

A child sitting at a desk for nearly two hours in silence, wearing a mask, puts up her hand to ask for help. The teacher steps out from behind a screen wearing a mask and puts on a visor. The pupil also puts on a visor. The teacher approaches the pupil and stops six feet away. The child points to her book and asks a question.
Is that what we want? Is it necessary?
Masking children is tragic, unscientific and damaging, according to the American Institute of Economic Research (AIER). Worse still, according to Dr. Paul Alexander, masks offer “zero protection”. The requirement that our children cover their noses and mouths for six to seven hours per day whilst at school – which remains a school-enforced requirement in Northern Ireland, acting on ‘guidance’ from the Government – is unnecessary and educationally destructive. It is self-evidently unhygienic. Furthermore, masks are harmful. Many scientific studies have confirmed the harmful physical, psychological and behavioural effects of mask wearing. To start with, we know that reduced oxygen levels increase anxiety, fatigue and brain fog, and decrease learning capacity.
Dr. Margareta Griesz-Brisson, Director of the London Neurology and Pain Clinic, is one of Europe’s leading neurologists. She states that: “To deprive a child’s or an adolescents’ brain from oxygen, or to restrict it in any way, is not only dangerous to their health, it is absolutely criminal. Oxygen deficiency inhibits the development of the brain, and the damage that has taken place cannot be reversed.” She refers to the acute warning symptoms such as headaches, drowsiness and a reduction in cognitive function. Dr. Alexander adds: “There is tremendous psychological damage to infants and children, with potential catastrophic impacts on the cognitive development of children.”
A review by Covid data analyst organisation Panda confirms these adverse effects including headaches, dizziness, shortness of breath and psychological impacts.
What are the psychological effects?
I was walking past a mother with a three-year-old child, when immediately the child grabbed her mother’s leg and hid behind her. The mother said, “She won’t meet anybody.”
Do we imagine that instilling fear into young minds will have no long-term effects?
What does the science say?
A widely known experiment called the ‘still face experiment’ reveals that children become emotionally distressed when they are unable to see and reciprocate facial expressions. According to these findings, having children spend time around people whose facial expressions are masked could have potentially disastrous consequences for their social and emotional development.
Dr. Raj Persaudi, a Consultant Psychiatrist, explains that the brain fills in the gaps in what we know about others and so the brain speculates on what the mask is hiding. He says: “In a pandemic the face mask looks like it might be concealing a dangerous infection. Filling in the gaps in what you know about others but doing so under background conditions where the brain projects threat onto the outside world, is now linked to serious mental illness.”
The message projected by masks is clear: You are a danger to me, and I am a danger to everyone.
What does this mean for the primary purposes of school?
Education requires an atmosphere conducive to learning. Learning cannot take place in an atmosphere of fear and anxiety, or where the child is unable to learn due to oxygen deprivation.
Teaching and learning require unimpeded visual and oral communication. Good teaching involves a variety of strategies, which take into account the different learning styles of pupils. It involves interactivity, group work, teamwork, discussion and detailed complex explanations. Imagine a question-and-answer session, a drama lesson, a language lesson, a poetry reading, a role-play session, or a singing lesson with masks.
Do we not value choirs, clubs, drama productions or sport? These all play an important part in children’s education and development. The development of leadership, teamwork and negotiation skills are enhanced through children’s participation. The insight gained by watching children participate in a range of activities enables teachers to recognise and value attributes such as commitment, leadership, and reliability. Important engagements with outside agents such as authors, sports coaches, careers officers, counsellors, translators, actors and artists are also inhibited by the wearing of masks.
Socialisation is a vital aspect of education.
Children with special educational deeds require personal contact with their teachers. For many, facial expressions provide reinforcement, and these visual clues are vital. Children on the autism spectrum need to be able to recognise facial expressions as part of their ongoing development. Teachers often assess the degree of understanding of their teaching from the facial expressions of their pupils. Expressions are essential in gauging emotions and for teachers to detect essential non-verbal communication around deep feelings.
Are children at risk and do they transmit SARS-CoV-2?
There is plenty of research confirming that children, should they contract the virus, are almost totally unaffected. Professor David Spiegelhalter, Chairman of the Winton Centre for Risk Management, and a member of the U.K. Government’s advisory body SAGE, using figures from the Office for National Statistics, reports that a five to 14-year-old has a one in 3.5 million chance of dying from COVID-19. And according to Heneghan and Oke, the Infection Fatality Rate for children and young people is “near zero”. Furthermore, in a systematic review, Ludvigsson concludes that in the first wave children were not the main drivers of transmission to adults, particularly the elderly.
During 2020, teachers were no more affected by COVID-19 than the general public, according to an analysis carried out by the Office for National Statistics. John Ioannidis, Professor of Epidemiology and Statistics at Stanford University, has estimated the survival rate after infection for healthy people under 70 at 99.95%.
All this evidence means that children are at very low risk from COVID-19.
But do masks work?
Scientific evidence from around the world is quite clear: masks do not work.
Panda reports that when we compare the epidemic curves in places with and without mandates, the infection curves look similar. In fact, we observe a higher number of infections per 100,000 of the population in places with mask mandates.
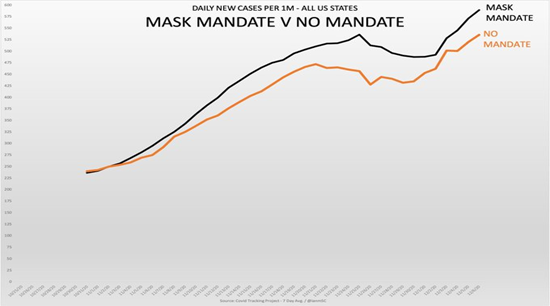
These findings are confirmed by recent American research carried out by Guerra and Guerra into case growth in states which had a mask mandate and those which did not. Their research showed that mask mandates were not associated with COVID-19 case growth. This finding was supported by Justin Hart, whose team’s research found that the group of states with a mask mandate did not have lower case numbers or growth rates than the group of non-mandate states in autumn 2020, as illustrated by Figure 1 below.
The Association of American Physicians and Surgeons concludes: “Wearing masks (other than N95) will not be effective at preventing SARS-CoV-2 transmission, whether worn as source control or as PPE. Surgical masks are loose fitting. They are designed to protect the patient from the doctors’ respiratory droplets. Their wearer is not protected from others’ airborne particles. The designer masks and scarves offer minimal protection. They give a false sense of security to both the wearer and those around the wearer.”
In the U.K., according to Carl Heneghan, Professor of Evidence-Based Medicine at Oxford: “There is no evidence that masks are protecting children and teachers in schools.”
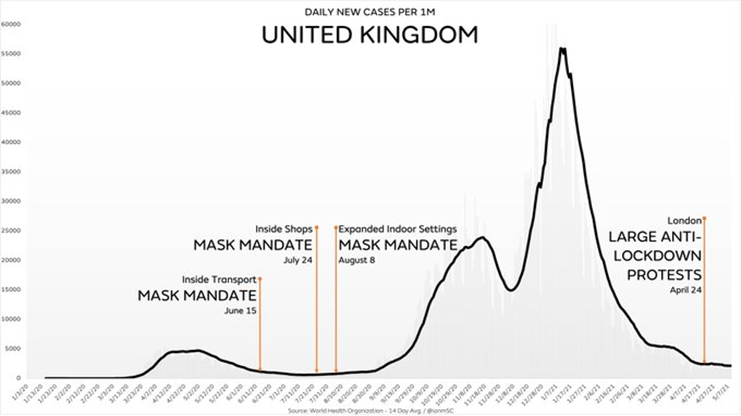
Figure 2 below shows that the effect of the graduated mask mandate was non-existent and also confirms that cases rose after the mandate.
A German study, written by the GMI Research Group reported a range of physical and behavioural side effects of masks in children, of which the chief ones were irritability, headaches, difficulty concentrating, less cheerfulness, fatigue, inability to sleep, anxiety and impairment of learning.
Worryingly, the authors added:
There are no manufacturer-independent studies on the use of masks for children and adolescents and due to the unknown materials used, there are no findings on the potential protective effects or side-effects of the often home-made ‘everyday masks’ worn by the majority of children.
Masks remain at the centre of the fear agenda; their continued use ignores their ineffectiveness and the harm they are doing.
The Government’s own recently published Evidence Summary for the use of face coverings in education settings found no statistically significant effect on transmission from facing coverings (0.6%) – the evidence showing they serve no purpose in controlling the spread of Covid.
The same Evidence Summary accepts the harm inflicted by face masks in class:
- 80% of pupils reported that wearing a face covering made it difficult to communicate, and more than half (55%) felt wearing one made learning more difficult.
- Face coverings may have physical side effects and impair face identification, verbal and non-verbal communication between teacher and learner.
- 94% of teachers thought that wearing face coverings has made communication between teachers and students more difficult.
The World Health Organisation (WHO) gives advice on how to use masks. It states that “the appropriate use, wearing, and cleaning are essential to make them as effective as possible”. It goes on to give advice on how to dispose of the mask safely, on how to fit a mask properly and the appropriate material of which the mask should be made.
I have difficulty imagining schoolchildren following such detailed advice.
The WHO also advises that the decision to use masks for children aged six to 11 should be based on the following factors:
- Whether there is widespread transmission in the area where the child resides.
- The ability of the child to use a mask safely and appropriately.
- Access to masks, as well as laundering and replacement of masks in settings such as schools and childcare services.
- Adequate adult supervision and instructions to the child on how to put on, take off and safely wear masks.
- Potential impact of wearing a mask on learning and psychosocial development, in consultation with teachers, parents/caregivers and/or medical providers.
Each of these conditions is critical. Schools are not equipped to ensure they are met.
Beda Stadler, Emeritus Professor of Immunology at Mainz University, expresses it clearly: “If you are young, you are not in danger, yet in many countries they are forcing six year-olds and above to go to school with a mask on. This is total nonsense.”
WHO advice for children over 12 reflects adult advice, but in my experience the limitations and reservations expressed above apply to all children in a school setting.
I should have thought that, given the obvious unhygienic nature of masks, governments would have conducted detailed risk assessments to establish their safety before requiring children to wear them.
Dr. Gary Sidley of the HART group sets out the core criteria for such an assessment. He recommends the assessment of:
- Oxygen levels at the start and end of the day.
- Impairment to concentration and ability to learn.
- The effect on children with hearing difficulties and special education needs.
- Impairment of psychological well-being.
- Potential harms of repeated use of dirty cloth masks.
- Impairment to non-verbal communications.
Why has this not been done?
Some final thoughts.
Where is the attempt to balance the miniscule risk to children from COVID-19 against the widespread potential for harm?
Article 3 of the United Nations Convention on the Rights of the Child states: “In all actions concerning children … undertaken by public institutions … the best interests of the child shall be the primary consideration.”
We are not putting the rights and needs of the children first. This is a disgraceful abuse of power against a sector of our society with no power to resist.
As the anti-Nazi German Christian martyr Dietrich Bonhoeffer said: “The test of the morality of a society is what it does for its children.”
It is time to unmask; our children have suffered enough.
Hugh McCarthy is a retired Headteacher in Northern Ireland. Until recently he served as a Director on two of the province’s main education councils and he remains a ministerial appointment on one.
Postscript: It has been pointed out to the Daily Sceptic that some experts maintain that mask-wearing does not inhibit oxygen flow. The website of the World Health Organisation says that “the prolonged use of medical masks when properly worn, DOES NOT cause CO2 intoxication nor oxygen deficiency”. The non-profit organisation Asthma and Lung U.K. says on its website that “most people with a lung condition, even if it’s severe, can manage to wear a face mask for a short period of time. Wearing a mask does not reduce a person’s oxygen supply or cause a build-up of carbon dioxide.” The American Academy of Paediatrics states that “masks have not been shown to affect a child’s ability to focus or learn in school. The vast majority of children age two or older can safely wear face masks for extended periods of time, such as during pre-school or at child care.” The organisation adds that “wearing a face mask will not affect your child’s lungs from developing normally. This is because oxygen flows through and around the mask, while blocking the spray of spit and respiratory droplets that may contain the virus.”
While that may be the view of some experts, Hugh McCarthy cites other experts, as well as scientific studies, to back up his claims about the harmful effects of making children wear masks. Indeed, the WHO, in its December 2020 statement on masks, said: “The potential disadvantages of mask use by healthy people in the general public include: headache and/or breathing difficulties, depending on type of mask used… disadvantages for or difficulty wearing masks, especially for children, developmentally challenged persons, those with mental illness, persons with cognitive impairment, those with asthma or chronic respiratory or breathing problems…”








