
Evidence from Europe suggests the vaccines did save lives.
The EU country with the highest excess mortality, Bulgaria, also has the lowest vaccination rate. By the end of 2021, only 36% of Bulgarians over 60 had been doubled vaccinated. Meanwhile, the EU country with the lowest excess mortality, Denmark, is one that managed to keep deaths to a minimum until completing the vaccine rollout. As of January 1st, 99% of Danes over 60 were double vaccinated.
However, this does not mean the vaccines’ effectiveness against death is as high as 90%, or even close to that. Numerous countries around the world have seen large spikes in excess mortality after their vaccine rollouts. These spikes invariably coincided with waves of Covid infections, showing that – despite high levels of vaccination – many people were still dying.
One interesting case study is Lithuania, which has the second highest excess mortality in the EU. You might assume, therefore, that it would have a low vaccination rate. But it doesn’t. By the end of 2021, 78% of Lithuanians over 60 had been double vaccinated – the highest level in Eastern Europe.
Compare Lithuania to another Eastern European country, Romania. As the chart below indicates, the vaccine rollout was proceeding identically in the two countries until the end of April 2021 – when Lithuania jumped ahead.
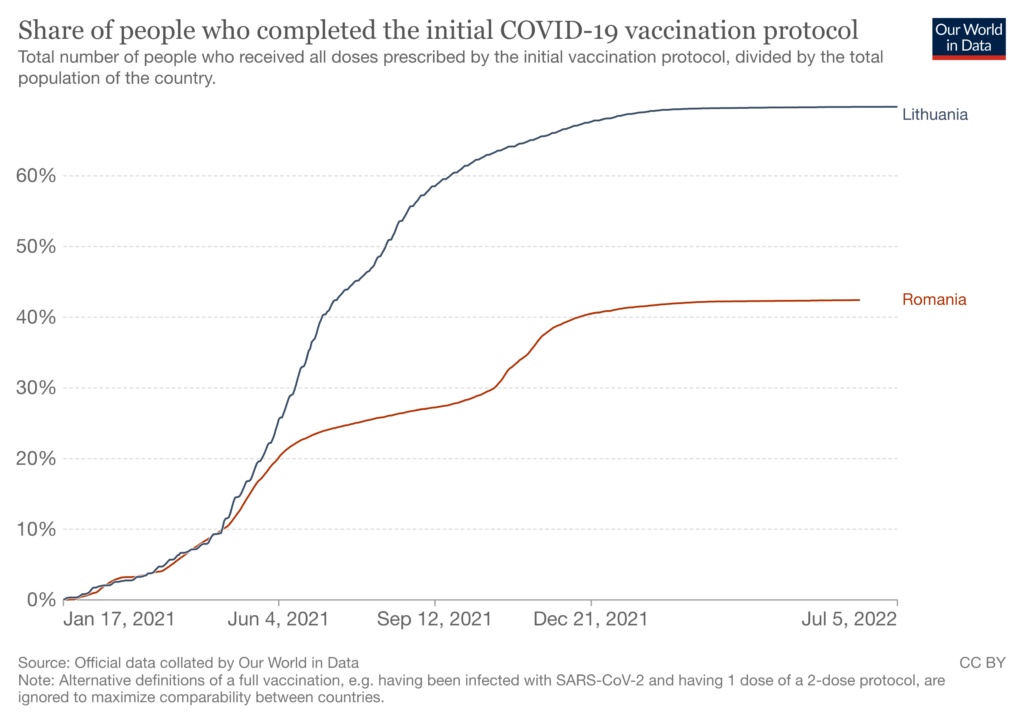
By the start of September, less than half as many Romanians had been double vaccinated. And as of January 1st, only 46% of Romanians over 60 were double vaccinated. So that’s a disparity an elderly vaccination rates of 32 percentage points!
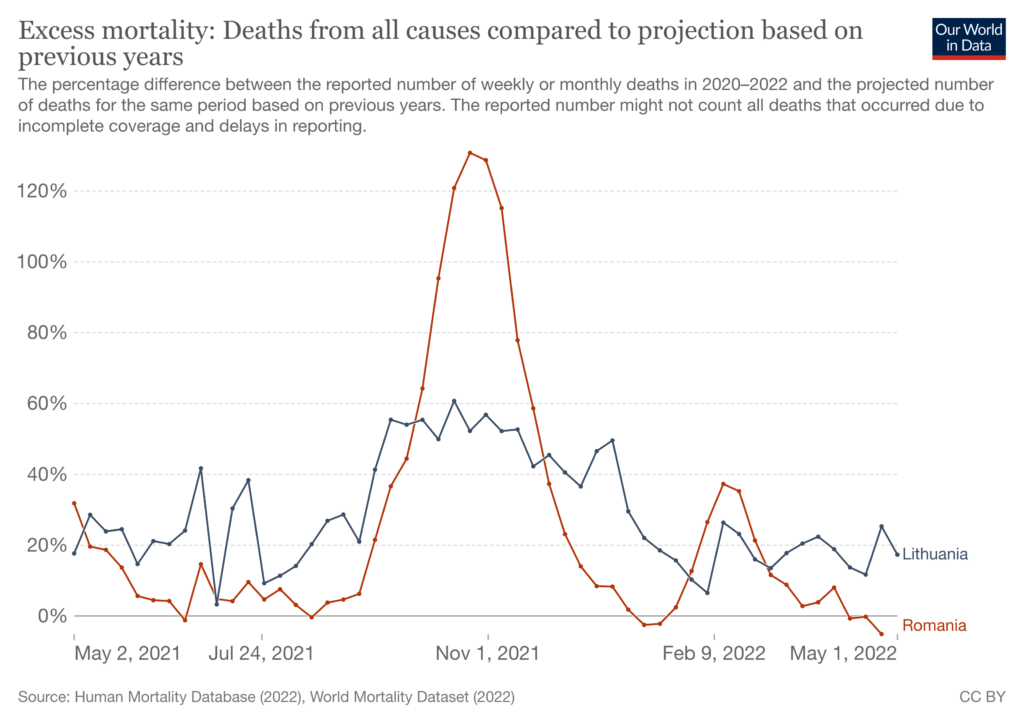
However, if we track excess mortality since the countries’ vaccine rollouts diverged, we see that it was actually higher, on average, in Lithuania. (Note: although the peak is higher in Romania, the average is slightly higher in Lithuania.)
Zooming out, this can’t be explained by a ‘catch up’ effect: the two countries’ saw similar levels of excess mortality during the first year of the pandemic. Lithuania saw a bigger peak in the winter of 2020, but Romania saw a bigger peak in the spring.
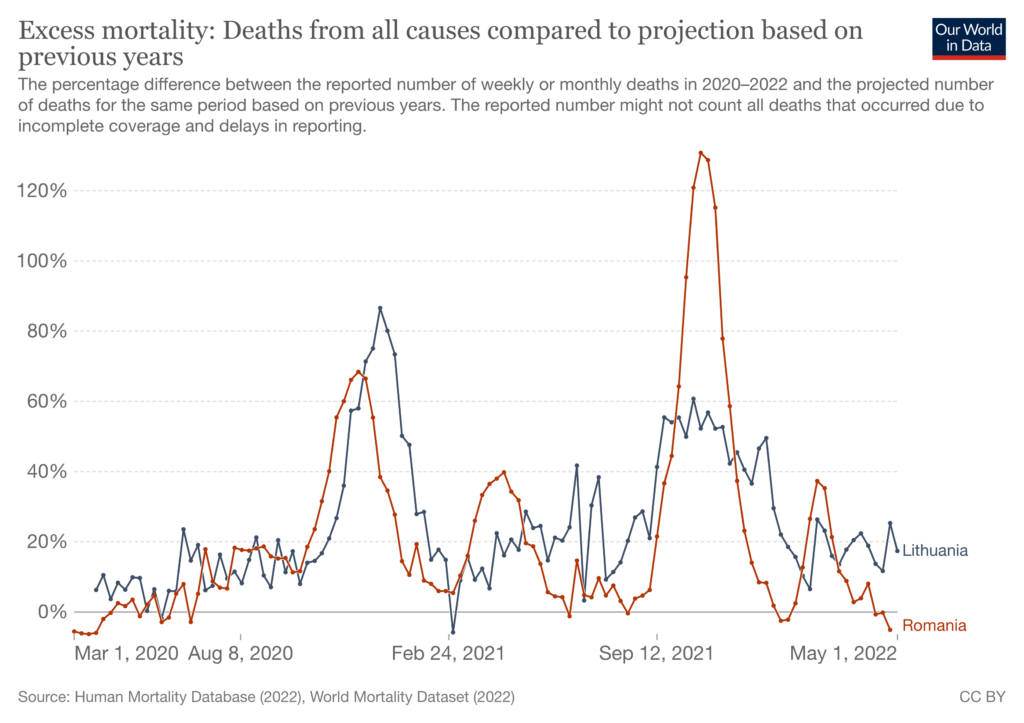
Nor can it be explained by Romania being richer, and having higher quality healthcare. As a matter of fact, Lithuania has a substantially higher GDP per capita – $46,000 versus only $37,000 in Romania.
Two peculiarities of Lithuania’s series are the spikes in June and July of 2021, when the rate of Covid infections was low. These spikes may have been caused by hot weather, though a search for “heat wave” during the relevant time period did not yield any results. If the two spikes were excluded, excess mortality would be somewhat greater in Romania.
Although Lithuania and Romania began their vaccine rollouts at the same time, Lithuania went on to vaccinate a much greater share of the population, including a much greater share of the elderly. Yet in the year afterwards, excess mortality in the two countries was similar – an observation that can’t be explained by wealth or ‘catch up’ effects.
Generally speaking, countries with lower vaccination rates have seen higher levels of mortality. However, even very high vaccination rates have been not been sufficient to prevent mortality from spiking – casting doubt on claims the vaccines are near-perfectly effective against death.
This post has been updated.













To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
Meanwhile the Covid enquiry in the UK continues to take its time.
The Covid enquiry in the UK is, by-and-large pure theatre. The conclusions of the enquiry had been decided before the enquiry even started.
Happy lawyers… once again!
As Domonic Cummings said….Many of the meetings are a foregone conclusion.
The CONVID enquiry in the UK remains a complete charade plain to see for anyone able to bring themselves to look.
A hero.
Each little victory opens the Overton window a crack. Good on yer, mate.
Thanks to Rebekah Barnett and the DS editors for this wonderful news from Australia, which we might never have heard through the mainstream media.
Aseem Malhotra is still in the firing line:
https://www.gmc-uk.org/news/news-archive/statement-on-judicial-review-of-our-handling-of-complaints-about-dr-aseem-malhotra
And the death of his uncle, and maybe it will get people more interested in our own state secrets that often are classified till 2045 to name a few.
Both his Uncle and his Father……Trump was persuaded not to open the Files….as they were too shocking……also Martin Luther Kings…..
There are a whole stack of ‘skeletons’ to be found. The reality will be terrifying. See attached and try googling any of the entries on it! Coincidences?
Hear hear!
Australia was one place I did not expect this to happen.
I think a lot of people who work in healthcare are feeling genuine remorse now. They were sincerely ignorant at the time and now can’t deny what is happening in terms of admissions for cancer. People showing up with no previous medical history, no risk factors, and finding out that they have advanced lung cancer. It is a terrible death even if it only lasts three months. Not just the lungs the whole body wastes away bones become so thin and then the final unspeakable agonies. To my mind this is the greatest evil in the history of humankind.
The BBC ran an article lamenting the fact that Stephen Bartlett allowed experts like Dr. Bay to voice their educated opinion or as the BBC put it “spread misinformation” on his popular podcast.
This is why BBC Verify is seen as a joke. When even courts find that medics have every right to question vaccines, lockdowns or any other pharmaceutical or NP intervention and indeed should be encouraged to do so it lays bare what Verify is – a dangerous tool of censorship and one-narrative control.