Twelve key questions about COVID-19 and lockdowns answered. All answers fully referenced from peer-reviewed research and leading authorities.
How deadly is COVID-19?
Stanford Professor of Medicine and Epidemiology John P. A. Ioannidis in the European Journal of Clinical Investigation has reviewed data from studies globally and estimated that the infection fatality rate (IFR) of COVID-19 is around 0.15%. It varies considerably by region (for reasons such as demographics and prior susceptibility) and between countries within regions. In Europe and the Americas it is around 0.3%-0.4%. In Africa and Asia it is around 0.05%.
It also varies considerably between ages and depending on the presence of underlying conditions. Cambridge Professor of Statistics David Spiegelhalter has used the mortality data from the spring 2020 epidemic in England and Wales to show that the risk of dying from a COVID-19 infection roughly increases by 12-13% for each year older, doubles every 5-6 years and is around 10,000 times higher for the oldest compared to the youngest. It is also roughly proportional to the normal risk of dying in a given year (though is partly in addition to that normal risk). Men have around double the risk of death of women of the same age.
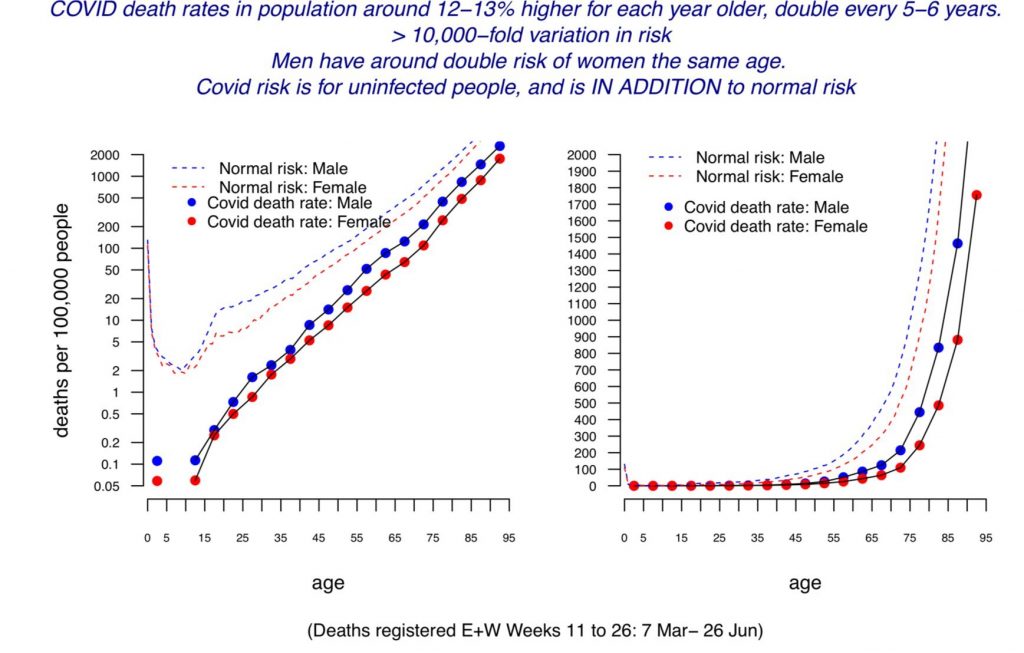
The average age of death from Covid in England and Wales in the spring epidemic was 80.4 according to the ONS, splitting 78.7 for men and 82.5 for women. The average age of death in the UK is 79.3 for men and 82.9 for women (though note these are modelled estimates of life expectancy at birth based on life tables, not the actual average age of those who die each year). Public Health England has estimated that life expectancy was reduced by 1.3 years for men and 0.9 years for women in 2020 due to the Covid and lockdown death tolls, though these figures are also modelled.
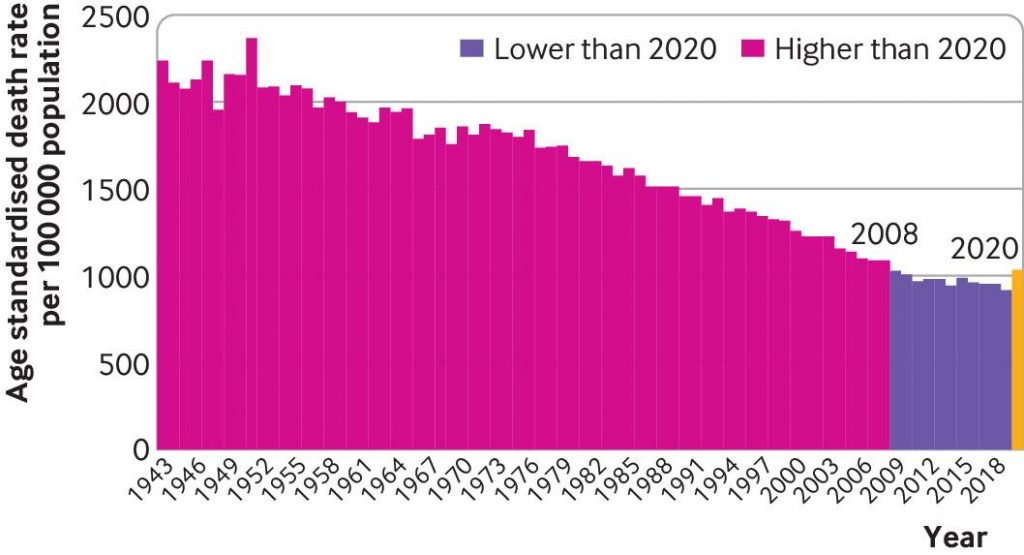
Economist John Appleby writing in the BMJ has shown that every year prior to 2009 was more deadly than 2020 in England and Wales once the size and age of the population is taken into account. The same analysis also shows that previous pandemics have not resulted in continued elevated death rates for more than a year or two despite not having vaccines for the diseases, indicating how the human immune system and the diseases adapt into a less deadly relationship.
A Swedish review of Covid deaths outside hospitals (i.e., in care homes and private homes) in one county found 85% were from a different underlying cause. In Northern Ireland, 38% of Covid deaths in spring 2020 were determined to be not primarily due to COVID-19. However, the same figure in England and Wales was 8%, suggesting significant differences in how Covid deaths are registered between jurisdictions.
How is COVID-19 spread?
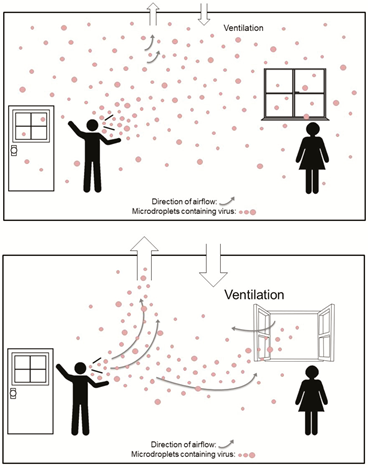
According to the most up-to-date data, COVID-19 primarily spreads via aerosols that build-up in the air of a room rather than via larger droplets or through contact with surfaces (fomites). This is why many of the measures taken to combat the spread of COVID-19, such as distancing, barriers, face masks (see below) and cleaning surfaces are ineffective.
Public Health England has used data from the Government testing programme to show that the secondary attack rate (proportion of contacts who catch the virus from an infected person) in private homes is around 10.1%. An American study in JAMA found it was 16.6%.
The low secondary attack rate in the high-exposure context of private homes is indicative of high levels of pre-existing immunity to the disease, as discussed in the BMJ by Peter Doshi. Note that immunity is not binary – a person can be resistant on one occasion and not resistant on another, for a variety of reasons. Cross-reactive T-cells that provide a measure of immunity have been found in a number of studies in 20-50% of unexposed people, or even up to 81%. Exposure without detectable infection (detectable by a PCR test) has also been found to induce a degree of T-cell immunity.
Infection with COVID-19 has been shown in a number of studies, including one on U.S Marines published in the Lancet, to confer natural immunity that gives around 80% protection from re-infection and 90% protection from symptomatic re-infection, with ten times lower viral load (corresponding to infectiousness).
What about asymptomatic and pre-symptomatic transmission?
Asymptomatic infection is typically characterised by a much lower viral load and consequently much lower infectiousness. The study in JAMA on household secondary attack rate (SAR) cited above found that asymptomatic infections had a SAR of just 0.7% versus a SAR of 18% for symptomatic infection. The proportion of infections that are asymptomatic increases among those with immunity from previous infection or vaccination, indicating that it is a characteristic of immunity.
People become infectious around two days prior to onset of symptoms as viral load peaks. This pre-symptomatic transmission is estimated to account for around 6.4% of spread, according to a study of actual transmission events from Singapore. Modelled estimates of the contribution of pre-symptomatic spread appear to go too high.
A review of studies of asymptomatic infection concluded that around 19% of infections are asymptomatic and the secondary attack rate of asymptomatic infection is 68% lower than symptomatic infection (though the authors say they cannot confidently distinguish asymptomatic from pre-symptomatic positive tests). Taken together, these percentages suggest that asymptomatic spread may account for around 6% of infections.
This means that people without symptoms, whether asymptomatic or pre-symptomatic, are not major drivers of the epidemic.
Do lockdowns work?
Restrictions on social contact, such as stay-at-home orders, business closures and gathering limits, have consistently been shown in peer-reviewed studies to have had no significant impact on outcomes such as Covid infections and deaths. Here is a sample, with a key quote from each.
- “Full lockdowns and wide-spread COVID-19 testing were not associated with reductions in the number of critical cases or overall mortality.” “A country level analysis measuring the impact of government actions, country preparedness and socioeconomic factors on COVID-19 mortality and related health outcomes” by Rabail Chaudhry, George Dranitsaris, Talha Mubashir, Justyna Bartoszko, Sheila Riazi. EClinicalMedicine (Lancet) 25 (2020) 100464, July 21st, 2020.
- “We find that shelter-in-place orders had no detectable health benefits, only modest effects on behaviour, and small but adverse effects on the economy.” “Evaluating the effects of shelter-in-place policies during the COVID-19 pandemic” by Christopher R. Berry, Anthony Fowler, Tamara Glazer, Samantha Handel-Meyer, and Alec MacMillen, Proceedings of the National Academy of Science of the USA, April 13th, 2021.
- “Stringency of the measures settled to fight pandemia, including lockdown, did not appear to be linked with death rate.” “Covid-19 Mortality: A Matter of Vulnerability Among Nations Facing Limited Margins of Adaptation” by Quentin De Larochelambert, Andy Marc, Juliana Antero, Eric Le Bourg, and Jean-François Toussaint. Frontiers in Public Health, November 19th, 2020.
- “Comparing weekly mortality in 24 European countries, the findings in this paper suggest that more severe lockdown policies have not been associated with lower mortality. In other words, the lockdowns have not worked as intended.” “Did Lockdown Work? An Economist’s Cross-Country Comparison” by Christian Bjørnskov. CESifo Economic Studies March 29th, 2021.
- “While small benefits cannot be excluded, we do not find significant benefits on case growth of more restrictive NPIs.” “Assessing Mandatory Stay‐at‐Home and Business Closure Effects on the Spread of COVID‐19” by Eran Bendavid, Christopher Oh, Jay Bhattacharya, John P.A. Ioannidis. European Journal of Clinical Investigation, January 5th, 2021.
Studies which conclude otherwise are invariably based on models rather than data.
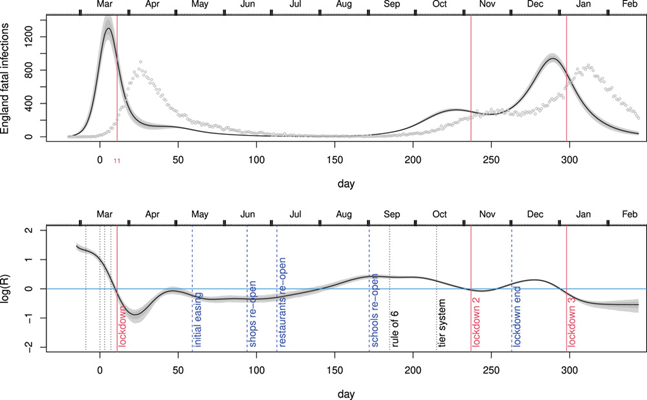
Professor Simon Woods, a mathematician, has shown that infections were in decline prior to the start of all three lockdowns in England.
You can find a useful round-up of the studies showing lockdowns don’t work at AIER.
Does social distancing work?
Many studies (including some of those above) which conclude that lockdowns don’t work nonetheless add that voluntary social distancing practices do reduce infections or deaths by suppressing spread. However, this is typically stated without supporting evidence. In fact, the evidence on this is also quite weak.
An international comparison study in Nature by R.F. Savaris and colleagues found that actually staying at home (measured by mobile phone mobility data) also made no significant difference to outcomes. “We were not able to explain the variation of deaths per million in different regions in the world by social isolation, herein analysed as differences in staying at home, compared to baseline,” they wrote. “In the restrictive and global comparisons, only 3% and 1.6% of the comparisons were significantly different, respectively.”
Another study in Nature found that those instructed to shield (self-isolate) because at high risk of serious disease in Scotland had more than eight times the infection rate and over five times the case fatality rate of the low risk who were not shielding.
Social distancing doesn’t have a significant impact on infections or deaths for a number of reasons.
Firstly, the fact that transmission is mainly via aerosols that build-up in the air of a room means that keeping a physical distance from people makes little difference to risk. A study from MIT used a model of viral dynamics to show that physical distancing makes no significant difference to transmission risk in indoor spaces.
Second, much of the spread, especially which leads to serious infection and death, is nosocomial, i.e., it occurs in care homes and hospitals. According to data from the ONS, 39% of Covid deaths in England and Wales in spring 2020 were care home residents. According to Public Health Scotland, between half and two thirds of serious Covid infections during the winter were picked up in hospital.
Third, not everyone is staying at home, even when they’re unwell. ONS figures show that nearly half of people in the U.K. travelled to work during the January lockdown. A major survey from King’s College London found that less than half of those with symptomatic Covid fully self-isolated during their infectious period.
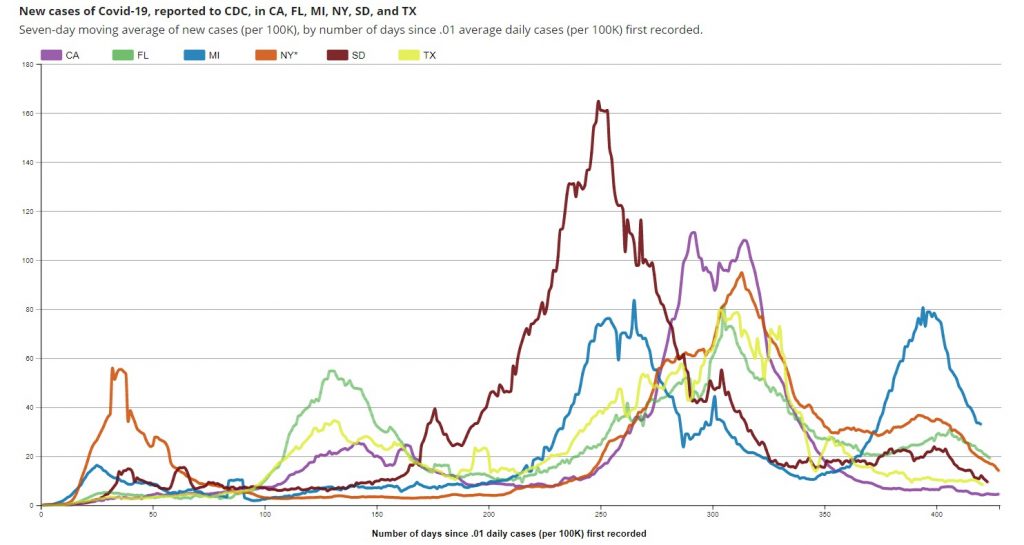
Because social distancing does not significantly suppress viral spread, there is no reason to expect a large new wave of infections when social distancing practices are eased or ended. This aligns with the experience of states in the U.S. such as Florida, Texas and South Dakota which ended restrictions or never imposed them and did not experience noticeably worse outcomes than states which maintained them.
Are lockdowns harmful?
Lockdowns are extremely harmful to human health and well-being, leading to large reductions in access to healthcare, education and sources of social support, and considerable reductions in economic activity resulting in large-scale losses of earnings and livelihoods.
A U.K. Government report estimated that the first lockdown would kill at least 63,000 people through missed medical care and worsened economic conditions. It argued this loss of life was justified because COVID-19 was predicted to kill directly up to 1.5 million people or around 2.2% of the population. However, this figure is many times higher than the death toll in any country on earth no matter how lax its response. The worst affected country as of May 8th 2021, Hungary, has lost less than 0.3% of its population with COVID-19 according to official data. Sweden, with looser restrictions, has lost less than 0.14%.
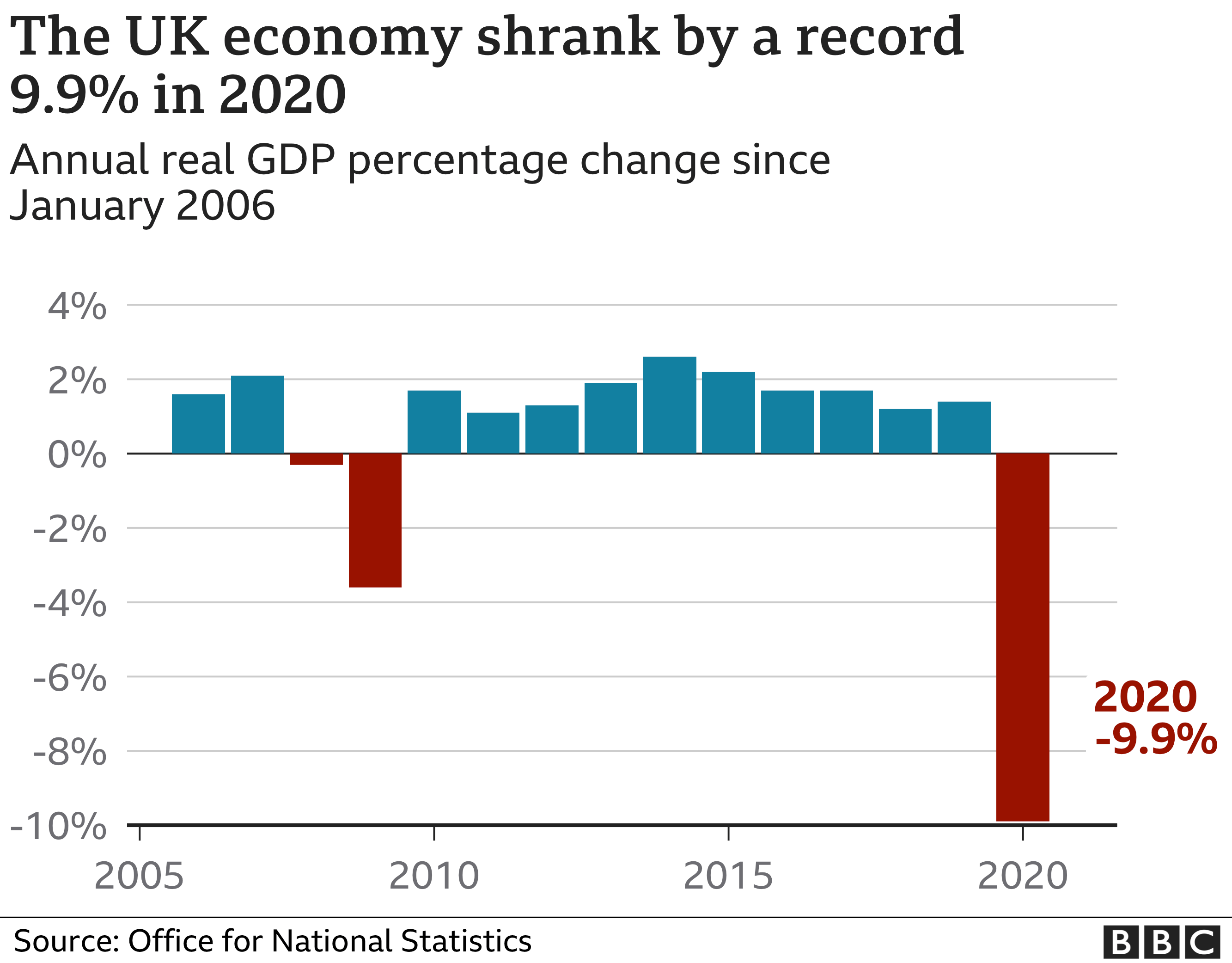
The UK economy shrank by almost 10% in 2020, the largest annual fall on record.
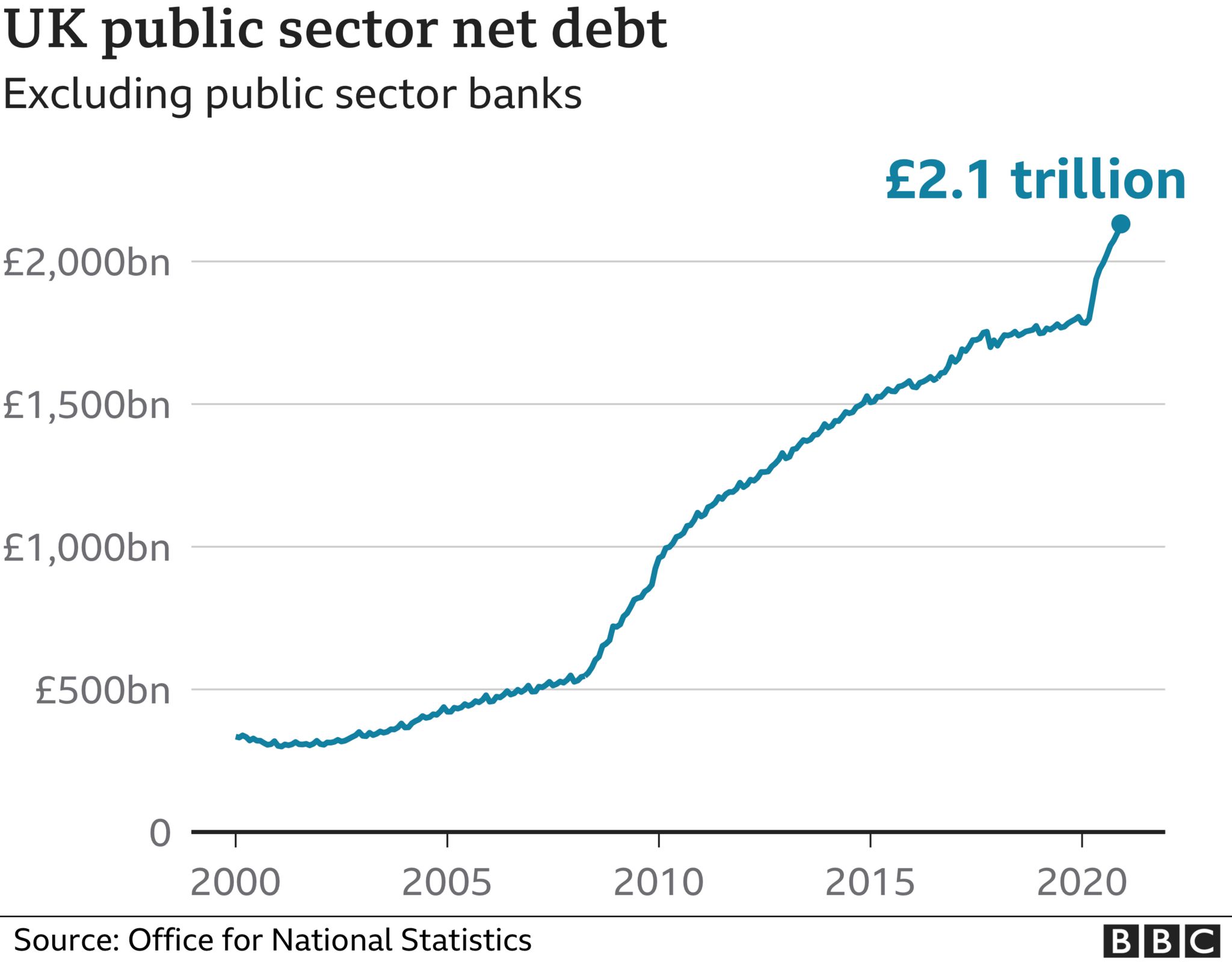
UK national debt has also jumped considerably during the pandemic to £2.1 trillion.
Lockdowns take a toll on mental health. The ONS estimates that the proportion of UK adults experiencing some form of depression is “more than double” what it was before the pandemic, increasing from 10% in 2019 to 21% in 2020.
The United Nations has estimated that disruption in healthcare services caused by government responses to COVID-19 in Afghanistan, Nepal, Bangladesh, India, Pakistan and Sri Lanka (home to some 1.8 billion people) may have led to 239,000 maternal and child deaths. Of these, an estimated 228,000 are children under five, who are at very low risk from the virus.
The United Nations has also estimated that an additional 207 million people could be pushed into extreme poverty over the next decade due to the long term impact of lockdowns.
A website has been created by the signatories of the Great Barrington Declaration to document some of the harms of lockdowns called Collateral Global.
Are the vaccines effective?
The vaccines appear to be effective at preventing serious COVID-19 infection. A study based on data from the ZOE Covid Symptom study app found that vaccination with at least one dose of a Covid vaccine reduced hospitalisation risk by 64%, a finding also reflected in the declining proportion of Covid hospital admissions among the more vaccinated age cohorts. Supporting this, the vaccines succeed in producing antibodies to SARS-CoV-2.
However, among those most vulnerable to the virus they appear to be less effective. The same ZOE study found that the elderly (over 60s) were up to three times more likely to be infected after at least one dose of a vaccine if they were frail than if they weren’t. A German study found a third of those over 80 fully vaccinated with the Pfizer jab did not generate antibodies.
A number of studies have suggested the vaccines are highly effective at preventing infection. However, many of these studies may be confounded by declining background incidence, and there is emerging evidence the vaccines may not be as effective against infection as such studies suggest.
Some coronavirus variants are showing signs of partial escape from vaccine-induced immunity. For example, the AstraZeneca vaccine was found to be only 21.9% effective against the South African variant. The need for regular boosters tailored to new variants has been suggested.
Are the vaccines safe?
A number of safety concerns have been raised about the vaccines, some of which have led to some of the vaccines being restricted or removed in some countries.
The U.S. vaccine adverse effects reporting system (VAERS) has generated reports of deaths linked with Covid vaccinations at a rate 30 times greater than with flu vaccinations (although the number of deaths associated with flu vaccines is very low). Hundreds of serious adverse reactions have been reported in the UK.
A major study in the UK reported “an abundance of patients admitted to hospital within seven days of vaccination”.
The vaccines involve using genetic instructions to induce the body to produce the virus’s spike protein. However, there are concerns that the spike protein is itself pathogenic. One study reported: ”The SARS-CoV-2 spike protein (without the rest of the viral components) triggers cell signalling events that may promote pulmonary vascular remodelling and pulmonary arterial hypertension as well as possibly other cardiovascular complications.” The spike protein by itself was shown to harm the lungs of mice.
Because the vaccines are new there is currently no data available on long-term safety.
There is also evidence that a Covid vaccination programme can cause a spike in infections. The association of vaccination programmes and Covid surges in a number of countries has been discussed in the pages of the BMJ. Dr. Clare Craig has argued against it being behaviour based (people letting their guard down) and pointed to the results from the vaccine trials which showed a reduction in white blood cells in the days following the jab that may indicate temporary immune suppression.
The risk-benefit calculation for Covid vaccination has been acknowledged by leading figures including Chief Medical Officer Chris Whitty to be different for those who are at lower risk from the disease, particularly the young. In the U.K., the AstraZeneca vaccine is no longer recommended for those under 40.
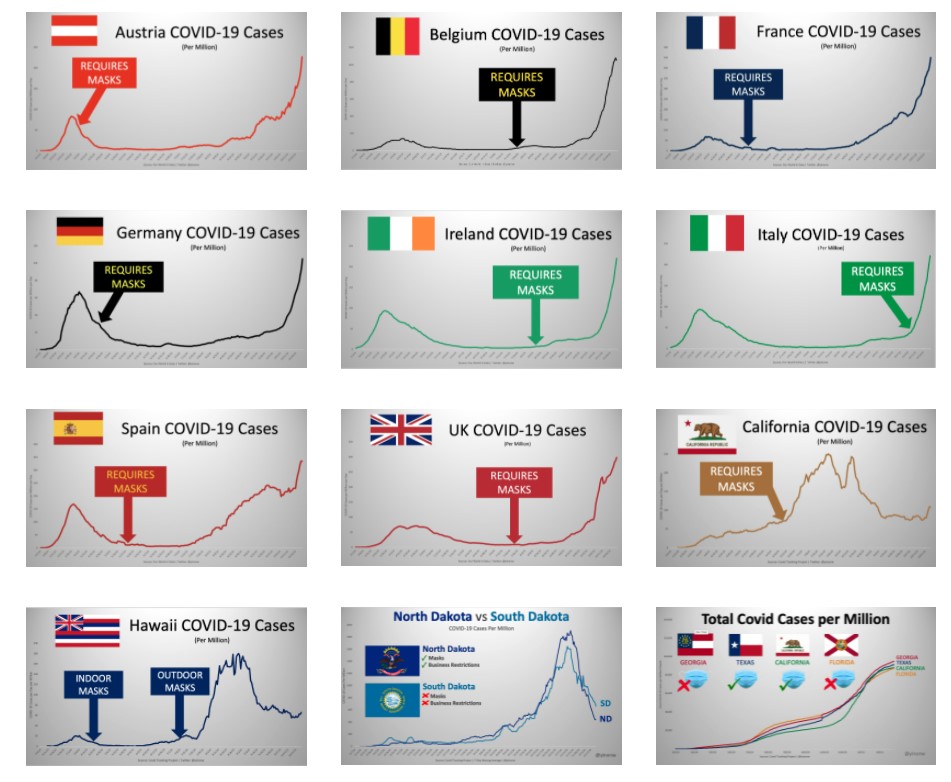
Do masks work?
Because transmission of COVID-19 is primarily via aerosols building up in the air of indoor spaces, face masks have little to no impact on risk of infection or transmission. This is because even surgical masks do not filter out enough infected aerosols to be considered respiratory protection devices. In addition, aerosols routinely escape with breath around the sides of the mask.
Accordingly, studies consistently find no significant benefit from wearing masks. The Danmask-19 randomised controlled trial (RCT) found that surgical masks provide no significant protection for the wearer from COVID-19 infection. This is in line with other RCTs for other similar viruses. One, published in autumn 2020, concluded face masks “did not seem to be effective against laboratory-confirmed viral respiratory infections nor against clinical respiratory infection”.
The Government’s scientific advisers admit masks are little use to the wearer, saying they “may provide a small amount of protection to an uninfected wearer; however, this is not their primary intended purpose”. Rather they are “predominantly a source control” (preventing transmission). The advisers cite the findings of a study by Brainard et al, which reviews a number of RCTs and concludes surgical masks provide the wearer with protection from just 6% of infections. The same study’s review of RCTs for masks as source control finds no evidence above low quality.
Yinon Weiss has plotted real-world data to show there is no sign of mask mandates altering the course or size of Covid epidemics in countries and states around the world.
Are masks safe?
A number of studies raise concerns about the safety of face masks used daily and for long periods.
A study in Water Research has called for a “full investigation” into the safety of face masks, after detecting easily detached particles of microplastics and heavy metals. “The toxicity of some of the chemicals found and the postulated risks of the rest of the present particles and molecules, raises the question of whether DPFs [disposable plastic face masks] are safe to be used on a daily basis,” it notes.
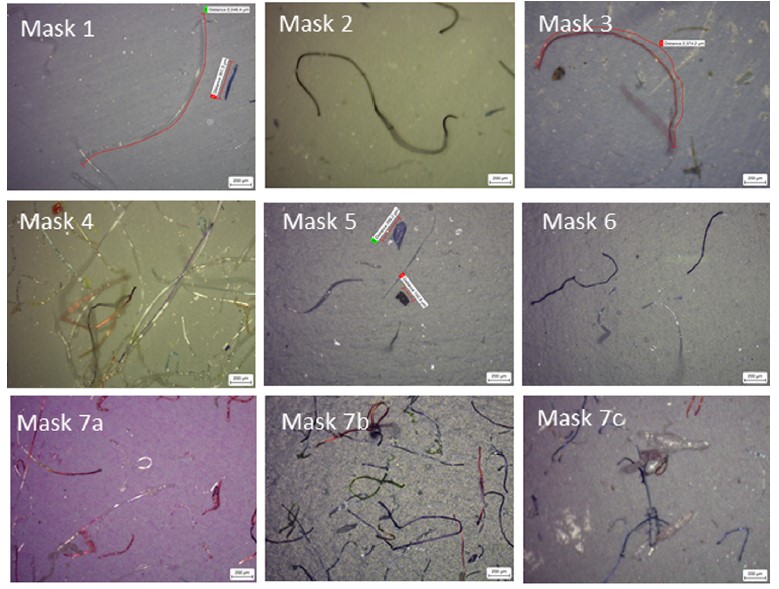
Professor Michael Braungart, head of the Hamburg Environmental Institute, has warned: “Many of them are made of polyester, so you have a microplastic problem. If I have the mask in front of my face, then of course I inhale the microplastic directly and these substances are much more toxic than if you swallow them, as they get directly into the nervous system,”
The World Health Organisation highlights a number of potential harms and risks of prolonged mask use in its guidance, including contamination, skin lesions and headaches.
A study in Clinical Research in Cardiology, “Effects of surgical and FFP2/N95 face masks on cardiopulmonary exercise capacity“, finds significant impact on lung function from wearing a mask during exercise: “The pulmonary function parameters were significantly lower with mask… the ventilation was significantly reduced with both face masks… Peak blood lactate response was reduced with mask. … Participants reported consistent and marked discomfort wearing the masks.”
Face masks have been found to be a transmission risk, with infectious virus remaining on the mask for several days.
There are also important psychological consequences from frequent and widespread mask wearing.
Are effective treatments available?
A number of treatments have been used by clinicians around the world that appear to have some beneficial impact on treating COVID-19. Among the most promising are Ivermectin, as detailed in the American Journal of Therapeutics, and Budesonide, as detailed in the Lancet. The safety profile of these established drugs is well-known and not controversial.
What should governments have done?
The UK Government has a Pandemic Preparedness Strategy, drafted in 2011 in line with international ethical norms and scientific evidence. It is primarily for an influenza pandemic, but also envisages a SARS-like pandemic and anticipates up to 315,000 deaths, most in the space of a few weeks. It primarily recommends hand hygiene and self-isolation of the infected. It does not recommend school closures, border closures, business closures, face masks in the community or bans on large gatherings. It aims to encourage “business as usual”, stating:
During a pandemic, the Government will encourage those who are well to carry on with their normal daily lives for as long and as far as that is possible, whilst taking basic precautions to protect themselves from infection and lessen the risk of spreading influenza to others. The UK Government does not plan to close borders, stop mass gatherings or impose controls on public transport during any pandemic. …
Large public gatherings or crowded events where people may be in close proximity are an important indicator of ‘normality’ and may help maintain public morale during a pandemic. The social and economic consequences of advising cancellation or postponement of large gatherings are likely to be considerable for event organisers, contributors and participants.
The Government should have followed this strategy, as it was doing until around March 16th 2020, and not been pressured into deviating from it. It should have recognised that no pandemic has caused elevated mortality for more than a year or two and maintained a sense of proportion.
That said, the strategy is notably silent on the role of hospitals and care homes in spreading the virus (nosocomial spread). It includes no special provisions for protecting care home residents, hospital patients, or any other vulnerable category. It could therefore be improved by considering how focused protection, as advocated in the Great Barrington Declaration, could reduce deaths among the vulnerable. It could also give more consideration to how infected patients could be more effectively isolated from uninfected patients in hospitals.
A further improvement would be to place more emphasis on quickly finding effective treatments besides vaccines, especially repurposed drugs which are readily available and whose safety profile is known.










