
The Australian Government has just published its inquiry into the Covid pandemic.
Much smaller and less legalistic than Lady Hallett’s leviathan, it primarily entailed commissioning researchers to elicit people’s lived experience of Australia’s COVID-19 response. Submissions were sought, with 2,201 received. Stakeholder meetings and focus groups were held.
This approach has an inherent hazard. It attracts and over-represents the politically engaged and the representatives of organised interest groups. It is less likely to capture the views of those – such as small traders and truck drivers – who just seek to live their lives with the least interference from government. Yet these often were the people most adversely affected by lockdowns.
Despite this limitation, the report does recognise vital points. Most notable is the acknowledgement that Australia’s Covid response eroded trust in government and public health. This, it is noted, has led to reduced uptake of vital childhood vaccines and to a large body of people distrustful of most or all government advice and initiatives. The same conclusion was reached a year earlier by academics at the University of Adelaide.
Further, and crucially, the report (p242) admits that the severe impacts of extended and universal lockdowns were “not appropriately considered”:
Isolation and quarantine arrangements, social isolation requirements, lockdowns, border closures and other public health measures affected the mental health and wellbeing of all Australians, but they had disproportionate effect [their bold] on some priority populations and on the viability of businesses. For many, such as children and people with existing mental health issues, it is very likely these impacts will be felt for some time. It is clear these impacts were not appropriately considered given these measures continued to be applied once the risk-benefit balance had shifted and proportionality was harder to argue. This must not be repeated in a future health emergency.
Quite.
Despite this scathing criticism, the authors believe that Australia’s approach – to close borders, lock down centres of viral circulation, vaccinate widely, then re-open – was broadly successful. They assert that it led to far fewer excess deaths than Canada, which they consider to be an otherwise comparable country (p276).
There are at least three objections to this self-congratulatory view:
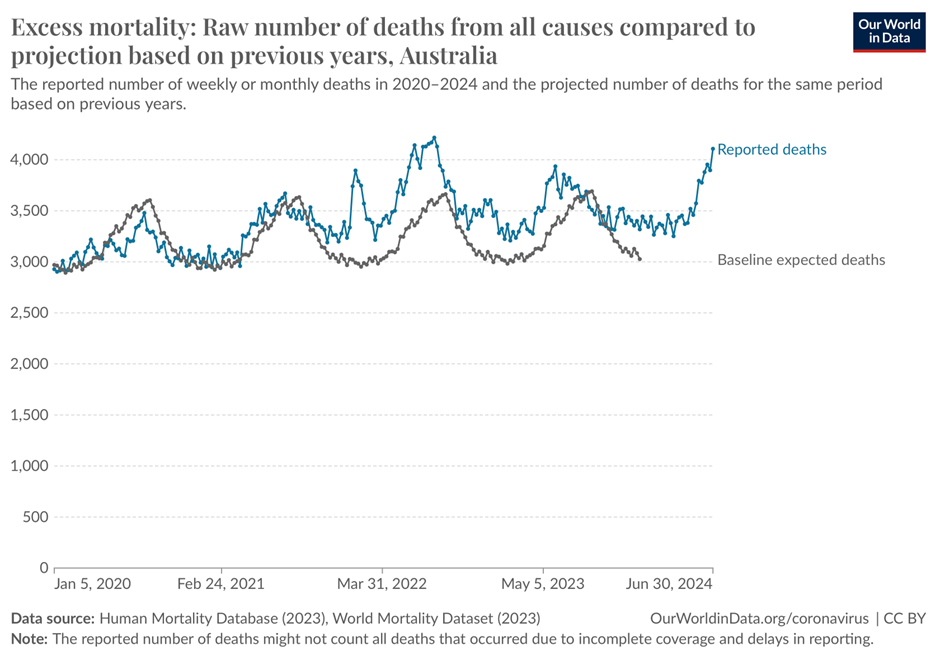
First: Australia, unlike Canada, is geographically isolated and the pandemic struck at the end of the southern summer, when people – with high vitamin D levels – are less vulnerable to respiratory viruses. To this extent Australia was simply lucky: the virus failed to gain early traction. Secondly, by the time Australia did re-open, SARS-CoV-2 had evolved to its milder Omicron forms. Again, Australia was lucky to avoid the first hit, and there was no guarantee of the virus’s direction or speed of evolution. Thirdly, the claim of fewer excess deaths is disingenuously based on the early pandemic period (2020-21) and fails to consider more recent years, when Australia has recorded substantial excess deaths. The Spectator’s analysis of all cause excess deaths from the start of the pandemic to January 2023 shows these higher in Australia that in Sweden, which had far fewer restrictions. What exactly is causing these later deaths, which seem to be increasing (figure)? Is it the virus, the vaccines, or the disruption of other healthcare when Australia was fixated upon Covid? The report is silent. It doesn’t acknowledge the phenomenon, and the dead have no voice.
Apropos Covid vaccines the Report is uncritically positive. In almost 900 pages there is not one mention of vaccine-associated myocarditis, other cardiac issues or blood clots. The Djokovic farrago passes without a note. Gosh! The inquiry’s Terms of Reference (Appendix B of the report) were wide, and vaccine harms were not excluded a priori. It is beyond credulity that the researchers failed to be contacted by anyone harmed by these products. Why are their voices denied, whereas Australia’s co-development, with Moderna, of new mRNA plants is highlighted (p 256)?
Surely it is more pertinent to discuss these aspects than to begin your report with a long, rambling piece of official wokery, which commences:
We acknowledge the Traditional Owners and Custodians of Country throughout Australia on whose lands we all work, play and live. We acknowledge their continuous connection to lands, waters, skies, culture and community….
and ends with a warning that:
This report contains material that may be distressing for some readers. If you need to talk to someone, support is available.
Two counselling helpline numbers are then provided for those affected.
You may, like me, believe that primary Covid vaccination did some initial good in high-risk populations, or you may believe that it did no good at all. What is beyond dispute is that the vaccines failed to stop viral transmission and circulation, as evidenced by the fact that the major Omicron surges came after the great majority of Australians were vaccinated.
Accordingly, there was no justification for Australia’s (and the U.K.’s) policy of giving novel mRNA and viral-vector products – with unknown immediate and long-term side-effects – to all age groups, including those at no significant risk from Covid. Nor of continuing universal vaccination after the failure to stop viral circulation was obvious. There was no justification whatsoever for the vaccine passport systems adopted, in various forms, by individual Australian states.
As he wrote in these pages, Professor Angus Dalgleish of St. George’s Hospital in London recently toured Australia, finding considerable medical disquiet about mRNA vaccines. He noted that around 1,000 medical staff in New South Wales alone had been sacked for refusing to comply with vaccine mandates. The voices of these dismissed healthcare workers are absent from the present report. Why? Perhaps they should ring the helpline. I hope they do so.
The report aims to inform future respiratory pandemic planning and has numerous recommendations to that effect. Many involve the formation of more committees and expert groups along with more central planning and the establishment of an Australian National CDC. The underlying aim seems to be to standardise responses across Australian states, not to ascertain the most appropriate response.
The recommendations pay lip service to civil liberties. Disturbingly, though, they fail to say that lockdowns, mask mandates and vaccine mandates must never be repeated in a ‘free’ country; the report suggests only (above) that they went on for too long. There is no clear, unequivocal condemnation of Dan Andrews’s nine months of lockdown in Melbourne, nor of its often brutal enforcement which, even in its early days (September 2020) was condemned by Human Rights Watch. Andrews, it should be remembered has recently received the Order of Australia from King Charles for his totalitarian efforts, and is promised a statue.
There are recommendations on countering misinformation but no admission of how much misinformation came from Governmental sources, for example on the efficacy of masks and vaccines and the evidence base for lockdowns and social distancing. It is this official misinformation that eroded trust in public health authorities. Until this is admitted and contrition shown, there is no remedy.
Overall, this report deserves five out of 10. Its curious omissions of views and experiences that must have been elicited by its processes need to be queried by the Australian media.
Dr. David Livermore is a retired Professor of Medical Microbiology at the University of East Anglia.










To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
I wrote a story today about Pfizer becoming a “corporate sponsor” of the Southeastern Conference (14 well-known colleges). In the story, I mention how ridiculous it is this sports league continues to push vaccines for student-athletes. I linked to two myocarditis studies (one showing 1-in-1000 risk, the other as low as 1 in 3000). I guess I need to go back into the story and add a link to this story/study.
I don’t think the 14 colleges of the SEC have thought enough about what this partnership could mean to them in the future. The potential liability is vast and they are not doing anything to improve their credibility with prospective future students.
https://billricejr.substack.com/p/the-southeastern-conference-is-now
So, is the mRNA technique flawed across the board, for any “vaccine” drug, or just the Covid-19 one? Does anyone actually understand the biology of it (yet)? It wouldn’t be the first time that the company involved made serious mistakes.
What are the other mRNA drugs?
Genuine question.
You can find drug research reports on TrialSite News, SciTechDaily, Cnet Science, and sometimes even Interesting Engineering, to name but four…
Thank you. One has become far more curious of late…
They had ones to treat things like cancer a while back. But there were apparently a lot of problems with it.
Far more likely to cause cancer it seems….
Funny how that works. Whether it’s cancer or covid, mRNA gene therapy really seems to be gasoline on the fire!
Robert Malone has gone into detail about this. He asserts that the mRNA technology is sound, but the problem less with the genetically engineered spike protein and the delivery mechanism (e.g. lipid nanoparticles for Pfizer).
Personally, I have a fundamental problem with the idea of genetic treatment. Prefer nature to take its course and what will be will be.
So other than the delivery mechanism and the stuff inside the delivery mechanism, it’s sound?
The delivery mechanism and the spike protein inside it is pretty much the whole thing, isn’t it?
What else is there left?
Th delivery mechanism into the cell, not the delivery mechanism from the cell into the body i.e. the translation of the mRNA. Listen to Robert Malone.
Hey, I’m not promoting this sh*t, I’m just repeating what I’ve read/heard.
“What else is there left?”
The 5G chemicals?
Aside from ‘unknown’ substances related to the adjuvants, the information for which is currently withheld for commercial reasons, it contains yummy things like:
Polyethylene glycol: https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8251011/
Incomplete RNA which is still biologically active – and with unknown effects: https://rwmalonemd.substack.com/p/mrna-vaccines-the-cia-and-national?utm_source=substack&utm_medium=email#play
Mould: https://khn.org/news/article/pfizer-new-vaccine-plant-persistent-mold-issues-history-of-recalls/
Metal fragments: https://www.riotimesonline.com/brazil-news/modern-day-censorship/international-research-groups-find-sharp-metal-objects-in-covid-vaccines-very-frightening/
Toxic metals: https://rumble.com/v1npo1k-dr.-mark-trozzi-toxic-metals-in-covid-shots.html
Other particulate contaminants: https://www.trialsitenews.com/a/failure-to-scale-covid-19-injection-vials-must-be-independently-tested-for-conformity-to-label.-9a77eba4
Others report such wonderful things as E coli, glass fragments, fibres, other diverse fragments – and a fly leg. Dr Hughes summarises some of the data here: https://ijvtpr.com/index.php/IJVTPR/article/view/52/96
To quote Alexandra Latypova – it really is a toxic garbage soup. https://rumble.com/v1p69bf-c-19-injections-regulatory-and-manufacturing-fraud-tessa-lena-tallks-to-ale.html
Thank you for submitting all these links.
Do you remember the scene from Disney’s Fantasia where the apprentice sourcerer is mixing up a spell? The list above shows that it is still about witch craft but using a lab rather than a cave, a white coat rather than a black cloak and pointy hat…
Good comparison: most people will remember The Sorcerer’s Apprentice scene in Fantasia.
Nature, by way of our immune system, is definitely not keen on any foreign body hijacking our body cells and rearranging their chemistry and function which is what virus and thecmRNA junk do. At the first sign, it sends T cells and cytotoxic agents to kill such cells. (And if those cells are in muscles, like the heart…)
That alone should tell us not to do it deliberately.
As I understand matters, and I do so in simple terms only, mRNA gene therapy was initially and still is used as a delivery system for cancer treatment by way of immunotherapy. Basically it seeks to turn on, or off, and thereby amplify, the activities of targeted cancer seeking cells, to enable them to destroy cells which have become cancerous. Look at CTLA-4, Jim Allison and Coley….Books, not google!
Used in this manner mRNA has great potential, but the downside is that it has to turn off elements of the immune system in order to work.
It didn’t take long for bigphama’s vaccinators/genetic engineers to realise mRNA would be the perfect delivery system for a new generation of “vaccines”.
However, the problem is they know next to nothing about how the immune system actually works (mind you, no one does) and, disastrously for the jabbed even less about the long term effects.
This paper gives a clue though:-
https://www.sciencedirect.com/science/article/pii/S027869152200206X
The paper also explains the inevitable blood clot risks.
Thanks for your response (and those from the others as well). The linked article is interesting, and I’m glad I didn’t accept the offer in March 2021. Then I said that I might change my mind when it becomes as established product. Not much chance of changing my mind now, given the emerging evidence.
Dr Palmer and Dr Bhakdi think it is. A quote from the article linked above: –
‘We note that the damage mechanism is which emerges from the autopsy studies is not limited to COVID-19 vaccines only but is completely general—it must be expected to occur similarly with mRNA vaccines against any and all infectious pathogens. This technology has failed and must be abandoned.’
Dr Bhakdi said at a recent MD4CE meeting that the human immune system is already perfect & adding anything to it will displace the balance. Good health, good diet, clean water, sunshine, fresh air & exercise are the best things to promote a healthy immune system.
And now they are trying to make mRNA flu jabs and RSV jabs and God only knows what else?
If it is getting into the bloodstream and producing an immune response there, that would suggest it’s a flaw in the design, clearly other vaccinations into the arm are not triggering a response like this.
Or a flaw in the administration of the stabs – the individuals who have been fast tracked into the role of “stabber” have not been aspirating the needle to check for blood to ensure the tip has not entered a vessel.
Probably both. The spike protein itself is toxic, and the mRNA technique goes everywhere in the body and makes it produce whatever protein it is designed to produce, ad infinitum.
Professor Sukharit Bhakdi posted on his Telegram group that it is now possible to distinguish the spike protein generated via the jab and the spike protein from the virus. He calls it a game changer.
Why is it a game changer?
Pathology.
The dead can’t lie… Hence the push & rush to destroy the evidence via cremation.
https://www.mdpi.com/2076-393X/10/10/1651
The autopsy in Dresden of the 76yr old which Will described seems to be the first instance where this method was applied and this result obtained.
Hence a game-changer to Bhakdi.
Not sure whether he doesn’t know about the one of the 55yr old, or whether that was later, then used the same method etc..
As I understand it SARS Cov-2 is a respiratory tract infection therefore the only exposure is ‘air side’ so it’s not clear to me how it would get into the blood stream. The disease attacks the lungs not the circulatory system.
The injection on the other had goes into the shoulder, it was supposed to remain local but we now know for a fact that it does not, so it’s reasonable to assume it is reaching the blood supply (unless there is some plausible other route around the body that bypasses the bloodstream).
So given the above two statements, it’s not clear how a natural infection in the respiratory tract would cause an immune response in the circulatory system (it’s this immune response which causes the clots I believe), however it is very clear how a jab would cause this.
It seems too obvious to be true in all honesty, would anyone like to comment on my reasoning?
You are right. It is idiotic to inject someone in the deltoid for a virus which attacks your respiratory system. Blood poisoning is the only result. Akin to cutting off your hand to save your foot from gangrene.
All of these quacksines contain poisons, that most people can’t pronounce or spell. They don’t do anything against a virus, hence the quacksinated making up the 90% death rate ‘from’ rona. Follow the money is what they mean by follow the science. The speed of science means the velocity of money which can be made.
Indeed, there is no plausible mechanism for how an injection in the deltoid can induce mucosal immunity in the respiratory tract. That is why a nasal vaccine would theoretically make more sense than an injectable one, but so far no successful one has emerged yet.
“The speed of science means the velocity of money which can be made.”
I do hope John Campbell calls in here because he really did not understand ‘the speed of science’ and I am sure your explanation will help him and many others. It has certainly enlightened me.
Many thanks.
Look at any development project. The balance between development itself and testing, fixing, certification, obtaining approvals etc is probably in the ratio of 20%:80%. The “speed of science” was only possible because they didn’t follow all the testing and certification stuff.
The virus can sometimes enter the circulatory system VIA the lungs, of course, but usually it does not do so in quantities anywhere near large enough to even approach the level of spike protein from the jabs.
Wow, just lovely. But it couldn’t be the “safe and effective” jabs, no. It MUST be the virus, climate change, working too hard (per Billy Joel), or maybe even karma. But not the jabs!
There’s even some blaming artificial sweeteners!
There are swathes of people I believe who should definitely take the booster without delay; yup!
Does that make me a good person or a bad one?
Blessed are the unvaccinated, for they shall inherit the earth. Or at least the west.
Peace of mind – not having to worry about every little twinge: blessedness indeed.
I’m feeling pretty blessed at the moment
Does anyone know why MPs continue to,think the covid vaccines are safe and effective when the data says otherwise. I continue to get responses from our Mp Simon Jupp to say the vaccines are safe and effective. Isn’t it the responsibility of the MPs to be current on their information about covid vaccines as they are being doled out to every Uk citizen despite not having an efficacy or safety data and certainly no long term data.
I have to admit, if I were an MP I sure would like to be on the right side of this debate when certain people are dragged into court and found guilty of criminal negligence, wouldn’t you?
Just lovely. Today I found out that one of my FB friends has congestive heart failure and was told she could die suddenly. She just turned 38. Kinda young to have something like that. Sure enough, she was jabbed about a year ago, then got a really bad case of Omicron shortly after that put her in the hospital. And now this. So much for “safe and effective”, right?
Why hasn’t anyone addressed the fact that the very nature of mRNA vaccines means that they will cause automatic damage to the body?
Consider this, the mRNA vaccines function by causing healthy cells to present pathogenic spike proteins on their surface so that the immune system will respond. What is the immune response? The destruction of that cell!
Therefore, ANY cell that takes in that mRNA material and starts to make spike proteins will be targeted for destruction by the immune system! Whether it is heart calls, blood vessel cells, organ cells, or nerve cells, if they present the spike protein, they will be destroyed!
So at BEST these shots make your immune system target arm muscle cells, and at worst your own immune system will be targetting what would normally be healthy cells all through out your body!