
All the broadsheets lead this morning with yesterday’s announcement from Dominic Raab that the lockdown will be extended for at least another three weeks and, in all likelihood, will last for three months from the date it was first imposed (March 23rd), which takes us into June. Raab also set out five “tests” that will have to be met before the lockdown will be lifted: that the NHS is able to provide sufficient critical care to meet demand; “a sustained and consistent fall in the daily death rates from coronavirus so we are confident that we have moved beyond the peak”; “reliable data from SAGE showing that the rate of infection is decreasing to manageable levels across the board”; that the supply of tests and PPE is sufficient to meet demand; and, finally, that any “adjustments to the current measures” won’t risk a second peak of infections that overwhelms the NHS.
The first thing to be said about these five “tests” is that the first, third, fourth and fifth all relate to the capacity of the NHS and its suppliers and could have been combined into a single “test”; only the second is non-NHS related. Would two “tests” have sounded as if the Government wasn’t taking the crisis seriously enough? They’re also frustratingly vague. How is “a sustained and consistent fall in the daily death rates” defined? We’ve seen a “sustained and consistent fall” over the last five days (April 12th – 16th) compared to the previous five days (April 7th – 11th). Does that provide us with sufficient confidence that “we have moved beyond the peak”? Presumably not, but we haven’t been told what will.
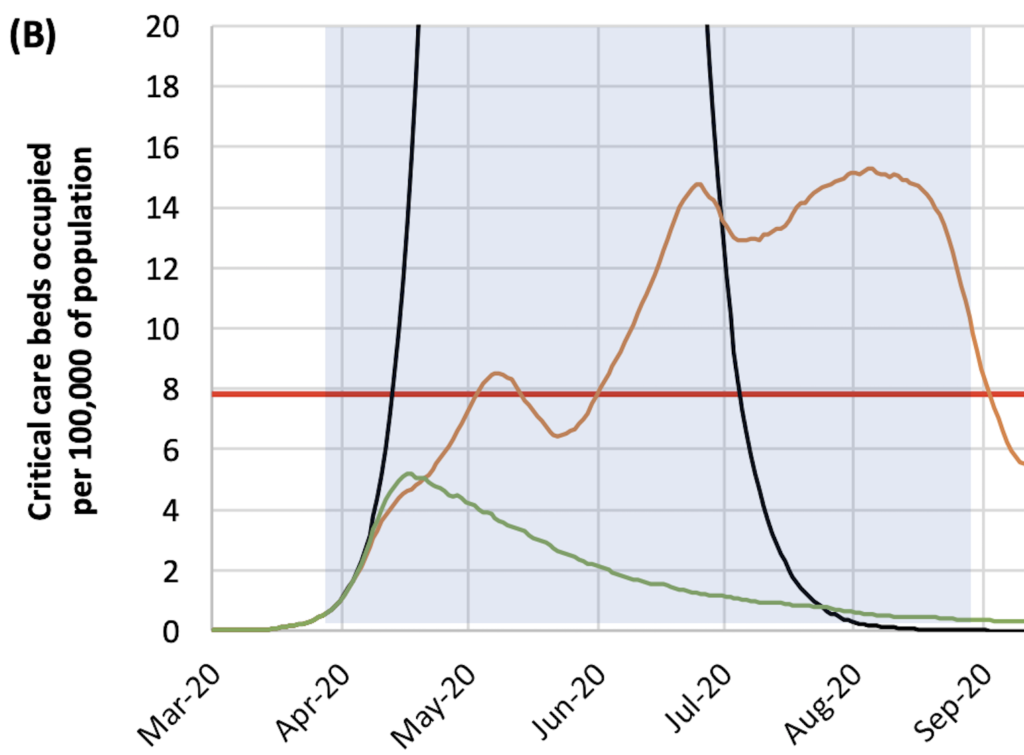
As far as assessing the capacity of the NHS is concerned, it would be helpful to know if the Government is still using the March 16th Imperial College model which assumed the NHS’s ICU capacity would remain constant throughout the lockdown period at eight beds per 100,000 of the population. This assumption is represented by the red line below – Fig 3(b) in the Imperial College paper. However, the NHS has significantly increased its critical care capacity since the lockdown began, not least by building new hospitals. Last weekend, we learnt that 37,500 general acute hospital beds were unoccupied, that only 19 patients were being treated at the new 4,000-capacity Nightingale Hospital in the ExCeL, and at least one of the new Nightingales won’t be needed. One reason for that is existing hospitals have been able to double their ICU capacity, according to the Health Service Journal. If you factor all this in, the red line in the diagram below moves above the orange line, which represents the estimated demand for critical care in a less extreme lockdown scenario, with schools and universities remaining open. Based on this, Dominic Raab could have announced yesterday that schools would reopen after the Easter holidays, i.e. on Monday, without any risk of the NHS being overwhelmed. (I’m indebted to a reader, Mike Hearn, for pointing this out.)
The other critical assumptions in the Imperial College model are that <5% of the UK population has been infected and the infection fatality rate (IFR) is 0.9%, both of which are looking increasingly shaky. New data from Robbio in Lombardy reveals that 10 times more people have been infected than was originally thought, with 22% of the population testing positive for antibodies, and a new paper by Mikko Paunio, a Finnish epidemiologist and key scientific advisor to the Finish Government, estimates that the IFR is 0.13%, making the virus roughly as dangerous as seasonal flu. Paunio submitted an earlier version of this paper to a MedRxiv prepublication site, as well as PLOS Medicine, but both rejected it. Consequently, I’ve decided to publish it on this site. If any epidemiologists want to challenge Paunio’s conclusions, feel free to do so in the comments.
One key piece of evidence cited by lockdown zealots is the latest ONS data that show a steep increase in the number of deaths in Week 14 compared to the five-year average. But according to the Times, only half the excess deaths in the week of March 28th – April 3rd were attributable to COVID-19, with the rest due to other causes. The likely reasons for this are delayed referrals for patients with serious conditions (because non-Covid patients have been de-prioritised) and a reluctance on the part of seriously ill people to go to hospital, partly because they’re worried about catching the virus and partly because they don’t want to be an additional burden on the NHS. In other words, the lockdown itself is responsible for about the same number of excess deaths as COVID-19.
There’s also mounting evidence that the lockdown is damaging people’s mental health. An article in Lancet Psychiatry says it’s likely to have a “profound and pervasive” impact on mental health, with two surveys showing many British people had experienced heightened anxiety and fear of becoming mentally unwell since the pandemic struck and are struggling to cope in isolation.
What’s particularly disappointing about the Government’s decision to extend the lockdown – and not announce any scaling back of the extreme social distancing measures – is that it’s increasingly at odds with the approach of other countries. Yesterday, Donald Trump announced guidelines for “Opening up America again”, and Italy and Spain are dialling back their own lockdowns. More generally, those countries that have avoided hard lockdowns have recorded fewer deaths per million – Japan (1.2 coronavirus deaths per million), South Korea (4.3), Singapore (1.8) and Taiwan (0.3) – than those that have effectively placed their citizens under house arrest – Spain (397.6), Italy (358.2), France (256.3) and UK (193.5). For this last bit of data, I’m indebted to Professor Ramesh Thakur, who has written an excellent sceptical essay on the “global lockdown”.
Don’t forget to email me with links to interesting articles, interviews and blog posts, and continue to post comments. If you want to receive this daily update in your email inbox every morning, fill in the form at the top of this page.












To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
Many thanks Toby. Brilliant stuff.
The US exit criteria are far clearer and measurable than the woolly UK ‘tests’. As the old management adage goes, if you can’t measure something then it is worthless (or something like that). The UK criteria are so subjective and easily fudged. It’s like something a weak manager would set for themselves so that they can wriggle out of being held responsible for not achieving the target. For a number of weeks, the UK government have been taking the easy option that they believe is least likely to get them the sack, as a poor manager would. Sad that this appears to be continuing. We desperately need some rational balanced leadership taking on board the views of all the ‘experts’ from many areas then making their own decision. This is what they’re paid to do.
Please keep up the great work Toby. It is much appreciated.
Regarding Paunio’s IFR estimate of 0.13%, this should be considered in the context of the ~11,500 COVID deaths in New York City, a population of 8m. This represents fatality of 0.144% for the entire population. Unless the entire population of NYC has been infected, and then some, Paunino’s estimate looks well off the mark. I do think incidentally, that the NYC data indicates that the infection rate is a lot higher than recognised. If for example the fatality rate of 1% is correct, admittedly a big if, then that would imply 15% infected.
According to Worldometer, the current NY death rate is 0.0873% of the population… therefore the estimation could still be good.
Also worth considering the difference between dying with and of, and of course whether excess deaths caused by the overwhelmed health systems are included in that number.
But so few die — why is higher infection rate a concern.
Hi Toby, great website and idea but you have left no way for us to communicate with you except by making a comment. I wanted to send you a link to a story from South Dakota, I thought it worth a look. But can’t do it. Aha, I’ve found the article: https://prepforthat.com/south-dakota-gov-warns-this-is-how-we-lose-our-country/
Thanks
Steve Lord
Schools reopened in France on January 12th yesterday. I have just seen the school bus go up the road and stop as usual outside the council flats. I waited and watched till it left again. Not one single person got on. Before we were let out the government could have put out messages to the effect that school kids have nothing to fear and they don’t pass it on. You would think a government would want the country to get back to normal as soon as possible. Instead of which, between every programme, right up to last week, they bigged up the R0; one person can infect three others and each of those can infect three others and so on. So now the school bus is running, but the kids are still not going to school.
By the way, the person who runs the French covidinfos.net site says that it is doing well and has 10,000 visitors a day. Out of a population of 66 million. The school buses won’t be busy any time soon.