
I feel nothing but pity for British and non-British HIV carriers alike, but I rather think medical care for the non-British is the responsibility of their own country, not ours.
That said, if we’re going to spend £15 billion a year on foreign aid, then allocating £497 million of it to testing for, preventing and developing cures for HIV/AIDS seems to me to be money well spent.
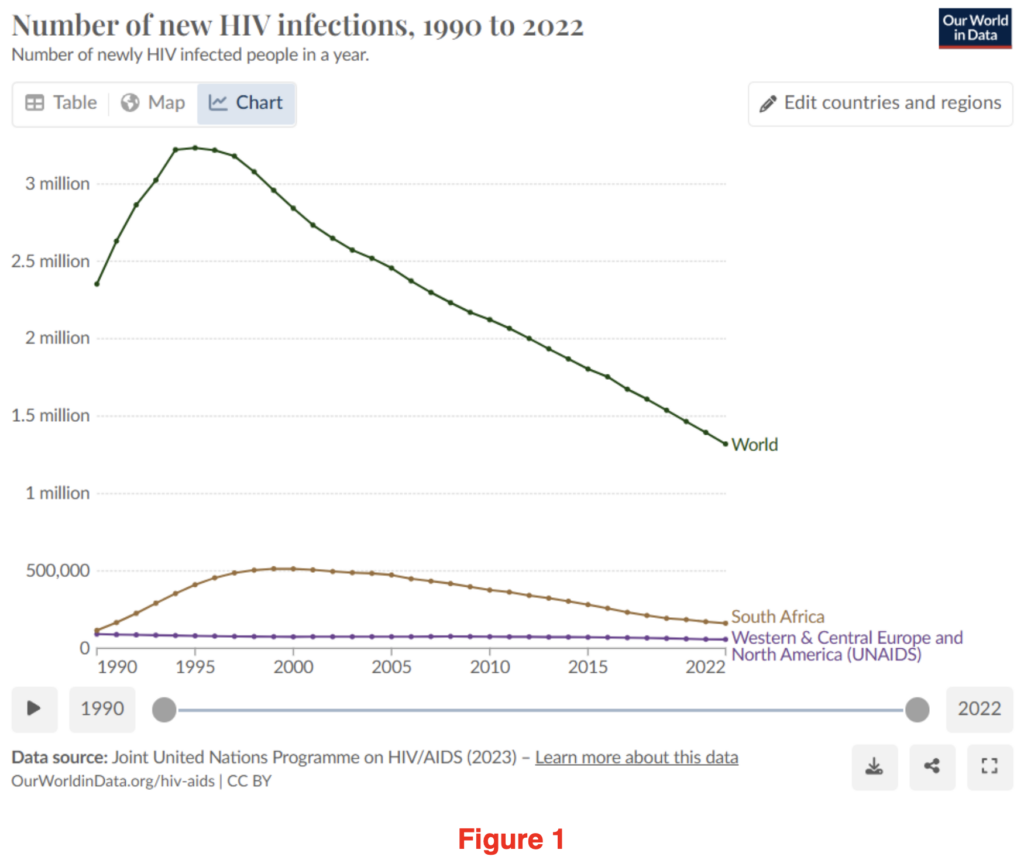
What’s more, it seems to be helping. HIV infections have been falling consistently across the world since the mid-1990s. The war on HIV/AIDS is one the world seems to slowly be winning.
It may have escaped your notice, but December 1st was World AIDS Awareness Day. Sir Keir Starmer made reference to it at PMQs on Wednesday 4th December and also issued a statement to mark the event, the main ‘takeaway’ of which was, “I am determined this generation will be the one that ends new cases of HIV within England by 2030.” Who could disagree? A laudable aim!
However, since the ‘pandemic’, I’ve become hyper-aware of nuanced language in government statements. Why equivocate by limiting it to “new cases of HIV within England”? Why not simply aim to eradicate HIV/AIDS cases from the country altogether?
I vaguely remembered reading recently that HIV cases in the U.K. were, contrary to the worldwide trend, on the increase. Could this be true and if so, was Sir Keir setting himself up to fail, or did his choice of words hide a different reality? I thought I’d just check out the data to see if Sir Keir was, as I suspected, being economical with the actualité?
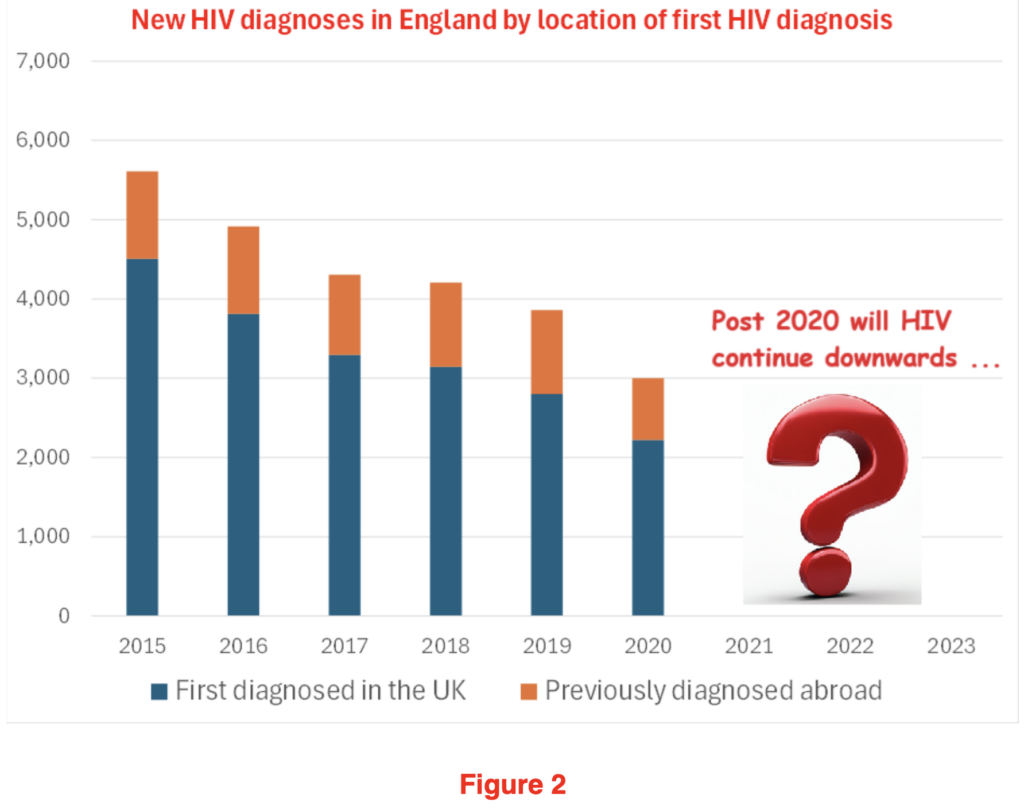
Fortunately, the UKHSA publish exhaustive data on new and existing HIV cases. If you’d looked at the figures for 2015 to 2020 (see Figure 2) you would think that this is all under control. New cases had almost halved over the prior six years. That this was, self-evidently, a good news story. Even better, that this was, that most rare of things, a good news health story. Surely Sir Keir must be well on his way to achieving his aim and eradicating new HIV cases within England by 2030?
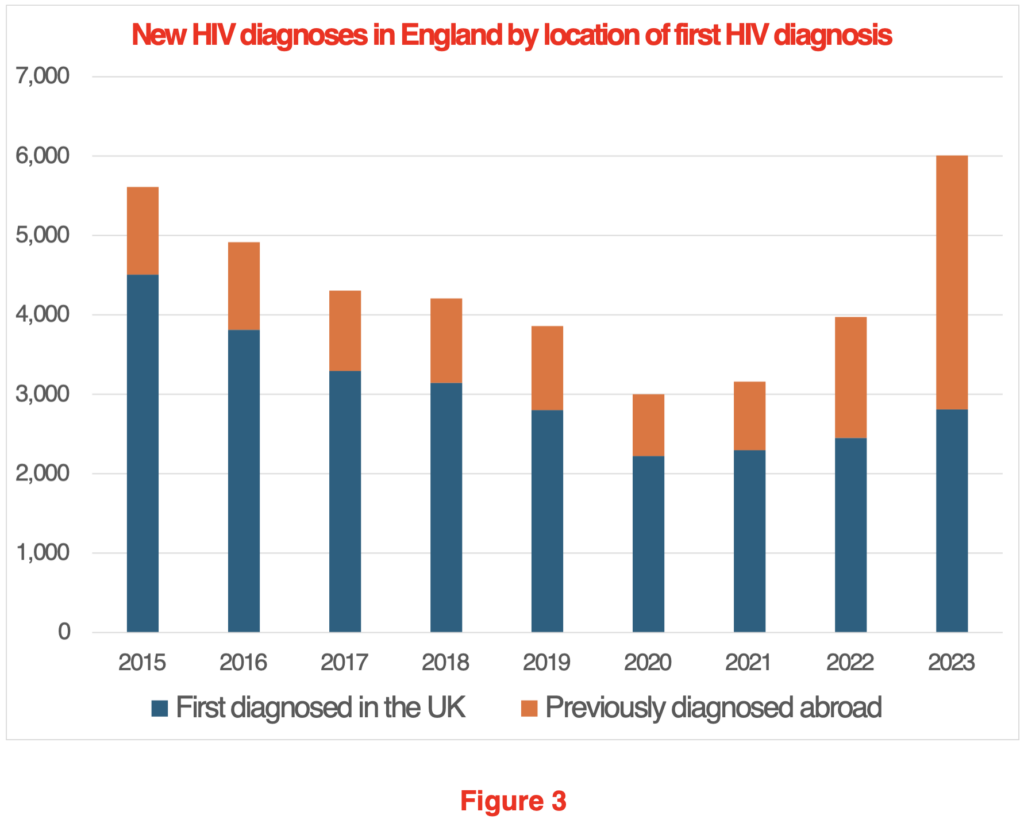
Alas, things have a habit of not working out quite how you expected. In Figure 3, I’ve added in the missing years from 2020 to 2023.
A rather different picture emerges. While diagnoses first made in the U.K. have drifted slightly upwards, new diagnoses, where the diagnosis was first made abroad, have gone up from a low of 778 in 2019 to 3,198 in 2023, an increase of over 300%.
I suppose the questions this throws up are; does it matter? Who are all these new HIV carriers? What, if anything, should be done?
Does it matter?
Each new HIV patient will land the NHS with a lifetime liability of about £520,000 at today’s prices. So, the 3,198 new patients from abroad who arrived in 2023 will land us, the taxpayer, with a future liability of about £1.6 billion. Of course, if it transpires that another 3,198 turned up in 2024, then that’s another £1.6 billion. You know the old adage, £1 billion here, a £1 billion there, pretty soon you’re talking serious money. So yes, if we want NHS funding to go to U.K. citizens, then we shouldn’t be taking on the lifetime treatment of non-U.K. HIV patients.
Recently the OBR published an interesting analysis demonstrating the relative cost to the taxpayer of varying types of migrants over their lifetime. Their data was converted into a handy chart by the Oxford University Migration Observatory that I’ve reproduced in Figure 4:
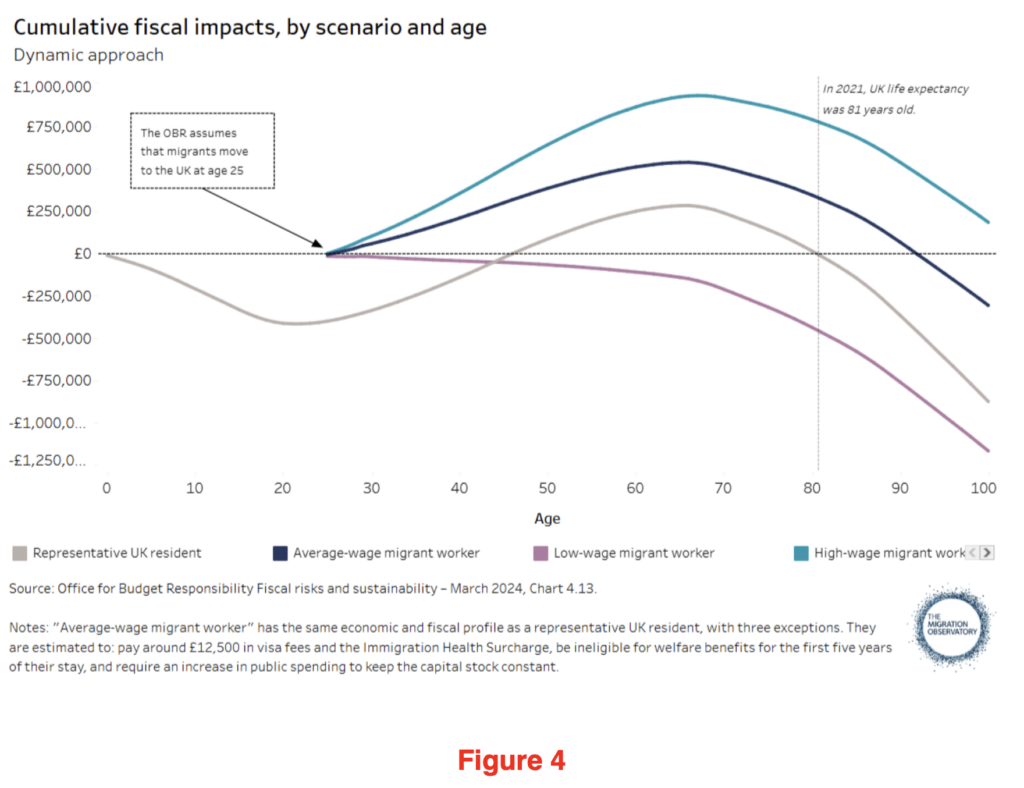
It shows that a “low-wage migrant worker”, should they live until they’re 81, would have cost the U.K. taxpayer £465,000. Call me a cynic, but my betting would be that the 3,198 HIV carriers who arrived in 2023 would tend to cluster in the ‘low-wage’ group, suggesting that each one represents something like a £1 million future liability to the taxpayer, once you add in their future HIV medical costs.
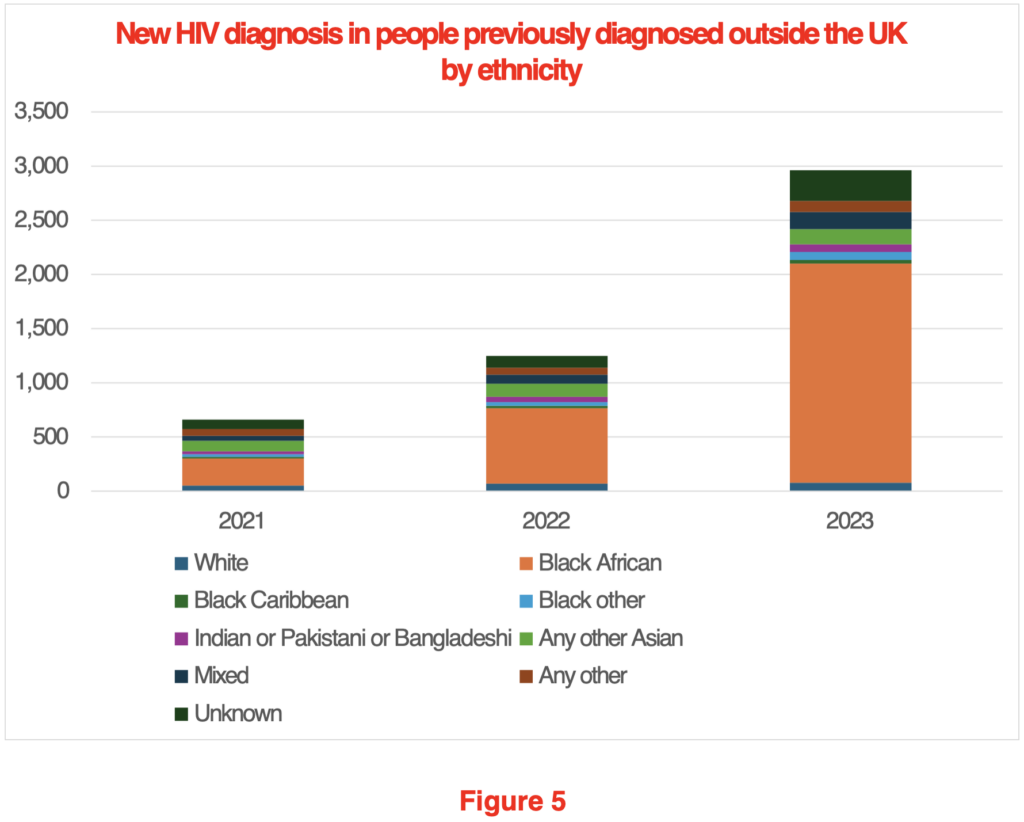
Who are these people who arrived with a pre-existing HIV diagnosis?
Figure 5 shows that by far the largest group, at 68% of the total (10% were of unknown ethnicity), were Black Africans. What’s more, almost 70% of these Black African HIV carriers are women. In all likelihood, many of them will have been granted visas as the dependents of other recent migrants.
What should be done?
This really isn’t that difficult a question to answer. We should make a negative HIV test a condition of being granted a visa. Presently this isn’t a requirement.
The Government’s press release marking AIDS awareness day makes great play of £27 million being made available annually to test people in A&E departments to find those already in the U.K. who are HIV positive. This implies that HIV prevalence is essentially a U.K. health issue. But the reality is, that if we want to reduce the incidence of HIV in the U.K., we need to acknowledge it is primarily an immigration issue. Rather than testing in A&E departments, the testing should be carried out prior to arrival in the country.
Testing in a migrant’s home country requires that we can trust the validity of the tests. It also glosses over the ethical issues raised by asylum seekers testing positive for HIV: should they be denied entry due to a positive test? There is also the risk that, if we deny treatment to recent arrivals or send them back to their home country, we may find that they go ‘underground’, with the risk of increased spread of HIV in the U.K. However, it should be possible to address all these concerns and still significantly reduce the number of new entrants arriving who carry the HIV virus.
Of course, it may be that the Government sees it as part of our ‘good world citizen’ role to take in HIV patients. If that’s the case, we should be clear about this to our taxpayers. But surely, the £500 million or so we spend annually from our Overseas Aid budget on HIV/AIDS initiatives should be the limit of our support for non-U.K. HIV patients. We shouldn’t be allowing people to come to the U.K. who inevitably create an ever greater burden on the public purse. The granting of a visa is conditional on multiple factors. Surely, it’s not unreasonable that a negative HIV test be added to the list?
It is this kind of disingenuousness from the Government that truly rankles. There’s an obvious problem, a relatively straightforward solution, but out of a misplaced sense of charity, or perhaps an overdeveloped desire to be kind, we find that our Government is misleading the public by focusing on a hunt for HIV carriers by the NHS, when we know the real problem should be addressed by our Border Force.











To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
“Governments don’t stay in power if they make people cold and poor”. They do if there is no coherent opposition to vote for.
And even if they don’t stay in power and get replaced, the next lot just carry on in the same way, so it makes no difference.
And they are rewarded with gongs for failure.
Which confirms what I keep repeating on here – our governments are NOT running the country.
Pitchforks.
Petrol bombs while we still have access to it.
All the petrol pumps have been damaged by climate zealots.
Pointing out the costs and suffering won’t put an end to insane climate policies.
The policies stem from the idea that burning fossil fuels leads to climate catastrophe and destruction.
In most peoples’ minds, a bit of suffering is better than catastrophe and destruction.
Years and years of brainwashing need to be undone.
But that isn’t going to happen without telling everyone that the whole CO2 climate catastrophe story is a giant hoax.
Too many people who try to argue against climate policy on the basis of the unacceptable costs don’t dare to challenge the broader narrative and that’s a big problem.
I think this is true for the Guardian readers I know, but I also talk to quite a few people much more grounded in reality and I am sure they would be more than happy to forget about the climate crisis if their bills went down.
People are saying that “the whole CO2 climate catastrophe story is a giant hoax” but they do not try to prove it. Probably they do not know enough to be able to.
The UN and WEF will be delighted that their planned destruction of the UK …. at the hands of the British Establishment and puppeticians is going so well.
Only a small percentage of the Earth’s surface has direct temperature reading instruments of varying accuracy and from which these averages of averages are calculated.
The result is numbers, not data.
Net-zero common sense for decades. And all because the earth has supposedly warmed 0.8 deg C since 1860 when records began at the low point after a little ice age.
To physicists, that’s an increase of 0.3% from 288 to 288.8 degrees Kelvin. Meanwhile the difference in average temperature between London and Manchester is 1.2 deg C. Go figure.
A simpleton’s yarn debunked over a decade ago by a Nobel Physics Laureate…
https://mediatheque.lindau-nobel.org/recordings/31259/the-strange-case-of-global-warming-2012
“…In this talk I will explain why I became concerned about the climate, and terrified by the one-sided propaganda in the media, In particular I am worried about all the money wasted on alternate energies, when so many children in the world go hungry to bed.”
Twelve years on, the Climate Theatre of the Absurd just runs and runs.
Thanks for the link.
Climate activists are average people
No, I think most of us would consider them below average retards if there answer to a lack of wind generation is just to build more of it. 1 + 1 still only equals 1 when it is the percentage of output from your windmills.
Energy, supply and demand.
The article covers comprehensively the supply end, or lack of it, but leaves out the zooming demand. According to the (fake) statistics, the population of Greater London in 2024 was 9,748,000, 1% more than 2023. Nevertheless, going by measurements of water consumption and sewage production, the real figure is close to 12m. And this is the curious thing. The NetZeroist fanatics also support enthusiastically open borders, ignoring the fact that increasing population levels lead to huge greenhouse gas emissions.
Friends of the Earth’s Tony Bosworth said, “We have an abundance of natural resources like wind and solar,” he says. “They’ll go on forever, and we won’t be reliant on expensive gas and oil.”
Bosworth ought to be sent, along with the Just Stop Oil filth who have just desecrated the grave of Charles Darwin, to Texas, to be instructed by the Texans about what happened to their wind & solar during the terrible “Polar Vortex” Blizzards in 2021. The wind turbines froze solid, the solar panels were covered with snow, and the people froze to death.
“The Texas Winter Storm And Power Outages Killed Hundreds More People Than The State Says”
“A BuzzFeed News analysis shows the catastrophic failure of Texas’s power grid in February killed hundreds of medically vulnerable people.”
“The true number of people killed by the disastrous winter storm and power outages that devastated Texas in February is likely four or five times what the state has acknowledged so far. A BuzzFeed News data analysis reveals the hidden scale of a catastrophe that trapped millions of people in freezing darkness, cut off access to running water, and overwhelmed emergency services for days.”
“The state’s tally currently stands at 151 deaths. But by looking at how many more people died during and immediately after the storm than would have been expected — an established method that has been used to count the full toll of other disasters — we estimate that 700 people were killed by the storm during the week with the worst power outages.”
“This astonishing toll exposes the full consequence of officials’ neglect in preventing the power grid’s collapse despite repeated warnings of its vulnerability to cold weather, as well as the state’s failure to reckon with the magnitude of the crisis that followed.”
Texas’s Winter Storm Killed Hundreds More Than Reported
Until the mainstream media stop repeating the net zero lies, it will remain difficult to get the honest message such as this article, through.