
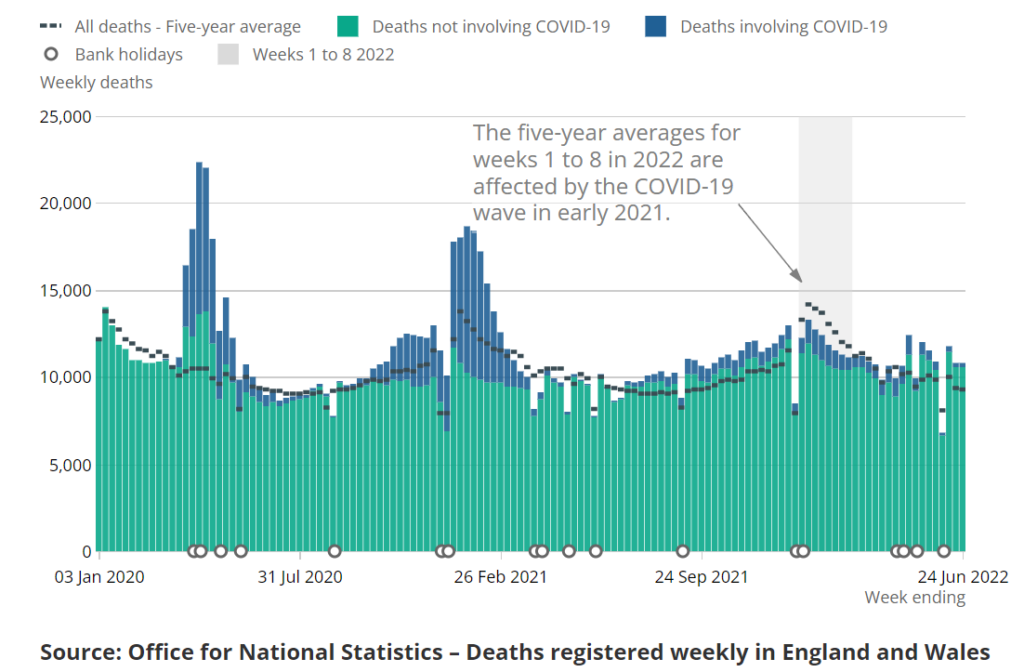
There were 1,540 more deaths than usual in England and Wales registered in the week ending June 24th, the most recent week for which data are available, according to the latest update from the Office for National Statistics (ONS), released on Tuesday. This is 16.6% above the five-year average. Of these deaths, 285 were registered ‘with Covid’ and 166 as due to Covid as underlying cause, leaving 1,374 from a different underlying cause.
This brings to 7,840 the total number of non-Covid excess deaths (above the five-year average) since April 29th, the start of the recent spike. Of these, a large proportion are occurring in the home, leading to calls for an urgent investigation into why thousands more people are dying than would be expected, despite Covid death numbers staying low. It is doubly concerning as following the 138,000 excess deaths since March 2020, a reduced number of deaths would now be expected due to the mortality displacement of people dying earlier than they ordinarily would.
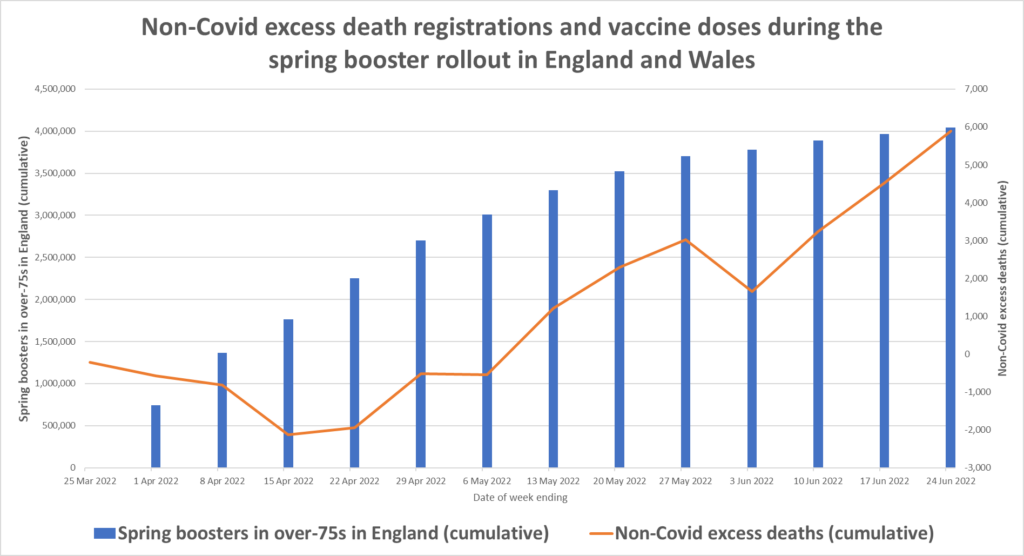
As I noted last week, the current spike in non-Covid deaths has broadly coincided with the spring rollout of boosters to over-75s, which began on March 21st. This pattern is depicted in the following two charts.
The first shows cumulative non-Covid excess deaths by date of registration since week ending March 25th (the dip in the week ending June 3rd is due to the bank holiday weekend). The rise in doses and deaths around the same time is obvious.
The second chart shows weekly (not cumulative) non-Covid excess deaths by date of occurrence (I have split the first week’s vaccine doses between the first two weeks as there was no report in the first week).
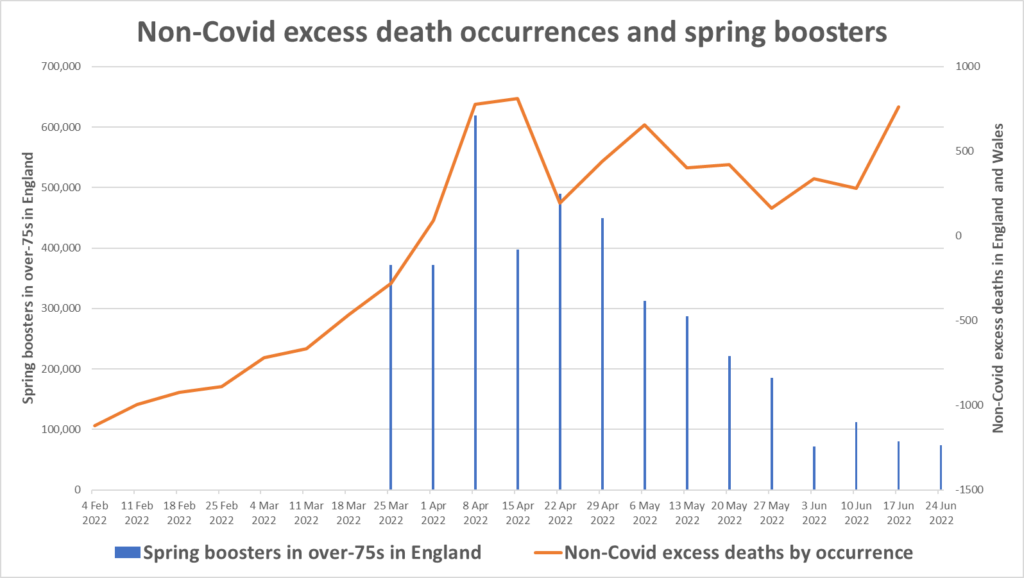
A correlation of sorts is evident between vaccine doses and non-Covid death occurrences. However, it can also be seen that non-Covid mortality was rising since at least the start of February, though with a marked acceleration around the time of the booster rollout. It is also clear that non-Covid deaths do not fall off as the rollout winds up, which might have been expected if the vaccines are the primary driver.
The sharp rise in deaths by occurrence in the week ending June 17th is particularly noticeable.
Breaking it down by age, around 75% of the non-Covid excess deaths registered since week ending April 29th have been in the over-75s, meaning around 25% of the excess deaths are in the under-75s, despite that age group not participating in the spring booster campaign. In the most recent week (ending June 24th) the proportion of deaths in the over-75s dropped sharply to 64%, compared to 72% the previous week. This suggests the latest spike since mid-June is being driven to a large extent by the under-75s.
This gives a somewhat mixed picture of how the current wave of non-Covid deaths may relate to the spring booster campaign. This does not mean vaccinations should be dismissed as among the causes, however.
A recent article by Michael Simmons appeared in the Spectator asking what is behind the surge in deaths at home. He briefly considers the possibility that the vaccines may be involved, only to dismiss it.
Might the rise in at-home deaths be linked to the Covid vaccines? A paper by BMJ Editor Peter Doshi is doing the rounds saying that in trials the jab’s side effects hospitalised more than the virus. But the data wasn’t actually that clear cut. Sir David Speigelhalter, a statistician from Cambridge, points out that the study “only considers Covid hospitalisation during the trials themselves, which covered only around two months at a time of low Covid. The true benefit of vaccines extend far beyond this period, so the harm/benefit comparison used in this study seems entirely inappropriate”. He doesn’t think the Doshi paper will pass peer review.
But why then is all this happening? …
This is clearly far too quick to dismiss the role of the vaccines. Even granting Spiegelhalter’s point, it only means the risk/benefit ratio may change over a longer study period. It doesn’t affect the absolute number of serious adverse events that occurred with the vaccines within the study period. Dr. Doshi and colleagues found that the vaccines were associated with excess non-Covid serious adverse events of around one per 800 people vaccinated (12.5 per 10,000 or 0.125%). Since 47.5 million people in England and Wales have been vaccinated with at least one dose, on these figures we should expect around 60,000 serious adverse reactions (at a minimum – the trial participants were younger than the general population).
This estimate of adverse events from the trial data is broadly in line with the real-world findings of an Israeli Government survey, which found 0.3% of vaccinated people reported being hospitalised as a result of their Covid vaccination, as well as a U.S. Government survey, which found 0.9% of vaccinated people reported seeking medical care as a result of their vaccination, and a German study, which found 0.8% of vaccinated people reported struggling with serious side-effects.
With up to 1% of the vaccinated needing medical care, it is thus not inconceivable that as many as 0.1% may suffer something very serious or fatal, perhaps higher in an older population. Taking 0.1% of the 4 million spring booster doses gives a figure of 4,000, a similar ballpark to the non-Covid excess deaths during the period.
Whatever the respective role of vaccines, Covid and lack of access to healthcare, this is clearly something which needs looking into properly.












To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
The two biggest health issues that I am personally aware of are cancer and heart issues. I have never known so many in my life.
Another funeral next week. Cancer.
Sorry to hear that. Same here; my wife works as a therapist and she is seeing more bereaved clients than ever. She saw two women in one day who had both lost family members to sudden and rapid ovarian cancer last week. Lots of heart problems too, and a couple of sudden unexplained deaths in youngish people. I think it’s quite clear what’s going on.
Ovarian cancer is neither sudden or rapid, I suspect that it is delayed diagnoses and treatment that is the root of the problem. Certainly people with stage 1 treatable cancers didn’t have a diagnosis until it had developed into stage 4 metastases.
I’m sure you’re right; This was a second-hand anecdote so I don’t know the ins and outs. Not sure if you’ve encountered Dr Ryan Cole, US Pathologist who has been talking for some months about the rise in cancers post vaccine and possible causal links. https://podcasts.apple.com/gb/podcast/effects-of-the-covid-jab-discussion-between-dr-ryan/id1286870871?i=1000568624325 This is an interesting discussion.
Forgive me CG but this is one page I wish we weren’t sharing.
A lot of this rapid onset stuff going on and I’m not sure it can only be blamed on the almost total shutdown of the diagnostic wing of the NHS recently.
Anecdote alert!….My mother’s neighbour in her 80’s died about a month after her 2nd “vaccine”, family were told that it was “rapid onset leukaemia”.
Fair enough? Feasible?
Well as it happens, this lady was a hypochondriac, despite being in fine fettle for her age she was always going to the GP for this, that and the next thing….my mum used to get verbatim reports regularly. Which is why my mum knows that her neighbour had been to the surgery about a month before her “vaccine”, had bloods done and subsequently been told the results were fine.
There’s Acute Myelod Leukaemia right enough, but didn’t think it killed people THIS quick.
Make of it what you will.
I was going to start this with “I have no scientific background”, but these days that is more likely to mean that the opinion is valid
In any event, last summer there was a news report in NL of a perfectly healthy 18-year old developing AML and dying within a matter of days. His age group was getting jabbed around that time. If you read up on what AML is, rapid development of blood cells and then figure that the poke is supposed to cause the rapid development of antibodies, which require blood cells/B cells from bone marrow, is it really that impossible that there might be a link between the jab and AML?
I’m sure what I said is over-simplistic, but to be honest, it is not up to me or us here to prove these conjectures, but the drug pfushers and the public health authoriteis to prove that this novel technology cannot cause such reactions.
Do any of the data people who drop in here have access to things like AML rates and whether they have increased in the last year?
From the NHS website
“Acute myeloid leukaemia (AML) is an aggressive cancer that grows quickly, so treatment will usually begin a few days after a diagnosis has been confirmed.”
https://pediaa.com/what-is-the-difference-between-myeloid-and-lymphoid-cells/
These days you can’t be sure whether that description has been changed recently to fit the current narrative.
https://bloodcancer.org.uk/understanding-blood-cancer/blood-cancer-types/
The funeral home directors have the real data that matters … if they would just report it … or if some reporters would somehow get it. On-line or newspaper obituaries could also tell the tale. Are the numbers of deaths going up? Is the average age of death going down?
In America, social security data would also tell us what’s happening as would Medicare and Medicaid data on hospitalizations and doctor’s visits.
Pastors could tell us if they are doing more funeral services. Florists could tell us if they are filling more orders for funeral flowers. Ambulance companies could tell us if they are making more emergency runs.
Ed Dowd and others have reported on sky-rocketing claims of life insurance policies in the 18 to 64 demo. Dowd recently said the number of Americans who are now classified as “disabled” has spiked by three million people in about one year.
In other words, there are countless metrics and dots that could be connected if any serious investigator did a decent amount of research and interviews. Perhaps the biggest tell is that such analysis is NOT being performed (at least by mainstream journalists or official government investigators).
And by whom? Shoveled into the remit of an Inquiry? It is quite likely that there will be a continued loss of confidence, which might cause problems of it’s own, while that rumbles on.
I’ve said this before and it bears repeating again; One does not become a senior public health wallah without knowing that you never investigate anything unless you are clear in advance that you are happy with the findings.
If we are going to get a proper investigation into any of this it will need to be both forced through and have independent oversight. We have a new health secretary from today so there is an opportunity here.
The ‘new’ health sec is even more hardcore WEF than the old one was. There is no opportunity to get an investigation as the diktat has come from without our jurisdiction that an investigation under any circumstances is not to be allowed to happen.
One thing I think I know by now: The public health authorities don’t investigate anything that might embarrass them if the results of said investigation became widely known.
At the risk of sounding like a broken old record, maybe this paper explains it:-
https://www.sciencedirect.com/science/article/pii/S027869152200206X
S. 14 gives biomolecular/immunological explanations for myocarditis but plenty more harmful effects await in the longer term.
For the life of me I fail to understand, lol, why nobody of apparent consequence seems to have read it.
The problems, as ever, stem from the fact that the statisticians know the square root of f**k all about immunology, virology, genetic engineering, electron microscopy and that’s not even mentioning bloody computer coders/programmers.
These are all incredibly complex areas of expertise which unfortunately means that the expert in one discipline has to be holly reliant upon the experts in the other areas being correct.
From a purely scientific point of view, our problems stem from the fact that our brilliant genetic engineers know zero about the effects their products have on the immune system as evidenced in Sections 3-7 of the paper.
Have you looked into the authors of the paper you have referred to?
Have you?
“The problems, as ever, stem from the fact that the statisticians know the square root of f**k all about immunology, virology, genetic engineering, electron microscopy and that’s not even mentioning bloody computer coders/programmers.” From the original post.
Lead author:
Stephanie Seneff Computer Science and Artificial Intelligence Laboratory, MIT, Cambridge, MA, USA, 02139
Nice of you just to mention only Stephanie Seneff, but you omitted to mention that she has a particular interest in immunology.
You also omitted to mention that one co author is Head of R. and D.in a biotechnology lab and that all authors have written papers regarding the immune system, particularly the innate system.
The paper, which is fully and comprehensively referenced, shows the benefits of shared expertise which seems sadly lacking in the one track minds of the genetic engineers employed by big pharma.
My amateur take is that these jabs screw up our natural immune systems. If you have a screwed up, compromised or weakened immune system, death from any possible cause will be much more likely in the future. We don’t know WHEN these deaths occur … just that they will occur earlier than they would have if said immune system had NOT been tinkered with.
Lost a 54 year old colleague to cancer in February. Lost my 50 year old best friend to cancer in March. Both stage 4 at initial diagnosis, both triple jabbed, both fobbed off by the NHS with ‘long Covid’.
My friend’s father in law share my view that the vaccines are behind this.
Something similar seems to be happening in NL. I am not a data analyst, statistician or any such thing, I am only looking at the mortality chart on the corona dashboard of the Dutch government (available in Dutch and English).
The Dutch government does not publish quite such clear numbers – or if they do, I don’t know where to find them. What they do publish is a bandwith of the expected mortality, with a lower and upper limit, with the expected number running in the middle. A quick glance shows that since March 2021, the mortality rate has been at the upper limit or above for virtually the entire time since. There are one or two points where it hits the expected number, a period Jan-Mar 2022 where it is somewhat below what was expected (but not below the lower limit), but for the greater part of the past year and a half it has been higher than expected or excess mortality. Yes, some of it is related to the corona wave starting Nov. 2021, this does not explain the high rate over the past 6 months, nor the persistent high rate since beginning March 2022. The week of 20 – 26 June shows excess mortality again that is significantly higher than the official corona deaths for that week.
I guess we will have to wait until they start giving the over 50s poke 4/5 in September – I expect the lack of efficacy and safety to become much clearer then, along with the inevitable rise in infections that follows a vaxx roll-out.
Another confounder is the other vaccinations offered to older people , including Shingles (70+) and pneumococcal (65+). Some of these will have been delayed because surgeries were closed.
Im not a statistician and so I’d appreciate someone explaining this, it’s only until May this year. https://www.ons.gov.uk/file?uri=/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/datasets/monthlymortalityanalysisenglandandwales/may2022/monthlymortalityanalysismay2022.xlsx
You seem rather like a man on a mission.
It does now seem the current high level of all age all cause mortality in England and Wales is continuing. Previously it looked like the spike coinciding with the Spring boosters was returning to a ‘normal’ level, but it’s not looking that way now.
Here’s my chart of all cause death occurrences vs the 2015-2019 occurrence average, which is the same data used by Will.
Ignore the last week as that’s affected by inaccurate estimates by ONS of deaths that have occurred but not been registered.
I wonder whether the mentioned 17th June 2022 occurrence blip upwards might largely disappear next week when occurrence data becomes more reliable, or not? By blip I mean it being above the previous week (10th June) figure; I’m guessing it will still remain above the 2015-2019 average.
In terms of allocating all cause deaths into those labelled as covid and non-covid it’s pretty clear that, even ignoring over-labelling of +ve SARS-C0V-2 deaths as covid, that covid labelled deaths are a very small fraction of all cause deaths.
The black dotted line is the blue line in the previous chart. And the top of the coloured bars is the green line in the previous chart. It’s just this chart splits out the green line deaths into covid labelled and non-covid labelled.
Chart again from occurrence data.
Maybe a trading update from the likes of dignity funerals will confirm excess mortality. Being listed on the LSE they would have to be honest about numbers. Surely.
Most analysts from the big investment banks ask lay up questions; they never seem to have dived into the financials much at all in advance, so don’t expect any clarity from earnings calls – you would have to do that research for yourself.
Certainly looking at the all cause England and Wales registered deaths age group data based both on the wide post 2020 ONS age categories, and the narrower pre 2020 age groups (the latter of which we can adjust for population numbers) there does seem to be some higher mortality going on across ages not just the over 75s.
So what is going on is multi-factorial.
A proper analysis needs a full comparison across all age groups. But just looking at the age 45-64 age group for example you can (just about) see the blue 2022 accumulated all cause deaths line (which does adjust for changing population numbers over time in each age group) increasing relative to recent years in recent months (although not relative to 2010 and 2011).
As an aside the first 2021 census data has been released but at the moment it’s just estimates at census date that has been released. So I’ve not adjusted my age banded population estimates, but I don’t think it will make much difference.
Will Jones – second graph, red line, doesn’t look very cumulative to me. Am I missing something?
In some weeks there has been a negative ‘excess’, so that reduces the cumulative total of excess deaths so I think it’s OK.
Because there is a delay between deaths occurring and deaths being registered and many vaccine deaths occur say a week or two after the date of vaccination, you might expect a negative excess during the first few weeks of the boosters starting even if the sole effect of the boosters was to cause excess deaths.
Noticed that Jeremy Vine has taken yesterday’s video down off of his twatter.
You know, the one where he reads out a wall of perfectly reasonable tweets that were in response to his bedridden “I’ve got Covid, something must be done”, video…..then mocks the content, and says “there’s a big anti-vaxx thing going on”.
Obviously belatedly realised, or was told, that he was quite successful in getting an important message out to hitherto unaware sheep people about the poor efficacy of the “vaccines”.
Thanks for that Jeremy, you complete and utter moron
What’s behind the surge…?
Let me take a wild guess.
It’s got to be something other than the blindingly obvious.
8000 excess deaths since April, no mention of it at the BBC, who have this shite near the top of their “News” page.
https://www.bbc.co.uk/news/entertainment-arts-62061739
NOT FIT FOR PURPOSE!
COVID Vaccines Increase Menstrual Irregularities Thousandfold, Fetal Abnormalities Hundredfold: Doctors’ VAERS Analysis
https://www.theepochtimes.com/covid-vaccines-increase-menstrual-irregularities-thousandfold-fetal-abnormalities-hundredfold-doctors-vaers-analysis_4564754.html
By Enrico Trigoso
Stand for Freedom – Never surrender your freedom to politicians
Friday 8th July 4pm to 5pm
Yellow Boards
A30 London Rd &
B3272 Reading Rd
Blackwater GU17 0AE
Stand in the Park Sundays from 10.30am to 11.30am
make friends & keep sane
Wokingham
Howard Palmer Gardens Sturges Rd RG40 2HD
Bracknell
South Hill Park, Rear Lawn, RG12 7PA
Henley
Mills Meadows (bandstand) RG9 1DS
Telegram http://t.me/astandintheparkbracknell
Some death data from the USA, courtesy of an American friend
https://www.usmortality.com/
I thought this was an important and rarely-seen point: “It is doubly concerning as following the 138,000 excess deaths since March 2020, a reduced number of deaths would now be expected due to the mortality displacement of people dying earlier than they ordinarily would.”
I’m a layman of course, but I also think “vaccine deaths” would continue months and even years after people got their original vaccines or boosters. It seems to me that different fatal conditions would take different periods of times to do their lethal damage. So, yes, one might expect to see a spike in the near vicinity of a booster roll-out, but deaths related to vaccines would continue to show themselves, right? Some people die within one week or one month of their booster, while others die eight months later or 14 months later.
Another way to express this idea is that if all boosters were suddenly stopped today, excess non-Covid deaths would continue to be markedly higher than expected.
We either have a software glitch or one very sick person on this forum.
Who on earth would downvote comments on here largely made in memory of persons recently deceased as a result of cancers and heart disease given what we know of their associations with the C1984 perforations?
The despicable coward clearly won’t own up and offer a defense of their position. God, their is some rubbish on this planet for sure.
I just logged out to prove it to myself, but it appears you can vote on btl comments if you are not logged in, so perhaps down voters are previous trolls who don’t want to contribute financially but still want to annoy. (I only tried an up vote though)
I think it’s a mistake because on, say, the conservative woman, you can’t vote unless you log in. Possibly something that needs changing?
Having said that, I do miss lots of comments, good or bad. There are so few now it all seems a bit thin.
Thanks for that T O B. I posted a comment a couple of days ago about my disappointment that so many previously regular posters had failed to sign up and help to keep this jewel shining and I stand by that comment. Nobody works for free.
I am glad to see the back of the trolls though and new people are coming on board. We’ll get there.
Let’s hope so.
Yesterday’s ONS publication on all cause deaths by vaccination status potentially gives some new insights into what is behind the recent increase in all cause mortality in England following the Spring boosters.
In particular it appears to show that the relative mortality of the vaxed (vaxed mean any dose throughout this post) relative to the unvaxed has worsened since the Spring boosters started (between March and May), although that’s a trend that has been happening for some time. And so the recent high all cause mortality has a significant component related to vaccine damage.
Here is a chart of the relative all cause mortality, measured using monthly age standardised mortality (ASM) from yesterday’s ONS publication. ASM adjusts for age differences between vaxed and unvaxed and reflects deaths mainly in the older population where most deaths happen.
In May 2021 all cause mortality was 1.91 times the rate in the unvaxed as in the vaxed (ASM of 1718.8 vs 901.6 per 100,000)
However non-covid mortality in May 2021 was similarly higher in the unvaxed relative to the vaxed at 1.87 times the rate (ASM per 100,000 of 1,673.4 vs 895.4). Given that an experimental vaccine can’t help with non-covid deaths (noting that there has clearly been no under-recording of covid deaths from when vaccines started) the higher all cause death rate in the unvaxed is not due to any vaccine efficacy.
So the higher rate of mortality in the unvaxed is probably due to the ONS significantly understating the unvaxed population or a selection effect because the general health of the unvaxed is much worse than that of the vaxed. This health (or terminal illness) explanation is unlikely to be the reason as the Norman Fenton etal paper showed as in practice it was the most vulnerable who were vaccinated first.
In March 2022 all cause mortality was 1.24 times the rate in the unvaxed as in the vaxed (ASM of 1,231.7 vs 992.6 per 100,000)
In May 2022 all cause mortality was 1.06 times the rate in the unvaxed as in the vaxed (ASM of 872.9 vs 822.6 per 100,000)
So the relative mortality of the unvaxed relative to the vaxed has reduced from 1.91 to 1.26 to 1.06 times from May 2021 to March 2022 to May 2022.
Some would say we shouldn’t try to unpick the ONS data because it is clearly wrong as indicated above; a reasonable viewpoint. I take a different view. I suggest we should ignore the absolute ONS mortality rates (for reasons implied above) as they likely incorporate an understatement of the unvaxed population. So the current 1.06 rate doesn’t mean the unvaxed are (adjusted for age) dying at a 6% higher rate than the vaxed. And we need to be careful with misallocated deaths occurring in the vaxed in the first few weeks after first vaccination (for reasons Clare Craig and others have given). However if we look at changes to the relative rates of mortality for periods after most of those first vaccinations in those most likely to die have happened then we can glean some information.
In particular the fall in the relative rates of all cause mortality in the unvaxed vs the vaxed from March 2022 to May 2022 is tentative further evidence that the Spring boosters have caused significant damage, rather than the high mortality just being about lack of access to healthcare due to the disastrous pandemic response that affects both vaxed and unvaxed alike.
This post is based on my first glance of yesterday’s ONS publication. So I may have made a mistake somewhere. And if anyone spots anything wrong with this logic then I would be interested.
It couldn’t possibly be due to the backlog of treatable cases of cancer, heart disease and innumerable other ailments caused by effectively closing down the NHS in readiness for a tidal wave of cases of the sniffles caused by a viral infection that statistically increased the life expectation of its victims, could it?
No, that would be far too easy…
Will, when you say that “It is also clear that non-Covid deaths do not fall off as the rollout winds up, which might have been expected if the vaccines are the primary driver”, you should mention the distinct possibility that vaccine-related deaths occur over a much longer period than the immediate aftermath of the vaccination.