When did the coronavirus first appear and begin spreading? Did it emerge in December in the Huanan wet market, or did it leak from the Wuhan Institute of Virology in November, or was it intentionally released at the World Military Games in October? Was it spreading internationally during autumn 2019? Has it been around for years?
Here I’ll present evidence that the coronavirus appeared at some point in the second half of 2019 and was spreading globally during that autumn and winter.
There have been a number of studies that have gone back and tested stored samples for evidence of the coronavirus, either antibodies or viral RNA. One of the most intriguing is a study from Lombardy in northern Italy by measles researchers (Amendola et al.) who had spotted that Covid could cause a measles-like syndrome (though the evidence on this claim is not fully clear and a measles-like rash was not a widely publicised symptom of the disease). The researchers tested hundreds of stored samples taken during 2018-20 for both antibodies and viral RNA. Eleven of the samples were positive for viral RNA from August 2019 to February 2020, including one from September, five from October, one from November and two from December. Four of these were also positive for antibodies, including the earliest sample from September 12th 2019 (both IgG and IgM). A striking 25% of the samples from September to December were positive for viral RNA, which seems on the high side even considering these were samples from people visiting hospital with measles symptoms; the percentage positive then oddly dropped to 16.7% in January and February 2020. The positive samples were genetically sequenced to reveal mutation information, reducing the chances of them being false positives – though it should be noted that the positives were of partial sequences, not complete ones, so cross-reaction remains a possibility. In addition, none of the samples tested positive on a SARS-CoV-2 PCR test and the first to be positive on more than one RNA component – the first strong evidence of true infection – was from December 15th in Milan. Comparison was made with a control group of 100 samples from August 2018 to August 2019, none of which were positive on any RNA fragment, though 12 were positive for at least one antibody, a result which the researchers called “inconclusive”. Their results led them to estimate that the virus emerged around July 2019.
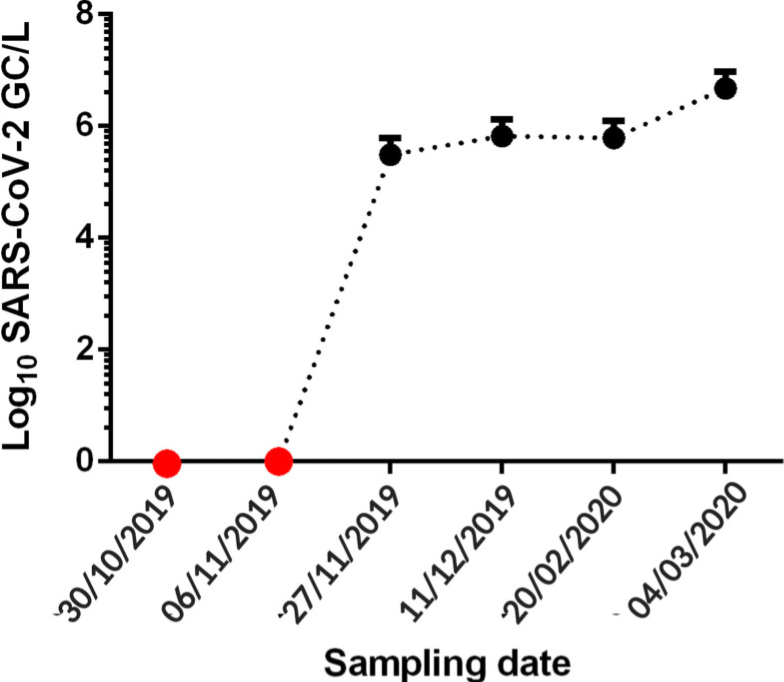
A separate study in northern Italy tested waste water from 2019 for viral RNA and found samples in Milan and Turin positive from December 18th, though negative prior to that, which is in contrast to the results of the first study – though in line with when the first strong positive turned up in Milan. The samples were again genetically sequenced, adding to their reliability.
A Brazilian sewage study found SARS-CoV-2 RNA in samples from late November and December 2019, but not in two earlier samples from October and early November. The samples were taken from one site in the southern Brazilian city of Florianópolis and were genetically sequenced for confirmation.
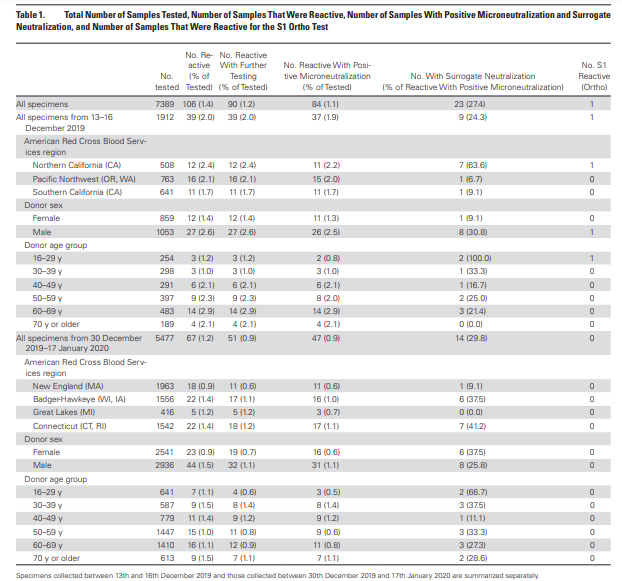
An antibody study of archived Red Cross blood conducted by the U.S. CDC found 39 antibody-positive serum samples collected December 13th-16th 2019 in California, Washington and Oregon. Overall, 2% of blood samples collected from these states on these dates tested positive for antibodies. The full results can be viewed in the table below. A 2% antibody prevalence in mid-December suggests significant community spread across America during November 2019. However, there were no earlier samples for comparison and no testing or sequencing of viral RNA for confirmation.
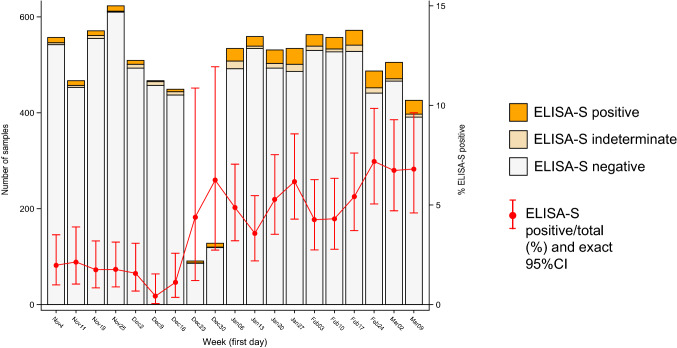
A study of stored blood samples in France examined hundreds of routinely collected samples in a population cohort and found around 2% prevalence of antibodies in November, rising prevalence in December and around 5% prevalence in January. These figures do seem on the high side when compared to the above studies, and the lack of testing and sequencing of viral RNA and the absence of samples from earlier periods suggest this may be less reliable evidence.
Another Italian study (Apolone et al.) tested blood samples from lung cancer screening for SARS-CoV-2 antibodies and found 14% of those from September 2019 were positive for SARS-CoV-2 antibodies, rising to 16% in October though oddly dropping back to 3% in January 2020. These pre-pandemic results are again on the high side and lack testing and sequencing of viral RNA as well as negative controls from earlier periods, meaning they may be cross-reacting. A Spanish study detected SARS-CoV-2 viral RNA in a sample of waste water from Barcelona on March 12th 2019; however, all the other historic samples up to January 2020 were negative and it is suspected that this is a false positive due to contamination or cross-reaction (the sample wasn’t sequenced).
What about early spread in China? It’s hard to get reliable data for this country. However, a leaked Chinese Government report found hospital patients (recognised retrospectively) admitted in Wuhan from November 17th 2019, suggesting the virus was spreading there during November and probably October.
A molecular clock study estimating the date at which the common ancestor of early viral samples was around put the emergence of SARS-CoV-2 as early as July, in China. A separate molecular clock study estimated the emergence between mid-October and mid-November in Hubei province, China; another put the emergence between early October and early December and reviewed other studies which found similar. A fourth estimated an emergence in late October with global spread occurring throughout the winter.
There is considerable evidence, then, that the virus was circulating both in China and internationally by November 2019 at the latest. We can also say with strong confidence that it was not circulating prior to July 2019, and it may not have been around before October 2019, depending on how reliable the European data from the early autumn are.
Some argue that all this evidence of early spread – despite coming from multiple sources and using robust validation methods such as sequencing – must be faulty in some way, as the lack of excess deaths prior to March 2020 makes it impossible for the virus to have been spreading widely over the autumn and winter.
My view is that this argument is insufficient to overcome the clear evidence of early spread. I don’t deny that there is something of a ‘mystery‘ that must be resolved insofar as the waves of excess deaths did not begin until March 2020. Some sceptics resolve this ‘mystery’ by arguing that the virus must therefore be no more deadly than other similar viruses, and thus that any excess deaths since March 2020 must all have been caused by interventions such as lockdowns, faulty treatment protocols and vaccines. However, I agree with Dr. Pierre Kory that we have undeniable evidence of waves of severe pneumonia with a common clinical profile that began in March 2020 and that are best explained by the novel respiratory virus to which most of the deceased tested positive. While some of the excess deaths will be due to interventions, and some of the Covid deaths will be misclassified, the majority of additional deaths from a respiratory cause will be due to the virus. Professor John Ioannidis used antibody data to estimate that the infection fatality rate in the Americas and Europe in the first wave was around 0.3-0.4% (higher in hot spots), which is several-fold higher than flu, usually estimated at around 0.1%.
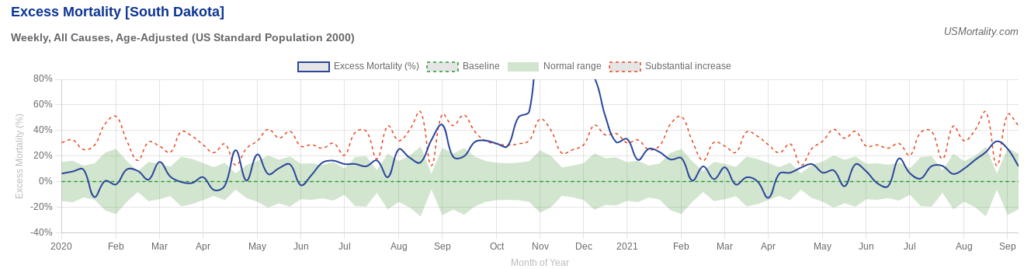
A good counterexample to the claim that all the excess deaths in the pandemic were caused by interventions and not the virus is South Dakota, which imposed very few interventions. Despite this laissez-faire approach it had a mild spring wave; yet then had a massive summer wave that resulted in greatly elevated deaths during the autumn. These deaths certainly can’t be put down to sudden panic: the state was so relaxed during its summer outbreak that it held a massive motorcycle rally.
So how to explain the lack of excess deaths during the autumn and winter of 2019-20? The most important point to be made is that while SARS-CoV-2 was clearly circulating during that winter, it does not appear to have been the dominant virus either in the community or in care homes and hospitals. Thus while, say, 2% of the population may have contracted the virus during the winter, because it was competing with other, milder viruses and wasn’t running rampant among the high risk population, its impact was limited and it did not cause noticeable excess deaths.
The early-spread-sceptic’s objection to this point is that the virus is clearly highly infectious so if it was present and circulating it’s simply not possible for it to have remained at a low level and not run rampant in, say, care homes, causing havoc.
But is it really true that the virus always causes a large wave of infections and deaths whenever it is present, and as soon as it arrives? The evidence suggests not. Just look at how it failed to take off in many places in spring 2020, not just South Dakota, but Japan, South Korea, Germany, Eastern Europe and large parts of the U.S. India notably wasn’t hit hard till Delta in 2021, and East Asia not until Omicron. In other words, the virus doesn’t always do what we’d expect, and in particular it doesn’t always cause a large, deadly wave as soon as it is present.
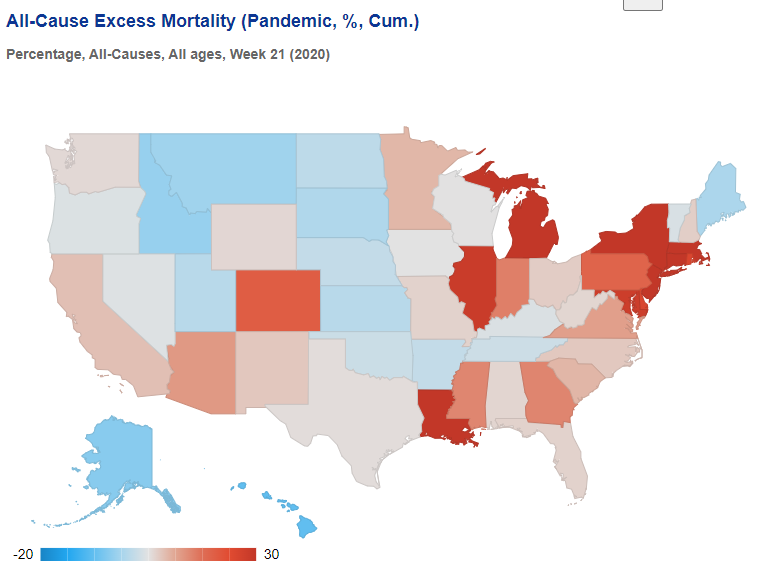
To illustrate, here’s the picture in the U.S. at the end of May 2020, after the initial wave. It’s a real patchwork, with clear concentrations of excess deaths around New York and around Michigan, Illinois and Indiana, plus Louisiana and one or two other states. Many other states had very few excess deaths during the spring. Yet we know the virus was circulating widely in every state.
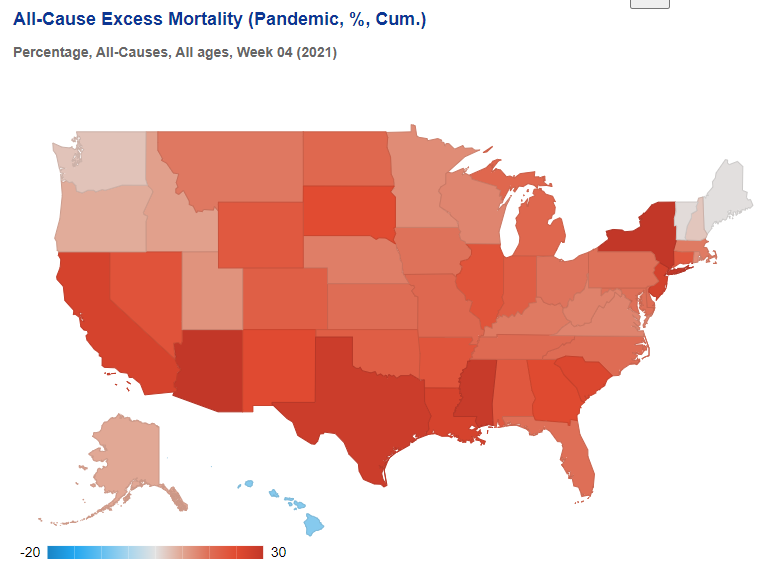
Then, by the following winter, excess deaths were high almost everywhere, meaning specific local treatment protocols or policy responses cannot be credited either with causing the deaths or averting them.
In Europe, too, there was huge variation in the impact during the initial spring wave, even though the virus was circulating everywhere.
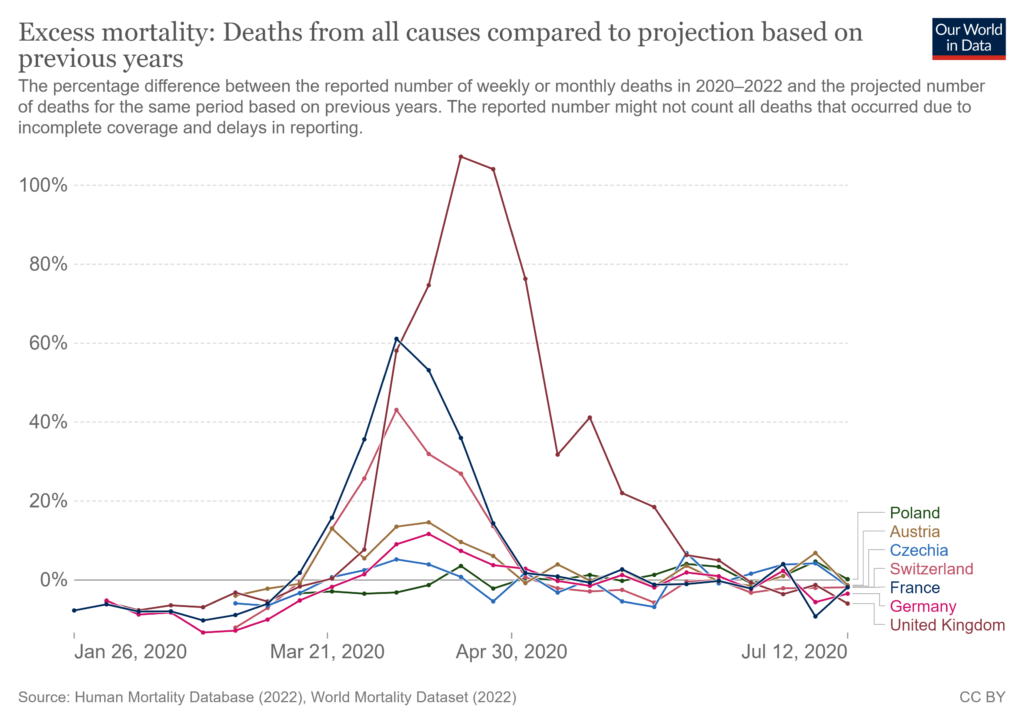
This wasn’t owing to policy responses, as shown by the very different outcomes the following winter.
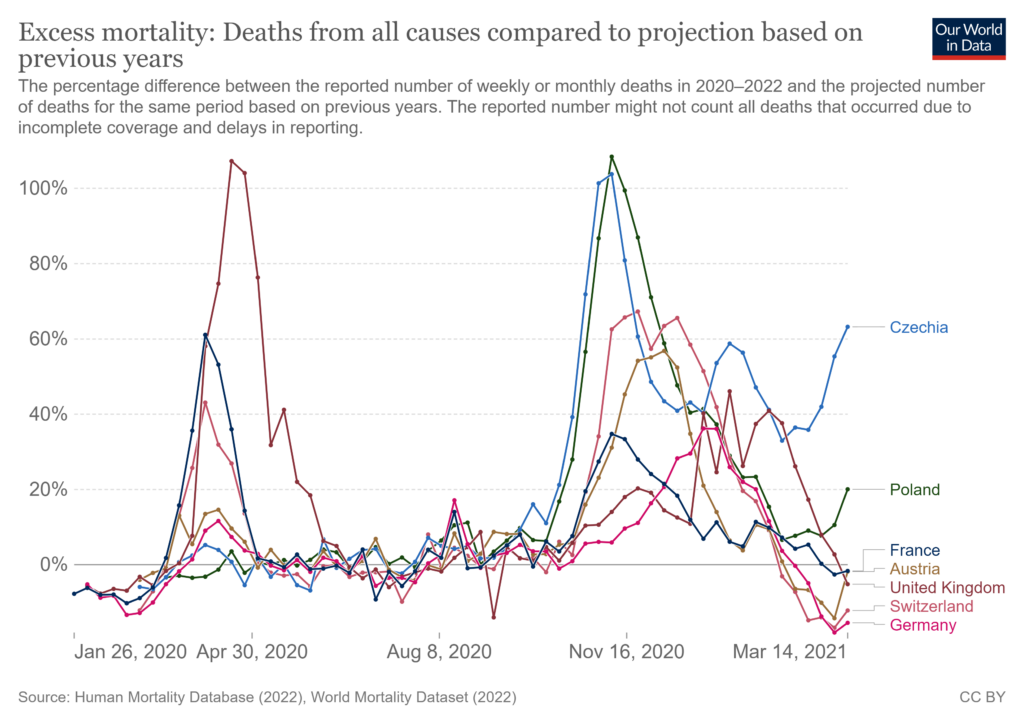
In line with these inconsistent outcomes, numerous studies have shown that outcomes during the first wave weren’t explained by policy responses. But they also aren’t explained by whether or not the virus was circulating, as it was circulating everywhere.
The evidence we have, then, from multiple studies with strong validation methods – including genetic sequencing of viral RNA – shows that the virus was circulating globally since November 2019 at the latest, with some evidence of its presence as far back as July, though not earlier than that.
The most likely reason there was not an explosive, deadly outbreak prior to March 2020 (or even later in many places) is that the virus was still in competition with other winter viruses so was not dominant or running rampant in hospitals and care homes. The large outbreaks from spring onwards may have been assisted by the emergence of new, more infectious (and possibly more deadly) variants. A winter Covid prevalence of around 2% largely among the low risk could easily go unnoticed among the usual winter diseases without triggering noticeable surges in hospital admissions and deaths.
On this evidence, then, it seems we can definitively rule out both an emergence before July 2019 (too many negatives and just one questionable positive) and after November 2019 (too many positives in a number of countries). The evidence is not currently consistent or robust enough to be able to pin it down more definitively than that.
There should, of course, be much more evidence on early spread. The World Health Organisation in June 2020 called for early spread to be properly investigated. However, very little has been done, and particularly in the United States, the various Government agencies have made no efforts to investigate early spread as part of their general neglect and squashing of all investigations into Covid origins.
Such silence and obfuscation only raises suspicions. And there is no shortage of reasons to be suspicious. The lack of genetic diversity in early samples, the high degree of adaption to humans from the outset, the absence of animal reservoirs and the presence of unique features that make the virus highly infectious among humans suggest that it was not natural but engineered, and thus either leaked from a lab or was released. Who was involved in the research that created the virus and the course of events that led to its getting into the human population is therefore a question of great importance that must continue to be pursued.











To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
Another important article from Will, objectively summarising the pharmacological (if that’s the correct word) evidence.
Why didn’t SARS-COV-2 kill loads of people in the fall of 2019? Well we know it’s seasonal (although not entirely what drives that seasonality), so that’s a sufficient explanation for now.
My feel is that the interventions did kill lots of people, but probably do not account for all the excess deaths seen in spring 2020.
There’s also the non-pharmacological evidence.
As I always point out regarding this topic, the Wuhan Lab deleted its coronavirus database in early September 2019 (correct me on date if wrong). And there’s the Gates ‘investment’ in Biontech in September 2019, and Event 201 on 18 October 2019.
Taken together these are massive smoking guns.
As I’ve pointed out before, my current favoured hypothesis is that the virus accidentally escaped from the Wuhan Lab in summer 2019, and was recognised as having escaped by late August at the latest. The Wuhan Lab staff then informed the US authorities (who, after all, had funded the research), but not the Chinese authorities.
The US authorities went into panic mode – there was no reason not to expect the devastating case fatality rates of SARS-COV-1. One can only imagine the terror this must have caused among those in the know. The US authorities then started to pursue what very limited mitigating actions were available to them: get vaccine research going fast (e.g. Gates Biontech investment), and get public health ‘experts’ thinking about what to do (e.g. Event 201).
By autumn 2019 the US authorities – for which we must read the intelligence agencies and parts of the military – were in charge (if that’s the right word) of the response, and they responded in about the only way intelligence agencies and military psy-ops units know how to work – which comprise an anathema to everything free-thinking, freedom-loving individuals in a true liberal democracy believe and value.
Then a load of second-raters caught a whiff of a chance to indulge their latent authoritarianism and self-righteousness, and loads of others caught the smell of money.
And a weak-minded, dumb population at large went along with it, all the way to repeated injections with a vile poison.
And we are left with an absolute fucking mess.
PS: An obvious follow-up line of research would be to investigate the background and genesis of Event 201, and in particular when and how the workshop parameters – which so intriguingly anticipated what was to come only 4-5 months later – were decided upon.
If those parameters and study criteria were identified only in the days and few weeks (i.e. from about late August 2019) before the actual Event, then we have a massive smoking gun.
It may well be possible (for someone with more time and connections than me) to probe and get to the bottom of this.
Excellent read and analysis TJN. We obviously can’t call any “exercise” that is conveniently held a few months before a genuine outbreak nefarious despite it appearing suspicious, but the timing and accuracy of the details leaves many to wonder how much is actual ‘pandemic preparedness’ or outright instigation (not necessarily in origin but simply their never letting a crisis go to waste).
Let’s not forget their more recent gaming exercise in ‘Catastrophic Contagion’ in Oct just gone (quite the eyebrow raiser just in name – sounds like an ELE grade of fearporn) but if a similar chain of events were to coincidentally materialise in the months after that too it would surely make even the least bit cynical among us be wary of Springtime 2023 for their ‘next move’ (if they’ve some sort of foreknowledge or crystal ball – op Lockstep / Spars whereby a crisis is used to further an agenda).
I hope I’m not predicting some sort of round 2 but the next crisis may not come in a predictable format, the cause alternate, but naturally to combat it.. the solution and intervention the same, or at least.. all rolled into one – climate lockdowns anyone? Who knows what they’ll conjure up if people do actually start dying for some unknown reason. Oh wait, I think that’s already happening.
Lots to learn from their breadcrumb trail[s].
Thanks for comments Lancer.
My (leading) question about Event 201 is aimed at examining the hypothesis that it was in response to an urgent request by US intelligence to come up with a plan or strategy on how to deal with a novel coronavirus outbreak – this as a consequence of their already being aware of a lab leak from Wuhan, terrified what the consequences might be, but of course unable to discuss publicly what they knew.
This scenario is of course fundamentally different from the one some ‘conspiracy theorists’ propose in that Event 201 is evidence of a ‘plandemic‘.
Got to dash now, but I’d welcome any commentary or criticism on the above posts – down-voters are most welcome to give their views.
How do you explain George Gao, Director-General of the Chinese CDC, being one of the ‘players’ for Event 201?
Wouldn’t it be expected that a range of interested nationalities would be invited to such an event?
His invitation doesn’t seem to me to form evidence that China already knew what was going on.
Your thesis is that WIV informed the US about the outbreak, but explicitly did not inform the CCP. It therefore seems kinda unlikely that the Director-General of the Chinese CDC would turn up to Event 201, which in your theory is an attempt by the US military/intelligence/Bill Gates to hastily war game their response to an outbreak they already know is incoming.
If the US knew but China didn’t know, how does George Gao end up being invited?
My suggestion (no more) is that the Event attendees didn’t know (weren’t told) that a coronavirus was on the loose. The exercise included invitees from across the world – as might be expected for an event of this type – and thus naturally a Chinese representative would be invited.
https://www.centerforhealthsecurity.org/our-work/exercises/event201/about
“largely among the low risk could easily go unnoticed among the usual winter diseases without triggering noticeable surges in hospital admissions and deaths.”
Strange, that’s exactly what’s happening now except its being deliberately ignored for a different reason, political embarrassment!
Suddenly the weekly death toll so openly shouted from every high point is now no longer important! You are now free to die of non covid illnesses in animimity!
If it was a deliberate leak, which I believe it was, then the most likely culprit would be the US. There are no lengths that the US would not go to in order to enact change and remain the dominant global force.
A deliberate leak seems unlikely to me – too risky, and they risk infecting themselves. One possibility is that it was deliberate but the aim was to test out fast “vaccine” development and lockdown measures. They’d done a lot of planning, and the military don’t like to go too long without using their planning/training/weapons/troops in a real-life situation. It sort of makes sense superficially – we have all this stuff we spend tons of money on, we have to test it properly in case we ever need it – but rapidly becomes self-perpetuating (e.g. manufacturing wars).
Nothing is off the table for me, no matter how seemingly unlikely. We have to consider what the actual risk was and when the PTB understood that risk. It is possible that the risk of virus was well understood before the virus was first ‘found’; that would negate your first argument. That theory would obviously feed into the hypothesis that what started in March 2020 was well planned beforehand. This I also believe.
So many possibilities and we’ll probably never know, without some degree of uncertainty, what happened and who pulled which levers.
Btw, Happy Xmas.
Likewise.
I think we will make further forward progress in 2023.
Many things will remain uncertain, maybe forever, but many things are already certain – we were lied to, and there was gross folly and evil from many sides.
My wife (a teacher at the time) brought home what could only have been the lurgy, obvious in hindsight, we have tried to remember if it was August or September 2019, we both had a mild tickle and runny nose, for about 2 days, then those abated but no taste or smell for 15 days after.
It was quite concerning at the time as nothing like it ever before and Anosmia for life seemed a bad way to live. Obvious now what it was. This was in SE England with no long distance travel in the time frame.
Posting for a friend from the Lockdown sceptics Reddit
“Convoluted article by Will Jones today.
Can somebody with posting rights please direct him to Rancourt’s work on total mortality of the last 3 years.
Lots here:
https://denisrancourt.ca/categories.php?id=1&name=covid“
What’s the basic point he’s making? I couldn’t see an obvious connection between this post and the links within the link you’ve posted. Obviously missing something.
Will Jones in the DS article makes reference to spikes in mortality that Will thinks were at least in part caused by covid. Rancourt’s point, from what I understand, is that all the increases in mortality were caused by government and other covid related measures. But I don’t know what his answer would be to Will’s specific points in this regard e.g. South Dakota. Feel free to join the LS Reddit and ask – the link is in today’s comments.
Ok, thanks.
Could not your Reddit friend see fit to put a blue one in the pot tof? Just to help the cause a touch.
I keep arguing with them about this site and keep regretting it as I just get aeriated. Some of them, especially those that used to post here, think TY is “controlled opposition” and/or a traitor to the movement, in this for his own ends etc. They feel very bitter about things that were said and done when changes to the site were made. I think their reaction is/was over the top and they took it too personally and they are way off the mark, but it takes all sorts.
I am seldom ill. I had what I described at the time as “a very nasty little virus” in mid-November 2019: incredibly tired for 3 days; fluctuating temperature and a persistent cough which took me 3 weeks to shift.
Where I live there are several large private schools in the vicinity, with (I estimate) about 50% foreign students each, and an International School which had a very large cohort of Chinese students.
I got the bug, along with many others in the town, about 2 weeks after the students returned from their two-week, October half-term break. I’m convinced it was Covid.
I’m unjabbed; I’ve lived life under the restrictions as close as possible to normal and socialised throughout. I’ve not “officially” had Covid.
Perhaps there were no significant excess deaths before March 2020 as it wasn’t until then that died with was included with died from
There was a significant spike in all-cause mortality I think in late March/early April 2020, so cause of death isn’t relevant. If it wasn’t covid, what was it? Lockdowns, neglect, DNR? Or some combination of covid and those other things.
In July 2019, the CDC shut down all research operations at the US military’s pinnacle infectious disease facility – Fort Detrick USAMRIID (United States Army Medical Research Institute of Infectious Diseases), over breaches in biosafety standards.
“The suspension was due to multiple causes, including failure to follow local procedures and a lack of periodic recertification training for workers in the biocontainment laboratories”, according to CDC spokesperson, Caree Vander Linden.
Seems like a pretty severe response from the CDC over some recertification issues…
Interesting. Maybe there’s a little more to this than meets the eye (or maybe not).
Do you have any sources?
https://www.fredericknewspost.com/news/health/fort-detrick-lab-shut-down-after-failed-safety-inspection-all/article_767f3459-59c2-510f-9067-bb215db4396d.html
Many thanks.
Btw, I had to use VPN to access this – not allowed to see it from within the EEC.
Attached for reference. [Edit] Open in new tab to view.
I can’t actually read that! But I guess it’s the newspaper article.
I’m glad you mentioned the South American occurrence, as well as the other European one, which suggests that “SARS-Cov-2” and it’s varieties probably emerged earlier than it was officially revealed.
About a year ago, after following some commentary either here or on it’s predecessor, I decided to shell out for a private blood assessment on the basis that what I had in late 2019/2020 might have been caused by it. It was a T-cell assessment technique based on a couple of test tubes of blood (if I had dealt with it so long ago, there would probably not have been any antibodies left). The clinician that dealt with the samples was based in Cheltenham, and the lab work was done in Abingdon, Oxon. The result was inconclusive, so no real evidence that it was “Covid-19”, though. Nothing unusual or particularly aggressive since then, and I’ve never used the jab on offer.
:… as the lack of excess deaths prior to March 2020 makes it impossible for the virus to have been spreading widely over the autumn and winter.’
There wouldn’t be excess deaths prior to March if COV 2 deaths were mistaken for Cold & ‘Flu deaths.
Infection to death = 21 to 28 days. Death rates UK & other European Countries peaked in first week of March 2020, meaning that, allowing for reporting delays, infection rate peaked early February.
From Hope-Simpson curve… the one the idiots were trying to level… this would mean the exponential phase of spread occurred during January 2020 rising quickly from a low base level at the start of that month. That would mean a low level, unnoticeable spread carried back into the 2019 ‘flu season’ – unnoticed because there was – until all the hysteria – no reason to suspect anything other than the usual respiratory viruses doing the rounds. And this is wholly consistent with evidence found in retained blood and sewage samples.
The importance of the early, unnoticed circulation of the ‘dangerous, fast spreading’ virus, is the remarkable absence of the vast number of expected victims, if not hospitalised, then certainly laid low at home in bed during January to March 2020 with heavy Cold & ‘Flu-like symptoms and the concomitant disruption to transportation, manufacturing, retail, schools and life in general.
Plus an early appearance indicates that the peak of the ‘wave’ was over and in decline weeks before the goons in charge unnecessarily locked down society and the economy.
This is why they want to rubbish the early circulation evidence.
“There wouldn’t be excess deaths prior to March if COV 2 deaths were mistaken for Cold & ‘Flu deaths.”
I expect I’m being thick but don’t follow what you’re getting at. Surely in this context “excess” deaths merely means the number of deaths from all causes in relation to some baseline like an average over the last 5 years. Unless you think the death stats are fiddled, the number of people dying from all causes as a % of population went up fairly dramatically around March/April 2020, and came down fairly dramatically not long after. So there was something different happening, or a combination of factors.
It is important to note that this means that the WHO ‘s pandemic early warning systems didn’t work.
Despite all of their self-congratulations over Covid, they only shown failure:
I’d say that the WHO have failed miserably — if they answered to a single country they’d be subjected to root-and-branch reform over their Covid response. Instead they’ve self-declared themselves to have been the savours of the world and are now insisting that every country sign up to their way of solving health crises.
Cock-up theory. Now unequivocally debunked.
There appear to be no adverse consequences to this failure, for them. Not only have they declared themselves saviours of the world but the world has by and large agreed with them – at least those in charge of funding. It’s a New World Order in which success and failure are not measured by objective criteria like saving lives but by how cuddly and politically correct your policies and statements are. I don’t think “reform” would work. As long as there is some kind of global public health body it will tend to indulge itself. We’re better off without them.
if they’d have insisted upon China opening its records at an early stage we might have found out more about the origins of Covid and thus saved lives
I do wonder if that is true. I suspect that the Chinese authorities were pretty much in the dark like almost everyone else, certainly in the second half of 2019. My hunch, however, is that the US Intelligence agencies did know about the emergence of SARS-COV-2 by then, and were acting as covertly but urgently as they could to mitigate what they believed might be a disaster in the offing (and in doing so thereby offering grist for so-called ‘conspiracy theorists’ further down the line).
if they’d have insisted upon China opening its records at an early stage we might have found out more about the origins of Covid and thus saved lives
Again, I do wonder about the extent to which this may be correct. My suspicion is that the Chinese authorities knew very little about what was going on (via US funding) in the Wuhan Lab, and that they understood even less.
My hunch is that we’ve all been too quick to place blame on China. My gut feel is that the real villainy lies in the US.
Happy to be proved wrong, but I think these are vital points which should be fully probed.
Regarding your main point – the WHO being unfit for purpose and effectively unaccountable: Yep, undeniable.
As far as the authorities (in China or anywhere else) being slow to recognise the emergence of a new disease: well I do wonder to what extent it is practical or even possible to recognise the emergence of a new(ish) respiratory virus, especially if it presents with symptoms common to just about every other type of respiratory virus.
There was also the strange late 2019 statistical signals of an unusually early influenza outbreak (I suggest that this was associated with Covid) and a strange spike in cardiovascular problems (this is probably the actual health problem that occurs with Covid infection — what we call ‘severe Covid’ is an immune overreaction seen in vulnerable groups, due to the nature of their ‘fragile’ immune system).
It is perhaps of interest that since vaccination started we’ve seen significant increases in cardiovascular problems. I suppose that this could be due to:
Whoever designed that spike had a particularly nasty and cynical turn of mind.
I suspect the gist of your post is correct.
One good thing about South Dakota taking it on the chin early on in Fall 2020 is that even the dreaded Delta didn’t seem to have any teeth in 2021. Kinda like in Sweden. In the long run, South Dakota ended up an average state in terms of cumulative excess death rates.
Another counterexample similar to South Dakota is Belarus, who also saw significant excess deaths as well with practically no interventions. Though compared to their neighbors, they really weren’t so bad either.
A Chinese scientist, assigned to investigate the virus, defected and is currently being given asylum in the USA. She said on GB News that the release was deliberate. It certainly put a stop to China’s enemy, President Trump, from being re-elected.
Anecdotally, I had what was unquestionably the virus in late December 2019. It knocked me out for three weeks and I struggled to fill my lungs for three months. My Dad was told by a nurse he saw at New Year that they were being ‘inundated’ with calls about a flu-like virus with headaches, coughing, breathlessness and loss of sense of taste and smell. The staff at the surgery all had it. My Dad declined badly from the Chistmas virus and got pneumonia afterwards; he spent the first week of lockdown in hospital. The first person I know who went down with the symptoms locally was a lady returning from an international conference at the start of December 2019.
The truth about COVID-19 opens a whole can of worms about bioweapons and vaccine research. It also makes you reassess the sudden emergence of viruses such as HIV/AIDS, which, after COVID-19, I suspect to be an earlier lab creation, perhaps intended to depopulate Africa.