
How many COVID-19 vaccine related serious adverse events are acceptable? In part 1 of this two-part article, we tried to answer this question by reference to the population and the ‘collectivist’s’ view. But when it comes to medical treatment it is the individual that is paramount and not society. Some of the greatest medical abuses of history have been justified through the ‘benefit to society’ argument and this is why ethical frameworks in medicine focus on the individual patient and the benefit and risk to him or her, and him or her alone.
There may be incidental benefits to society, but these are additional effects of treatment and not its purpose, which must be to benefit the patient. This latter point is made in the ‘Green Book’ in the opening sentences from the chapter on informed consent for vaccination (Chapter 2).
It is a legal and ethical principle that valid consent must be obtained before starting personal care, treatment or investigations. This reflects the rights of individuals to decide what happens to their own bodies and consent is a fundamental principle of good healthcare and professional practice. (our emphasis)
No mention of broader societal consideration here, but a very clear statement as to whose rights are important. So, in thinking about what is an acceptable level of serious adverse events (SAEs) from the COVID-19 vaccinations, we need to bring it down to the individual level and be able to describe the benefit and risk to the person receiving the vaccination. If there are genuine benefits to the individual, then these may well produce population level benefits, but ultimately it is the individual who needs to decide on whether the treatment will be of benefit to him or her.
A point that the Green Book goes on to make when discussing what valid consent means:
For consent to immunisation to be valid, it must be given freely, voluntarily and without coercion by an appropriately informed person who has the mental capacity to consent to the administration of the vaccines in question. (our emphasis)
So, what does “appropriately informed” mean when it comes to the benefits and risks of the COVID-19 vaccinations to the individual?
The 90% ‘lie’
To be appropriately informed first means understanding how serious COVID-19 is to the person who is going to potentially receive the vaccination. We can get a sense of this from estimates of the SARS-CoV-2 infection fatality rate (IFR). A relatively recent paper by Pezzullo et al. gives just such estimates of the IFRs for different age groups based on a meta-analysis of 31 pre-vaccination studies. These are summarised in Table 1 and give us our baseline ‘seriousness’ by which to measure the individual effectiveness of the COVID-19 vaccines in preventing death. Obviously, these are median figures and so if you are someone who has a pre-existing condition that raises your risk above this level, but this speaks to the need to understand your own risk (and benefit) if you are to consent to treatment.
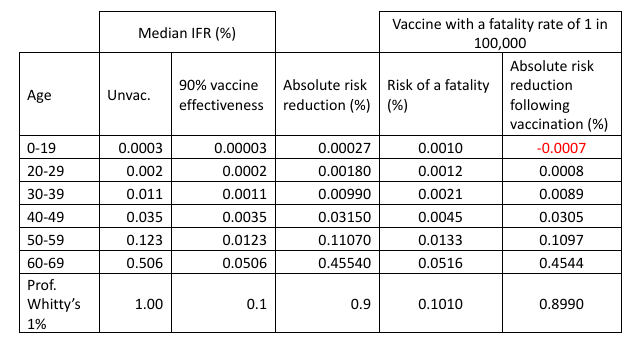
Two things leap out from this analysis. First, the ‘ageist’ nature of COVID-19; for those under the age of 19, the likelihood of dying from SARS-CoV-2 infection is three in a million, whilst for those in the 60-69 age group it is 1 in 200. Second, none of these IFRs comes close to the 1% that Professor Chris Whitty used as his theoretical example of a disease with a low mortality rate for which he said:
For a disease with a low (for the sake of argument 1%) mortality a vaccine has to be very safe so the safety studies can’t be shortcut. So important for the long run.
Having established how serious COVID-19 is to oneself, the next question becomes what benefits do the COVID-19 vaccinations offer with respect to the likelihood of dying from SARS-CoV-2 infection? The ONS figures on vaccine effectiveness suggest that the COVID-19 vaccines have an initial relative effectiveness of 90% in preventing COVID-19 related deaths and this ‘90% effective’ benefit is routinely used as the justification for getting vaccinated. But, putting aside the question as to whether this figure is accurate or not, what does ‘90% effective’ actually mean? Well, for the 0-19 year-olds this means we changed their risk of dying from SARS-CoV-2 infection from three in a million to three in 10 million, which is indeed a relative risk reduction of 90%, but is an absolute reduction in risk of 0.00027% (Table 1). Whilst for the 60-69 year olds the risk of dying of COVID-19 has gone from 1 in 200 to 1 in 2,000, an absolute reduction in risk of 0.45%. The benefit to the 60-69 year-olds is about 1,700 times greater than to the 0-19 year old, despite the vaccine being (for the sake of argument) ‘90% effective’ in both groups of people. For a disease with a ‘low mortality’ IFR of 1% the vaccine reduces the risk to 0.1%, an absolute reduction of 0.9%.
So, in terms of being ‘appropriately informed’, being told that the vaccine reduces your risk of dying “by 90%” is the great statistical ‘lie’, because it potentially leads to a complete misunderstanding of the real benefit to you as an individual. For example, if you are a healthy 20-something year-old then a ‘90% reduction in risk of dying from COVID-19’ sounds like a great benefit from vaccination because it tacitly suggests that you are at significant risk from COVID-19 itself. That is until you realise that a 90% reduction in risk really means reducing your risk of dying from COVID-19 from 1 in 50,000 to 1 in 500,000, an absolute risk reduction in the IFR of 0.0018%. A trivial gain in overall risk reduction following a SARS-CoV-2 infection.
So much for the benefits, what about the risks – what is the risk of suffering a fatality following a COVID-19 vaccination? As discussed in part 1, estimates of these figures vary from 12 in a million for the mRNA vaccines to potentially as high as 1 in 5,300 for the AZ vaccine. If we focus on the mRNA vaccines (not least because it appears that the AstraZeneca vaccine is being quietly dropped from use) and for simplicity’s sake assume that the risk of a vaccine induced fatality is 1 in 100,000 per dose for everyone receiving the jab (10 in a million), then what does this mean for an individual’s risk of dying if vaccinated against COVID-19? Now we need to consider not just the residual chance of dying from COVID-19 if vaccinated (assuming 90% effectiveness) but the added risk of dying from vaccination itself which means simply adding the two risks together to get the overall risk of dying (Table 1). We can then go on to work out what the absolute risk reduction is if we take this rate of vaccine fatality into account. Doing this, it is immediately apparent that with a 1 in 100,000 level of vaccine fatality, vaccinating children and the under-19s actually increases their likelihood of dying by about three-fold (from three in a million if unvaccinated to 10 in a million if vaccinated) and for those in their 20s, this level of vaccine fatality halves any gain from COVID-19 vaccination (from 0.0018% to 0.0009%), because the absolute risk reduction from even a ‘90% effective’ vaccine is so modest that it is impacted by the 1 in 100,000 chance of a vaccine induced fatality. For those more at risk from COVID-19, this level of vaccine fatality does not substantially alter the overall benefit of vaccination, although the absolute reductions in risk remain modest.
The benefits to an individual of having a COVID-19 vaccination are not just about reducing one’s risk of death, but also avoiding potentially serious illness. A full-blown bout of COVID-19 is a deeply unpleasant experience, which might end up in a trip to hospital and so having a jab to avoid serious illness is also of genuine medical benefit. But, as is obvious from the definition of an SAE (see part 1), vaccine-induced injuries and SAEs can also be truly awful, and even life-altering, without necessarily being fatal. More people will benefit from any positive impact of the vaccine on serious disease, but similarly more people will also suffer non-fatal SAEs and so, the real balance of benefit/risk comes from understanding these broader impacts of the vaccination. As discussed in part 1, effectively quantifying such benefits and risks outside of a clinical trial is very difficult as we’re depending on spontaneous reporting and there will be lots of assumptions and biases in the analyses. In the end, we can only really focus on ‘countable’ things like deaths and hospitalisations but the vast majority of potential benefit (reduction in disease severity due to COVID-19 vaccination) and injury (SAEs and AEs that are still significant and potentially life altering) will not be reported and so will be invisible to the assessment of benefit-risk.
Multiple doses
But there’s a further consideration we need to take into account when trying to be ‘appropriately informed’ about the benefit and risk and that is that a COVID-19 vaccination is not a single jab but multiple jabs. This is necessary to achieve (and maintain) the ‘90% effectiveness’ of the vaccination, but each dose carries the risk of an SAE and so to really understand the risk means figuring in the impact of needing to have several injections, in other words what is the overall risk for the vaccination course?
Let’s assume that most SAEs are not fatalities and that the SAE rate associated with the mRNA vaccinations is 10 times higher than the potential fatality rate i.e., 1 in 10,000 per dose (which would still be classified as very rare events). What does this mean if you were to have a course of three jabs i.e., primary dose and then two boosters? To calculate the risk across all three doses, we need to work out how likely you are to not have a vaccine induced SAE for this course of treatment. For each dose the odds of not having an SAE are 9,999 in 10,000 or 0.9999. For all three doses, the odds of not having an SAE are therefore 0.9999 × 0.9999 × 0.9999 = 0.9997. Which means the risk of a vaccine SAE over the three-dose treatment course is three in 10,000 (1–0.9997 = 0.0003) or about 1 in 3,300. The risk over all three doses is substantially greater than from an individual dose, although each dose carries the same 1 in 10,000 risk.
In contrast, the benefit does not increase with multiple doses. In fact multiple doses are required if we are to receive the ‘90% effective’ benefit, assuming that it is actually this great in the first place (see for example these two discussions on vaccine effectiveness). Even assuming the original vaccine effectiveness was 90%, because the current COVID-19 vaccinations are against variants that are different to those endemic in the population now, the effectiveness of subsequent ‘boosters’ actually drops off, meaning that the assessment of benefit and risk must also change for the new variants compared to the original variants. Obviously, anything less than this ‘90% effective’ figure proportionally reduces the benefits discussed here and the consequent balance of benefit and risk.
Overall, understanding the benefit-risk ratio of any treatment can be a fluid thing, especially for an evolving infectious disease like COVID-19, and so it needs to be constantly reviewed and refined. As a result, it turns out that being ‘appropriately informed’ about your individual benefit-risk for the COVID-19 vaccinations is extremely difficult, despite the billions of doses that have been given to people around the globe.
Final thoughts
The issue is not that the COVID-19 vaccines have SAEs, all vaccines carry some risk of such adverse drug reactions. The issue is that these vaccines have been used in an indiscriminate way across entire populations, with individuals at very low risk from the disease being encouraged, and even coerced, into getting vaccinated. As we discussed in part 1, this kind of wholesale use of these new vaccines is almost the logical conclusion of the ‘collectivist’ view of vaccine benefit against COVID-19 once we allow perceived broader societal benefits to become part of the calculation. Also, we must not forget that unlike a treatment given to someone who is ill, vaccinations are given to otherwise healthy people and so, if these vaccines are going to be ‘safe and effective’ for everyone, then they need to be not just ‘very safe’ but extraordinarily safe. This is for the simple reason that for most healthy individuals, COVID-19 is not a disease that has major risks and so the benefits from the vaccination are consequently small (vanishingly small in some cases) and so to try and make the benefit-risk equation balance for many people means having levels of vaccine safety that are almost beyond the bounds of pharmaceutical possibility. Of course, if we decide to count the potential benefits to society, we can skew these calculations, but even here these societal benefits need to be pretty large and tangible if they are to balance out even rare levels of vaccine-related SAEs.
As Professor Whitty noted in his WhatsApp message to Matt Hancock, with a disease with such low mortality “safety studies cannot be shortcut”. Yet, this is precisely what happened because one cannot do a two-year safety study or long-term follow-ups in six months. As discussed in part 1, trying to get a handle on vaccine safety post-marketing is challenging, especially in identifying and quantifying very rare safety issues. Worryingly though, rather than potentially being very rare events (occurring less frequently than 1 in 10,000 doses), reanalysis of trial data suggests that the risk of an SAE from the COVID-19 vaccines could be as high as 1 in 800 per dose, although this number is subject to some dispute. But if this 1 in 800 per dose figure is accurate then because, as we discussed above, the vaccinations require multiple doses the risk over a course of injections will be even higher, approaching a 1 in 250 chance of having an SAE over a course of three doses. In fact, in a world where every person over the age of 50 has a COVID-19 ‘booster’ every winter, if this rate of SAEs per dose was to remain unchanged, then the likelihood of having an SAE before your 80th birthday would be about 1 in 25. With these rates of SAEs, it is hard to see how it would be ethical to justify vaccinating all but the most vulnerable individuals.
Having a drug-related SAE is a bit like being involved in a major car crash in that the likelihood of this happening might be low but the consequence to the individual can be catastrophic. We need to bear this in mind when talking about SAEs and vaccine injury from the COVID-19 vaccinations: just because such events are rare or a ‘statistical tail-effect’ they are still real people, experiencing real life-changing events. Worrying about the safety of the COVID-19 vaccines doesn’t make one an ‘anti-vaxxer’ any more than worrying about the safety of cough medicines or drugs makes one an ‘anti-piller’. It recognises that people suffering from a vaccine-related SAE have as much right to a healthy life as those unfortunate enough to catch serious COVID-19. Unfortunately, ignoring safety signals does not make them go away.
How many COVID-19 vaccine induced SAEs are acceptable? Difficult to say but just because it is an awkward question doesn’t mean we should stop asking it. Perhaps the more pertinent question for today is:
How may COVID-19 vaccine related serious adverse events would it take before we decided that these vaccines have a problem?
George and Mildred are pseudonyms of senior individuals working in the pharmaceutical industry.












To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
Israeli situation is discussed here.
https://www.rintrah.nl/suppression-of-the-innate-immune-system-the-main-cause-of-the-pandemic-of-the-fully-vaccinated/
We’re two months behind Israel.
Many thanks for posting that. It explains so much that is puzzling.
I thought of trying to summarize it, but no. It really does require reading in full. Just never get on the treadmill of these mRNA vaccines. (The Chinese may have got away with this, though the worry with their vaccines has always been ADE, so the jury is still out on that one.)
I think it’s rather telling – or rather, not telling – that we don’t distinguish between the experimental non-mRNA and the experimental mRNA pre-infection treatments when recording “vaccination” status along with critical care and deaths.
I’d love to see the breakdown in AZ versus Pfizer and Moderna.
This one I can corroborate – my sister-in-law, an ICU nurse, has reported empty, or nearly empty covid wards at the two hospitals she works at for several weeks. Given what most of us believe about the dangers of the ‘vaccines’ esp. OAS/ADE, wouldn’t we expect to see something more akin to Israel? How can we account for the difference? I’m baffled.
One difference would be that many-to-most UK citizens at high risk (i.e. the elderly) were dosed with Astra Zenica, the non-mRNA experimental treatment.
Apparently:
“Since more than half of ICU admissions have not been vaccinated, this suggests an intrinsically milder virus rather than just increased protection from vaccination.’”
According to the UKHSA there are around 5x more deaths in the vaccinated compared with the unvaccinated — now, that’s perhaps just because the vaccines are protecting them, but…
…Why aren’t these dying vaccinated people getting a bed in ICU? Are they dying before they get a chance to get admitted? Or maybe there’s a secret society of unvaccinated doctors turning the vaccinated away from ICU?
Or are these figures just really dodgy, as usual.
3 things spring to mind. Anecdotally, there seems to have been an upsurge in sudden deaths. These would appear to be predominantly among the vaccinated, so yes, dead before they get to ICU. Secondly, isn’t it possible that the treatment of patients may differ according to their vaccination status? If the unvaccinated are getting poorer treatment due to nhs staff bias, then maybe they’re more likely to deteriorate and need intensive care. Thirdly, I believe that ICNARC and UKHSA use different estimates for their unvaccinated population. ICNARC uses the ONS estimate, which likely underestimates how many people are unvaccinated, and therefore overestimates the proportion of unvaccinated that end up in ICU.
I have suspected for some time that treatment given in hospitals will differ according to jab status.
I’ve no proof, just a gut feeling as 20+ yrs experience of working with the medical profession means I am well aware of what some of them are capable of.
If everybody gets the same treatment why is one of the first questions about your jab status?
I agree. I can’t help but think there is something sinister, or at least very questionable, going on. A few weeks ago a relative (also a sceptic) told me he’d read an article in The Times which presented an anecdotal frontline report from an A&E doctor. In the report, reference was made (in passing) to having to identify the vaccine status of covid patients, as they were put in different areas “reflecting the need for different treatment”. What this meant in practice wasn’t explained.
The almost 5x was pure numbers, not proportion — in the last figures it was 5012 deaths with 2 or 3 doses, and 1177 unvaccinated.
I realised that. My comment about defining “unvaccinated “ denominators was just in response to your comment “or are these figures just really dodgy, as usual”. (If they can fudge something as basic as the uk population, what else will they fudge? Another one, clearly, is their definition of “unvaccinated”.) It wasn’t intended to explain the discrepancy per se. Perhaps I should have clarified at the time.
Yes these figures are definitely “dodgy”. I believe they don’t include admissions from care homes and have my suspicions that unvaccinated patients are rested much more regularly (and possibly at a higher cycle rate?) than the vaccinated. As you point out the vaccine shows completely different figures for deaths – around 80% jabbed. So the vaccine means that once hospitalised you are at a much higher risk of dying then? Or the figures are manipulated junk?
Spiegelhalter is a regime gatekeeper. Nothing he says can be taken at face value.
Israels problems may be related to the number who have been quadruple stabbed.
As the damage to the immune system is acknowledged to be cumulative, it may well be that the Israelis have many more over a threshold where their immune system can no longer cope?
This is just abuse of the term “vaccinated.”
Hospitalised but no injections – unvaccinated.
Hospitalised after one jab but exceeding the timeline for injection two = unvaccinated.
Hospitalised after two jabs, but not boosted to heaven, yet = unvaccinated.
I completely agree (see post). Add to this list “Unknown” which are also classed as “Unvaccinated”.
One can only suppose that this misinformation is being supported by doctors, just as they don’t report teenage heart attacks as adverse reactions (see Tommy Robinson’s Telegram posting yesterday – sorry, I can’t link to it) and continue to cash in on injecting while refusing to do their job of actually seeing patients.
The Australian tyranny is just a test run
https://www.conservativewoman.co.uk/the-australian-tyranny-is-just-a-test-run/
James Delingpole
Tuesday 8th February 2pm to 3pm
Yellow Boards By the Road
A329 junction London Road & Oak Avenue
Near Oakingham Belle pub
Wokingham RG40 1LH
Stand in the Park Sundays 10am make friends, ignore the madness & keep sane
Wokingham Howard Palmer Gardens Cockpit Path car park Sturges Rd RG40 2HD
Henley Mills Meadows (at the bandstand) Henley-on-Thames RG9 1DS
Telegram Group
http://t.me/astandintheparkbracknell
Delingpole’s article is superb – and the film is well worth watching (especially if they’ve sorted out the original volume problems)!
I think it is important that any time the term “Unvaccinated” is used it really needs to be in quotation marks since an unknown number of them have been vaccinated.
We need to show scorn and contempt for the way the term is used, as we should also for the term “Cases” and “Asymptomatic Infection”.
The German health and panic minister stated yesterday that Israel’s problems stem from too few elderly being vaxxed and boosted in comps with Europe.
As far as I can tell, that statement is completely fact free/a lie, it contradicts the statements from doctors there that 3/4 of the ICU patients are vaxxed and the general booster overload and lead there.
But even if it was true, it would then confirm that vaccinating people not at risk and younger ones was and is a misguided strategy and that any vaxx mandate for them, which he is now planning to introduce, is medically ridiculous.
Omicron seems to be having a much more significant impact on the population in both Israel and the USA.
Both of these countries used almost exclusively mRNA vaccines. The majority of adults in the UK were vaccinated with the Oxford Astra Zenica vaccine (at least the first two doses) Could it be that AZ is more effective at protecting from serious illness in the longer term than the mRNA vaccines?
It could be, yes. I’d note that while all the vaccines induce a pretty poor cellular immune response (but lots and lots of antibodies), AZ produced the highest amount of t-cell response (still poor, but higher than the others). We’ve little idea how any of the vaccines are modulating the innate immune response (there’s some papers saying that the mRNA vaccines at least have an impact on the innate immune system, but really we need much more data).
Alternatively, it could be a vaccine dose separation issue — in the UK we started vaccinating at the same time as Israel, but delayed the second dose by two months. This has put us two months behind Israel ever since.
It is called immune erosion. This is from the head of healthcare in Israel.
The Israelis have had 4 jabs. Their natural immunity has been more effectively suppressed (wrecked) than our population with a sizeable number who haven’t been jabbed, or have only had one or two.
Why “excluding Scotland”. Surely with vaxpässen and muzzle mandates still in force here, we must have reached zero by now? That’s what The Science demands, and reality must defer to it.
”One mystery is why Israel’s Omicron wave is proving a rougher ride in terms of ICU admissions and deaths compared to ours.”
Really? A ”mystery” is it? Not to a lot of us who’ve read about what jabs do to the immune system – and Israel has certainly done a lot of jabbing.
The Propaganda Loyal BBC & the Highly Trust worthy health & Prime Minister, with their Cameras & Photographers would have been all over this if they had a few patients. Lest not forget how much we spent on Nightingale Hospitals either!
Why is Israel’s situation as regards ‘COVID’ ICU numbers and deaths recently than here in the UK? Probably becuase:
1) They’ve used the Pfizer and Moderna vaccines throughout, which appear (in my view from reports) to cause immunity fatugue, i.e. their effectiveness wears off quicker and quicker and once it doesm the more vulnerable people’s immune systems are worse off.
They may be ‘dependent on the jabs’ so much that it could induce many auto-immune diseases, as some scientists and clinicians have speculated. Unfortunately, some many not know until years down the line, whereby it’s too late to make much of a difference.
The Oxford/AZ one did not seem to be anywhere near as ‘bad’ on that front, whilst lower initial immunity, it appears to last longer and not induce this immunity deficit so much/soon. Noticeably most oldies here got the AZ jab (my elderly parents did).
Whether this now changes in the coming months, as most of the booster jabs appear to be of the Pfizer/Moderna ones.
2) The has been a lower take up of jabs in the UK, especially in younger people, and also young children have not had them at all – yet.
Combine this and, in England (which makes up the majority of the UK population) lesser lockdown restrictions and more ignoring of those rules, the virus (especially since it ‘got milder’) has been far more extensively circulating in the below 50s population here, giving many more the better, longer-lasting natural immunity.
3) Israel rolled out the boosters quicker than we did, they are now on No. 4, but they rolled them out at a time of the year when they were least needed, and thus, IMHO, wasted before the aforementioned immune system problems kicked in just as the worst of winter illness was approaching.
It also means that the immune system problems are worsened because many have 2, not 1 booster and in quick succession.
What appears to be now coming out is that the effects of mRNA vaccines are still relatively unknown over the medium to longer term. To expect entire populations, inculding under 50s who in theory have decades of life to live, to have these jabs which are not fully tested despite them predominantly not being those seriously ill is an utter disgrace.
As more have said, any vaccines should have gone to just the most vulnerable, with them and everyone else using a holistic approach to both treatment and boosting the immune system by way of better diet, exercise/fresh air/sun, including vitmain D, zinc and a couple of other supplements, especially in colder less sunny months.
All the less vulnerable/younger people should then have just got on with their lives as before, shielding the vulnerable at the lowest level required without destroying what life they have left.
To show the Covid daily death figures are nonsense if the current trend continues we’ll shortly have fewer people seriously ill with Covid in ICU’s than die every day with Covid. A clear contradiction.
What “mystery” re Israel? The “vaccines” make many more susceptible to illness, as their immune systems get attacked by the snake oil. As per Mike Yeadon. mRNA mayhem is in the pipeline now…
Medical clinics and hospitals in USA are denying life-saving Ivermectin medicine even with court orders. Big Pharma doing all that they can to push the vaxx and inoculate us while effective and cheap COVID cures exist. There turns out to be censorship that we have never seen before for those who are looking for these treatments. We say over and over again that indepenedent researchers found Ivermectin safe and very effective for these Flu-Corona symptoms. Getting Ivermectin is easy https://ivmpharmacy.com