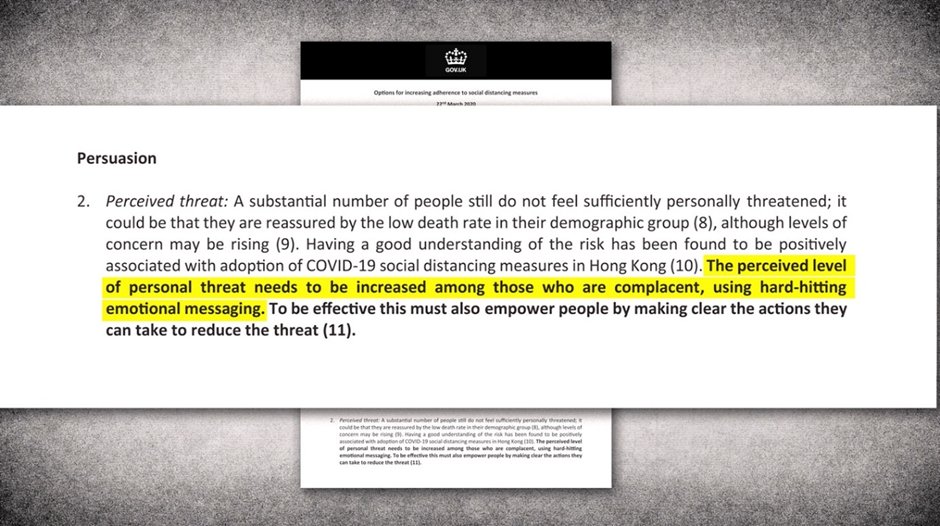
As Laura Dodsworth writes in a recent article, the claim by members of SPI-B (the U.K. Government’s Scientific Pandemic Insights Group on Behaviours) that they opposed the use of fear to control public behaviour is demonstrably false. It’s a minuted fact that they advised directly threatening a sizeable proportion of the U.K. population:
It’s disturbing enough that a group of senior academics see fit to deny historical fact in a major medical journal, yet Dodsworth’s other anxiety is even more troubling:
My second significant concern was the astonishing idea that the authors could “leave aside the ethical and political dimensions of this argument”. How can psychologists leave aside the ethical dimensions of using fear, whether for an article or advising Government and drafting the plans in the first place?
The psychologists base their claim that they wouldn’t have recommended threat (even though they did) on a selective reading of the literature:
The scientific literature tells a very different story. It shows that frightening people is generally an ineffective way of persuading them to engage in health protective behaviours.
However, basic facts, most scientific research in the field, and their previously published writings undermine their denial.
Ethics-free behavioural science is impossible if it is used to change behaviour
Professors Reicher, Drury, Michie and West were all members of SPI-B. There is no record of any of them objecting to the use of “hard-hitting emotional… threat”. Yet this is such an extreme recommendation that it’s surely reasonable to conclude that they would have opposed it had they disagreed with it.
The idea that you can separate behavioural science from politics and ethics shows lack of knowledge of all three disciplines. It is possible to use scientific methods to try to understand human behaviour without making value judgements, but it’s impossible to endorse techniques to change human behaviour without being slap bang in the middle of the ethical arena.
And this, undeniably, is where they sit. They say, for example:
Information is important and must provide clear and specific guidance for exactly what behaviour individuals should adopt to implement social distancing. …
‘Protect each other’ messages should stress how desired behaviours benefit the group and protect its most vulnerable members, including those we love. …
Messages should give clear, specific and calm advice, helping households to plan together how to commit to social distancing. …
Messages should be communicated via professionally designed and appealing mass and social media campaigns.
These are imperative statements. They cannot possibly be ethically neutral. They are central to the authors’ entire position – lay them to one side and there is nothing left.
It’s definitive of ethics that any intervention in the life of other sentient beings requires justification. It’s a fundamental component of ethical deliberation. All ethical codes, principles and standards are premised on it.
At least some SPI-B members appear unaware of this elementary fact. Instead, they regard the application of methods of persuasion as an unproblematic technical exercise – a pragmatic approach to behaviour change which has no need to justify its goals, need take no account of the diversity of human values, can ignore established principles of applied ethics and – incomprehensibly – is able to overlook the complexities of human psychology. Like Dodsworth, I find this extraordinary.
A similar document by other behavioural scientists – MINDSPACE – published by the Cabinet Office, shows equally questionable assumptions. A wordsearch of the MINDSPACE document for ‘ethical’, ‘ethics’ and related terms returns no results. Reicher et al.’s work is equally free from mention of ethics. MINDSPACE does raise what it calls the “moral hazard problem”:
If we think the state is making decisions for us, we may absolve ourselves of the responsibility to take charge of our own behaviour.
Which is a bit rich since behavioural scientists of this ilk don’t trust us to take charge of our behaviour in any case. The entire point of MINDSPACE – indeed the entire point of applying behavioural science at all – is to make people think and act in ways we would not otherwise do.
This is manifestly not an impartial endeavour, yet Susan Michie, one of the SPI-B group, explicitly believes it is. According to her, it is sufficient merely to provide the conditions most likely to achieve a “specified behavioural target“. She sees her job as nothing more than creating “reliable classifications” to help identify which “modes of delivery” (MoDs) will work best in which circumstances:
By providing greater clarity about how an intervention and its components are delivered, researchers can add to knowledge as to how MoDs influence intervention effectiveness, both directly and in interaction with other intervention-related entities. This will inform the selection of appropriate MoDs for interventions.
Value judgements, ethical deliberation and goal justification are simply not in the picture. All that matters is whether a strategy will change whatever behaviour happens to be in the scientists’ sights.
It’s difficult to understand how anyone can maintain this point of view. It contradicts a fundamental of Western thought, namely that ethically aware human beings are bound to consider the moral calibre of both the goals and the methods of their actions. It’s almost universally accepted that the first question that should be asked by anyone with moral conscience is “should this be done?”, not “does this work?” It is no small matter that a group of influential behavioural scientists do not appear to recognise this.
Other behavioural scientists are more perceptive, suggesting moral limits to behavioural science interventions. Dr. Helena Rubinstein writes:
In the past, there has been public unease about the use of the psychological sciences in the commercial sector. This produced a backlash against apparently subversive techniques, but also resulted in the setting up of a code of practice supported by the industry.
The same may be needed with respect to the use of behavioural science. As a starting point, we suggest the following guidelines:
1.Behavioural interventions built on untruths are unacceptable.
2.Nudges that make it difficult for people to choose otherwise are unethical: people must have the freedom to choose differently.
3.Behavioural interventions should be scrutinised for unintended, as well as intended, consequences.
4.Consent should not be hidden: interventions should be transparent wherever possible.
5.Practitioners should be comfortable to defend their approach, methods and motives in public.
Unlike Michie and her colleagues, Rubinstein understands that there is a profound ethical difference between exercising methods to change a person’s behaviour if he or she requests help, and exercising methods to change a person’s behaviour without being asked.
The scientific literature shows that using fear to change behaviours can be an effective strategy
Reicher et al. cite a single paper in support of their claim that frightening people is an ineffective means of persuasion. Unfortunately, they do not seem to have read it fully. Despite what they suppose it says, it affirms that threatening people does work so long as you enable them to act to mitigate the perceived threat:
Current evidence shows that information about the severity of possible negative consequences from risk behaviour may prompt defensive responses. These counterproductive responses may be avoided by providing instruction on how to successfully implement the recommended actions as well as convincing people that they are personally susceptible to the threat.
This is precisely the approach which underpins the fear tactics the group advised and now want to deny – threats do work given certain conditions; therefore, threatening people can be considered a legitimate behavioural science strategy. This conclusion is further supported by a massive meta-analysis which for some reason they overlooked:
Fear-based appeals appear to be effective at influencing attitudes and behaviors, especially among women, according to a comprehensive review of over 50 years of research on the topic, published by the American Psychological Association.
These appeals are effective at changing attitudes, intentions and behaviours. There are very few circumstances under which they are not effective and there are no identifiable circumstances under which they backfire and lead to undesirable outcomes,” said Dolores Albarracin, PhD, Professor of Psychology at the University of Illinois at Urbana-Champaign.
The authors’ argument contradicts their other work
Reicher et al. maintain that it’s advisable to: “Avoid authoritarian messages: Messages based on coercion and authority can in some circumstances achieve large changes in the short term but can be hard to sustain in the longer term.”
Yet this is the polar opposite of what they say in other published work. Susan Michie, for example, has extensively promoted a “behaviour change wheel” (BCW) which she describes as “a new method for characterising and designing behaviour change interventions”. At the hub of her wheel there are “three essential conditions: capability, opportunity, and motivation”, “nine intervention functions aimed at addressing deficits in one or more of these conditions” and “seven categories of policy that could enable those interventions to occur”.
These are summarised graphically:
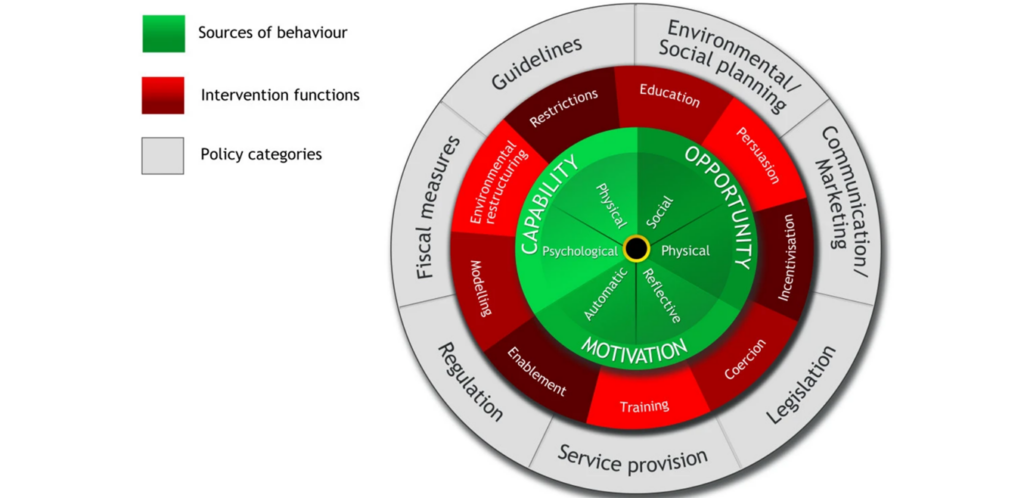
The idea is that any behaviour requires capability, opportunity and motivation. If you want to change a behaviour you can use a range of interventions (in red) and broader policy (in grey). Taken in isolation this makes some sense, but when the BCW is examined in conjunction with the groups’ advice on “harnessing behavioural science in public health campaigns” it becomes absurd.
Michie and her collaborators urge caution about implementing restrictive measures for epidemics. Yet this, unambiguously, is what her BCW advocates: “restrictions”, “persuasion”, “modelling”, “regulation”, “training” and “coercion” are all essential tools of this type of applied behavioural science.
In previous publications they consider coercion a useful manipulative tool, in their denials they don’t: “We recommend coercion. We don’t recommend coercion.”
This is classic double-think – the acceptance of contrary opinions or beliefs at the same time. In case there’s any doubt, coercion (which they favour) involves threatening people (which they claim they didn’t want to do):
Coercion involves compelling a party to act in an involuntary manner by the use of threats, including threats to use force against that party. It involves a set of forceful actions which violate the free will of an individual in order to induce a desired response.
(Coercion is the) use of force or intimidation to obtain compliance.
(Coercion) occurs if one party intentionally and successfully influences another by presenting a credible threat of unwanted and avoidable harm so severe that the person is unable to resist acting to avoid it.
Apparently they have left memory, logic and reason to one side as well as ethics.
Their view of ‘empowerment’ is twisted
The scientists say they really wanted to ‘empower’ us:
This emphasis on empowerment is even clearer when one looks across the corpus of SPI-B reports. It reflected a conception of the public as an asset rather than an impediment in the pandemic. The advice was to engage with the public and focus on supporting them in doing the right thing rather than assume they need frightening and coercing in order to stop them from doing the wrong thing. This is particularly clear in another report of April 3rd 2020 on “harnessing behavioural science to maintain social distancing” (subsequently published as a journal article). Among the key principles set out in the paper were the need to avoid authoritarian messaging based on coercion, an emphasis on enabling behaviour rather than the use of punishment or castigation, and the need to engage with communities in order to co-design interventions with them as opposed to imposing interventions upon them.
SPI-B did indeed recommend giving people control. But not because they consider personal autonomy an intrinsic human good, rather because limited freedom of choice is thought to increase compliance with ‘doing the right thing’. In normal parlance, if you empower individuals, you enable them to choose for themselves. In SPI-B speak ‘empowerment’ means ‘enabling them to do the right thing’ as defined by ‘experts’ who self-evidently know best.
It’s very hard to see how fostering population-wide guilt, nationwide mass media propaganda campaigns and targeting potentially recalcitrant groups of people is empowering according to any established use of the term.
They believe the only thing that matters is that a behavioural intervention works
Every moderately educated school student understands that ‘the right thing to do’ is usually open to interpretation. In a diverse society ‘doing the right thing’ can have a different meaning for different people. ‘Doing the right thing’ can mean protesting authoritarian restrictions on free movement and assembly, or writing articles critical of Government policy, for example. How can university professors fail to understand that in social context ‘doing the right thing’ is a contested concept?
Michie laments that the U.K. Government failed to use key elements of the BCW (even though it did use them):
Just by identifying all the potential intervention functions and policy categories this framework could prevent policy makers and intervention designers from neglecting important options. For example, it has been used in U.K. parliamentary circles to demonstrate to Members of Parliament that the current U.K. Government is ignoring important evidence-based interventions to change behaviour in relation to public health. By focusing on environmental restructuring, some incentivisation and forms of subtle persuasion to influence behaviour, as advocated by the popular book ‘Nudge’, the U.K. Government eschews the use of coercion, persuasion or the other BCW intervention functions that one might use. (My italics)
In other words, government is too flaky. It should use whatever might work from the BCW smorgasbord without worrying about ethical niceties:
The BCW… forms the basis for a systematic analysis of how to make the selection of interventions and policies. Having selected the intervention function or functions most likely to be effective in changing a particular target behaviour, these can then be linked to more fine-grained specific behaviour change techniques (BCTs). Any one intervention function is likely to comprise many individual BCTs, and the same BCT may serve different intervention functions… Thus, the BCW approach is based on a comprehensive causal analysis of behaviour and starts with the question: “What conditions internal to individuals and in their social and physical environment need to be in place for a specified behavioural target to be achieved?” (my italics)
As Laura Dodsworth notes, Michie and her colleagues do not exclude any interventions – if an intervention will change a behaviour they can see no reason not to implement it. If you’re oblivious to ethical considerations then what is to stop you advising the use of fear?
No-one asked them to manipulate our behaviours
The collaborators are proud of their controlling tactics:
As a group of behavioural and social scientists who have shared their advice with Government through the U.K.’s Government Office for Science, we have collaborated to develop a series of principles to inform interventions to promote whole population adherence to social distancing measures.
Their paternalistic assumptions are overwhelming. Perhaps the biggest is that the ‘whole population’ needed coercing to ‘adhere’ to rules we had no part in making, were not consulted about, and for which there was no clear evidence:
Airborne transmission of COVID-19 is highly random and suggests that the two-meter (6 foot) rule was a number chosen from a risk ‘continuum’, rather than any concrete measurement of safety.
Early social distancing is either doing nothing or making things worse. This is likely because the virus spreads mainly in hospitals, care homes and private homes rather than in the community, so social distancing of the wider population beyond a basic minimum (washing hands, self-isolating when ill, not getting too close, and so on) has little impact. The countries with the highest death tolls are often those which fail to protect their care homes adequately, with up to 82% of COVID-19 deaths occurring among care home residents.
SPI-B uncritically accepted the need for social distancing, made no recommendation to educate the public about the actual data, and had no interest in enabling people either to dissent or act on any alternative view. Informed consent was simply not a consideration.
What does this ‘behavioural science’ amount to?
Having read other publications by the main authors, and considered similar behavioural science writings, I conclude that the only possible answer is ‘not very much’. As far as I can see, at least in the hands of Michie and her colleagues, the primary function of applied behavioural science is to manipulate people into acting in ways we would not naturally. It assumes a crude distinction between ‘doing the right thing’ and ‘doing the wrong thing’ the manipulators think requires neither explanation nor justification. It also assumes that those of us not equipped or not willing to do ‘the right thing’ need to be persuaded to do it, using crude psychological devices. The use of threat, coupled with Orwellian ‘empowerment to comply’, is one such device.
I cannot find any more substance than this. If I’m mistaken, I’m open to a mutually informative discussion in public.
Finally, on a personal note, having published a frustrated analysis of Covid evidence and policy in September 2020, both mystified by and critical of the woeful thinking and insidious coercion we were all subject to then, my advice to the behavioural scientists and the many others addicted to control remains the same four years on. The public is neither an ‘asset’ nor an ‘impediment’. We are knowledgeable human beings able to make our own choices given the chance. We need unfiltered information, unbiased support to process it if necessary, and practical democratic mechanisms that allow us to respond – free from coercion – to policies that affect our daily lives.
David Seedhouse was the first lecturer in medical ethics to be appointed to a U.K. university in the 1980s. He is currently Honorary Professor of Deliberative Practice at Aston University.












To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
There is ample evidence that covid was in the UK before November 2019
We were on holiday at the end of October and the hotel had a few coachloads of Chinese tourists stating for 1 or 2 nights. A week after we returned home we both came down with “An Unknown Flu Like Virus” – Doctors words on the note my wife obtained to present to work. It took a long time to shrug off.
We went to a Christmas event and several people we spoke to had a similar experience
We live in East Anglia, the UEA has several Chinese students, Felixstowe is just down the road and has the largest UK container port owned by a firm based in HK
Some might say coincidence and tin foil hat
Lots of some virus around in autumn of 2019, i got something very like what became known as covid in late Sept/Oct after going to a college reunion attended by people from all over the world. I had a temperature for a couple of days and a dry cough that lasted for several month. Several friends had something similar over Christmas. I don’t think it’s coincidence, I think this has been around for long before it was branded as covid and a PCR test devised to find it. God knows what that test is finding now, the common cold?
I know this sounds ridiculous, but…in May 2019 I took a flight on holiday. I have always been prone to catching bugs on flights, and this was no exception. I was really ill. So utterly exhausted with a terrible cough and banging headache with a high temperature. (Spoiled the holiday). I could barely breathe so went to my gp when I got home and was prescribed a steroid inhaler for the first time in my life. It took me many weeks to recover, but, a few months later I developed heart problems, for which I will be on medication for life. The heart thing could be coincidental, but up to that point I had been in good health. Whatever it was, it was most certainly some sort of coronavirus. If I had had it a few months later, it certainly would have been counted as covid.
Incidentally, despite doing my best to ignore all government edicts, I have failed to catch covid 19!
Also “ridiculous”, and I’ve mentioned it on here before…..late May 2019 we were in Salou, only an hours drive away from where the water samples @Arfur Mo mentions below were taken, (it was Barcelona btw and the samples were identified in April)…..and myself and my partner were hit with a 5 day bout of persistent cough, sore throat, fever and listlessness.
So were our Belgian friends who had arrived a week before us, and my sister and her family who arrived a few days after us, both of whom were staying in different hotels. In fact wherever you went in the resort people were coughing all over the place and the pharmacies were choc a block with people buying cold remedies.
We are convinced we have had covid…..my biggest surprise given the amount of people that would have been infected with this in that area during that period is that I haven’t heard anyone else refer to it at any point since.
Of course at that point it wasn’t marketed as the “danger” it is now.
Good that you were actually treated, before the edict that COVID sufferers were not to receive treatment until hospitalised! It sounds like your GP knew what they were doing; budesonide (as inhaled steroid) has just been retracted as a recommended treatment in the UK, for unspecified reasons but presumably to make way for the much more expensive treatments from Merck and Pfizer.
There have been reports from Spain and/or Italy(?) that the virus was also found in potable water samples taken in early 2019.
There also the bizarre short lived ‘vaping disease’.
My wife and I came down with something unusual in that November. We did not know what it was but the main symptom was a temperature and strange fatigue. We have often wondered if it was covid. Too late for antibody tests.
Tcell spot test available through Oxford immunetic. Long term immunity can be measured.
I’ve been sitting on this for a while because it sounds too far fetched. At Christmas 2018 I had the worst flu I have ever had. The illness lasted about a week, and the debility and fatigue went on for about another month. The symptoms were a very deep deep chesty phlegm producing cough, tightness of chest and pain breathing, high fever for several days with night sweats, continual headache, fatigue, loss of taste, loss of appetite. I self medicated with Bushmills malt and paracetamol. Even then it was difficult to see a GP so I didn’t bother. I have until now thought it was just a very bad flu, but the symptoms match exactly.
How do these symptoms differ from those commonly seen for OC43, HKU1 or Influenza A?
I’m not saying it couldn’t have been SARS-CoV-2 or something similar that’s as-yet unclassified, just interested to understand why you think it’s this rather than something else.
The clue is in the exact match of the described symptoms, with nothing like it experienced previously, in spite of having had the flu.
It’s not an exact match to the March 20 Covid, because that was a dry repetitive cough. But could have been a very early variant I guess.
Which of those symptoms aren’t a match with the list of symptoms for OC43?
Pah! I had COVID on Jan 1st 2000. Headache, nausea, lethargy, all the tell-tale symptoms. Luckily it only lasted a day.
Luxury! And you try and tell the young people of today that and they won’t believe you. How was the risotto and Château de Chasselas?
Oddly enough I can’t remember. The Covid seemed to strike sometime after lunch on New Year’s eve caused complete memory loss about events between then and the next day. A nasty little bug.
I had 2 days of missing time
You and me both, went to bed on the 20th December and dragged myself out of my pit on the 3rd January. Never experienced anything like it. A week or two later I was recounting my experience to an elderly neighbour, he did the usual ‘That’s nowt’ cry and then regaled me with his experience overseas with the Asian flu, fell asleep on a Sunday after dress parade (military) and woke 5 weeks later. He said they’d sent a telegram to his parents saying he’d probably be dead by the time they received the telegram, them were the days….. LOL
Was he in a shoebox int’ middle’t royd?
If you are exposed for the first time to a new novel variant of Influenza and it belongs to a variant group to which your immune system has not been previous primed you will often get very seriously ill. This happened to me in 2009 with Swine Flu (H1N1).
Despite a very long history of almost constant viral respiratory infections going back almost two decades (due to a undiagnosed medical condition) Swine Flu was in a complete different league when it came to severity. Took me months to recovery.
The timeline for the first appearance of SARs CoV 2 in the general population in Wuhan is Q1 2019 as the desperate attempt by the CCP at cover up started in April 2019. The clinical symptoms of all upper respiratory viral infections are pretty much the same. The infection of the olfactory nerves is usual but not unique to SARs Cov 2. It is not uncommon with other human corona-viruses.
In fact the “really bad cold” most people have once or twice a decade is usually a human corona-virus infection. Because thats how long HCOV infection immunity usually lasts. And most HCOV infections in adults tend to cause at least mild symptoms. Although that’s not the way it feels at the time. They usually account for at least 10% of all pneumonia deaths every year.
That’s all good to know, thanks!
I came down with a summer flu like virus in late July 2019, took me out for around 10 days. Due to a number of reasons, I put it down to picking it up in the water a few days before. I had been at my local beach, where you can see Felixstowe port in the distance. I was the only person in my family/social group who didn’t come down with the winter viruses 2019/20.
The military games were held in Wuhan September 2019.
In October 2019 we had several patients attend the urgent care centre with cough lasting weeks. This was in Leicester, with De Montfort and Leicester Universities both having significant numbers of Chinese students. I had a cough lasting 6 weeks with change in taste for the last 7 days, on reflection I wish I’d gone to see my GP, but the problems resolved themselves so I didn’t. I live in Loughborough and my wife works in the library there, again with a significant number of Chinese students.
LOL. Are you mates with the author of this hit piece, with the tinpot covid detective hat on.
Its funny you mention Felixstowe – I came down with a flu-like virus just a week or so before the very first lockdown (3 weeks to flatten the curve) back in March 20/20 – I caught it off my brother who had been working in Felixstowe for a number of weeks there when he came down with the flu-like bug and travelled back home to recover – I caught the virus when i visited him with some shopping – both himself and his wife were too ill to go out for some grocery shopping themselves so I got a few items for them – a couple of days later I came down with the very same flu-like virus – lasted about 4/5 days – and it spread like wildfire throughtout my family – we all treated it like bad case of flu because thats just what it felt like – some had it milder than others – I didn’t even bother going to the doctors with it – treated it with plenty of rest, sleep and paracetamol (lemsip) for when I felt a bit rough but generally just stayed home for a few days (as you do) until I got over the worst of it – the endless coughing was annoying though.
“ the endless coughing was annoying though.”
that was what I ended up with after a short-lasting respiratory infection in March 2020 (raided temperature two days, lethargy and nausea for another 3-5 days). The cough lasted for months, and occasionally I can still the aftermath.
Several people I know had the same thing, but most of them were ill around Xmas 2019.
I don’t know if it was CV19, but I’ve had absolutely nothing since then. Not so much as a sniffle.
Yes, the cough. I had a mystery cough that started in late July – early August 2019. It persisted and I coughed up a lot of sputum. After trying the usual pharmacy concoctions unsuccessfuly (and not wanting to take antibiotics) I saw a homoeopath three times over the next 2 months and I got the impression he was mystified by it. Eventually it petered out late November after I started taking a herbal mixture of ivy-thyme, made by Vogel and obtained at the local health shop. I also heard, anecdotally, about other local people getting ill in December with covid like symptoms.
Incidentally, a decade ago my wife developed heart failure. One possibility that persists in our minds is that it may have originated from an unknown viral infection, acquired during a plane trip to Trinidad. On the same flight there was a large contingent of moslems returning from Mecca (via London). One individual was clearly unwell and coughing a lot. My wife made the mistake of going to the same WC after he had just come out of it. Coincidence?
There are apparently several Chinese/HK owned businesses in Northern Italy thanks to economic issues a few years ago so not really surprising the virus appeared there.
Also, if developing some sort of pathogen in a lab, you’d surely need to know how it affects humans in the real world as lab animals might not respond in the desired way. I guess if you can design something that will incapacitate super fit military folks, the general population will be far harder hit.
Another one here- first week of January 2020 I had 9 days of flu-like illness, loss of smell, a headache that even doubling up on ibuprofen and paracetamol didn’t shift, a fever, a cough that lasted for weeks and chilblains (later rebranded as “covid toes”). Pretty sure I caught it at a New Year’s Eve party, since I really hadn’t been anywhere else. I was confined to bed for a few days, though I did drag myself out to a large and busy supermarket in the middle of it for more painkillers. I couldn’t get a doctor’s note so I had to go back to work, where they took one look at me and sent me back home.
I’ve never been troubled by flu before but just assumed that’s what it was, until the covid toes thing came out. I took an antibody test earlier this year but it just said I hadn’t had covid on the past 6 months, which I knew!! I wish I’d taken one sooner but they were only available for a short time in 2020, quite expensive and then were withdrawn from sale.
And despite my best efforts, including sharing a bed with a certified covid-ridden husband, I haven’t managed to catch the thing since.
Much like me and my other half, December 2019 to end January 2020. Mild fever, felt rough, loss of taste, horrendous cough…worst I’ve ever had. You could cough for an hour at a time, with brief respites, which left you gasping. I was better in about a week, his lasted longer, but neither of us have had so much as a sniffle since.
And we don’t wear masks, sanitise everything in sight, or shy away from people, yet here we are!
If China should get around to producing and using an ethnically targeted bio-weapon, it could be all too easy, couldn’t it?
We were on a cruise no. Atlantic July 2019. Very ill with cough, fever, difficulty breathing, bedridden. Seen by ship doc. Came home still unwell, nurse at surgery said when asked what was wrong with me “we are seeing some very weird viruses”. More antibiotics given. Bus loads of Chinese everywhere we visited on the cruise. Probably just coincidental.
our corrupt pharma funded scientists and government can see the Moronic is peaking in S Africa – Now is the time for a ‘circuit breaker’ lockdown so as to take credit for the natural peak of infections when it inevitably happens in the UK – and the charlatans can tell the sheep, ‘imagine how bad it would have been if you hadn’t had your
ineffectivebooster’Plus “It would have been over quicker if not for all the selfish anti-vaxxers”
It’s possible, here too they introduced lockdowns when we were coming near to the peak. They know by know there is a time line to the peak as well, whatever intervention is used.
Having said that, in NL they seem to be turning to panic mode. Infections and hospital admissions are coming down – but there is going to be a new unscheduled press conference tonight and it’s already been leaked that the OMT has advised that everything but essential shops be shut down. Went to the shops earlier, absolutely heaving because people have heard rumours a total lockdown will start this evening.
If that’s the case, something else is going on. To shut down everything one week before Christmas, even though the numbers are going down – they’re scared of something. They might get away with saying a shutdown starting as of Christmas, but in the busiest days before Christmas when people still have tons to do – nope, that will cost the government dearly and if it does happen, it’s because they are truly worried.
I’ve said before, NL started it’s vaxx roll-out late and it was prolonged. We now have almost the entire vaxxed population probably in negative effectiveness territory, right as we go into the darkest, coldest time of the year with people mingling indoors. I’m sticking with the belief that there is ADE or something like that going on and they are terrified where it could go.
There’s now ample evidence that the vaccines make things worse. Eg, the latest data from Imperial College show this quite clearly (eg, see here)
IMO they know that they’ve made things worse and are desperately trying anything that might help — hence the mad rush for boosters. I think that this will only make things worse again (they’ve got about two months post booster with a positive effect, then it’ll likely go even more net negative).
I note that they’re not actually telling us this — I presume that they’re scared of the public reaction if they knew…
That should be easy to see in NL then. They started handing out boosters to the over-80s at the end of November – which would put them back in negative territory some time in February. The OMT is predicting a rise in omicron infections starting in January.
So the most vulnerable in negative territory, right as a fresh wave of the most infectious ever (well, until the next most infectious ever) variant starts, coldest time of year, a winter indoors without fresh air and sun. This will be running alongside a continuing booster campaign (i.e. all those people with extra susceptability up to 2 weeks after being poked, feeling invincible after getting the 3rd poke) – they don’t expect to have everyone here poked until some time in March.
The next couple of months are going to be sooooooo long. Bears have the right idea.
It occurs to me that all those people who can’t go on foreign holidays in the sun will have lower vitamin D levels than normal.
Your article suggests that they are piling mistake upon mistake and following your last paragraph about natural immunity if they were to force the unvaccinated to be jabbed against their will they would be criminally robbing them of the strength and protection of their natural immunity.
I’ve been wondering if they at least suspected that they had made things worse for the jabbed. In that case though, and barring a level of criminal genocide that even I can’t credit, surely they would at least leave the un- vaxxed alone and quit pestering them to begin their ongoing jabathon?
The current process might have short-term mitigation against NHS overwhelm but they are surely factoring in a major cancer/stroke crisis in the mid-term. If I were BJ I’d be seeking an exit-strategy and heading for the hills rather than pledging to take the Party into the next election.
According to the HSJ, as an extra incentive to ‘get it done’ pushing boosters, GPs and pharmacies will be paid an extra £5 per jab between Christmas and the New Year.
A slight whiff of desperation in the air?
But they will still scrupulously ensure free and informed consent…
Never mind, they can “vaccinate” the elderly every 50 days…
Reapeat after me: There is NO, zero, zilch, correlate for immunity against SARs CoV2
Nonsense. What is the evidence for this statement?
Read Stanley Pearlmans papers on T cell immunity, understand the mechanisms of the innate immune system from first principles, construct a mental picture of what exactly happens on infection from a respiratory virus in the epithelium, how the innate immune system recognises the first protiens expressed by the cell (hint: not the spike) and the long chain of events that happen BEFORE we produce antibodies.
Then understand the secondary response, where antibodies come in to clean up the cell debris from the infection, undersand affinity.
Then describe what happens when the spike protien is injected into the muscle (where non of the parts of the innate immune system reside) and you may begin to understand why antibody levels are NOT a correlate of immunity.
I started finding Pearlman’s papers , but was distracted by another paper referenced to one of his;
”T-cell responses to MERS coronavirus infection in people with occupational exposure to dromedary camels in Nigeria: an observational cohort study” by a whole host of Wangs and Chens etc. Must be something significant in there…..
Best to understand innate/adaptive immune systems from first principles first, but yeah I agree with your point, but you’re not going to see that “something significant” from a couple of papers. Start here: https://drasticresearch.org/
come back in 6 months when you’ve worked out where UNC/DARPA fits in, so you can head off the limited hangouters like Ridley et al. and see the bigger ~20yr mRNA transfection development picture.
It is not surprising that the Drastic site refers to a purported Chinese bioweapon site but not the numerous known US bioweapon sites. FWIW I do not believe SARS-CoV-2 was an explicit bioweapon, rather something long anticipated for use as a political weapon of mass destruction.
These are countries hosting US outsourced bioweapons research labs (to sidestep the 1974 Bioweapons Convention), not the number of labs. There are at least 12 in Ukraine alone. Even the UK Porton Down labs are involved (one experiment involved the release of an unidentified aerosol at an unidentified operational London Underground tube station).
http://dilyana.bg/wp-content/uploads/2018/04/51-696×465.png
The host countries have no or limited say in what research is carried out. The US ‘sciencetists’ (often private contractors) operate under full diplomatic immunity, including immunity to luggage search. There have been reeports that these labs have also been used by Big Pharma to carry out drug trials on poor, foreign people. There have been numerous strange disease outbreaks close to these labs.
https://thealtworld.com/dilyana_gaytandzhieva/the-pentagon-bio-weapons
Remember there are now 2 DRASTICs (my link is the original independant bunch with Billy Bostickson, Yuri runs the compromised limited hangout bunch) plus the Sirotkins work who were ousted (by Yuri) early on.
Having followed this for almost 2 years, I think the clearer picture is about development of an mRNA transfection platform, DARPA funded Moderna into existance (as a limited hangout?) they were all originally looking for something to use a similar entry route as HIV to transfect cells, hence all the collecting of SARs viruses to use as a chimera mRNA load carrier. “Bioweapon” kinda puts the wrong emphasis on it IMO, tho I agree it all does look too much of a coincidence to be anything non nefarious.
They had to work out how to beat the natural immune response to get the mRNA transfections to work, did they know the method they chose reprograms the innate immune system? Did they even care? Is this why they need 100% of people vaccinated regrdless how illogical it seems? Do they need to eliminate the control group to hide the evidence?
Don’t want to appear rude, but I was posting about this stuff over 12 months ago. Our German/Californian legal friend has assimilated quite a lot of evidence about these developments and Fauci’s involvement since his AIDs days.
I was just trying, unsuccessfully to introduce a bit of levity into a dire situation. If we lose our sense of humour we are truly dead.
non taken, crack on matey
The case numbers do seem to decrease a little in the period about 2-3 weeks after vaccination.
That said, I agree with your analysis — the role of IgG antibodies in fighting covid appears to be very limited.
There’s also very little in the way of cellular immune response after the vaccinations.
I think it is likely that most of the initial findings that the vaccines were effective against covid were illusory — this was to do with who was vaccinated and when.
I think there may be a role for very short lived IgA antibodies in protecting against covid, but this effect is gone by about 50 days post vaccination. After that point they appear to make things worse.
Case numbers are nonsense, even Dr. Peter McCullough said as much on Rogan recently, they found something like 97% false positives in “Asyptomptmatic” infections in the paper he quoted.
If you’re “Asymptomatic” you ain’t shedding viral particles. Period. The virus is endemic already.
“Effectiveness” of the vaccines were quoted in relative numbers, in absolute numbers the effectiveless was <1%.
Logically the innate immune response to all ~31 epitopes is at least 30x more effective against SARs CoV2 than antibodies to a single protien.
If there’s a rise in cases post jab/booster (which appears to be the case in most countries) I find it more indicative of the short term negative effect on the innate immune system. The longer term effects are more worrying IMO
https://www.medrxiv.org/content/10.1101/2021.05.03.21256520v1
I think there is something going around. I don’t accept that it is a problem except in some vulnerable groups (the elderly and obese, mainly).
While I agree that asymptomatic people generally don’t spread covid, it is likely that the vaccinated have a suppressed innate immune response which is leading to very high viral loads without much in the way of symptoms — thus it is likely that the asymptomatic vaccinated do spread covid.
Vax shedding is a different thing, we know the spike gets into exosomes, we know exosomes can be found in the epithelium, logically they could be shed via this route, but we need data to prove it, who’s going to fund THAT study (lol as if)
This is not the same as “asymptomatic” spread of SARs CoV 2.
It is already known that shed exosomes carry viral particles.
“Virus-infected cells release exosomes that are implicated in infection through transferring viral components such as viral-derived miRNAs and proteins.”
https://pubmed.ncbi.nlm.nih.gov/32544615/
But how much, and for how long, do multiple vax make it worse, what effect does it have on controls etc. this is the data we need to draw any conclusions.
Sure — it is amazing what we still don’t know — almost as if they don’t want to know…
I’d certainly like to see the studies — we’ve 2 years into covid and 12 months into mass vaccination and still there’s very little work done on how they work vs natural immunity and pretty pathetic efforts (government funded) into vaccine side effects.
Even the effect on the ‘vulnerable is a bit of a myth – right from the start it was noted that it was mainly replacing other causes of mortality, with a mean age of death higher than the natural average. Vulnerable people die.
What’s more, they didn’t vaccinate those about to die, leading to misleading estimates of how well the vaccines were doing.
From the paper:
“In conclusion, the mRNA BNT162b2 vaccine induces complex functional reprogramming of innate immune responses, which should be considered in the development and use of this new class of vaccines.”
If that is the case, then these drugs are opening the route to a lot of non-covid grief for those having taken them.
Maybe this explains why Pfizer has bought up a company specialising in producing drugs to deal with immune system issues.
Headline: Arsonist buys fire truck company
Nice country you got there. Shame if something …. bad …. was to happen to it. Capiche.
The Pfizer study looked at people who had covid like symptoms. It’s perfect reasonable to think that the vaccinated group may well have had the virus but the symptoms were subdued enough that this group didn’t feel bad enough to report anything.
being infected is one thing, being symptomatic is another thing, asymptomatic shedding is not a thing.
Don’t ruin the BBC’s over simplified explanation of immunity.
The Fallacy that antibodies=immunity is the lie this whole transfection charade stands on.
If everyone understood the correct basic immnuo biology, this thing would be over by the morning.
Nice summary of something knowledgeable people have been saying for 22 months.
Didn’t stop them then, won’t stop them now. If the French senate ignore this when voting on changing the health pass to a purely vaccine pass I think we will all have confirmation that ‘this is not about what they say its about’.
I think we will all have confirmation that ‘this is not about what they say its about’.
I think we’ve had that confirmed many times over, but more confirmation is always to be welcomed even though we already know that the “the authorities” will remain totally blind to it.
Missing from the Amanuesis article is any direct reference to the scandalous level of death and damage caused by the Covid vaccines, that aren’t vaccines.
I’ve spoken about this elsewhere.
It appears that there’s a negative net overall effect when non-covid hospitalisations/deaths are taken into account.
I think we already know don’t we..
Macron and his cohorts were sent in to destroy France, and are now doubling down.
and they appear to being cheered on by a majority of the French.
No one knows how safe it is to give mRNA vaccines repeatedly – annually or more frequently. We do know, however, that Moderna switched to making vaccines because the company had found unacceptable side effects with giving mRNA products as a drug i.e. repeatedly. Vaccines were viewed (at that time!) as a one-off intervention and thus not subject to this problem.
Amanuensis also mentions influenza vaccines as an example of a vaccine that is given annually without safety concerns. Those vaccines don’t contain adjuvants, apart from the version given to people aged 65 and over. The lipid nanoparticles in mRNA vaccines apparently act as an adjuvant and there is concern that giving these annually could have deleterious long-term effects.
Apparently the FDA has separate evaluation paths for ‘vaccines’ and ‘genetic therapeutics’. The vaccine route has less onerous qualifications. Surprise, surprise.
The mRNA vaccines contain PEG why was flagged as an adjuvant early on
https://www.authorea.com/users/318363/articles/448294-polyethylene-glycol-as-a-potential-adjuvant-treatment-for-covid-19-induced-ards
I thought adjuvant use was common in recent ‘vaccines’. Cheap adjuvants to do the heavy lifting coupled with some patented semi-plausible magic sauce to allow for a x100 to x1000 price tag seems to be the route to riches.
Surely the time has come now for more direct action, if we all request LFT kits daily then throw them away then the supply will last hours and the problem will disappear. It’s easy, a kit online and one from our local (x3) chemists.
Then can’t be bought for ‘love nor money’ in chemists in Central London. There is no timescale for delivery of new stock.
Would a box of these make the ultimate Christmas gift?
The new boxes we opened at work last week have replaced the plain old blue and white packaging with a fancy new logo and the words ‘not for resale’
For someone you want to worry to death?
What do you mean you are only testing once a day! You selfish under-tested spreader.
This is brilliant. I think the talk of BCGs is useful as this is something that people can easily relate to. This piece might be strengthened by the addition of a few references to studies in my view.
Did a post about this here the other day with a couple of links stolen from other dailysceptics commenters if anyone’s interested:
https://drkmatr.substack.com/p/jabs-every-3-months-no-thanks
That immunity acquired through infection is superior to that acquired through vaccines is, I believe, now well established. Surely it is better to allow the virus to spread amongst those who are not particulary vulnerable. One of the problems with the booster programme is that it amounts to a medical experiment, in that we simply don’t know whether repeatedly injecting people with mRNA can have any long-term adverse effects. Personally, I am not prepared to take the risk, particularly for a “vaccine” that protects against a virus that in all likelihood will cause me only a mild illness.
Indeed. Early research into the spread of pathogens identified the concept that not every need be immune for a disease to stop spreading – the origin of ‘herd immunity’. They also found that the ‘herd immunity’ level was higher in homogenous populations, ie variation in individual immunity is a good thing.
And it is an experiment. A Phase III Clinical Trial to assess the type and relative risk of adverse reactions. These are normally carried out at the expense of the manufacturer. Emergency Use has been tacked on to allow Big Pharma to get the epidemiological data at no cost to themselves. Legal Immunity also removes the need for them to stop the trial if too many fatalities or other serious adverse reactions occur.
Amanuensis, how greedy of you catching covid twice spare a thought for us poor souls who haven’t had it at all yet! What are our antibodies doing, poor show nearly 2 years on.
spare a thought for us poor souls who haven’t had it at all yet! What are our antibodies doing, poor show nearly 2 years on.
I do struggle with the science on this, not afraid to admit it, what I do know is it’s so new, complex and disputed that I won’t be having it!
A welcome piece, looking at one of the fundamental issues.
However, this whole area of immunity is complex, and, consequent.y, to a range of analysis – some of which are far from as sanguine about the current leap in the dark.
“For now, the booster appears to offer a significant level of protection against infection.”
Not established, I fear. And that’s where we have to roll back to basics to get perspective on these complex issues :
1. This moderate respiratory virus does not require a rush to vaccination.
2. These are not actually ‘Vaccines’ in the defined sense, and need to be treated with caution
3. Reasonably safe treatments cannot be developed in this timescale
4. The abandonment of a proper testing regime undermines any assurance of efficacy or safety
5. Data on adverse events are massively concerning.
6. Observational data is, at very best, ambiguous.
7. The treatment is acknowledged to fail on two major criteria : immunity and transmission.
In the light of all these, speculating about finer points of the immune response is, essentially, polishing a turd.
The important bits are appear and for now. I’m not sure that the effect is real, and I’m fairly sure that any positive effects will be very short lived, with net negative effects after.
And the key point is surely that there is, inevitably, a great deal of uncertainty about the effect of this unprecedented vaccination programme – the effect both on individuals and on populations – which is what makes the policy whereby clinical trials have been subverted and conventional, cautious, practice abandoned such a scandal.
The scientists/doctors advising governments must surely also have similar suspicions, they can’t all be hypnotised (I can believe some are true believers, because that’s how all religions work, including that of the Holy Vaxx).
If you are correct, why do you think they are still pumping this stuff into people?
Genuine belief that there is no alternative to the booster at this point in time, or fear that they will be skinned alive if enough people realise that their health has been put at greater risk than if they had not taken the vax?
this is what I cannot understand, where is the precautionary principle in all this?
It would appear to have been cast out into the desert, along with common sense.
I just read a comment on another thread that is quite disturbing.
The commentor said that they knew someone who had participated in the Novavax trial, had 2 shots, but as it wasn’t recognised for travel, had ended up getting 2 x pfisser + booster. 5 shots for the same virus within 1 year, what could go wrong? And that’s not a rhetorical question, I am really, really curious to see what could go wrong, I suspect the answer is “a very great deal”.
I also don’t think it makes that much difference that Novavax is not mrna, you are still giving your immune system a hiding for, in essence, nothing, particularly if you never actually encountered the lurgy during the time period that you had the all-singing, all-dancing, all-powerful Antibodies.
The beauty for the pharma companies is of course that the pick and mix approach ensures that no single vaxx can be pinpointed in terms of damage, genius.
Big Pharma has total legal immunity for Emergency Use of experimantal drugs as long as the drugs are labelled ‘vaccine’.
The precautionary principle gets in the way of Big Pharma profiteering. There are numerous new billionaires following this scam.
It’s nothing to do with health.
It’s about Control.
Digital ID.
I am not a scientist or medical man, but I was a police officer and I now how to assess and process evidence – both hard and soft i.e. circumstantial.
To my mind, surely the ‘golden rule’ should be – you don’t take a drug to counter any illness that does not pose a significant risk to your health.
Jabbing the young and healthy offends nature – and nature is a very powerful force.
Then there is the instinctive ability to to smell malfeasance; and in the case of covid, one was struck by how quickly governments moved to dismiss treatment, to dismiss the concept of natural herd immunity, to severely stifle discussion of anything but the government’s line on vaccines and to dispense with our human rights to refuse jabs.
NOTHING ABOUT ANY OF THIS HAS SMELT RIGHT.
It is a massive financial fraud. Other motives can be conjectured, but there is so much money flowing with next to zero auditing it makes the $18 billion delivered to Iraq post 2003 by the US air force only for it to disappear without a trace look totally above board.
Peter McCullough (Joe Rogan podcast) says that you can’t get Covid twice. True or false? CDC website says it is very rare (although as a govt body they probably wouldn’t want to commit themselves to ‘never’)
I had it three times in Jan/Feb 2020 over 6 weeks. This was the time that the virus was mutating very rapidly. I suspect I ended up dealing with at least 3 variants, each weaker than the one before (or the immune system was learning to cope better). You might think that medical researches would be interested in looking into such incidents, but nada.
Presumably he means in the sense of getting it as a serious systemic disease, rather than as a cold?
He was unequivocal and said that if you thought you had it twice, actually you had a false positive all times but one. To be honest, this did made me wonder a bit as it contrasts so sharply to ‘folk wisdom’, or ‘folk unwisdom’ as it were.
We’re used to the idea that we can get repeated infections with other coronaviruses (30% of ‘colds’). However, our immune response deals with these reinfections with only a minor ‘sniffle’ in the vast majority of cases.
The situation with vaccine mediated immunity appears to be different — increased risk of infection after vaccination. I fear that there may also be negative consequences in the longer term (as seen with pretty-much all candidate vaccines for coronaviruses tested prior to 2020).
Dear Amanuensis, forgive me for the indirect posting. Picking up on your point on immune escape, I wonder as I think T-Centralen does, how vaccines with ARRs of 0.7% to 1.4% can place any pressure on the viral population in order to produce immune escape. Surely the ‘Wuhan’ variant spike protein (actually patented and printed genetic code as I understand it, and now largely extinct as it has a v. high rate of mutation) will follow Smith’s Law and produce more infective (and less virulent) strains which will successively dominate and infect more widely. This provides a convenient ‘immune escape’ excuse for what is actually ADE from a number of causes, and the severe immuno-suppression, from repeated injections (to all diseases), and this is before taking into account the other vaccine injuries. Might you be in a position to write an article which explores this?
I had it in March 2020 (confirmed with an antibody test) and have it again currently. I’m assuming it’s because this latest variant is sufficiently different to the first to bypass the original immunity. In any case, I don’t feel very well, but in no way is it serious enough to make this much fuss over.
I had similar experience at the end of the summer. I had it originally in July/Aug 2019 (picked it up in transit in France) – was severely affected but my GP said it was “just a virus”. Had nothing – not even a sniffle all of 2020 and most of 2021, until the end of the summer when I think my immune syst encountered delta variant and mounted a challenge. Felt a bit ropey for a couple of days and would have said I had a summer cold and treated it as such – with high dose vit c and quercetin and in days it was gone.
I think I might have had COVID (if it exists) in November 2019, when Saint Boris’s autocue said “it’s nothing to worry about”: coughing and chest tightness I’d never had before. As for BCG, at the time I was afraid of injections, so I “lost” the forms, and sneaked elsewhere while everyone else queued. Nobody checked. Still unvxd there. But it is a good point about “how many is too many?”.
“. . . if it exists”.
No proof that it does. The so-called “novel” SARS virus was never properly isolated and tested live subjects using a placebo group. The same goes for the computer-generated “variants” being used to keep the vax bandwagon rolling.
Shades of the HIV/AIDS scam. Throw a blanket over a a bunch of common medical sympoms/conditions, say it’s a new disease caued by a new virus and give both a name. Easy peasy.
The COVID “pandemic” has made a barely discernable a blip on all cause mortality charts. Yet the mass psychosis generated threatens to deliver us completely into the unscrulous hands of the criminal pharmaceutical cartel and political puppets pushing the nefarious Great Reset agenda.
We don’t need more booster shots in our pin-cushion arms. But some of us clearly DO need with a smart kick up the backside to wake us up to what the shamdemic is really all about.
The man from NZ definitely had too many….10 in a day, wonder how he’s fairing.
I would have thought repeated injections into the same area would produce noticeable bruising / swelling which makes me think – is the story real?
If done rapidly enough the immune reaction (swelling) wouldn’t have had time to start.
“the man who allegedly got up to 10 Covid-19 vaccine shots”
There are so many conditionals in this it stinks. Presumably he had to travel to 10 different sites, wait in queues, etc, etc. Could it be done in one day as stated? I have no idea. I do find it difficult to see it going ahead without incident. What about the 10 so-called Johns who paid him? They supposedly commissioned the fraud and would be equally guilty.
“is the story real?”
Crossed my mind as-well, considering how some of the articles are phrased:
“A MAN has had 10 coronavirus inoculations in one day as part of an apparent anti-vax ploy.” – Express
It does have the odour of a propaganda piece.
His risks were of massively increased likelihood of clot-related conditions and myocarditis. Also there’s a risk of autoimmune conditions after a certain amount of time (maybe 6 months).
The repeated challenge of the immune system with more doses just after recovery from earlier doses will have a different impact on the immune system.
Ie, his immune system will have responded to a single ‘terrible infection’ which then goes away — the immune system thinks its response is ‘successful’. Repeated doses are like having continuous reinfection — the immune system will think its response is ‘unsuccessful’ and will massively enhance its response after each challenge to try to deal with the situation.
I’d suggest that the consequence of 3x doses at 3 month intervals would be worse than 3x the dose given at once.
Can you have too many vaccines?
Yes if the one designated for your arm comes from one of the bad batches Kate has been posting about courtesy of information passed on by Mike Yeadon
Can the author provide evidence (not just circumstantial) that he “caught” covid (twice), when germ theory hasn’t been proven?
It’s a serious question. And how do we know that the symptoms people are experiencing are a disease called covid when the virus hasn’t been isolated and the tests used to detect it are fundamentally flawed?
No it’s NOT a serious question.
Anyone who states “the virus hasn’t been isolated” doesn’t understand modern virology.
I suspect many virologists don’t understand so-called viruses
So why did a Canadian province dismantle all its covid rules following a court case where the defendant in his defence when prosecuted for breach of the covid rules asserted that the virus hadn’t been isolated and asked for proof of such. The judge agreed with his request adjourned the case and when they returned to court, prosecutors had to admit there was no evidence the virus had been isolated and the case against the defendant was dismissed. Following the precedent set by the case the Canadian province had no justification for continuing with the legislation enshrining the covid rules.
They didn’t. https://leadstories.com/hoax-alert/2021/08/fact-check-alberta-man-did-not-prove-covid-19-is-a-hoax.html
No.
It might be that the first infection wasn’t covid. It had the hallmarks of a very mild case of covid but I can’t be sure.
The later infection was confirmed with positive tests. (I note that these might be false positives, but that’s all we’ve got to go on at the moment).
Thank you for your reply. I’m just concerned that the vast majority of people take it as read that “covid” is this specific disease when so little is truly known about what “it” is, and how (or if) it is transmitted. I don’t think we are at a point when anyone can say they definitely caught covid from person B.
An interesting article and a point that I have pondered myself many times. It was obvious from the start that vaccinating everyone will put selective pressure on the virus to develop escape from the generated antibodies. Even the sellout scientists were suggesting that only the at risk should be vaccinated but now we have bloody everyone vaccinated the times with a vaccine that is 40 fold less effective.
Most people will have no idea that forty fold means that this means if it was 100% effective against the original strain it is now 2.5% effective so to get the same effectiveness you’d need 40* the antibody level!!!
So many fundamental contradictions and uncertainties or unknowns in “the science” on all this. Can you catch covid again, or can’t you, and what does it mean if you do? Do viruses “do waves” or don’t they? Are “variants” new diseases or the same one, for these purposes? Do the “vaccines” help or don’t they?
For me, the overwhelming concern is that I just do not regard this disease as sufficiently dangerous to warrant significant precautions beyond what would be appropriate for a nasty flu (except perhaps for a tiny minority of people with particular vulnerability), or incurring any significant costs in addressing it.
Accordingly, fundamentally the main problem is the involvement of government, which imposes such costs upon me willy nilly, and makes it basically impossible for me to ignore the panickers and get on with my life with fellow sensible folk without being dragged down to their fear-filled level of existence.
Interesting piece, thanks.
Says it all really.
In the face of uncertainty it’s unwise to double down. Do you really want Godzilla (Covid) and King Kong (Vaccine) battling it out in your body?
The best course of action in many situations is to do nothing.
What is the impact of repeated doses of the vaccine on adverse events probabilities? Is it additive, multiplicative or exponential?
Pfisser will be happy to answer that question in about 5 years, after it’s finished its studies on the largest trial ever.
Wasn’t their data just locked away for 75 years recently?
It’s not been locked away as such. As I understand it, the FDA takes its work very, very seriously and can only release 500 pages a month, as it has to review them first. As there are over 300,000 pages (more have been added, that’s when it went form 50 to 75 years) for the FDA to go over with a fine-tooth comb, it will take the FDA many years to do this properly (that, in any event, is the argument of the FDA).
Too bad it didn’t show the same diligence when going through the same number of pages within a 100 days, after which it allowed the use of this sludge.
The Pfisser trial data is supposed to be published in 2023 I think. Considering the question marks surrounding the data Pfisser has released so far, as raised, inter alia, by the BMJ’s Peter Doshi, the data they do release will probably be meaningless.
I thought the control group had all been offered/given the vaxx now, so the trial is now useless
I meant the on-going trial of the hundreds of millions of people currently getting their 3rd and soon their 4th poke
Some risks will reduce while others increase.
If you didn’t have an extreme reaction immediately after vaccination the first time, you probably have lower chance than the average person of having a severe reaction the second time.
This raises the question of what constitutes an adverse event. If you have three doses of a vaccine and this causes imprinting such that your immune system mounts a less robust response against a variant, resulting in you getting a severe infection – is that an adverse event?
Intervals will also be important – a constantly stressed immune system might be more likely to result in autoimmune disorders. Given more time to recover between doses, this effect might not be seen in the same way – allowing immunity to wane might be a good thing depending on the situation.
So a bit of a non-answer but I think the most honest answer is “it depends”.
Short term side effects should increase (immune system sensitisation). It would be helpful if the vaccine surveillance systems (Yellow Card) would report by dose, but they don’t (in the UK at least).
The Medium- and longer-term side effects are unknown at present. I guess we’ll find out eventually.
Very clear and informative article – thanks.
What you actually mean is that you had a cold and a positive pcr test. Why are you helping to prolong this farce by getting tested?
IMO it is those insisting on testing all the time that cause the problems. Getting tested on onset of symptoms is’t the problem. In my case I have vulnerable elderly to consider and I’m content to curtail my activities if there’s a chance that I might spread covid to them (they’re vaccinated but I have no confidence that it offers them any significant protection).
Why do you need to test if you have symptoms? If you test negative are you still going to visit them? Do you not think something other than covid might be able kill them too?
Also did you do that in all the previous years of your life? No, of course not. (hopefully) You just took the sensible option not to visit vulnerable people while having a cold.
You’re just prolonging the shitshow if you insist on playing their stupid games.
You are considered to have life long immunity to tetanus after 5 doses. Only if you have a tetanus prone wound would prophylactic tetanus be given. It should be noted that the prophylactic tetanus vaccination is usually Revaxis which is a triple vaccination against tetanus, polio and diphtheria.
Measles remains active in the body, which is why I still had antibodies some 50 years after the acute infection.
The virus responsible for shingles, like it’s cousins do in other cells, remains in a latent state in neurons after chicken pox, until it switches to the active lytic state when it presents as shingles. Shingles vaccine is routinely offered to the over 75’s.
With regards to TB, I had the heaf test followed by the BCG when I was 14. The BCG is no longer administered routinely as it is less than 50% effective, it is now only administered to those at high risk. Typically this would be the families in certain ethnic groups and healthcare workers.
Great article. It also highlights that we have even more unanswered questions now, than we did a year ago. A couple that I can think of related to this article..
How accurate and reliable are T cell tests?
If reasonable accurate in predicting strong immunity, then why weren’t these made available to the public, rather than through private clinics?
If accurate and the known risks of mass vaccination were accounted for, then why wasn’t everybody T cell tested before vaccination?
From a government’s perspective, they probably thought it was quicker and easier just to get everyone vaxxed. When they first said benefits outweighed risks, this was looking at simple numbers – x number saved from corona death compared to x number dying or injured by vaxx. Simple numbers, not taking account of age or health status, those making the decision didn’t care about that, just the headline numbers they could throw out.
I also suspect Pfisser’s marketing department has been advising government’s all along on how to proceed, providing press releases, providing data and arguments, etc.
I wrote the attached letter to the Health Minister of Northern Ireland the other day. He hasn’t bothered to respond, I did say it was urgent, so I suppose I have to go public with it. I proudly declare my transvax status, and will not be minimised, discriminated against, victimised or excluded.
https://gab.com/boomerbloke/posts/107457128120261269
So Many Unexplained Heart https://s.w.org/images/core/emoji/13.1.0/svg/2764.svg Coincidences… – YouTube
Sports persons and children.
“vaccines are given on medical advice (even those given for travel, etc.)”
The last time I had a vaccination was for foreign travel. The nurse asked me where I was going, and then got out a newspaper cutting from The Sunday Times to work out what vaccinations I needed. I don’t know what she was trying to prove, but it didn’t give me a warm feeling. Maybe it was a precursor to the future of epidemiological decision making.
I haven’t had the Covid vaccine. Not due to anything I read in The Sunday Times, but based on the old-fashioned method of risk/benefit analysis.
Never had a single vaccination in nearly sixty years (somehow dodged the school vaxes), never been to hospital for any reason bar once (minor ailment, that cured itself because I got fed-up being messed around by the NHS, & never went back) Never get sick, rarely get infections (had flu once in mid 30s). Feel fine. Have no doctor not registered with a GP. Never had covid!
V. few vacs. since school. Almost certainly I’ll refuse all from now on, having woken up to the scam.
Dr. Malcolm Kendrick’s book ‘Doctoring Data’ is an essential read if you want to preserve your own health as long as possible. As a default, stay away from the NHS.
Vernon Coleman says similar. I’m not quoting him directly but he says most illnesses or ill health is caused by the actions of doctors. Iatrogenic illness.
No wonder you have enjoyed such good health – long may it continue.
I’m of similar mind – it is my intention to stay away from doctors, espec the NHS, for as much as humanly possible!!
Lyons-Weiler, J., Thomas, P., 2020. Relative incidence of office visits and cumulative rates of billed diagnoses along the axis of vaccination. Int. J. Environ. Res. Public Health 17, 8674.
We performed a retrospective analysis spanning ten years of pediatric practice focused on patients with variable vaccination born into a practice, presenting a unique opportunity to study the effects of variable vaccination on outcomes. The average total incidence of billed office visits per outcome related to the outcomes were compared across groups (Relative Incidence of Office Visit (RIOV)). … Unvaccinated children in the practice are not unhealthier than the vaccinated and indeed the overall results
mayindicate that the unvaccinated pediatric patients in this practice are healthier overall than the vaccinated.Had COVID in November just gone. I remember having proper flu (not just a cough and cold) when I was 7 and again in my earlier teens. Both times wiped me out. To me, COVID felt almost identical however without the dizziness or eye ache that I had with the flu. Point being, other the last two, most of the symptoms we pretty much identical. I’d add not a reason to lock a country down or suggest mandates. Just try your best to do what you can for the most vulnerable where possible.
the booster lifts your antibody levels to 100x that seen from natural infection?!
that not ringing alarm bells for anyone?
I do think an article that concludes that natural infection is better than vaccine induced is oddly served by starting by claiming reinfection though! Did you get your T cells or antibodies checked out before getting reinfected? How can you be so certain it was the same illness? Chinese aircrew can carry other viruses than just COVID, I’m sure.
Nobody caught it twice, they had a cold/flu and a positive test.
Early on there was a Dr. practice in the US gene tested all 3000 +ive samples they’d collected, all were either flu A or flu B, non were covid.
Don’t forget to have your booster shot before we lock you down again. It takes a special kind of stupid to comply.
“It is important to note that the antibodies haven’t waned – they’re still there, only they’re now less effective at neutralising Omicron.”
The decline in Israeli vaccine effectiveness happened long before Omicron emerged though. And given that Delta originated in India at a time when under 10% of the population was vaccinated, it’s hard to imagine that vaccine escape related evolutionary pressures caused that particular variant.
But with ONS estimating that 90% plus of the British population currently have antibodies, it is clear that some antibodies are not providing the required protection.
And isn’t the presence of antibodies which fail to neutralize the virus the very definition of antibody-dependent enhancement?
As someone posted few days back WEF reported on the emergence of B.1.1.529, or later known as the variant of concern omicron back in July 2021.
https://web.archive.org/web/20211126173158/https://www.weforum.org/agenda/2021/07/how-scientists-detect-new-covid-19-variants/
Seems implausible to me that this necessarily originated (same for Delta) where they say nor hasn’t been swishing around the planet in far more prevalence than noted.
As I say repeatedly, the lower atmosphere has more virus than there are stars in the universe. The idea that there is a certain geographical point associated with a variant is nonsense, as is the idea you need an aircraft to transport it.
What seems to have happened is that whoever is calling the shots of this shit show decided that calling this cold ‘omicron’ would be a good way to support more social panic and disruption and of course support a flagging mRNA ‘vaccine’ campaign,.
Henry2 apologies if all this has already been discussed here, your post has only just alerted to me to this clear evidence of Management and Manipulation on a global basis. Surely no-one can doubt this anymore?
I should have spent longer testing this, as I usually do. The article supposedly
dated 12 July has a link which takes you to an article dated 26 November. Now I know wayback records history but I didn’t realise it employed the TARDIS. On the same footing I just can’t help putting an R in Davos, showing my age I suppose when that show was worth watching.
You’d enjoy “Pseudo-Pandemic” by Iain Davis if you want to see the bigger control picture, you can get a free copy on his blog https://in-this-together.com
Yes read that. Iain has produced some excellent pieces over the last 18 months or so.
Amanuensis obviously knows much more than I do about vaccines, but it has been very obvious to me for ages that “vaccinating” the non-vulnerable population with a leaky and variant-specific vaccine can only serve to make the situation worse and prolong the pandemic. One is therefore forced to only two possible conclusions: That the government is really, really stupid, or they actually want the pandemic to go on for much longer than necessary. Either way, we have to find a way to get this message out to the mass of people who at this point are completely misinformed and, in my experience, extremely resistant to any and all attempts to enlighten them. This pandemic will not end until vaccination stops and we gain real natural herd immunity. I have tried to tell people. They don’t want to listen. It’s incredibly frustrating.
It used to be that vaccinating anyone who was ill or malnourished at the time of vaccination was medical malpractice. You didn’t challenge the immune system when the immune system was already challenged. But, quite amazingly, that has gone entirely out the window in recent years.
The Pfizer clinical trial participants were healthy people. Look for “Exclusion Criteria” at these 2 links:
https://cdn.pfizer.com/pfizercom/2020-11/C4591001_Clinical_Protocol_Nov2020.pdf#page31
https://clinicaltrials.gov/ct2/show/NCT04368728
But, then, who did they turn around and vaccinate first??! All the people who were excluded from the clinical trial, all of the so-called ‘vulnerable’!
It’s been extraordinary to watch medicine being turned on its head for the last 2 years.
And where are all the doctors (like my Dad) and all the mothers (like my own) who knew how to get us through any illness with simple stuff like gargling with hot salt water or lying with your head over a big glass jar vaporizer? Steam from a pot of water simmering on the stove and an ionizer in my bedroom have been my go-to things whenever I felt the least bit dodgy the last 2 years, and I’ve not been able to justify lying in bed with a book for more than 2 days (once) and 8 hours (on another occasion). Actually, that 2nd occasion was over the summer and I sat outside all day with my book, got some sun, and breathed fresh air into my lungs. By 4 in the afternoon, I felt fine again. And I’ve done my best not to follow any of the rules during this whole thing, going anywhere and everywhere and not wearing a mask anytime I could get away with it. But, I am also not one to reach for any pharmaceutical, if I can help it. Nothing that will suppress my own immune system.
Thanks for pointing this out reads.
“It used to be that vaccinating anyone who was ill or malnourished at the time of vaccination was medical malpractice. You didn’t challenge the immune system when the immune system was already challenged”
My ill mother who has just had a bout of something – flu? covid? – despite being double jabbed is “desperate” to have her booster and gets very cross when I point out that she is currently too unwell to risk it.
Vaccines are snake oil, highly profitable for pharma (repeatedly dosing healthy people is a business model dream for them) but they cause immense harm to their victims.
I believe I had Covid in mid-January 2020.
I had been to a dinner party with some Chinese friends who’d got back from Shenzhen not long before, and weren’t feeling too good.
A few days later I had a high fever and a very bad cough.
Total lack of smell and taste – I usually smoke Marlborough Reds but couldn’t smell them or taste them!
Headaches, muscle aches, fatigue, blurry vision, sweats, etc.
The fevers lasted a few days, the cough took months and I felt very tired until March.
At one point in late January I phoned my doctor and the receptionist said “she’s off ill – she’s got that nasty chest bug that’s going round, everyone’s getting it”!
So I think that the first wave was dramatically under reported, and was well into its peak by the time we locked down – it’s just that our testing was dire and we didn’t know.
CCTV evidence of the outrageous act of over vaxxing and its consequences has finally been released
https://www.youtube.com/watch?v=S5A0fhme7ys&t=245s
Nothing like an unsubstantiated statement to kick off the article. Did you use a fake unvalidated piece of shit worthless test to persuade you to morph fantasy into fact.
Its a miracle. Definitely not one of thousands of other reasons you could have had these symptoms. Defo the rona. Tunnel vision brainwashing at work.
Get your hamzat suits out people, Chinese pilots who literally shit Covid 247, all over the world.
This makes sense. Havent we already got enough of this breed of person polluting the collective consciousness about viruses that dont exist and tests that are based on fraud. Cant these people actually do any critical analysis.
Hows about DS actually applies some real scepticism. If people are allowed to write this bullcrap above the line, surely you can balance it with alternative opinions which actually use real science, not Gates billions science – ie fraud.
This is comedy right.
Why not cover the fact that this constant relentless unnatural unnecessary and completely nonsensical stimulation of the immune system is likely to cause an epidemic of immune system degradation. Why carry on publishing bullshit like this which tricks people into believing these jabs actually serve a purpose. He admits as such when stating how they are just manufacturing the Wuhan spike protein. They are manufacturing a toxic protein, found nowhere in nature, designed in a computer. Its fucking Frankenscience. But all you do is churn out one article after the next claiming how great this is. What the hell is wrong with you people.
The reality is simple. The jabs mess around with the immune system and the manufacturers are a bunch of criminals. If you want criminals tinkering with your one and only immune system, take the jab, believe in crap like this article.
No mention of the fact that Bovid is a nothing burger and that any measures taken in its name are bogus and based no fraudulent made up “science”.
Let’s hope the Simpsons got it all wrong. Let’s hope we all escape the needle.
https://www.youtube.com/watch?v=oqdMLWTHER4
Explain this
“And as we all know, the double-jabbed are suffering from negative vaccine efficiency and are thus more likely to catch Covid than anyone else (somewhere between –50%, –100% or even –150%). The only people who don’t seem to know this are politicians…”
None of which chimes with the references you give.
I call bollocks – but perhaps the enlightened can explain.
https://www.ons.gov.uk/peoplepopulationandcommunity/healthandsocialcare/conditionsanddiseases/articles/coronaviruscovid19latestinsights/vaccines#vaccine-effectiveness
Evidence
Our healthcare system is about to experience a tsunami! Potential side effects of jabs include chronic inflammation, because the vaccine continuously stimulates the immune system to produce antibodies. Other concerns include the possible integration of plasmid DNA into the body’s host genome, resulting in mutations, problems with DNA replication, triggering of autoimmune responses, and activation of cancer-causing genes. Alternative COVID cures EXIST. Ivermectin is one of them. While Ivermectin is very effective curing COVID symptoms, it has also been shown to eliminate certain cancers. Do not get the poison jab. Get your Ivermectin today while you still can! https://ivmpharmacy.com
The C19 jabs are not conventional vaccines, so shame on you Daily Sceptic for keeping silent about this scientific fact!!!
It almost looks like the Daily Sceptic only exists to keep people distracted from what is really going on, not only regarding the C19 fraud, but from what’s happening in the world… and why!!!
Well written article and highlights the muddled approach of recurrent mRNA vaccination against a Coronavirus which is mutating. The conclusion of the article could well be that boosters in those who have had SARS-Cov-2 infection is both experimental and has risk of adverse reaction with no obvious benefit.
This would not have passed any ethics committee.
Also the Pfizer study on children specifically excluded this group—“ In addition, in the phase 1 study, children with a previous clinical or virologic Covid-19 diagnosis were excluded. “
Your article highlights that the vaccination policy is not based on a risk vs benefit for the patients but risk vs benefit for politicians consideration of how they feel their population would view them.
These pages have indicated that many voices are desperately concerned about Government SAGE etc
Should we organise a Skeptic SAGE? Toby over to you.
My school physics teacher used to say, “Science is 5% basic principles 95% common sense”. This article exemplifies it. It’s a sad indictment on human behaviour with the COVID scamdemic that the 95% gives so much scope for malfeasance, corruption and criminality – and that the majority of the population are so easily led and don’t think for themselves.
Well there you have it. A booster 100% ineffective that is being injected into humans with god only knows what type ofadverse events and deaths will follow. Not one study done to recommend these boosters. Dangerous? Unheard of in the medical world. And yet doctors pushing the untested treatment like there is no tomorrow. My faith in gp’s is zero. My GP got the hell out of our practice sept 2020. He saw the writing on the wall. Now two others are gone. I think I know why.
”…I was rather cross about catching Covid, because it does lead to some inconveniences..”
So – why did you get tested then? Surely the result of finding you had ‘covid’ was EXACTLY what it would have been (in saner times) had you contracted flu – go to bed, keep away from other people, and suffer until you felt better.
This obsession with testing is what is driving this madness.
(Good article though. Thanks.)
Thank you Amanuensis.
Your observations and this article provide plenty for us all to think about. Everything is so clearly and logically described and explained.
The scientists who have drawn up (and are so sure that) their Covid vaccination strategy is obviously the right approach are compelled to provide an adequate response to your article. Absolutely compelled to respond in the interests of public safety. They cannot be allowed to ignore the contents of this extremely important article.