
Much of the developing world continues to suffer serious casualties from COVID-19. But some wealthier countries are groping towards the end of the pandemic. Based on their experience, it is now clear that neither eliminating the virus, nor vaccinating against it, offer a way out. Even if everyone is vaccinated, we will still need to learn to live with this disease and, above all, to restore a saner evaluation of risk.
The Lunacy of “Zero Covid”
As Australia clearly shows, a ‘zero Covid’ approach is not a way out of the pandemic but only prolongs the agony. Australia is exceedingly boastful of its record during the pandemic, recording under 31,000 cases and just 910 deaths. However, Australia has not managed this feat thanks to a well-designed pandemic preparedness system. In fact, it was no better prepared than most neoliberal states, collapsing into extremely costly emergency lockdowns and internal and external border closures. Prolonged lockdowns through 2020 failed to eliminate the disease, and governments failed to build the healthcare capacity necessary to deal with Covid patients when the country is not locked down. Consequently, today, all it takes is a small handful of cases to trigger state-wide lockdowns. The entire state of Victoria (population: 6.9m) locked down two weeks ago over 18 cases. Australia is locked in a doom-loop of lockdown-unlock-lockdown.
Australia’s ‘zero Covid’ approach has also meant agony for thousands of its citizens stranded overseas. Some 34,000 remain unable to return home, because the Government has limited the number of inbound flights, pushing their costs to unaffordable levels (unless you are a wealthy celebrity). This limit in turn reflects the state’s inability to organise decent quarantine processes. As of February 2021, some 90% of Australia’s cases and deaths were traced to quarantine hotels. Bringing stranded citizens home therefore portends higher case numbers – irreconcilable with a ‘zero Covid’ objective. Consequently, they remain stuck overseas and even threatened with imprisonment if they try to return, with many sinking into destitution. This is an astonishing violation of citizens’ basic rights. Perhaps more astonishing still is the fact that two-thirds of Australians do not think the Government should do more to help their stranded compatriots. As it stands, most Australians seem happy with the Government’s official position that the country will remain hermetically sealed-off from the rest of the world for another two to three years.
This toxic combination of government ineptitude and warped popular attitudes is now blocking Australia’s exit from the pandemic. The Government’s misplaced sense of pride in its ability to manage COVID-19 apparently blinded it to the necessity of securing an adequate supply of vaccines. The rollout has also been exceedingly slow and halting, reflecting wider state dysfunctionality. But public take-up has also been very limited. Australians seem to have imbibed a misplaced sense of pride about how wonderfully they have managed COVID-19, to the extent that many see no need to rush to get vaccinated. And, in an echo of European governments’ behaviour, as if to distract attention for its own procurement and delivery mistakes, Canberra has fuelled confusion and doubt about the vaccines’ safety, exacerbating vaccine hesitancy. Consequently, just 7.1% of Australians have been fully vaccinated, placing the country between Albania and Kazakhstan. This naturally prolongs the lockdown doom-loop, because the link between cases, hospitalisations and deaths has not been broken by widespread vaccination.
The Australian government’s newly announced four stage strategy to exit this doom-loop remains exceedingly vague. The first stage is actually a step backwards, with quarantine places set to half. The only positive aspect is the recognition that COVID-19 must eventually be managed in a way “consistent with public health management of other infectious diseases”, like influenza. This is an effective admission that the new coronavirus cannot be indefinitely suppressed – that is, ‘zero Covid’ is a ridiculous pipe dream. Indeed, it always has been: once a novel virus like this has achieved widespread community transmission, it inevitably becomes endemic in the human population, like influenza and the common cold. No country can avoid this fate, unless it remains permanently segregated from the rest of mankind. Australia is thus, belatedly and half-heartedly, embracing the inevitable, framing vaccination as the way to step back towards a more normal approach to the management of public health.
Vaccines = Freedom? Not so fast…
However, the British experience reveals that vaccination is also insufficient to end the doom-loop of endless restrictions on our freedom. The British Government’s decision to procure vast quantities of vaccine – 400m doses – and to insist on domestic production and watertight supply agreements is the sole bright spot of its otherwise disastrous response to the pandemic. It has put it well ahead of other European countries, arousing much bitterness and rancour among EU leaders, whose own response has been even worse. Currently, over half of the population has been fully vaccinated.
But the really crucial milestone was reached back in spring. Over-50s and those with underlying health conditions account for 98 percent of deaths and 80 to 85 percent serious illness from Covid. Consequently, once this group is vaccinated, the major risks to the population as a whole are eliminated. Notwithstanding uneven take-up among ethnic-minorities and in poorer areas, this threshold has long since been crossed.
And yet, Britain’s so-called ‘Freedom Day’ on June 21st – the point where all remaining restrictions were supposed to have been abolished – was postponed to July 19th. And rather than abolishing the restrictions, the Government has now merely devolved decision-making to businesses and other organisations, which will mostly perpetuate them in the name of “making people feel safe”. Half a million people per week are being told to self-isolate by the NHS app, causing serious harm to the NHS itself. Meanwhile, certain scientists and commentators continue to rail against the lifting of restriction, and reports suggest the Government is planning to extend emergency measures like lockdowns, social distancing and mask-wearing over the next five winters. It seems highly probable that, unless something shifts over the next couple of months, as cases inevitably rise over winter, alongside the seasonal flu epidemic, we will be plunged back into lockdown.
The nervousness around so-called ‘Freedom Day’ was not driven by any rational assessment of the data. True, July ‘cases’, measured by PCR tests, were rising on July 19th, thanks to the latest, ‘Delta’ variant. But ‘cases’ have always been an illegitimate way to measure the progress of the pandemic, because ‘case’ historically meant a clinical diagnosis accompanying actual symptoms, plus a positive test. Many ‘cases’ are entirely asymptomatic, yet there is precious little evidence that asymptomatic individuals spread the disease, despite this being a major assumption underpinning lockdown policy.
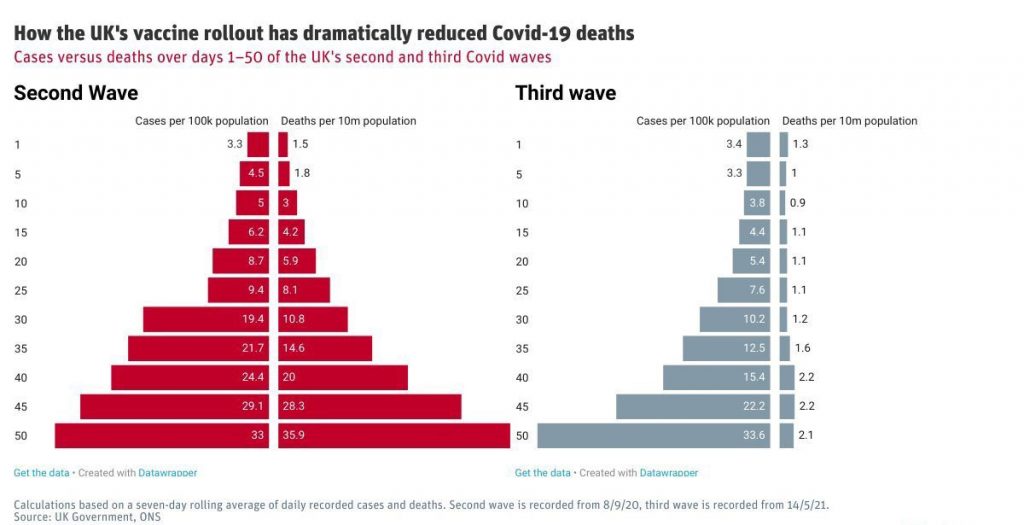
More importantly, the extent of vaccination – which, combined with acquired immunity to COVID-19 and similar diseases – has clearly broken the link between infections, on the one hand, and hospitalisations and deaths, on the other (see Figure 1). Put simply, ‘cases’ may have been rising on July 19th, but hospitalisations and deaths remained relatively flat.
In the week ending July 2nd, 109 people in England and Wales died with COVID-19 on their death certificate. We know that this measure over-records the impact of the virus, as not everyone with the disease is killed by it, but let’s accept this top-end figure for the sake of discussion. In the same period, there were 8,808 deaths from various causes; COVID-19 caused just 1.2% of these. The current level of deaths is actually well below the five-year average.
As of July 15th, 3,964 patients were in hospital ‘with’ the disease, 551 of whom were being ventilated. Again, this is not a precise measure because many people are admitted to hospital for other reasons, then test positive for COVID-19 (as many as 40 percent acquiring the disease in the hospital itself) – but, again, let’s accept this maximal figure for discussion. For these patients and their families, the illness will be serious and distressing, and they deserve our sympathy and support.
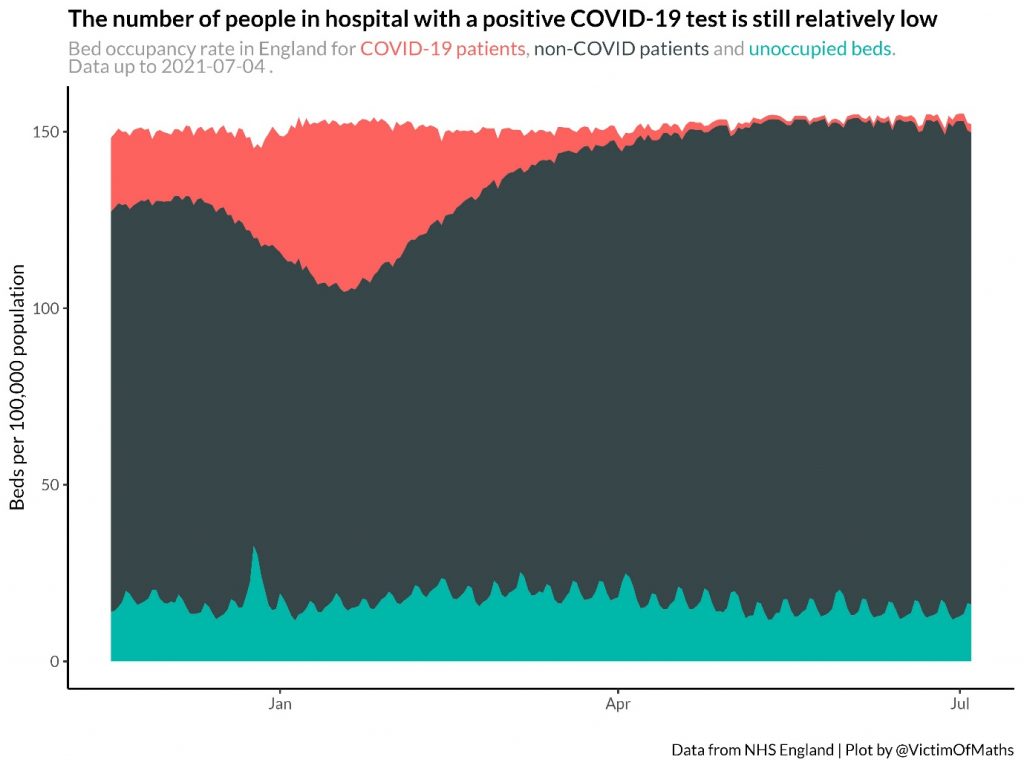
Nonetheless, they clearly do not represent an existential threat to the NHS, which has over 122,000 beds in various specialisms in England alone. Indeed, the NHS has never been very close to being overwhelmed by COVID-19 cases, even during the torrid winter of 2020-21 (see Figure 2). It strains credulity to believe that it will be overwhelmed this summer, when vaccination rates are so high, and vaccines are proven to reduce transmission, the severity of symptoms, and the risk of hospitalisation. And yet this appears to be believed by the self-same individuals who bash ‘anti-vaxxers’ as conspiracy theorists. Who are the true anti-vaxxers, if not people who implicitly deny the vaccines’ efficacy?
Moreover, if we are genuinely concerned that NHS capacity might be exceeded, rather than simply agitating for continued restrictions on the citizenry, we ought to be asking why the NHS is so fragile. Why is the NHS so incapable of protecting us, such that we (still) have to protect it? Why, 18 months into a pandemic, is hospital bed capacity actually lower than at the start? Why is the NHS’s intensive care unit capacity so low compared to other similar countries – more than four times lower than the U.S. and Germany, for example? Why are we allowing the NHS app to produce widespread absenteeism among NHS staff, further limiting capacity? Why is in-hospital transmission so unacceptably high?
These questions would at least move us in the right direction, because they would refocus attention on policy failure – on human factors, rather than fatalistically assuming that we must remain victims of natural forces beyond our control.
The Only Way Out is Through (Our Fears)
Clearly, vaccination is not the magical escape route from lockdown that many thought it might be. Restrictions – and public demand for them – can persist even when high vaccination rates have transformed the relationship between cases and deaths, and the continued disease burden, is readily manageable with existing public health resources. Why?
Answering this question involves reflecting on why they were imposed in the first place – and thus turns less on issues of vaccination rates and hospitalisation data, and more on problems of politics and social psychology.
Lockdowns and other societal restrictions were never recommended in pre-Covid pandemic planning by the World Health Organisation or national governments, because they were of unproven and dubious efficacy and came at tremendous cost. That most countries collapsed into some form of lockdown, throwing out their existing pandemic planning, thus indicates decisions taken in moments of panic, amid mounting, media-induced fear among the general public.
In most (though not all) countries, governments lacked the necessary authority to resist such pressure and hold to existing plans, which focused on delaying the spread of new diseases and mitigating their impact. Crucially, moreover, in many places, including Britain and Australia, the state was also very poorly prepared to do even this. Successive governments failed to invest in necessary capacities, outsourcing planning and preparedness to local authorities and private companies. Consequently, existing systems soon collapsed, adding to the sense of panic. As the U.K.’s Deputy Cabinet Secretary told the Prime Minister’s chief adviser on March 12th – the day that test-and-tracing was secretly abandoned because the U.K. could only handle five tests per week – “I’ve been told for years there’s a whole plan for this. There is no plan… I think we are absolutely fucked.”
Lockdown was thus the result of panic and state failure. It appealed to politicians because it gave the public what they seemed to be clamouring for, and bought time to organise a better response. The trouble is that justifying and securing compliance with such draconian measures entailed a colossal propaganda effort that has permanently skewed public perceptions of the virus, and inverted the proper relationship between state and citizen. As Laura Dodsworth chronicles in A State of Fear, the U.K. Government deliberately mobilised behavioural psychology to instil fear into the population to increase compliance with lockdown measures. The media has followed suit for its own purposes.
A conformist culture ensued in which dissenting voices – even among world-leading scientists – have been silenced, censored, or subjected to abuse. Sceptics are derided as “Covidiots”, “selfish morons” and people who want to “kill granny”. The proper relationship between citizen and state in a democracy has been turned on its head, with the Government telling the public what to do, rather than vice-versa, and demanding that people stay home to “protect the NHS”, when the NHS’s job is actually to protect us.
This combines with the ‘sunk costs fallacy’: our reluctance to admit that previous decisions were mistaken due to the costs they have already imposed, which pushes us to double-down on those decisions. The politicians in charge can never admit that lockdown policies were disproportionate because the costs they have imposed on society are colossal. But the same extends to the official opposition, who have – if anything – only demanded stricter measures. Parliament also remains fundamentally delinquent: having declared its work inessential in March 2020, it is still not functioning normally today, limiting still further the capacity for critical self-reflection.
Equally, thanks to the politicisation of science that accompanies technocracy, many scientists have become cheerleaders for lockdowns. Their reputations would be destroyed were it to be admitted that they did more harm than good. Many ordinary people have also made such significant sacrifices – some of them genuinely appalling and inhumane – that it would be traumatic to consider that they were perhaps illegitimate.
The issue of ‘sunk costs’ must be a reason why, even today, we still lack a serious official cost-benefit analysis of lockdown policy. The only analysis ever published by the U.K. Government is a flimsy document from November 2020, which declined to use the normal quantitative measures used to justify health interventions – “quality-adjusted life years” (QALY) – presumably because it would reveal that lockdowns could not be justified. Normally, when deciding whether to fund a treatment or intervention, the NHS weighs the cost against the number of QALYs it would save, with each QALY valued at £30,000. Independent analysis suggests that each QALY would have to be valued at between £96,000 and £1.97m for lockdown to make sense, depending on how effective lockdowns are in preventing deaths (itself a matter of some dispute, with many studies arguing that they are ineffective).
The stated desire of many people to continue practising restrictions even after they are lifted also reveals the way in which hyper-hygiene has become a marker of moral superiority. When mask-wearing is (falsely) advertised as a way to protect others, naturally, it becomes virtuous to wear a mask. Moreover, this virtue is openly broadcast to others at relatively low cost. When others decline to wear masks, this allows one to signal not just moral virtue but also moral superiority. As one prominent commentator puts it: “In a nutshell, post July 29th [sic] there will be people prepared to wear masks because they care about other people. And those who don’t. And that’s it, isn’t it?”
Here, pandemic politics intersect with Britain’s tedious culture wars in which left-liberals continuously seek to assert their superiority over the masses of racist, sexist, transphobic (etc.) troglodytes that supposedly constitute the bulk of the population. This, rather than any rational assessment, presumably lies behind the assertion of 1,200 scientists that unlocked Britain will become a breeding ground for lethal variants of COVID-19: they are unable to see their fellow citizens as constituting anything more than a fetid Petri dish.
The panicked retreat into lockdown and the subsequent reign of terror has destroyed our societies’ normal capacity to assess risk and make rational trade-offs, while playing into some very negative cultural tendencies. We have focused myopically on a single disease, to the exclusion of all other health problems, many of which will be exacerbated by lockdowns. We have also lost sight of a host of other social values, inflicting enormous damage on young people’s education, socialisation and wellbeing, not to mention the corrosive impact on civil liberties and democracy. Through a one-eyed focus on a single disease – one with an average infection fatality rate of 0.05% for the under-70s – we have made a small number of epidemiologists the arbiters of human flourishing, and they will not easily relinquish their newfound power and status.
Vaccination can never be a silver bullet for these problems, which can only be confronted collectively, through vigorous public debate and political activism. It will be very difficult indeed to shift mindsets and unpick the authoritarian ways of thinking and governing that have taken hold over the past 18 months. ‘Shots in arms’ is child’s play by comparison.
Dr. Lee Jones is a reader in International Politics at Queen Mary.











