they can maintain that situation. The time and place to do that was Wuhan in November.
The relevant number then becomes the CAR or clinical attack ratio. This is the percentage of the total population who need medical attention. Tegnell estimated 1% as a worst-case upper bound for this and figured Sweden would cope with common-sense social distancing measures. History is proving him right.
The WHO have the CAR somewhere around 10% or higher as they say 20% of cases are likely to be critical (if R0 were 2, then 50% of the population would end up infected, they estimate R0 as at least 2 probably higher).
The number of people who die is what it is. So long as you treated everyone as best as you could that’s all you can really aim for. In practice very little hinges on how fatal it is compared to flu.
Using lockdowns to try to reduce the burden on health services is a bit like treating a broken fingernail with radiation. It sure causes a lot of other problems and doesn’t really help.
There’s no way anybody is going to keep them up until there’s a vaccine so when they come out of them the deaths are pretty much going to find the equilibrium they would have done anyway. It just means you’re broke and dead rather than just dead.
A much better idea is actually sustainable social distancing measures that you can keep in place for a year if you need to. Things like: stay at home and go to bed if you have a cold. Deciding what these measures should be is what SAGE should be thinking about now, and no doubt they are.
I can agree with all of that! It’s a first for me here. I am very doubtful that SAGE does have a wider remit. I think the politicians are asking them narrow questions and not about the lock down adverse impacts. None of the politicians have suggested there is any balancing being done. “We are guided by the science”. They need to be guided by the sciences and economics.
And, at this point psychology; I can almost feel my mental health getting worse by the day, each day I get slightly less hopeful and positive. I’m lucky though; I have a balcony and a lovely wife. People are going to snap though, eventually. There’s a reason that confinement is used as a punishment.
Yes Thomas, I would include mental health as part of medical advice. There are many, many areas that ought to be “folded-in” to the decision making now. We can probably have a go at the excess child & domestic abuse. We have data on diseases not treated including cancer. None of the data is perfect – it never is. The Covid models aren’t perfect. It’s all estimates and risk weighted stuff. The government really needs to get in and look wider now the virus is seemingly contained.
BoneyKnee, you’re quite right here. It does present more danegr than regular flu, though far less than bird flu or the 1918 flu (believed to be some form of bird flu). Not enough danger to justify the lockdowns though. We need to recognise that covid-19 is “worse”* than flu so that lockdown zealots can’t try to claim we are ignorant of the effects of the disease.
*Worse meaning here more likely to cause severe cases in some proportion of the population, plenty of individual cases have been milder than flu. Asymptomatic influenza has, to my knowledge, never been observed. It is the percentage chance of serious harm we need when weighing disease severities, not what the average or mild cases are like. For influenza the chance is very low, for covid-19 it is a little higher, for the likes of bird flu, measles, SARS(original), or ebola that chance is much higher. And none of those ever resulted in national lockdowns.
The lockdown “protects” the people who are least likely to be badly affected. Meanwhile they throw the people who ARE likely to die from it under the bus. It makes absolutely no sense – unless there is an agenda. There’s certainly a Narrative. Mere facts don’t derail it.
Please check out Chris Snowdon’s refutation of the “tweaked 5 tests” story. (Velvet Glove, Iron Fist)
Fake news promulgated by bored journalists!
omg, this is wonderful https://velvetgloveironfist.blogspot.com/
https://velvetgloveironfist.blogspot.com/
I wanted to share this spoof of COVID journalism, written by an author who wishes to remain anonymous, because it’s too funny to keep to myself:
Length of 2020 Continues to Increase
Experts reported Friday that the number of days in 2020 is now up to 151, up 14 from just two weeks ago. By contrast, in January, there were reported fewer than 31 days. Days are now being added at a rate of 7 every week. “This rate of increase does not seem to be slowing,” reports Dr. Inu Meritte of the Tri-County Technical College’s Department of Culinary Hygiene, “and at this rate, we project that the total will reach over 365 before year’s end.”
According to most published data from the OPM (Office of the Pontifex Maximus), the WPDP (Weeks Per Days Percentage) is holding at slightly over 14%. “We are not seeing a change in DPWR at all, which suggests that we must continue the most stringent controls,” says Merritte.
There is some reported evidence of days extending back into 2019. “If we add the currently un-counted days in late November and December of 2019,” says Merritte, “the count is even higher.”
When asked about claims from right-wing websites that the inexorable passage of time, being our perception of the entropic principle inherent to the universe as we understand it, and also basic arithmetic, is neither interesting nor a valid basis for policy, Merritte said, “This is a dangerous position to take in the face of the ever mounting count of days.”
Professor Feil Nerguson has predicted we may see as many as 500,000 extra days in 2020 if we do nothing to stop this. He suggests we must cease all sales of watches, calendars and diaries with immediate effect.
Nerguson has advised the only way to prevent this crisis will be to stay at home indefinitely until sufficient suspended animation pods can be produced in order to prevent the population from ageing, and also to prevent time from being allowed to occur.
Prime Minister Jojo Bonson however added that through our hard work we were beginning to turn the tide and that there might be a glimmer of light at the end of the tunnel. If we pull together as a nation, he said, stay at home, and clap bravely for 1 hour every 7 days, we might just yet wrestle our invisible assailant to the floor and bring the total for the year back down to a still regrettable 365,
Can we see the model that predicts the 365 number or are Microsoft tidying it up?
So we have The Association of American Physicians and Surgeons writing in support of Dr Trump’s favourite drug. Who are they? They are not a medical body. They are a political advocasy group – very right wing. Wikipedia has this
The association is generally recognized as politically conservative or ultra-conservative, and its publication advocates a range of scientifically discredited hypotheses, including the belief that HIV does not cause AIDS, that being gay reduces life expectancy, that there is a link between abortion and breast cancer, and that there is a causal relationship between vaccines and autism.
Like all good doctors they oppose gun control and are against Social Security and public health care.
Toby Young will be well aware of all of this. The credibility of the AAPS is near nil in medical matters. It is not a medical group. Why do people have to push a cure? Hydroxychloroquine is juts one drug among many that will be being looked at. The last proper study by the USA Veteran Association said don’t use it. I don’t really care one way or the other. Whatever the truth is it would seem that the drug ain’t that marvellous for Covid. What is the agenda here? Is it to keep undermining people’s trust in the medical profession? Why post that ridiculous YouTube link with the young woman claiming hospitals are knowingly murdering patients?
https://en.wikipedia.org/wiki/Association_of_American_Physicians_and_Surgeons
The British Medical Association is a very left wing trade union and would of course be more to your taste. This organisation heavily invested in project fear at the time of the remain/leave battle and its then editor Tony Delamere said he would be emigrating to Germany if Britain voted for Brexit. Whether he did actually leave these shores is unknown.
A bit of whataboutery there? I’m not sure the BMA are pushing any treatment one way or the other.
Completely agree with RDawg’s latest post regarding practical action. Loads of confirmation bias available here, but now what ?
Don’t get me wrong, this site has been a huge release for me: to know others feel the same about the situation, to read thought provoking comments, to find data sources to research and read up etc.
But I am increasingly left with a “So what next” feeling. Realistically what can any of us do individually or collectively to have an impact – either on the press, the BBC, the government or ….
Strong words and views here are a great source of frustration offload and “told you so” moments, but how do we gather momentum for action ? And what action would / can that be ?
Ideally we need a very good QC and lots of money, and someone willing to be the public face of a legal challenge. Dare I mention Gina Miller, but we need the covid equivalent.
Have you seen this?
https://robintilbrook.blogspot.com/2020/04/challenge-to-lockdown-restrictions.html
Honestly I think the best course of action is just to start getting on with it. Life I mean. In whatever ways are available to us. If you can work, work. Get outside. Remain cautious in terms of distance between yourself and others (I think we can agree raves still aren’t the best idea at this juncture ;p) but get out and about. Be courteous to the police and other authorities but firmly refuse to be cowed by them.
As I’m sure someone said on one of the other pages – there’s a lot to be said for quiet resistance. I think more and more people are going to slowly start sticking their heads above the parapet in the next week or so, even if they generally remain in their fortresses, emerging briefly every thursday to bash their helmets.
Tbf I’m saying this as I’ve decided to go back to work on Monday, after weeks of avoiding it under the guise of ‘working from home’ aka being on call. But as a key worker my office has remained open and I have had the option of returning before now, but have been being a good girl keeping away. No more. I’m in the priveleged position of being ABLE to work so I’m going to take advantage. – Wow. How amazing does that sound now? ‘Privileged position of being able to work’?
Interesting point Farinances. I guess ultimately we can all take comfort in the fact that this lockdown WILL be lifted eventually. (Toby will also probably be relieved to have his life back again ha!) However, I am fearful about how things will look on the other side. The idea of indefinite “social distancing” and the potential of future lockdowns fills me with dread. Doing this just once has set a very uncomfortable precedent.
As a youth worker who supports young offenders, it frustrates me that I am being paid to stay at home. My job involves working 1:1 with vulnerable young people and delivering workshops in pupil referral units. None of this can be done from my living room, and young people don’t want to engage with me via phone or video chat. There really is no substitute for face to face work. Frustratingly I will just have to wait until the schools are allowed to open again and my director says I am allowed to do home visits again. It’s the lack of control that really gets me.
How frustrating for you. In a time where you could be of so much use, and do so much good, among people who are least likely to be affected healthwise but most likely to be affected economically, socially, etc.!
This might be relevant in regards to the care home deaths in recent weeks.
A government document, Covid-19 Hospital Discharge Service Requirements, published on 19 March, directed that elderly hospital patients be moved into nursing homes or other social care accommodation to free up hospital capacity. Unbelievably, given how poorly equipped most nursing homes are and the unique frailty of their residents, the document states: “Some of these patients may have Covid-19, whether symptomatic or asymptomatic. All of these patients can be safely cared for in a care home if this guidance is followed.”
Dr Wilson said: “To mandate that care homes should take back Covid+ patients with such a high risk of cross infection and high mortality rate in vulnerable residents seems unfathomable. Surely the sensible policy would have been to limit care home admissions and offer safer alternatives. The tragedy is that this was preventable, as there is capacity in the live-in care sector.”
https://robintilbrook.blogspot.com/2020/04/did-nhs-management-deliberately-spread.html
They could be using the EMPTY nightingale hospitals to treat the most vulnerable/care home covid positive patients. I just don’t understand how these people’s minds work. Or don’t work as the case may be.
Yep, plus they won’t take residents FROM carehomes that need hospital care, I commented about that yesterday, there’s also a Dr Malcolm Kendrick kicking up a fuss about this, his blog is worth a look.
I hadn’t realised that Prof Ferguson was a fervent remainer.
I suppose it’s far too cynical to wonder if his doom laden predictions are aimed at locking us down for as long as possible in the hope the damage caused leads to a reversal of Brexit.
No that’s much too cynical.
It is much too cyncial, I’m a remainer and I think lockdown is bonkers. I think class would be an interesting analysis, particularly that of opinion formers. Seems to me this is a posh panic.
I’m a Remainer. I believe in free movement and creating opportunities for my children which would be better within the EU, than out of it. However, that conversation is done. We have a more pressing one right now. One which could fundamentally change the lives of every single person with immediate effect and for an entire generation. One that is self-inflicted under the belief/ pretence of saving lives and some idealistic world where the state pays a universal income.
My personal opinion is the evidence points to the exact opposite of that in terms of detrimental consequences to society of prolonged lockdown, and it’s currently being ignored.
I agree that success is to be found uniting under a common goal and utilising growing evidence to strengthen that position, rather than entering needless arguments that end up counter-productive.
Thanks, yes I commented at length yesterday that I’m pretty much done with remain as a ‘camp’ as their behaviour towards the working classes was just revolting after the election, no wish to be on the team that calls people ‘gammon’ and like you say it’s moot now, that ship has sailed (despite still thinking we’d be better off staying). I’m all for being on team ‘sanity’ re lockdown, which I would hope is apolitical (and which is why I’m so annoyed that the response of our opposition was to harangue the Gov on ‘doing it better’ rather than questioning the policy per se, there was no brake on this at all). I’ve already been told that caring about the economy is ‘right wing’, ditto civil liberties, ditto fretting that nothing good comes out of complacency + economic depression + recrimination (which will surely soon follow) – maybe I’ve just read too many history books!
A “posh panic” is a fantastic way of putting it.
I’m trying not to get too bogged down in political division but when one correlates attitudes to Brexit and attitudes to the working classes (two things which we all know are often inextricably linked)……. I see your conspiratorial wink and raise you a nod.
But hey, given the amount of self-confessed Remainers on here admitting they sympathise (granted with the much-vaunted, eyeroll-worthy constant insistence that they VOTED REMAIN! of course ;p) with lockdown scepticism, I don’t think we should despair. There is sense in all ranks it would seem.
Only when it’s relevant to the conversation as far as I’ve seen. Weirdly on the Times comments I get called a ‘Brexiteer’.
Ehehehehehe, a likely tale. It’s mad.
Kinda like when gay people who are conservative get accused of ‘not being gay’. You’re a remainer who questions lockdown- so you’re not a proper remainer! Welcome to the club actually. I’m a left-winger who voted for Brexit, and apparently some sort of unicorn (despite the fact my political hero is Tony Benn whose position on the EU everyone seems to have conveniently forgotten about).
It is truly bonkers, that’s what I’m finding so hard to compute, how suddenly credulous people are. I lived in the EU for five years, that little country is my second home, so I really am a proper remainer, not that it matters now, we lost, but still. And I’m rapidly reviewing what I am politically after all this, the left campaigning for poverty might be a bit of a deal breaker (deal was pretty much broken before that for various reasons) but middle class lefties screaming for lockdown and wanging on about the evil tories killing people, whilst conveniently ignoring the very real health outcomes of poverty was eye opening to say the least.
Hopefully, in time, as more people start to see our side of this (because from the data coming out all over the world right now, and corresponding experts who are Ferguson-model-sceptical saying as such, it’s inevitable) it may become a balm of sorts that will heal some of the divisions we’ve seen. Sense will eventually prevail!
Well… apparently I still retain my hope in the human race!
I was not impressed by Toby’s article in The Critic mentioning ‘Remainiacs’, for linking Lockdown criticism to views on Brexit. Apparently the vast majority of our fellow citizens are Lockdown Supporters, so it is obviously a condition that crosses political divides. Critics can also be found across traditional political divides.
Lockdown Critics are stronger if we focus on the strenght of our argument, and avoid being associated with a political colour. It is too easy for Lockdown Zealots to dismiss our arguments if they can tarnish them by association with political views they already opposed.
Yes. I find Toby is linking in ideas and sources that are odd and political – far right like the The Association of American Physicians and Surgeons. I too think that this polarisation or is it a form of tribalism is damaging. The debate is about the pros and cons of the lock down and how to come out of it. This isn’t simply about what SAGE says about Covid. There are many other issues to balance. Rubbishing the hard science is not necessary. Calling Ferguson Strangelove just reduces Toby’s argument to name calling. You can accept what SAGE says today and factor in other elements – or even ask them to and add some other specialists. Trashing scientists is never good for society.
Reduces his whole argument, or just part of his argument? Is trashing some scientists ok? What if their science isn’t peer-reviewed? Are we allowed to trash them and/or their science?
Also something I’m increasingly learning throughout this shitshow –
How scientific is modelling? I think we all need to start questioning modelling after this.
These epidemic models are actually really simple. You can write one yourself in a few tens of lines of code if you’re so inclined. But they depend on the numbers you put in.
The number of deaths doesn’t even come out of the model, it goes in. All the model does is plot those graphs, but you can work out the total number of deaths and the total number needed to achieve herd immunity if you know the IFR and R0.
The fraction of the population you need for herd immunity is 1 – 1/R0, and the total dead is that result multiplied by the population size times the IFR.
There may be some small changes to those totals if the epidemic proceeds at a different rate due to lockdowns here and there (Wittkowksi had a good paper on this) but the differences are small.
Ferguson and the government just go on about models to give it an air of scientism. It’s actually just some very basic math.
I’ve co-written models to predict peaks in analytical spectra, used in turn to predict spectra for synthesised pharmaceuticals candidates. To optimise the calculations you use real data, massive amounts of it that have been scrupulously checked for their validity to use as the models basis for predictions. Even after this, the models output can still be utter crap and this is with sound control data.
Models contain what the modeller feels will enhance it but it has to be scientifically sound and relevant. Yet still models are littered with equations that have no business being in them, numerous fudge factors, etc.
The point is, if top of the market models, which contain excellent databases and control data still cannot be used with real confidence in the pharma industry, how in gods name can her majesty’s government use a model that has none of the above to drive policy? How we can possibly predict any numbers with any confidence for a disease with totally unconfirmed transmission parameters, unconfirmed lethality, etc? Even the shittest politicians on earth should have massive doubts about putting anything on Ferguson’s modelling yet the government has put everything in it. It truly is petrifying what were doing.
Yes, number of deaths is an assumption, based on estimates of how contagious the virus is and its lethality (IFR), not a result of the model, not a result of ‘the science’. The simulation model is about modelling the spread of the disease by contact reduction. This is the heart of the model and is pretty sophisticated by all accounts (although sophistication is no indicator of accuracy). But ironically it’s the view that ‘500,000 people could die if we didn’t do anything’ that the Government says is the science that it is following. It’s no such thing, it’s an assumption of the model that the Government is following; an assumption based on very limited data. This reflects Prof. Ferguson’s view that the virus is akin to the 1918 Spanish flu which killed 20 million. Proper scientific advice as to how lethal the virus is should have been ‘we don’t know yet’. To which a rational response would have been: OK we’ll keep an eagle eye on the situation, gather more data, get a clearer idea of what we’re dealing with, do random sampling to get a better estimate of the IFR, continue to advise the public to take the sort of precautions you would with a highly contagious virus, ramp up NHS critical care capacity just in case ie do more diagnosis of the illness before deciding to amputate the patient’s leg.
Number dead = IFR * (1-1/R0) * population-size
If we use 0.9% and 3 for the IFR, that works out as 360,000 for a UK-sized population of 60m. This is roughly where Ferguson’s model was at.
If we use 0.1% and 1.5 we get 20,000. When it’s all over 33% are immune or dead (that’s just 1-1/R0).
If we use 0.9% and 1.038, we also get 20,000. At the end of it all 3.7% are immune or dead.
If your health system is completely overwhelmed IFR at most doubles. Social distancing, lockdowns, etc. reduce R0.
The real numbers are likely to be somewhere between 0.1% and 0.9% and 1.5 and 3. The IFR will vary quite a bit depending on the age and vulnerability of your population and R0 varies quite a bit depending on population density.
0.9%/3 were reasonable numbers to put in based on what we knew around the start of March. But at this point it’s hard to believe that fewer than 3.7% in places like Italy, Spain the UK and NYC have had the infection, or that R0 was anything like as low as 1.038 with the (thankfully) half-arsed lockdowns in at least the last two of those places, especially given how late they started. Sweden would also have way more deaths by now. So either IFR or R0 or both is lower.
I think they know this. They also very likely have access to secret antibody test results from Porton Down. They’re continuing to defend the 250k estimate just so they can take the credit for reducing deaths to “only” c. 20k.
@BoneyKnee,
(Speaking personally, not as a moderator.) So we shouldn’t trash Trofim Lysenko? Or the Nazi “scientists”? Science – as distinct from scientism, which is what you’re espousing — is always open to debate and question. That is precisely the nature of science. Peer review is an institutionalised form of “trashing”, aimed at finding fault in new hypotheses. Anyone saying we can’t question scientists does so because they agree with what the scientist in question is saying, and don’t want those conclusions to be questioned. That’s more akin to religion than science.
*claps like a seal for Ian*
Sorry. I certainly didn’t mean scientist shouldn’t be questioned. As you say, peer review is a foundation of science. Calling Ferguson Dr Strangelove is not a critique. It’s done here a fair bit. The models are not “right” they are models. A model is not the thing itself. It is an approximation. Those in business know that business models don’t tell us the future they give us some ideas about what an opportunity looks like, its risks and rewards. In many ways modelling isn’t science. I think we probably agree to this point.
Models are better than back of the envelope stuff for complex problems. Even so the quick and dirty might offer some insight. I find the rubbishing of expertise an issue. The focusing in on Prof Ferguson as if he alone said “Lock down now!”. He didn’t. The analysis is what it is. Flawed but indicative. We know Covid can bugger up our health systems. The issue is how to manage it and what the costs are to us of avoiding death or full hospitals. Banging on about Ferguson doesn’t answer those very hard questions. I don’t believe SAGE has even been asked to look at it yet.
How much does the 77th Brigade pay per post?
It’s arguably the case that most of the great mistakes of history were made by “experts”, since it stands to reason that leaders don’t ask the advice of reputed fools. Questioning and even mocking the court or political advisors of the day is – absent an election or civil war – the only way we (as ordinary citizens) have to try to influence decision-making in the way we think is right.
In this case, Ferguson is a public figure – someone who professes expertise and is advising government – yet he seems to have made a series of wrongly catastrophic projections time after time. Of all the criticisms that Ferguson may reflect upon in later years, being called Dr Strangelove will I doubt be felt by him the most trenchant; and at this point if one sincerely believes (as many of us do) that a great deal of suffering has effectively been caused by him, the little mockery we dish out is hardly out of proportion, much less a cause for serious complaint.
Discussion on here and elsewhere is about the quality of the modelling by Imperial College and it’s reliability, as this has driven govt. policy. Yes, Ferguson personally did not say ‘Lock down now’ but his doomsday predictions had the same effect because govt was spooked by them. ‘Rubbishing of expertise’ is a perjorative term;. I would rather describe it as ‘peer review’; a fundamental part of the scientific process which may highlight flaws and weaknesses in an analysis.
Ferguson is not shy of issuing his instructions to the government, even in public.
“Speaking to BBC Radio 4’s Today programme, Prof Ferguson, of Imperial College London, said easing the lockdown after another three weeks would depend on “how quickly case numbers go down”.
…”And I should say, it’s not going to be going back to normal. We will have to maintain some level of social distancing, a significant level of social distancing, probably indefinitely until we have a vaccine available.”
https://www.bbc.co.uk/news/uk-52308201
Ferguson also wants to move faster. He says in the same interview:
Asked whether the government is moving towards having a lockdown exit strategy in place, Prof Ferguson said he would like to see “action accelerated” and called for more infrastructure.
“I’m reminded by the fact we had a Department for Brexit for government – that was a major national emergency, as it were – and we’re faced with something which is, at the moment, even larger than Brexit and yet I don’t see quite the same evidence for that level of organisation,” he said.
He also says on vaccines in the same interview:
“Remember, there are four coronaviruses that already circulate in human beings. They cause the common cold, and we don’t have vaccines for any of them,” he said.
Something is not being reported. Prof Ferguson is actually very transparent which government is not. He does not “issue instructions”. He is not the decision maker. He is one of many.
I’m not sure it’s relevant though. The government are still clearly implementing his model, its hard to dispute that. I’m sure there are many decision makers but they’re still seemingly making decisions based on conjective, debatable outputs from a disease model or at the very least heavily influenced by them. The question is, considering modelling of this nature is so unreliable, why government are treating its outputs as likely reality? They are at best guesses, and other less catastrophic models/opinions/hypotheses are equally as valid and yet totally ignored by government.
If any model predicted the end of world and it was scientifically top notch, peer reviewed, predicted well in previous events, etc, we’d just have to accept it, we’re in deep trouble.
Fergusons model isn’t this, its based as much as possible on data (new and legacy) but any disease, let alone novel, cannot possibly, with the best will and effort in the world, be accurately modelled to anywhere near the level that has driven government policy.
Err on the side of caution by all means, but causing the potential breakdown of the very fabric of society is erring to ridiculous, unwarranted levels of caution
Or, alternatively, listen to those who really know what they are talking about, since data inputs for models are thin on the ground and not so reliable in many cases:
https://www.fwdeveryone.com/t/puzmZFQGRTiiquwLa6tT-g/conference-call-coronavirus-expert
Dated 06 Feb
How many Covid 19 deaths in high density housing Hong Kong? Precisely four to date……
Ferguson has been spectacularly wrong time and time again. In fact he has never been right. That doesn’t stop him, or the government from following him.
We now have a considerable amount of data (although some of it has obviously been manipulated) is it not beyond the bounds of possibility that some other Authority might come up with something more, er, authoritative?
Here is something thought provoking:
I recently got into a debate with family members over the effectiveness of lockdowns, I tried to press them for evidence that they ARE effective, to which the response was “500k deaths predicted, we are only at ~20k now due to lockdown”. Clearly this relies on the studies being correct, but hey ho – why should they not believe an esteemed scientist? Incidentally, this argument DOES put the burden of proof back on me, I would need to prove that the studies were overdramatic, and not accurate.
Obviously there are just the cases of Sweden and Iceland to look at for this. Fortunately, Sweden has active scientists who ran the numbers, predicting rosy outlooks for Italy/Spain but MASS EXPONENTIAL DEATH in Sweden. Read it here: “Estimating the impact of mobility patterns on COVID-19 infection rates in 11 European countries”
https://www.medrxiv.org/content/medrxiv/early/2020/04/17/2020.04.13.20063644.full.pdf
This was written about 2 weeks ago. All you need to do is compare this to the actual death rate as of this week and laugh at the difference. Excerpt out of the report:
Love it.
I can’t convince my lot not to stand like seals clapping for fish every Thursday night…Drives me crazy
I note from Toby’s update today that ‘The R number’ has been added to the verboten phrases on RDawg’s swear jar list. I’ve mentioned the word, so I’ll accept the fine and have made a $10 contribution to Toby’s site to pay my dues.
So ‘The R number’ and the fact that the Government has changed the wording of its fifth test (effectively to keep R below 1), watering it down considerably. It used to stipulate that the Government would only start easing the lockdown if it was “confident that any adjustments to the current measures will not risk a second peak of infections” but now the words “that overwhelm the NHS” have been added.
There has been a really useful conversation elsewhere on the site about the absurdity of achieving a certain R value as a policy objective. With the amendment to the fifth test, R is not the critical factor, not the dial you watch to stop it going into the red zone – it is the capacity of the NHS. So, hopefully, we are back to where we were before mission creep led to the perpetuation of lockdown, only now with a significantly increased NHS capacity. There now is really no reason not to end the lockdown, as there’s enough wiggle room in the other four criteria to claim they’ve been met. The newly minted fifth test should not be a constraint – any signs of capacity being breached, then knock up a few more Nightingales – far cheaper than locking down the economy. Of course, ending lockdown doesn’t mean reverting to status quo ex ante (as Boris might say), because there will be a number of measures that it will be sensible to keep in place. In other words, getting back to where we were pre-Ferguson-panic: sensible, advisory measures to take when faced with a very contagious virus – maybe even back to a world where you quarantine the sick, not the healthy.
I hope my fine will cover multiple transgressions within the same comment so: would I be right in thinking that R is not an observed value but a modelled number? That may seem like a nerdy technical question but I think it’s quite important.
If it is a modelled number I am tempted to draw parallels with climate change as in: We have a climate emergency. OK, you mean we have an actual observable emergency? Erm, no, it’s just that our models predict that the climate will change in future such that we will have an emergency.
…and finally. Toby, I think you should sponsor a competition (prize $10) for contributors to the site, to find the best first name for baby Johnson. Whilst ‘Covoid’ might not be appropriate, how about ‘Ovid’?
Can I add ‘OUR NHS’ to the list? (Emphasis on ‘our’)
My opinion is that we should spend the summer allowing the infection rate to run as high as possible without overwhelming healthcare systems. We have all this extra healthcare capacity in place, people are all ‘psyched up’ to deal with CV19, so lets bring it on now. Surely we don’t want to leave it until the autumn for the rate to start going up again, that would be the worst time to handle any increase.
I don’t think there is going to be a vaccine, and even if there is, it isn’t going to as soon as we’re led to believe. We have to proceed as though there will be no vaccine, until there is.
(Yes, I do know there’s no evidence yet that weather/temperature affects the CV19 virus – but it’s a possibility)
Regarding a vaccine for CV19, and Bill Gates alleged involvement in it, I read a very good comment a few days ago, which was (paraphrasing):
I wouldn’t trust Gates to cure a virus in Windows 10, let alone people…
I don’t do conspiracy theories but did Prof Neil Ferguson programme his model to stop Liverpool winning the league
Yes, his model predicted that Liverpool would win the League by a margin of 575 points
Yes, finally the ‘mainstream’ are waking up with the comments of theresa may “we cannot have a situation where the cure for the disease does more damage than the disease itself”. Exactly what Trump said over a month ago / and me! Lets see what wider coverage this gets before the 90% believers also wake up from their state / sage / imperial college induced six week coma of “moronity”.
I think you’ll find much of the moronity is furlough induced, a lovely holiday for many, happy to sell their souls for a few weeks in the sun on 80%
I think you’re right and let’s not forget the public sector workers who are no doubt on full pay
Sister (teacher, no school age kids) responded when I told her on a family zoom call that I was praying things would be eased off soon that she hoped it continued into the summer as it was good for hard working and undervalued teachers to have some time off to recharge. Had to snap shut the laptop screen and jump up and down on the spot screaming for a few minutes before rejoining. I suspect this attitude is widespread with a strange willingness to ignore the economic reality of who pays the salaries.
We had a conversation with our daughter’s school teacher who was in school for the first time in 5 weeks yesterday bemoaning how busy she was. It’s a different world.
There’s those on furlough. For my workplace I would love to see it extended, personally I would hope to see it scrapped at June 30th. The redundancies that follow will jolt a few people basic into reality. Then there’s the increasing momentum I keep reading about universal basic income and job guarantees (really) and reclaiming the economy’ etc.
What we are doing is sending a vast proportion of hard-working, independent SME’s to the wall and all we will be left with a handful of juggernauts who have the financial capability to get through this. It defies logic. I’ve already written about the social and mental issues.
Let’s not even start on the precedent the world has set for when this returns, or the next thing, or if something serious for the majority of the population actually came along.
I’ve been saying this for awhile – right now, everything seems fine. Wait until lockdown is lifted and there are no jobs to return to. Then we’ll see how people react. I’m just continually dumbfounded by the laser-eyed focus on lockdown and NOTHING ELSE.
interesting article in the Helsinki times. They believe they might have ‘overcooked’ the lockdown and it will peak in the autumn!
https://www.helsinkitimes.fi/finland/finland-news/domestic/17606-finland-on-pace-to-face-peak-of-coronavirus-epidemic-in-autumn-says-thl-s-salminen.html
There’s an article? I’ve only seen a lovely picture of a tram…
“Salminen on Monday said to TT that Sweden’s strategy can lead to a higher mortality rate but also the epidemic dying out more quickly. He also emphasised that the final outcome will not be known until later.”
Reading these intelligent, articulate people speaking plainly and honestly immediately prompted a conversation with my wife and kids about whether we need to relocate to Northern Europe, or maybe stay in the US and start a political party or something more radical.
Minnesotans are supposed to speak plainly too, our Scandinavian heritage. But recent events prove that has now been lost.
I’d hate to abandon my country, but I have completely lost faith in the whole of our government, its decision making, its ability to think holistically about its actions, its simple responsibility to the people. How can I remain here, supporting this through taxes and contribution to GDP, intellectual property through the patent office, etc.? How can I remain silent and thus in passive support of this travesty of the most basic human justice? I would rather live in a socialist nation where I know exactly what I am getting than to be lied to every day, and to be subject to a community who willingly engenders the same.
We live under omnipotent robber barons disguised as sincere, bumbling busybodies. Just take a look at the world’s most dangerous nerd. The feigned incompetence is a strategy itself. A bit like Drunken style Kung Fu where the proponent appears to batter his opponent by accident.
Dr Vernon Coleman says it well:
“I would not be so committed to the notion that the coronavirus is being used to control us, if it were not for the fact that our freedom and our freedom of speech have been thoroughly torn apart. And, of course, no government anywhere could possibly be as inept as governments now appear to be – unless there was an ulterior motive.”
http://www.vernoncoleman.com/main.htm
I ‘get’ that the effect of the virus is being hugely exaggerated, I also ‘get’ that the populace is being manipulated and controlled using the virus as justification. What I am struggling with, is the simple question – WHY?? (and I’m not looking for daft conspiracy theories). Finally, why the fuss over care homes? These aren’t known as ‘God’s waiting rooms’ for nothing. You don’t go into a care home expecting to come out skipping like a Spring lamb, in fact you don’t expect to come out at all – it will be a mercy for many of them. I imagine the ‘care home operators’ May be concerned over an imminent lack of ‘stock’
Well part of the answer is in your first sentence. Honestly, are you confused as to why governments and large corporations should want more control and manipulation? You shouldn’t look for “daft” conspiracy theories but you should look for plausible ones because they are right there in your face and there is no point pretending otherwise. You shouldn’t abandon the word “conspiracy” just because the media has deliberately associated it with “daftness” or “lunacy”. Everybody understands that influential figures collude with one another behind closed doors. It’s nothing more complicated than that.
As to the care homes, you also answered that in the first sentence. I don’t think you are confused at all, you are perhaps just unwilling to accept your own conclusions.
I always like to have a gander at what our friends in power who meet annually for the Bilderberg Group meetings are chatting about. In 2019 it was:
– A Stable Strategic Order
– What Next for Europe?
– Climate Change and Sustainability
– China
– Russia
– The Future of Capitalism
– Brexit
– The Ethics of Artificial Intelligence
– The Weaponisation of Social Media
– The Importance of Space
– Cyber Threats
https://bilderbergmeetings.org/meetings/meetings-overview/index.html
Oh lord. I’m just watching the Daily Doom update. (More fool me).
The medical woman person (don’t ask me her name, all the talking heads look and sound the same to me at this stage) just said re: not quarantining people coming in on flights
“We have to be careful we’re not disrupting everything, for very little gain”.
Can they hear themselves?!
Needless to say another shoe got chucked at the screen.
The airports have been opened this whole time with flights arriving daily at Heathrow from Italy, Spain, New York, etc.
The horse has bolted, we’re locked in the stable, so any future quarantining of visitors is pointless and will completely destroy the tourism economy. In Scotland, tourism makes up 5% of GDP, worth around £6 BILLION(!) a year.
I am British and living in Singapore. I have read two linked articles on your recent newsletter:
1) Lockdown only made corona crisis worse, claim experts
Israeli professors’ mathematical model shows quarantine effects more damaging than the disease, which could better be controlled by precautions.
By Abigail Klein Leichman APRIL 28, 2020, 7:20 AM
2) The return of Project Fear
It didn’t take long for the Remainiacs to weaponise the coronavirus crisis
Which reference Singapore as not going into lockdown.
This is not true. At best, businesses are closed, schools are closed, only essential services (narrowing every day) are open and we must all wear face masks, even children as young as 3 when outside our homes. They even banned masked, distanced, household only children from scooting through the botanic gardens, and dog walkers from walking dogs inside private condos, Stopping to talk to someone outside of your household, at a distance whilst wearing a mask is risky.
At worst, we must show ID to enter supermarkets, move at an acceptable speed when outdoors or be shooed on by security or visitor services staff in the Botanic Gardens (my children committed the crime of stopping to watch a bug this week), all green spaces, beaches, etc., are taped off and we are herded onto pavements and pathways to discourage us going outdoors, ‘exercising’ as a family is not illegal yet, but it’s clear it is not preferred. Citizens are encouraged to report non-compliance via an App. Fines are a hefty $300 for locals, for foreigners like me we face instant deportation. People share photos of adults or children outside without masks on chat groups with calls for police action. We entered into four weeks of lockdown, for week 2 to see a four week extension to June 1st. Eight weeks locked down in total, at least.
Just wanted to set the record straight.
Wow. Thankyou for this.
Scary stuff. (I had an inkling all was not rosy- one of my uni friends lives in Singapore and has been keeping me updated)
Like others, I am really appreciating this site. What can one person do? I have written to my MP, shared this site with colleagues and tried to make the case with family and friends. Pray?
Not sure about today’s swear jar entries, most of them are clearly COVID buzzwords can be appropriately used in an anti-lockdown context too:
“The peak passed long ago, the R0 value is lower than 1. Because of the lag between infections and deaths we know that i nfections began dropping many weeks ago. We don’t need to fully complete the five tests, testing tracking and tracing isn’t so hard, lets give our NHS heroes a well deserved break from misery at home and end the lockdown”
The swear jar should be reserved for pure propagande phrases designed to further a sinister lockdown agenda, not for all the phrases inevitable in most COVID conversations.
Hi Iain,
The swear jar idea was a flippant, satirical comment I made in response to our bombardment of certain key phrases by the mainstream media. I don’t have anything against the phrases per se; but when such phrases are used to morally chastise those who question lockdown, it does become quite sickening.
For example, how many times have we been exposed to the message, “Stay home. Protect the NHS. Save lives”? It’s become something akin to Chinese water torture.
I’m not sure they prepared for how effective the brainwashing has been. People are now, it would seem, sat on their sofas having heart attacks because they’ve thoroughly absorbed the message.
Iain, I agree with the original swear jar, and the “Stay home…” lie is a disgusting piece of pervasive propaganda, I just didn’t think that the latest additions were of the same manipulative totalitarian quality as the original list of swear jar statements.
F****** Mask
To the tune of Bob Dylan’s Maggie’s Farm.
This song must be sung wearing a mask, to muffle the swearing.
I don’t wanna wear this f****** mask no more.
No I don’t wanna wear this f****** mask no more.
I wake up in the morning wash my hands an pray for rain.
I got a head full of ideas that are driving me insane.
It’s a shame he way they make me stay at home.
I don’t wanna wear this f***** mask no more.
Don’t complain about masks, complain about lockdown. Complain about Stasi neighbours turning on each other. Complain about cops who threaten to “search shopping trolleys” and “make something up” because they don’t like seeing someone outside. Complain about government(s)( all but Sweden’s it seems) which destroys millions of livelihoods. Complain about the starvation this is bringing on the poor and the lack of food variety it is bringing on the not so poor. Complain about the worlds billionaires getting 9% richer while all this sh*t goes on. Complain about the futures of the young being sacrificed so that someone on a ventilator can spend a little longer paralysed and sedated before they die. Complain about the cancellation of “elective” surgeries forcing people to spend months in agony. Complain about a media which cares only for deaths on front pages and not for lost quality of life. Complain about the whingeing fools who somehow think this is a morality tale and that by denying ourselves pleasure the author will write the final chapter to save us. We need to target our anger against an overbearing nanny state, not against things which somewhat work and maybe help the (unfortunately not yet immune) herd to feel less worried about going out.
Neil Ferguson, as many people know, uses a mathematical model to threaten us with the apocalypse on a regular basis: SARS in 2002, avian flu in 2005, swine flu in 2009, not to mention foot and mouth disease in 2001 which resulted in the needless slaughter of 12 million animals. Each time his predictions of mortality are wrong by several orders of magnitude. You wouldn’t bet money on a horse on the strength of Neil Ferguson’s model let alone close down a whole country. Why is the British government so in thrall to him?
Neil Ferguson is acting director of the Vaccine Impact Modelling Consortium (VIMC) based at Imperial College. This is funded by the Bill and Melinda Gates Foundation and by GAVI, the Vaccine Alliance. Interestingly, the British government is the largest sponsor of GAVI and has pledged to donate £1.44 billion between 2016-2020, money which, after many years of austerity, you would think it could ill afford. GAVI is in turn connected with the Digital Identity Alliance which believes, bizarrely, that “to prove who you are is a fundamental human right.” Vanessa Beeley attempts to unravel the tangled web in an article on UK Column. She says, “The scientific clique influencing government decisions is one that is incorporated into a for-profit Big Pharma industrial network which will, undeniably, benefit from the measures being taken by the British Government — a government that is financially embedded in the same complex.”
One doesn’t want to get too conspiratorial about covid19 and lockdown, but it does seem that huge amounts of money are being spent behind our backs in rather creepy ways.
Digital Identity Alliance which believes, bizarrely, that “to prove who you are is a fundamental human right.”
OK you have my attention. That line is scary. Are they trying to convince me it’s my human right to be monitored online?
They are saying exactly that.
Dave Cullen (Computing Forever) goes into this and a number of other articles that are available:
https://m.youtube.com/watch?v=k4NtMlTMJ74
The Rationalisation of Tyranny
All sources are listed here:
https://computingforever.com/2020/04/29/the-rationalization-of-tyranny/
The Digital Identity Alliance is a really worrying organisation. It seems to me their ultimate goal is tracking everyone, everywhere. It’s little to do with proving who you are; much more about revealing where you are.
The times is now scaremongering…. sorry, reporting…. that COVID has death rates as high as Ebola (presumably if you select a group of patients small enough to have the same demographics)
https://www.thetimes.co.uk/article/covid-19-death-rates-are-comparable-to-ebola-for-hospital-cases-nhs-study-finds-p75frbq33
Yep, sadly many of the MSM, including the BBC are running with this story:
https://www.bbc.co.uk/news/health-52473524
This is disgraceful journalism, and incredibly misleading. Ebola has an IFR of between 25-90%. Covid-19 is around 0.1 to 0.5%, depending on which source you read.
What are the media playing it? This is scandalous.
That is the stupidest headline I have ever seen. We should be flooding the BBC with complaints over this.
It’s about keeping us as scared as possible for as long as possible. Scared people are easier to control.
And its not as if the BBC don’t have previous on this, e.g. Panorama (TR’s expose` of John Sweeney), or the latest Panorama episode which included far left Corbyn supporters to bash the government over PPE.
Uuuuuggghhh I take back my comment comparing newspapers to TV favourably
That’s my subscription cancelled, that’s not journalism.
https://off-guardian.org/2020/04/29/lokin-20-the-lockdown-regime-causes-increasing-health-concerns/
Just read the WHO guidelines for testing for covid 19- If the patient is in an area where covid 19 is not known to be prevalent then – “A positive NAAT result for at least two different targets on the COVID-19 virus genome, of which at least one target is preferably specific for COVID-19 virus using a validated assay (as at present no other SARS-like coronaviruses are circulating in the human population it can be debated whether it must be COVID-19 or SARS-like coronavirus specific);
In other words it is only preferable if the genetic sequence is actually covid 19. It doesn’t have to be. It could be from a related virus. In fact, it says, it is debatable whether it is necessary at all to get a sample specific to the covid 19 virus. The very unscientific reason is because if there are no other Sars-like viruses at the minute it can’t be anything else! (How can they possibly know that no other SARS like viruses are circulating? Are they omniscient?)
If the patient is an area were SARS is prevalent then
“In areas where COVID-19 virus is widely spread a simpler algorithm might be adopted in which, for example, screeningby rRT-PCR of a single discriminatory target is considered sufficient. ”
So only one target is now needed.
It then goes on to say “one or more negative results do not rule out the possibility of COVID-19 virus infection.”
It then lists all the reasons why the test might produce a false negative but does not mention false positives for which the PCR test is notorious. In other words keep testing until you get a positive result.
It then goes on to say don’t bother isolating the virus. Yet isolating the virus is the only definitive way of knowing that the virus actually is, or maybe that’s the point. If it isolated maybe it will not turn out to be new virus at all but one that has been about for ages.
file:///C:/Users/smcmu/Downloads/WHO-COVID-19-laboratory-2020.5-eng.pdf (relevant info is on page 2)
This article by Rod Liddle is unbelievable:
https://www.thesun.co.uk/news/11512177/boris-must-stop-breakdown-of-lockdown-or-nastier-one-on-way/
I did a double take when reading it, having to check it was actually him.
Last time I read an article of his he was talking about what size hole you need to make in a mask to pass a fag through. Now he’s spouting nauseating stuff like this:
“Our Government has got to stick to its guns.
In my opinion it was a little late imposing restrictions on movement in the first place.
But at least in the end it did the decent thing — putting the health of the most vulnerable of our country above the need to make money.”
I feel a bit sick.
He does this sometimes our Rod. He had a pop at the badger cull thinking he was some kind of farming expert not accepting that many farmers’ herds were TB free for the first time in 20 years in my area of Gloucestershire and the west country after a few rounds of the cull. I do love Rod but sometimes he talks out of his backside.
A LOT of people who should know better have been sucked in to this. Unfortunately there are quite a few writers and commentators I can no longer take seriously because of the terrible judgment they have displayed in this affair.
And now the WHO is in love with Sweden’s model? Are we perhaps seeing some light indicating that this tunnel might have an end? And that we’re not just all buried alive….
https://nypost.com/2020/04/29/who-lauds-sweden-as-model-for-resisting-coronavirus-lockdown/?fbclid=IwAR21SVv82J1smTiXGS7tEbnAB46pXgF7cTU_mJN0WnECx6ty_o3QkC3Gldc
I think I foresaw this response. If Sweden’s strategy turned out to be successful and it wasn’t possible to force them to change their approach, or trash their data or massage everyone else’s while maintaining the fear, the only response the zealots could make would be to re-evaluate Sweden’s approach as being ‘lockdown in all but name’.
As a fellow physics grad I am embarrassed at the lack of scientific method from Ferguson. There was no evidence for this lockdown and he is ignoring all new evidence…
https://www.spiked-online.com/2020/04/30/how-the-lockdown-fuelled-the-care-homes-crisis/
It’s awful what we’ve done to the elderly, hospitals are also refusing to take patients from carehomes, even when they clearly need hospital treatment, which might explain the overall rise in deaths.
Of interest:
Sweden’s vindication is complete; Graphing the actual coronavirus epidemic in Sweden against the pro-Panic side’s wild projections
With this flu-virus epidemic now in clear and sustained decline in Sweden, we can measure the magnitude of their epidemic against the Neil Ferguson predictions for what a Swedish-style response would mean:

It looks like he was at least 75x too high.
Great link.
It identifies one of the big questions for any forthcoming enquiry:
Given Prof. Ferguson’s previous modelling track record of alarmism, with previous consequent massive collateral damage, how could it be that his model was used for decision support, again…..?
https://www.anti-empire.com/lockdowns-boosting-who-now-lauds-sweden-as-a-model-for-other-countries-to-copy-going-forward/
Finally, I understand what all the fuss is about:
http://inproportion2.talkigy.com/images/momo_ages_200429.png
England suffered, two weeks ago, a spike in all causes deaths of age group 15-64 unparallelled anywhere else in Europe, probably in the developed world.
For all we know, that graph is still rising…….but only in England, nowhere else in Europe.
Why?
That’s a really wide age gap, wondering if that would be at the older end untreated heart symptoms, stroke, cancer and other treatable issues? A&E admissions are 75% down, 2 million procedures cancelled, and I read somewhere suicide is up (either that, or we are all in denial and heartless!). Is it broken down by age further anywhere? I’d also like to know what’s going on with maternity, as family member is heavily pregnant, all her antenatal care is cancelled, she has to give birth alone on a ward with pot luck on the doctor, and no post natal care, where I live we don’t have a stellar record on not killing mothers and babies as it is – she’s in her early twenties, and scared out of her wits.
Questions to which, no doubt, all here would like answers.
Apologies for the slightly gnomic post above. Had to sweep out (on a perfectly legal, within guidelines, but officially frowned upon, for some unknown (or not really) reason), exercising before the high viz tabard wearing chief air raid warden mentality are about.
Further detail re age group further breakdown will probably have to wait for the ONS monthly analysis, like this for Covid 19 figures for March 2020:
https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/bulletins/deathsinvolvingcovid19englandandwales/latest
For what it is worth, two possible conclusions immediately spring to mind:
1. Healthcare outcomes, for whatever reason, for age group 15-64 in England are a great deal worse in England than possibly anywhere in the developed world
2. Mortality figures for the period in question have been massaged to produce a politically convenient spike by bringing forward figures that would normally have been registered later, improbable, inconceivable, as that may be…….Nevertheless, when you have excluded the impossible……etc…..etc
Time will tell…….
But you put your finger on the single most serious matter of this whole fandango: the terror, panic, induced in the most vulnerable. For that reason, if for no other, any future enquiry must be utterly independent and utterly ruthless. Level of confidence in that happening? You know the rest………
https://www.youtube.com/watch?v=Jvr6X054xLY
“Mortality figures for the period in question have been massaged to produce a politically convenient spike…”
It’s felt that way from the start. The authorities gleefully exaggerating the whole thing, even though, in the end, it makes them look incompetent.
Did you see that ploy they used the other day to ramp up the fear? Big colour photos of children with something called Kawasaki disease, “possibly” triggered by Covid-19, but only a handful of cases – seemingly normal for this disease. Matt Hancock is “very worried” by it, apparently.
It may produce the result they want – compliance from the masses – but at what cost? Until the WHO/Gates/Imperial syndicate produces their ‘vaccine’, parents will always have this at the back of their minds, totally out of proportion to the risk.
Was Public Health England’s antibody tests results ever released ?
On the 9th of April at the daily press conference Sir Patrick Vallance mentions about it here at (19:50)
And Oliver Wright asks a question about it at (21:42) to which Sir Patrick Vallance answers at (23:32)
https://www.rev.com/blog/transcripts/united-kingdom-covid-19-briefing-transcript-april-9
I am waiting for this! It will show just how many people have already had it.
One country you will never hear much about, as the WHO refuses to acknowledge it even exists, is Taiwan. 22 million people, right next to China, lots of population flow back and forth, and how many deaths they had? SIX. New Zealand? 19. How did they do it? By closing borders completely and quarantining returning citizens. They have had NO lockdown internally. So, almost no deaths, no lockdown. Our politically correct leaders and scientists insisted we keep borders wide open to avoid ‘stigmatising’ foreigners, and people die as a result.
Your point is further underlined by a study into measures taken in Hong Kong, but no lockdown!
‘Our study shows that non-pharmaceutical interventions (including border restrictions, quarantine and isolation, distancing, and changes in population behaviour) were associated with reduced transmission of COVID-19 in Hong Kong, and are also likely to have substantially reduced influenza transmission in early February, 2020.’
https://www.thelancet.com/journals/lanpub/article/PIIS2468-2667(20)30090-6/fulltext
Hong Kong has a great deal of knowledge regarding coronaviruses:
‘At the University of Hong Kong, Nicholls has spent the past 25 years studying coronavirus and he served as a key member of the team that characterized SARS. The Hong Kong University Faculty of Medicine’s Clinical Research Centre also created the world’s first lab-grown copy of novel coronavirus, according to CNN correspondent Kristie Lu Stout, giving researchers a major breakthrough in understanding the behavior of the virus.’
That refers to Professor John Nicholls a clinical professor in pathology at the University of Hong Kong and expert on coronaviruses
And guess what he said, 06 Feb :
‘So my thinking is this is actually not as severe a disease as is being suggested. The fatality rate is probably only 0.8%-1%. There’s a vast underreporting of cases in China. Compared to Sars and Mers we are talking about a coronavirus that has a mortality rate of 8 to 10 times less deadly to Sars to Mers. So a correct comparison is not Sars or Mers but a severe cold. Basically this is a severe form of the cold…..This virus will burn itself out in May when temperatures rise. Wash your hands.’
‘Sunlight will cut the virus ability to grow in half so the half-life will be 2.5 minutes and in the dark it’s about 13m to 20m. Sunlight is really good at killing viruses. That’s why I believe that Australia and the southern hemisphere will not see any great infections rates because they have lots of sunlight and they are in the middle of summer. And Wuhan and Beijing is still cold which is why there’s high infection rates.’
‘HK (Hong Kong) has far more cleanliness (than China) and they are very aware of social hygiene. And other countries will be more aware of the social hygiene (than China)…..’
https://www.fwdeveryone.com/t/puzmZFQGRTiiquwLa6tT-g/conference-call-coronavirus-expert
Covid 19 deaths in Hong Kong? 4, in a high population density city. Hong Kong weather today? A pleasant 26 C, mainly sunny!
There are plenty of real experts around who know what they are talking about…..but no-one appears to have listened to them.
is it really true there was no lockdown in HK? I am finding conflicting reports. This is potentially a great case study.
Exactly. There are countries that dealt with the virus successfully, and those that didn’t. We chose to follow the example of those that didn’t.
On Taiwan, a friend of mine who was there in November said they were hearing rumours even then of a new virus coming out of China. They didn’t wait or get stifled by political correctness, but acted at once with entirely sane measures which could easily have been implemented here too, instead of the ‘nuclear’ option.
Just before the lockdown, a doctor I know told me the NHS was doing its best to learn from and imitate the Italian response… er…..??
Interesting anecdotal (ok, I know, but still) ‘evidence’ about low demand for tests.
https://unherd.com/thepost/stop-obsessing-over-the-100000-test-target/
Finally…170 scientists and researchers have got together and issued a joint statement concerning the deployment of the NHSX contact tracing app.
https://drive.google.com/file/d/1uB4LcQHMVP-oLzIIHA9SjKj1uMd3erGu/view
Maybe we can approach them to band together to address other concerns or use that kind of template to that ourselves?
I thought it would be interesting to have a look at the most politically incorrect country in the world, Belarus, and how they are dealing with the Covid-19 pandemic. All information is from Wikipedia and the actual epidemic curve is extremely informative and much better than Worldometer.
The first case was an Iranian student 28th Feb but very quickly there were sporadic and increasing cases in clusters indicating local transmission but the real explosion was in the beginning of April. Different from neighbouring Russia with a more “Western European” style with tourist coming back infected and then the explosion of case.
Belarus did ambitious testing and closed borders, quarantine, contact tracing and isolation of cases. The only social distancing was prolonging the ordinary spring break in schools with two weeks but no other social distancing at all. A WHO delegation in April noted, in a very diplomatic report, the very ambitious old-fashioned approach with testing, contact tracing early on and isolation but recommended social distancing measures school university closing, stopping mass gatherings etc.
Not something for Europe’s last dictator, Lukashenko.
Quotations” “You just have to work, especially now, in a village […] there, the tractor will heal everyone. The fields heal everyone”. Playing ice hockey “”it is better to die on our feet, than live on your knees […] sport, especially on ice, is better than any antiviral medication, it is the real thing” “People are afraid. Thus, I want to tell them the following: not a single person had died from coronavirus in our country. Not a single one! They died from a bouquet of chronic diseases”” “Utter nonsense. Children cannot wear these masks, especially in schools. There was no such requirement. If there are those who required it, they will answer for it. It’s better to open the window and let fresh air in”
At least you can say that you cannot accuse him for political correctness.
How are they doing in the epidemic? It seems to follow the same pattern as everywhere and they don’t seem to have reached the peak yet but there is a slowing of the increase the last days. Deaths and cases are well below the number in the UK per capita at least so far. It would be fascinating if someone studied the Belarus pandemic afterwards, especially if the March cases indicated massive asymptomatic spread before the explosion of cases in April.
The last dictator in Europe must also be laughing seeing how many tinpot dictators have been created in Italy, Spain, France and the UK by this pandemic.
awesome account. I have appreciated your comments very much. Would you mind if I shared this?
also are there some links you could share? It is OK if they aren’t in English.