
Five years ago, we reviewed gender-affirming hormones in children and adolescents.
To find the evidence, we searched PubMed Clinical Queries for systematic reviews (the original search strategy is available here).
Our conclusions stated:
There are significant problems with how the evidence for gender-affirming cross-sex hormones has been collected and analysed that prevent definitive conclusions from being drawn. …
The development of these interventions should, therefore, occur in the context of research, and treatments for under 18 gender dysphoric children and adolescents remain largely experimental. There are a large number of unanswered questions that include the age at the start, reversibility, adverse events, long-term effects on mental health, quality of life, bone mineral density, osteoporosis in later life and cognition. We wonder whether off-label use is appropriate and justified for drugs such as spironolactone, which can cause substantial harm and even death. We are also ignorant of the long-term safety profiles of the different [gender-affirming hormone] regimens. The current evidence base does not support informed decision-making and safe practice in children.
The review formed part of an independent analysis for the BBC’s Panorama programme, in which we said transgender teen care “needs urgent regulation”. Also, Carl wrote an article in the Times saying it was time to end the experiment on children.
In the intervening years, we’ve been labelled as transphobes, subject to three different complaints at the University of Newcastle, where Tom was a visiting professor, the University of Oxford and the BMJ, where we posted the original review.
All of these were dismissed – it’s hard to argue that reviewing the evidence should be subject to complaints. But it did have a chilling effect to shut down our BMJ Evidence-Based Medicine posts.
Now, five years after we published our review, NHS England says children will no longer routinely be prescribed puberty blockers at gender identity clinics. Its review found that there was “not enough evidence” that they were safe or effective. A 2022 review by Dr. Hilary Cass reported “gaps in evidence”.
At Trust the Evidence, we do not have any vested interest in the outcome of treatments when we review the evidence.
Yet, consistently, we have found that an evidence-based approach has proved controversial. People tend to hold strong beliefs and convictions about various treatments, which is precisely why an impartial, evidence-based approach is crucial. When the pharmaceutical industry’s competing interests and financial gains are considered, having an evidence-based approach is essential for reviewing the evidence and informing decisions.

For all those following an evidence-based approach, it’s essential to be ready for the onslaught of complaints, insinuations and abuse that comes with the territory. However, keeping to an evidence-based approach is critical to informing decisions—in the end, the evidence will win out — and the question is how many are harmed before we get there.
We’ve posted the review in full on Trust the Evidence.
Prof. Carl Heneghan is the Oxford Professor of Evidence Based Medicine and Dr. Tom Jefferson is an epidemiologist based in Rome who works with Professor Heneghan on the Cochrane Collaboration. This article was first published on their Substack, Trust The Evidence, which you can subscribe to here.
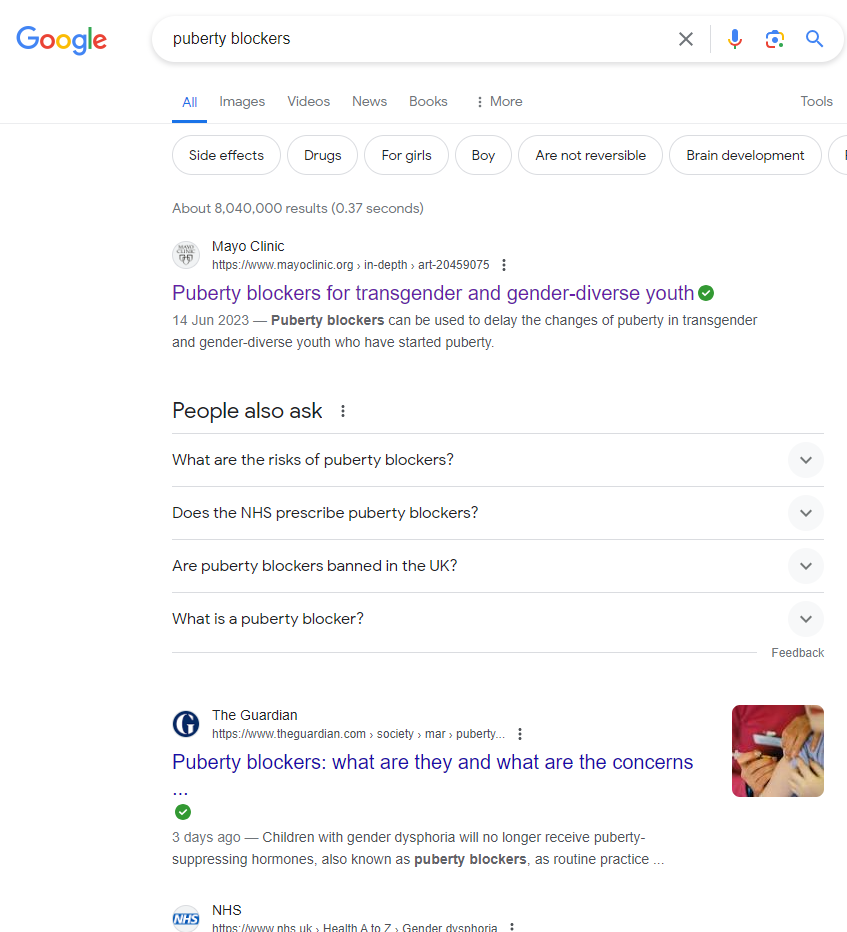
Stop Press: A Google search for puberty blockers in the U.K. brings up as the first result a pro-trans American web page from the Mayo Clinic that lists five “benefits” of puberty blockers at the top including “improve mental well-being” while side-effects are buried near the bottom. The NHS page stating that puberty blockers “are not available to children and young people for gender incongruence or gender dysphoria because there is not enough evidence of safety and clinical effectiveness” is the third result down – and barely visible without scrolling.











To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
“A Midwestern Doctor” seems to agree –
https://www.midwesterndoctor.com/p/puberty-blockers-are-incredibly-dangerous?utm_source=post-email-title&publication_id=748806&post_id=136194340&utm_campaign=email-post-title&isFreemail=false&r=x6a6a&triedRedirect=true&utm_medium=email
Just add puberty blockers to the long list of life altering/harming drugs that bigpharma shoves down one’s throat or injects into the bloodstream. And there’s always more to come.
How badly we need more people like these.
Who needs actual evidence though when you can model anything to show anything you want.
Highlight from the article (paraphrase):
One of the purposes the drugs nowadays referred to as puperty blockers were originally developed for was chemical castration of pedophiles. But their effects are certainly completely harmless and entirely reversible.
“An unregulated live experiment”
Now then. When and where have we seen this before?
Next we’ll learn that the manufacturers of these unnecessary and harmful drugs enjoy immunity from prosecution, along with everyone involved in this obvious crime against children.
“We wonder whether off-label use is appropriate …”
Off-label use is never appropriate, otherwise who needs the MHRA (a possibly tongue-in-cheek question)?
It seems to me that the best policy is to take no medications whatsoever – except for the occasional paracetamol or aspirin for a headache.
I’ve found aspirin to be entirely free of effects but not paracetamol. While its beneficial effects are disputed with some people believing they’re a mere placebo effect and nobody has an idea how it actually works (if it does), its side effect are very real and unpleasant, even when ignoring the fact that it sometimes kills people by causing spontaneous kindey failure.
When I had the broken tooth NHS wanted to prevent from being pulled really hard problem (I was obviously already trying to use a private dentist but even then, one is still subjected to NHS Make them wait! rituals) in 2020, I took paracetamol regularly, not really because it helped against the pain but because I knew it caused mild euphoria which I considered helpful in my rather depressing situation. At first, this just worked. Then, I transitioned into a situation where I would start having flashes of pain almost immediately after waking up until I started the daily paracetamol routine. I then developed a progressively worse physical restlessness which culminated in me being unable to work for about ¾ of a day due to being so restless I couldn’t manage to sit down. To counter that, I drank about ⅔ of a bottle of wine until late in the afternoon. I was then somewhat back to normal and could actually get some work done. An emergency appointment with my GP resulted in me being put on beta blockers and mild (codein) opiates. I stopped taking the latter after three days on the gounds that I positively hate coming off opiates (why that would make anyone want to take more of this shit escapes me) and eventually, got rid of the beta blockers as well. Since then, my body has thankfully recoved almost completely.
Bottom line: Never again.
But private medicine can still prescribe them?
That the NHS was being advised by WPATH is bad enough. Read the leaked files. Criminal
https://environmentalprogress.org/big-news/wpath-files