
I am a physician-epidemiologist who has consistently questioned the safety and efficacy of the COVID-19 vaccines. In the summer of 2021, I was the lead author on the first major study pointing out the risks of post-Pfizer vaccination myocarditis in adolescents. We found that the potential benefits of full vaccination did not appear to outweigh the risks in healthy adolescent males just looking at post-vaccination myocarditis risks alone. Not long after, I was senior author of another analysis published in BMJ-Journal of Medical Ethics that found the harms of the booster dose in college age students likely outweighed potential benefits by at least 18-fold. What is more, I have written multiple times about the COVID-19 vaccines being implicated in numerous deaths and have a related peer-reviewed paper hopefully coming soon. Finally, I have most recently voiced my concern about the production process of the Pfizer mRNA vaccine and the potential risks of DNA plasmid contamination to the Public Health Integrity Committee.
But if you want to bring attention to safety issues with the mRNA vaccines or other pharmaceutical products, using biased publications or prematurely jumping to conclusions is not the way to do it. We can’t complain about the pharmaceutical industry publishing biased research if we turn around and promote equally, if not more biased research about vaccine side-effects. Not only do we need scientists who are not captured by pharma, we need scientists who are not captured in general – by any ideology. We need scientists who are critical thinkers and can acknowledge limitations in data and identify inappropriate methods and causal inference.
Furthermore, avoiding inappropriately scaring people – be it about Covid or the vaccines – is good public health.
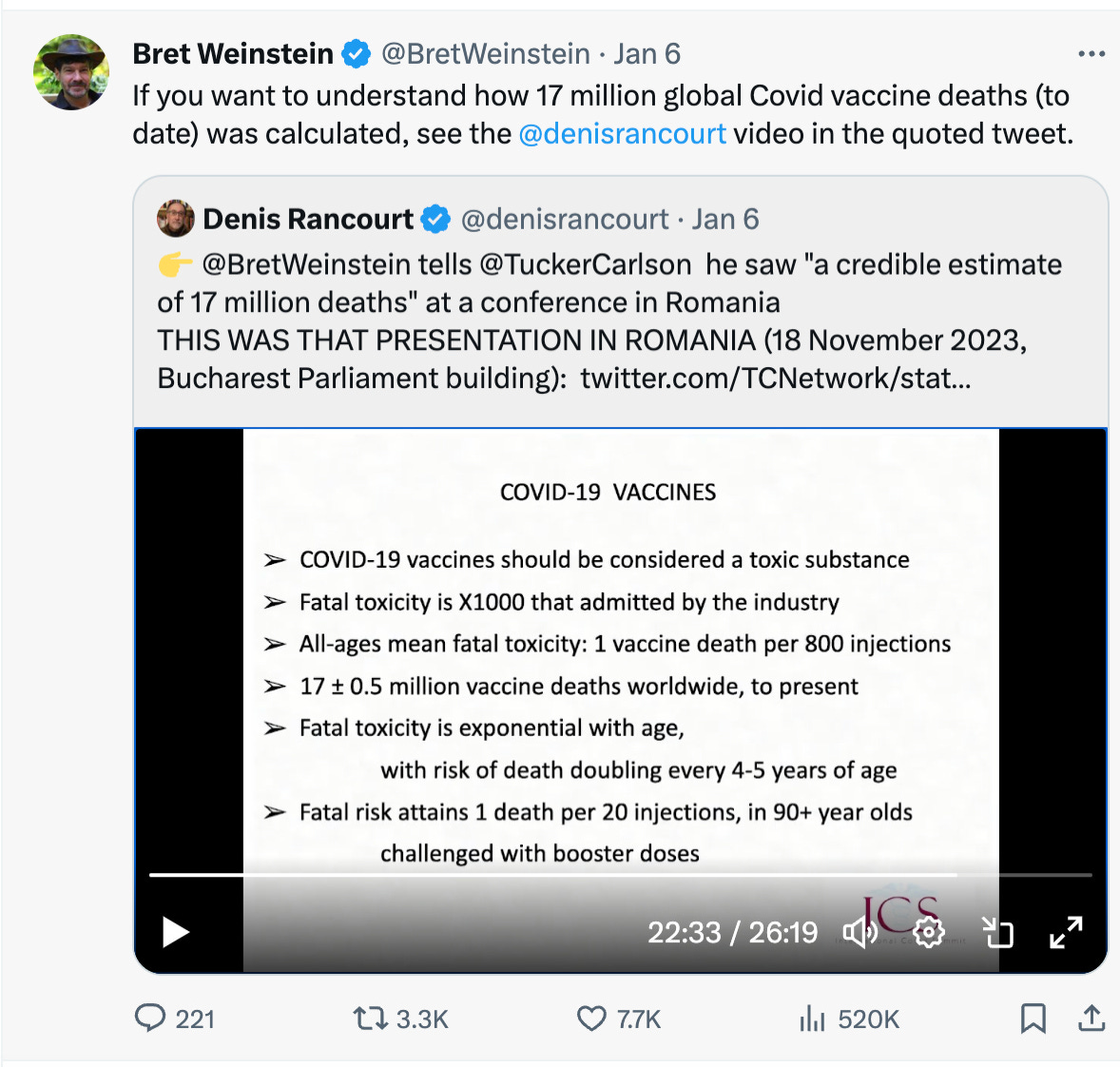
17 million deaths due to the vaccines?
Bret Weinstein (in his fascinating interview) on Tucker Carlson said he “saw a credible estimate of 17 million [deaths] globally from this technology”, meaning the vaccines. Now, this was a bit confusing since they were discussing mRNA vaccines at this moment and it was unclear if he meant all types of Covid vaccines. But I immediately thought: 1) Woah… what percent of vaccinated people would have died and how many people would that mean would have died in little, highly-vaccinated Denmark? (For those who don’t know, I am a Danish citizen). Then I thought: 2) What confounded dataset did he use to get this estimate?
But I also want to point out I found it interesting Bret did not give any sort of range in terms of potential numbers of people killed, how this estimate was arrived at or what kind of residual uncertainty there was about the estimate.
To answer the second question so you are not scrolling ahead, I quickly learned Bret was referring to this analysis by Rancourt, Baudin, Hickey and Mercier, J.: ‘COVID-19 vaccine-associated mortality in the Southern Hemisphere.’
Basic Maths/Sanity Check
If 17 million people died from “the vaccines”, that would be of course 17 million out of 8.1 billion if everyone in the world were vaccinated, or 0.21% of the population killed. But ‘only’ 5.55 billion people have been vaccinated with any vaccines, so that’s 17 million of 5.55 billion or 0.31% of all vaccinated people killed.
China with 1.5 billion people had an over 90% vaccination rate but almost exclusively did not use mRNA vaccines, so this could alter the numbers a lot depending on whether or not we are only looking at mRNA vaccines. But this analysis looked at multiple different types of vaccines, including India’s Covaxin and China’s Sinovac, so I am including all vaccinated people in the denominator, though ideally each vaccine platform should have been investigated separately.
If we just look at the country of Denmark, with 5.9 million people with an 82% vaccination rate and 0.31% risk of death per vaccinated person, this would mean about 15,000 excess deaths in this country caused by the Covid vaccines alone so far. And actually, the number would be higher because of a skewing towards an older population. (Rancourt’s analysis, as you can see in the figure above, suggests the fatality rate is one in every 20 injections for people over the age of 90!)
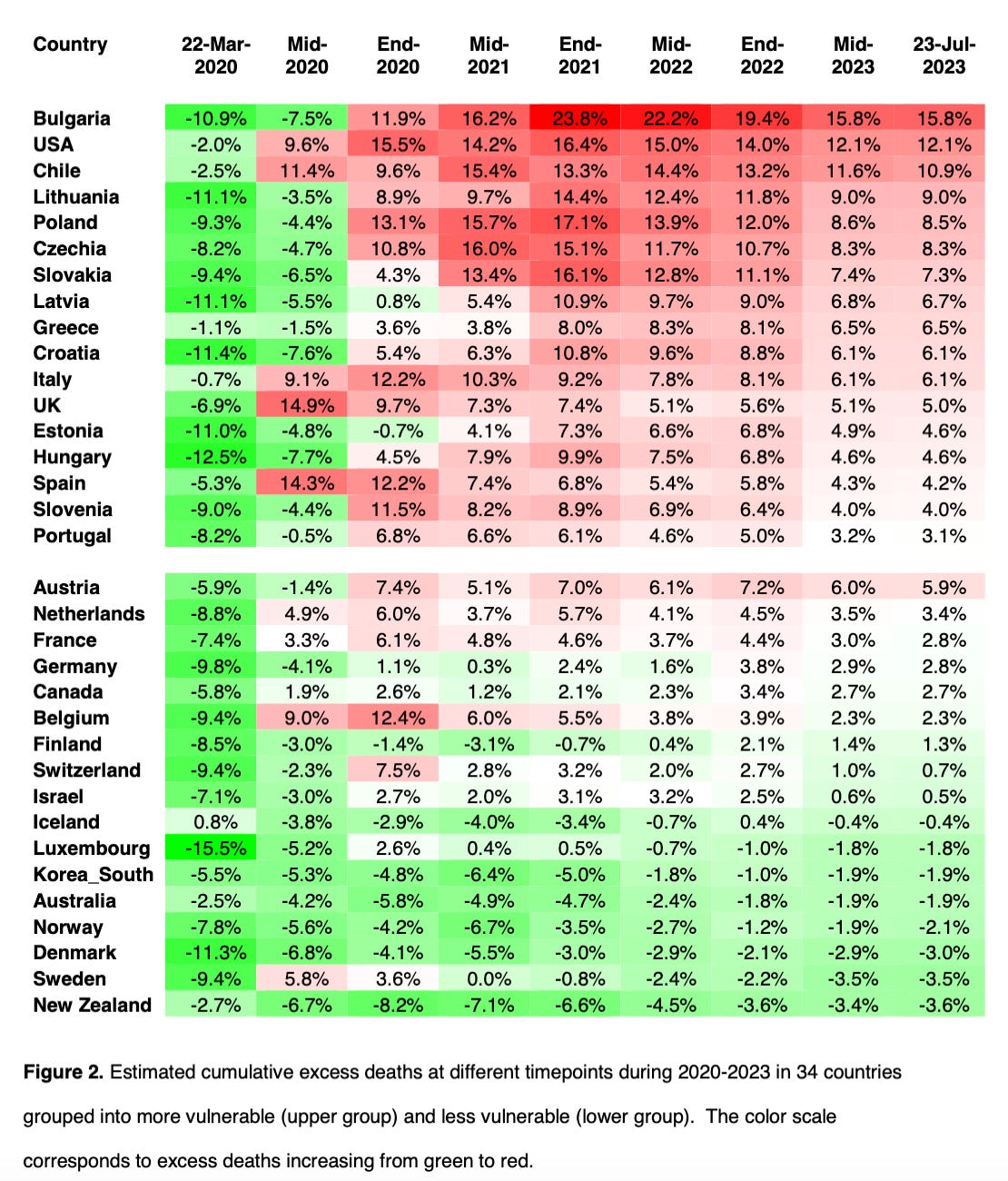
But, according to a recent analysis by Ioannidis et al., if you look at Denmark’s change in excess mortality from the second half of 2021 through 2023, there isn’t any. In fact it had fewer deaths than expected during the pandemic period. And multiple countries with relatively high vaccination rates had decreases in excess mortality from 2021-2023. In general, countries with lower vulnerability (as measured by GDP) had low to no excess death in 2021-2023.
In other words, if the excess mortality being seen across the globe right now is due to the vaccines, why are we seeing less or no excess in some of the most highly-vaccinated countries?
Now of course excess mortality depends on the baseline period you use, so estimates will differ, but if you look Denmark’s own data, it estimates around 6,000 total extra deaths from 2021 up to the start of 2023, but the peaks of the excess are in December-January and don’t correspond well with the vaccination rollout. In spring of 2021 it was seeing fewer than expected deaths. Also, interestingly it was seeing higher-than-expected deaths each winter since 2015 starting before Covid and the vaccine rollout.
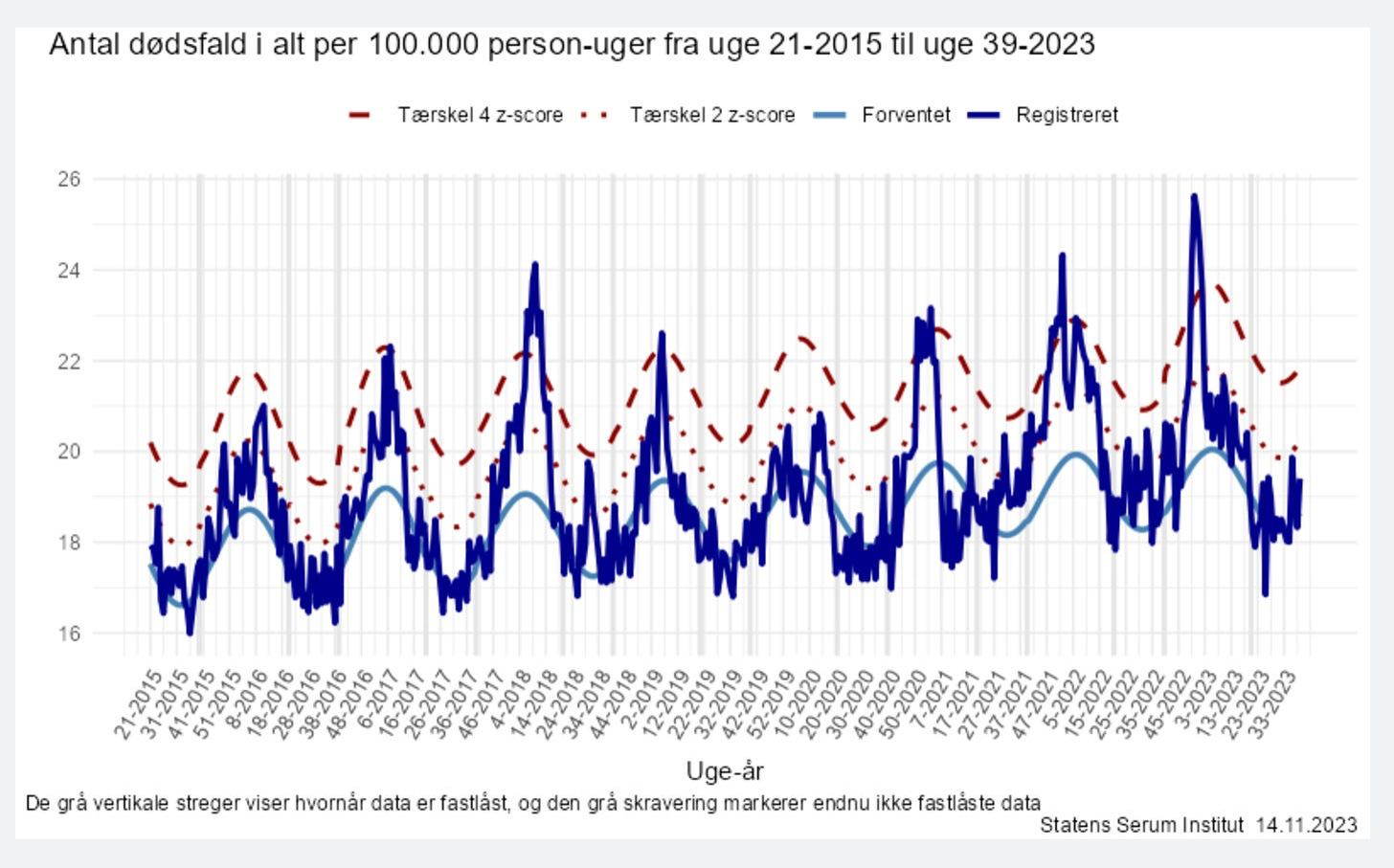
The light blue line is expected deaths and the dark blue line is observed deaths. Week numbers are on the x-axis. Antal dødsfald i alt means “total deaths in all”.
So how did the Scandinavian countries ‘hide’ upwards of 10,000 extra deaths? Did they simultaneously come up with another miracle cure that saved approximately this many lives?
In other words, this 0.3% death rate or 17 million worldwide deaths due to vaccines does not pass a basic sanity test. The other issue is correlation does not necessarily equal causation.
Analysis by Rancourt et al.
So let’s break down why the Rancourt, Baudin, Hickey and Mercier analysis Bret cited in his interview should not be used for causal inference. Note, the authors actually say “definite causal link”.
The first issue is the authors analyse only 17 countries. But why only 17 and why these 17? They don’t explain but should have. For example, why did they look at the Southern Hemisphere and not the Northern? They also did not only include countries with high vaccination rates; in fact, some have relatively very low rates of around 40%. What I am getting at is – were these countries chosen because they had excess all-cause mortality peaks that corresponded with the vaccine rollout, and were countries that didn’t excluded? In other words, was there selection bias?
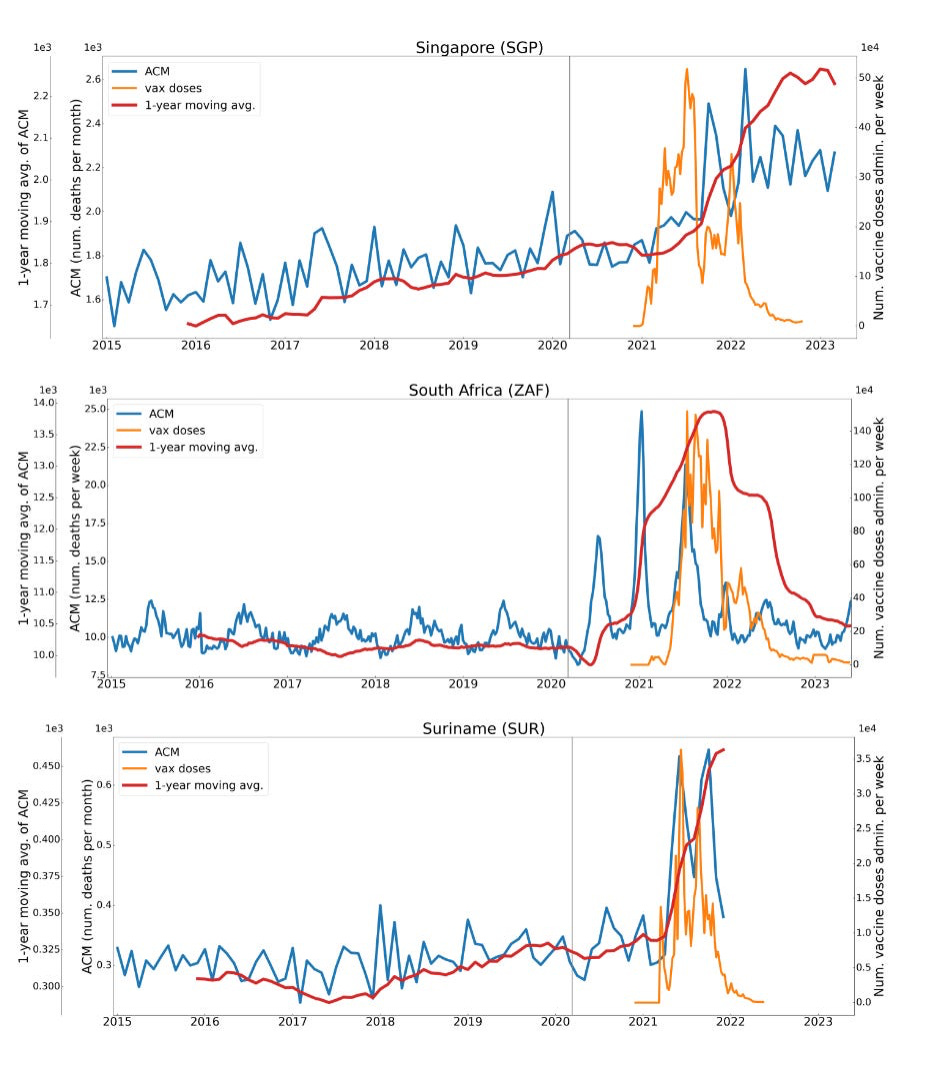
Second, you can see from Rancourt et al.’s analysis figures below, the peaks of all-cause excess mortality do not clearly correspond to the vaccine rollout nor is any association that does exist consistent in appearance and timing from country to country. The orange line is vaccine doses administered and the blue line is all cause mortality.
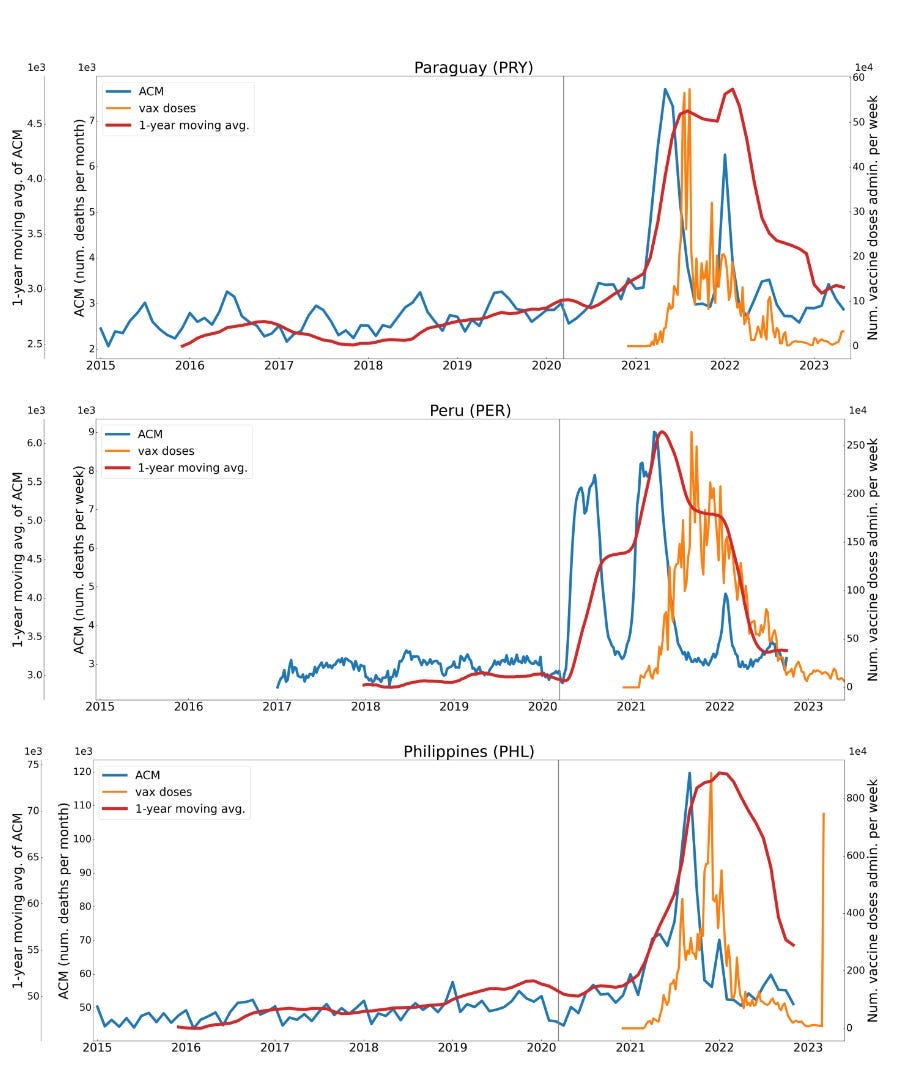
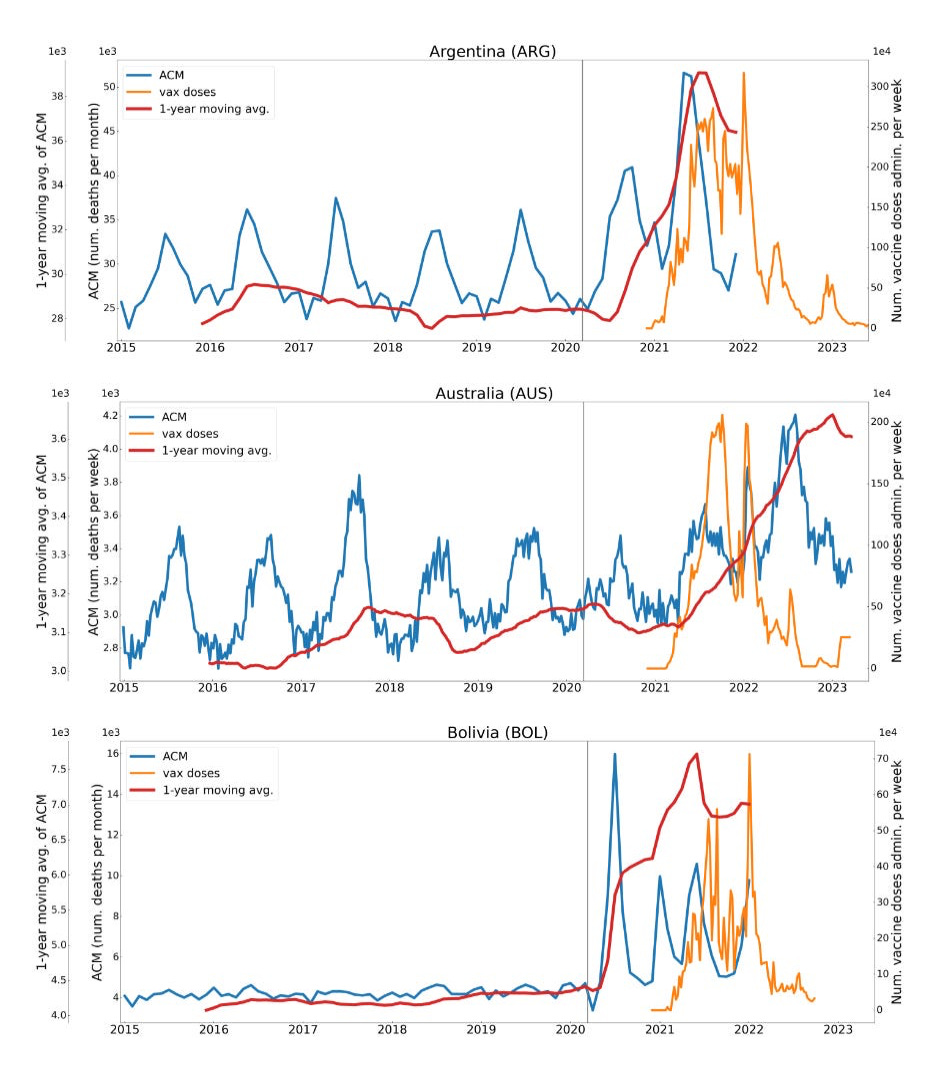
Certainly, something is going on with increasing all-cause mortality rates in these countries. But in Bolivia, Peru and Argentina it starts well before the vaccine rollout. Rancourt et al. do appropriately acknowledge this and adjust for pre-vaccine rollout increases in all-cause mortality in their analysis.
Third, many things changed across the globe shortly prior to and during the vaccination rollout: school closures, lockdowns, increased crime, depression, drug abuse, decreased sports participation, delayed medical care, job loss and increasing poverty levels across the globe.
With so many potentially impactful changes on human health occurring at once, one cannot with certainty attribute the excess deaths post-vaccination rollout to the vaccines, let alone attribute all of the excess deaths to the vaccines – but the latter is just what the authors did.
(To make it clear I am not taking political ‘sides’ here, we have seen similarly inappropriate causal inference before when studies even in NEJM inappropriately infer causality about mask wearing in schools and lower Covid infections. Or when observational studies of Covid vaccines attribute all decreases in death rates to the vaccines rather than the fact more-vaccinated people tend to have better underlying health.)
Fourth, we don’t have the vaccination status of the deceased. In included countries, such as South Africa and Suriname, which appear to have stronger correlations between vaccination rollout and excess mortality, vaccination rate is lower than the global average, at only around 40%. If a large proportion of the population that counted in the excess deaths in some of these countries was unvaccinated, that certainly speaks against vaccines being causal!
Fourth, we don’t know (or aren’t told) the causes of death. If there has been an increase in substance abuse, suicide and homicide deaths, just maybe we should not attribute those to the vaccines – or Covid for that matter.
The crazy example of India studied by Rancourt et al.
In an earlier analysis, Rancourt’s team looked at the vaccine rollout in India and concluded the vaccine rollout caused 3.7 million deaths out of 350 million doses given in India over a four-month period in the spring and summer of 2021. Because the excess all-cause mortality occurred synchronously with the vaccine rollout, the analysis does not attribute any of the excess deaths to other causes. This would have been more than one death per 100 doses given(!). Attributing all of these deaths to the vaccines interferes with an appropriately thorough investigation of what happened in India, what the causes of death were, why they occurred and how many of the deceased were in fact vaccinated. It also really detracts from the credibility of investigating vaccine-associated deaths and adverse events.
U.S. excess mortality and poverty
In another analysis by Rancourt et al., they find a very strong correlation in the U.S. between excess mortality and poverty (this is from the presentation linked to in the first image above). So if vaccinated people are more likely to be higher socioeconomic status and white, how is this finding consistent with the notion it is vaccines and only vaccines causing increases in all cause mortality? Maybe people in poverty could be dying in excess for other reasons related to all of the societal changes since March of 2020?
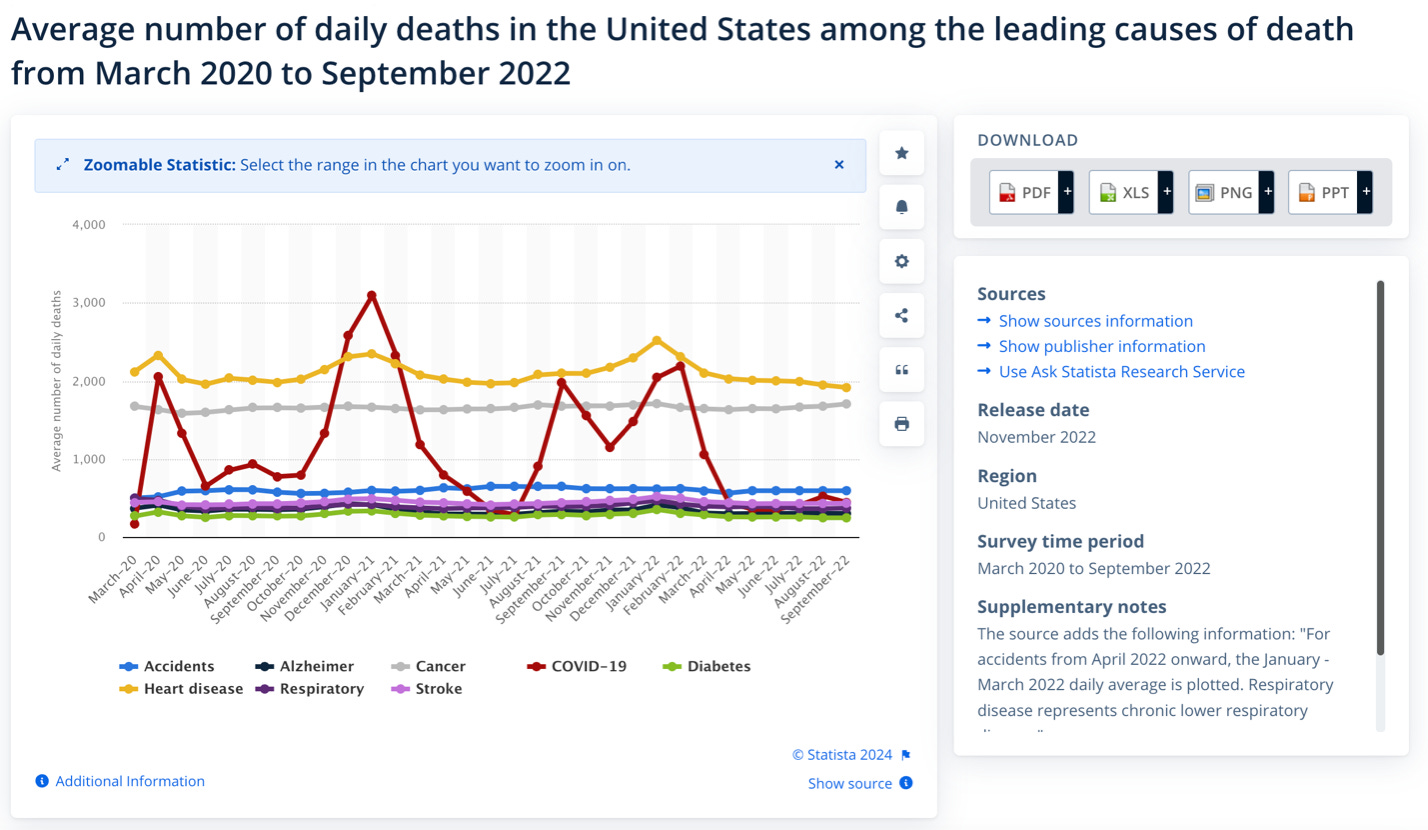
Causes of death in the U.S. since the vaccine rollout
I saw on X today a testimony from John Beaudoin saying in the U.S. causes of death “shifted to blood and circulatory” after the vaccine rollout. That alone would not give definitive evidence it was the vaccine, as, just for example, people have been gaining weight and exercising less, but that is not even the pattern the U.S. has been seeing since the vaccine rollout, as the chart below shows.
Are the 17 million excess deaths due to Covid instead?
The below figure has been circulating by ‘fact’ checkers to debunk Bret Weinstein’s claim and Rancourt’s analysis. I first saw it posted by Jeffrey Morris. Dr. Morris explains he thinks the figure shows the excess deaths can be better explained by Covid deaths than vaccination.
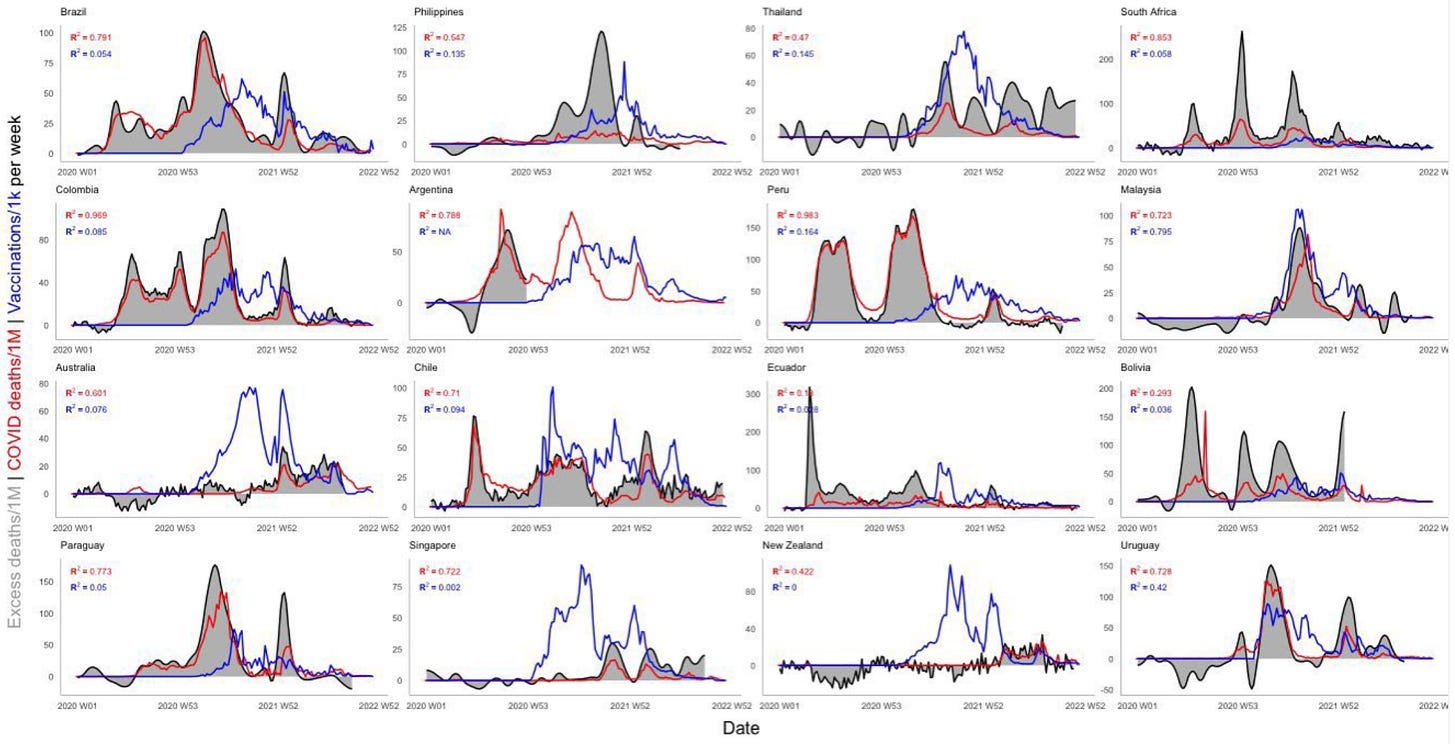
Indeed, this figure shows a calculated R2 or proportion of variance that is higher for Covid deaths and all-cause mortality than for vaccine rollout with all cause mortality. But the correlation with Covid deaths has a lot of uncertainty and I’ll explain why. When people are being admitted to the hospital with deadly conditions, they were almost always tested for Covid and the more deaths there were, the more incidental Covid deaths you would have had. So it should not be at all surprising ‘Covid’ deaths increase as all deaths increase if nearly everyone dying is being tested for Covid. I’m not saying Covid did not kill anyone but I am acknowledging the uncertainty about the amount of deaths being due to Covid. Furthermore, while it is clear peaks in all-cause mortality do not correspond as well with vaccination doses, this analysis appears to have started calculating the proportion of variance even before the vaccines started being administered, which falsely lowers the R2 for the vaccines. So, conclusions can’t be drawn from the above about Covid or vaccines in terms of causality no matter how many ‘fact’ checkers use it. But it brings up an important point that correlations or R2 does not equal causation.
Estimating how many people have been killed by the Covid vaccines
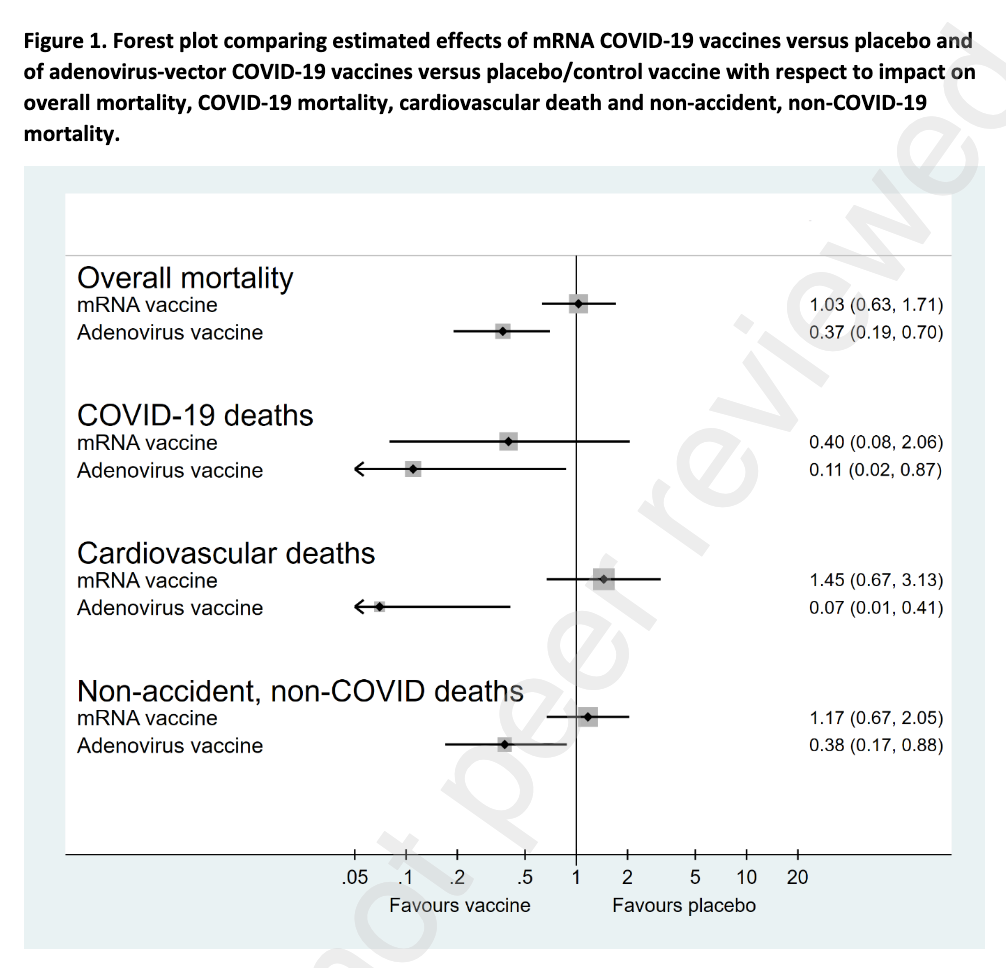
Because the Covid vaccine randomised trials were not powered to assess efficacy against all-cause mortality, establishing causal relationships between vaccination and lives saved or lost is difficult. Very difficult. One analysis of the existing randomised data by my podcast co-host Christine Stabell Benn et al. found no increase in all-cause mortality among the mRNA vaccinated but confidence intervals were wide, the follow-up was only three to six months and, we now know, the Pfizer vaccine given in the trials was not the same as what was given to the public. The adenovirus vaccines, in spite of known risk of fatality, still were found to have an all-cause mortality benefit, but the follow-up was only a matter of months.
The fact that vaccinated people tend to be healthier makes drawing conclusions about differences in all-cause mortality by vaccination status from observational studies extremely challenging. A recent excellent study of previously-infected in Austria who had received their fourth booster found a 21% decreased risk of all-cause mortality among those who had received four doses compared with those who had only received three in spite of a higher (though non-significant) risk of COVID-19 mortality. The authors, I think appropriately, attribute decreased non-Covid mortality rate to healthy vaccinee bias.
But there are still opportunities to link vaccines with death including through 1) autopsies with characteristic, rare changes in the heart or 2) in fatal conditions that are rare and clearly linked in timing to vaccination. The best example of the former is sudden cardiac death with autopsy-proven myocarditis shortly after vaccination. The best examples of the latter are fulminant myocarditis within weeks of vaccination or death from anaphylaxis or vaccine-induced thrombocytopenia and thrombosis (VITT).
Self-controlled case series (SCCS) offer another opportunity and one did find a small but non-significant signal for increased cardiac death post-second dose of mRNA vaccination in 12-29 year old males corresponding to 2.8 extra deaths per million doses given, in spite of healthy vaccinee bias. The signal was a lot clearer for 12-29 year-old females who received the AstraZeneca vaccine of 60 excess cardiac deaths per million doses of adenovirus vector vaccine.
As I described previously, the SCCS design is more amenable to causal inference as it analyses only people who died and have been vaccinated and looks at their risks pre- and post-vaccination. Because of healthy vaccinee bias, changes in health around the time of vaccination and challenges with length of the follow-up period these studies can show a causal link but quantifying it is more difficult than in randomised studies.
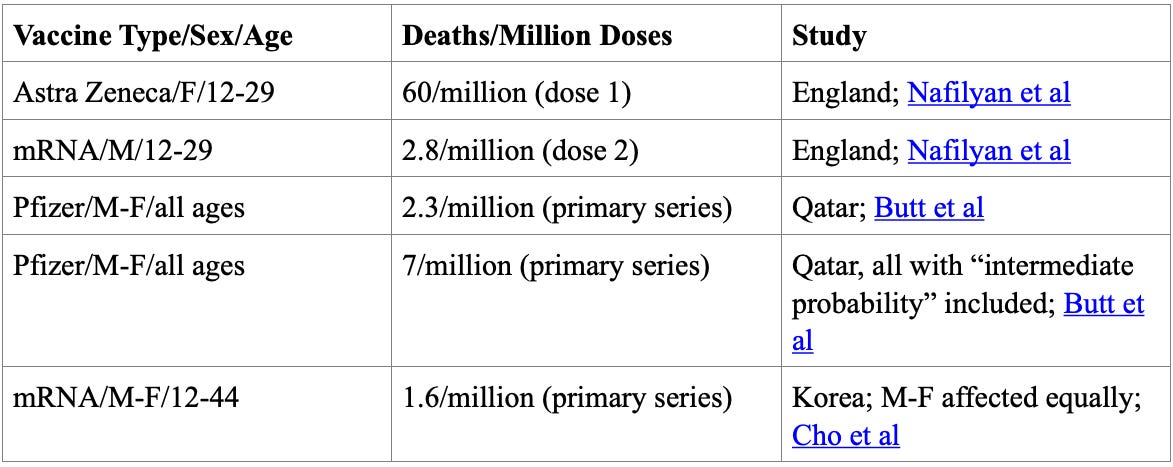
The above should be considered minimum estimates based on only the known and proven cases or on a self-controlled case series that was more likely to provide an underestimate due to healthy vaccinee bias around the time of vaccination. As the German and Korean autopsy series pointed out, a number of deaths attributed to the vaccine would have been missed had an autopsy not been performed due to sudden cardiac death shortly after vaccination.
Conclusions
I have deep sympathy for people who have lost a loved one to COVID-19 vaccination and I am dedicating this post to them. My criticism of Rancourt et al.’s analysis stems from the fact I think people are owed as accurate data as possible. In regards to my current position, I don’t think COVID-19 vaccines should continue to be used and I have made this clear publicly on multiple occasions including here. This is based on lack of evidence of efficacy and an incompletely defined risk profile.
Now I want to give quick shoutouts to Denis Rancourt and his colleagues for attempting to answer a very difficult question and inspiring this post. I am sure he will have responses to what I wrote and they are welcome. Second, I did not get into all of the parts of Bret’s interview that I loved, but I thought this tweet from Aaron Kheriaty summed up my feelings brilliantly:
Controversial claims and interpretations should lead to conversations and more data, not cancellations. Bret actually said in the interview that we need more physician scientists doing honest investigative journalism about current health issues like post-vaccination deaths and excess mortality. In that spirit, I hope this post can start a productive discussion. Please feel free to point out anything you feel I got wrong or things I should have included.
Dr. Tracy Beth Høeg is an Epidemiologist at the Department of Epidemiology and Biostatistics at the University of California, San Francisco and Associate Professor of Clinical Research at the University of Southern Denmark. This article was first published on the Illusion of Consensus Substack page. Subscribe here.
Stop Press: A debate took place last night between Denis Rancourt and Tracy Beth Høeg to look at the 17 million deaths claim. Tracy tweeted about it here.












To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
Phew. Lots of numbers, graphs, research, thanks for the work you’ve done here.
I’d be really interested to see you do a similar piece attempting to explain the huge increase (I forget the exact numbers but the increase was something like 20x above average) in professional sportspeople dropping like flies from December 2020 onwards (I believe the research I saw talked specifically about 2021 in total, even though it was obvious it was happening as the year was passing)?
I have no idea how many deaths have been caused by the Covid vaccines, but can anyone show me evidence from anywhere in the world that the Covid vaccines are safe?
I don’t personally know anyone who died because of the Covid vaccines but I personally know three people who have suffered permanent damage because of the Covid vaccines.
I read this when it first came out 2 days ago and highlighted by Steve Kirsch.
We will have to wait and see what Denis Rancourt’s rebuttal to Hoeg’s claims were.
However, if it was 17 million or 1.7 million or 170,000 deaths from the experimental jab they should be stopped NOW.
17 million dead post stabs seems low – out of the 7 billion stabbed this gives a death rate of 0.25%. I would gander that it is more likely 4-8 x that level.
How many were injured – a billion?
Hoeg – who wrote this article sounds like another pharma shill, couching her anti-anti-stabbers in graphs and numbers which mean little.
Surely she is not ‘anti vaxx’ but ‘cautious’ about the mRNA poisons…blah blah blah.
The analysis is simple. Dec 2020 they rolled out the jags. How many who were stabbed died who wouldn’t have died vs the unstabbed. The ratio is 95% vs 5%.
The data is available and easily digested (unlike this article).
I did not find this article difficult to digest – I found it less thorough than many.
Big Pharma were permitted to bring out vaccines in a tenth of the normal time and it was permitted by weak, and may I say, woke politicians who have largely indeminified these companies. The death rate per million is too high whatever it is and one of the issues that has been lost in debate is that the vaccine failed to either stop the virus or its spread.
The enemy that was as great as that was the ‘Lockdown’ policy which had a domino effect from N Italy and then China, across the world bar Sweden. That policy killed the most people and should be the one with as great an investigation as the vaccine.
Denis Rancourt has how replied to Hoeg’s criticism.
https://denisrancourt.substack.com/p/my-response-to-tracy-beth-hoegs-criticisms?publication_id=1767404&post_id=141020553&isFreemail=true&r=1ninci
“Furthermore, avoiding inappropriately scaring people – be it about Covid or the vaccines – is good public health.”
I’m not sure these two things are equivalent. The downside of scaring people inappropriately about “covid” was trillions of dollars wasted, billions of lives disrupted etc etc. The “downside” of “scaring people inappropriately” about “covid vaccines” is that they won’t take any more “covid vaccines” which have hardly been tested, are probably not safe and you don’t actually need them.
Indeed. But the real question is “Was it appropriate to scare people into taking a toxic, untested, experimental medical intervention that they did not need for a pandemic that did not exist?”
What is appropriate now is to generate enough concern in those who have taken this awful jab to do whatever they can to ameliorate the effects. There are all sorts of detox protocols being developed by authentic qualified doctors who are not compromised by big pharma. The World Council for Health is a good starting point.
Great work and good to see decent, civilised discussion, an increasing rarity these days. However, as they are still being pushed, even mandated in some countries, I have a horrible feeling that despite all the evidence and despite all the calls for the jabs to be withdrawn, the concept of jab-induced immune damage, illness and death is becoming worryingly normalised. Is it because we’ve had decades of psy-ops indoctrination & media propaganda giving Big Pharma so much slack on drug and vaccine harms (thalidomide, guardasil, fentanyl, rotavirus, swine flu, etc) that we’re becoming inured to it? It wouldn’t surprise me in the slightest, given the massive increase in mRNA platform development for drugs right across the board despite its inherent and so far unresolved problems. If so, it does not bode well for humanity.
17 million excess deaths.
All I know I’ve never seen so many ambulances and hearses.
Lets not forget on Ted Talk in about 2010 Bill Gates said that he wanted to reduce the worlds population by 10-14% using …. guess what ….
Why are so many minor celebrities under 60 dying suddenly?
Microsoft Windows 11 updates?
I yield to no one in my contempt for Gates, but repeating this does our credibility no favours. What Gates meant was that if people in less developed countries had access to vaccines, then infant mortality would fall and they would not feel the need to have very large families (i.e. to guarantee someone would be there to look after them in their dotage).
Now we may not agree with his many assumptions here, but the idea that he accidentally let slip his demonic plan to reduce the world population by lethal injection is a little ridiculous.
I would tend to agree.
Below is a link to one of his blog posts, from 2016.
I do not know how anyone with at least one iota of normal life experience could read it and not realise that – in very many respects – he is a complete fool.
https://www.gatesnotes.com/Smells-of-Success
Sadly, he is a very rich fool. Problem, that.
I’m sure a lot of us have anecdotal stories about deaths and injuries.
Since the jabs were rolled out four people on my small Estate (with about 24 residents) have had strokes: three are dead, one is in a bad way and has now gone to a Care Home.
Two other neighbours have developed undiagnosed, debilitating neurological problems.
Husbands of two friends (both late middle age) have had heart attacks. One of them had another booster and shortly afterwards another heart attack; he is now semi-disabled.
Five acquaintances have developed cancers; three dead, one terminal, one is receiving treatment and may survive.
Then there’s a litany of friends and acquaintances who have recently had various medical problems requiring treatment: blood clots; an undiagnosed neurological disorder; a liver problem which required surgery; plus the usual “I’ve got Covid again; I feel awful; I don’t know what’s wrong with me, I never feel well.”
Something doesn’t add up here. The table above shows that New Zealand has never had any excess deaths. Every other source has shown NZ has been suffering a huge number of excess deaths. Ditto Australia, Israel etc etc.
Also every article I’ve seen shows an absolute coincidence between the introduction of vaccines and excess deaths in the following weeks. Suddenly that’s not the case?? It certainly was the case in early 2021 in the UK.
Finally Denis Rancourt provides a clear explanation as to why he choose the Southern Hemisphere countries that he did. (I believe it was to use their ‘summer data’ when flu should be low). If this author hasn’t found that out I expect she hasn’t looked very hard.
So even with a cursory glance, there seems to be significant issues with this narrative.
There is, of course, more to this matter than vaccine mortality.
The vaccines, covid and influenza, give rise to Giant Cell Arteritis (GCA).
The corticosteroid treatment of GCA can cause severe dementia.
‘The most important and common complications are cerebrovascular disorders including cerebral venous sinus thrombosis, transient ischemic attack, intracerebral hemorrhage, ischemic stroke, and demyelinating disorders including transverse myelitis, first manifestation of MS, and neuromyelitis optica. These effects are often acute and transient, but they can be severe and even fatal in a few cases.’
A review of neurological side effects of COVID-19 vaccination, Feb 2023
‘Studies have investigated the mechanism by which mRNA vaccines induce GCA; the onset of this condition is attributed to cross-reaction of produced antibodies with tissues. In addition, conventional GCA, SARS-CoV2 infection, and adverse reactions after vaccination against SARS-CoV2 promote excessive production of interleukin-6, which may be involved in the pathogenesis. Therefore, the use of an mRNA vaccine against SARS-CoV2 may be linked to the development of GCA.’
Development of giant cell arteritis after vaccination against SARS-CoV2: A case report and literature review, June 2023
‘Our brief narrative review confirms that a steroid dementia syndrome exists. According to several experts’ opinion, steroid dementia syndrome is an overlooked diagnosis.’
Does a steroid dementia syndrome really exist? A brief narrative review of what the literature highlights about the relationship between glucocorticoids and cognition, 15 March 2023
‘“I was excited to know someone did this study that really validates what we’ve known for a long time — that steroids cause brain atrophy and a lot of neuropsychiatric symptoms or side effects,” he stated.’
Prescription steroids affect brain structure, study finds, Medical News Today 06 Sept 2022
The paper “COVID-19 Vaccine-Associated Mortality in the Southern Hemisphere”, by Denis G. Rancourt, Marine Baudin, Joseph Hickey, and Jérémie Mercier, can be found here:
https://denisrancourt.ca/entries.php?id=133&name=2023_09_17_covid_19_vaccine_associated_mortality_in_the_southern_hemisphere
Dr. Tracy Beth Hoeg questions why Rancourt’s team analysed only 17 countries and why these 17, and why did they look at the Southern Hemisphere and not the Northern?
Rancourt’s paper analyses mortality data from almost all the South American countries, as well as South Africa, Australia, New Zealand and some southern equatorial countries, i.e. a comprehensive and representative selection. Those countries were presumably chosen because they had reliable and publicly available statistics covering the period of analysis. Seventeen is, in my opinion, a large enough selection if resources are limited. Finally, Denis Rancourt has already published papers analysing northern hemisphere countries: USA, Canada and France.
I have copied Denis Rancourt’s abstract to the paper below, which describes how the 17 million number was calculated. Further details are naturally in the paper itself.
Seventeen equatorial and Southern-Hemisphere countries were studied (Argentina, Australia, Bolivia, Brazil, Chile, Colombia, Ecuador, Malaysia, New Zealand, Paraguay, Peru, Philippines, Singapore, South Africa, Suriname, Thailand, Uruguay), which comprise 9.10 % of worldwide population, 10.3 % of worldwide COVID-19 injections (vaccination rate of 1.91 injections per person, all ages), virtually every COVID-19 vaccine type and manufacturer, and span 4 continents.
In the 17 countries, there is no evidence in all-cause mortality (ACM) by time data of any beneficial effect of COVID-19 vaccines. There is no association in time between COVID-19 vaccination and any proportionate reduction in ACM. The opposite occurs.
All 17 countries have transitions to regimes of high ACM, which occur when the COVID‑19 vaccines are deployed and administered. Nine of the 17 countries have no detectable excess ACM in the period of approximately one year after a pandemic was declared on 11 March 2020 by the World Health Organization (WHO), until the vaccines are rolled out (Australia, Malaysia, New Zealand, Paraguay, Philippines, Singapore, Suriname, Thailand, Uruguay).
Unprecedented peaks in ACM occur in the summer (January-February) of 2022 in the Southern Hemisphere, and in equatorial-latitude countries, which are synchronous with or immediately preceded by rapid COVID-19-vaccine-booster-dose rollouts (3rd or 4th doses). This phenomenon is present in every case with sufficient mortality data (15 countries). Two of the countries studied have insufficient mortality data in January-February 2022 (Argentina and Suriname).
…
Synchronicity between the many peaks in ACM (in 17 countries, on 4 continents, in all elderly age groups, at different times) and associated rapid booster rollouts allows this firm conclusion regarding causality, and accurate quantification of COVID-19-vaccine toxicity.
The all-ages vaccine-dose fatality rate (vDFR), which is the ratio of inferred vaccine-induced deaths to vaccine doses delivered in a population, is quantified for the January-February 2022 ACM peak to fall in the range 0.02 % (New Zealand) to 0.20 % (Uruguay). In Chile and Peru, the vDFR increases exponentially with age (doubling approximately every 4 years of age), and is largest for the latest booster doses, reaching approximately 5 % in the 90+ years age groups (1 death per 20 injections of dose 4). Comparable results occur for the Northern Hemisphere, as found in previous articles (India, Israel, USA).
We quantify the overall all-ages vDFR for the 17 countries to be (0.126 ± 0.004) %, which would imply 17.0 ± 0.5 million COVID-19 vaccine deaths worldwide, from 13.50 billion injections up to 2 September 2023. This would correspond to a mass iatrogenic event that killed (0.213 ± 0.006) % of the world population (1 death per 470 living persons, in less than 3 years), and did not measurably prevent any deaths.
…
She didn’t manage to convince us that the Jabs are actually safe & effective did she ! 17 million maybe a worst case scenario but even if it’s miles out it’s still heinous ! Also if she’s proved right & it’s only say, half that number then it’s ok is it ! NOT …!!!
She did not say that at all.
She wants these products off the market.
There is a debate about how many deaths were caused by these vaccines. I like her thought process. It is not simple. Have been looking at Sweden’s data and in this highly vaccinated country we have not seen the levels of excess deaths. Now this does not prove anything, but I agree with the author that more work is needed.
Could the batches used be relevant to where deaths/injuries from the vaccine occurred?
Thank you for this excellent article.
i think we can only work this out by analysis of vaccinated and non-vaccinated groups. And we need large numbers. Using the VAX-Control group (https://vaxcontrolgroup.com/) may be good, but ideally public health data from multiple countries should be used.
i do challenge the healthy vaccine bias. You could argue that people who are more health conscious were more likely to do research before being vaccinated and reject vaccination?
I also think the emphasis on deaths and cardiac related issues may miss important other side-effects.
The fact of the matter is that these jabs ARE causing injury and death and as Andrew Bridgen pointed out in his recent speech on excess deaths other vaccines have been “pulled” with far far fewer deaths occurring.
Just stop the bloody things now!
The most important conclusion to be drawn from this article is that “Controversial claims and interpretations should lead to conversations and more data, not cancellations.”
Thank you to The Sceptic for publishing this article by somebody who clearly understands the complex statistics involved and who hopefully does not have any vested interest in one or other side of the debate.
What we have needed from the outset is open and honest debate not unqualified “fact checkers” and cancellation of legitimate research, analysis and observations in MSM, social media and medical and scientific journals. We have not needed pharmaceutical representatives, scientists, doctors and advisers dependent on funding from those with a clear vested interest, global organisations funded by those with an obvious agenda, charitable funds heavily invested in the pharmaceutical industry etc presenting a one sided narrative and cancelling and censoring debate.
We have never needed the completely unethical mandates. We have always needed policies to be determined on the basis of a thorough risk benefit analysis. Legally valid informed consent should never have been abandoned. Policies should always have been based on the precautionary principle and the dictum of primum non nocere. Doctors should not have been silenced and threatened with erasure from the medical profession.
Need I go on?
Bravo to the Daily Sceptic for publicising a genuine, sincere, article from sceptic-through-to-her-bones Dr Hoeg. Really enjoyed reading this intelligent critique of a great interview.
I don’t pretend to understand all of this …. but I am quite relaxed about someone challenging a scientific/evidence-based theory on the basis of another scientific/evidence-based theory.
What I refuse to accept are the blatant lies spouted by the Covid Propagandists which are not scientific or evidence-based ….. and which refuses to admit or address the issue that the experimental jabs have clearly had significant harms for a great many people.
Before even looking at the detail, one thing which is blatantly obvious is that this particular researcher has taken the published average deaths to determine expected mortality WHICH INCLUDES the inflated excess figures and does not consider either that one would expect mortality to decrease after an alleged pandemic of significance. You cannot state that there are marginal decreases when the figures you are using are inflated!
Having now had time to read Denis Rancourt’s original paper, I am afraid Dr. Tracy Beth Hoeg’s critical article does not take Rancourt’s earlier papers nor his current conclusions into account.
Hoeg firstly displays only 9 of Rancourt’s 17 graphs (possibly due to lack of space) showing mortality against vaccine rollout, stating that “the peaks of all-cause excess mortality do not clearly correspond to the vaccine rollout nor is any association that does exist consistent in appearance and timing from country to country”.
As I wrote in my above post, Rancourt states in his paper that “Nine of the 17 countries have no detectable excess ACM in the period of approximately one year after a pandemic was declared on 11 March 2020 by the World Health Organization (WHO) …”. This alone is a clear indication there was no deadly virus circulating in those countries.
Concerning this pre-vaccination period (from WHO declaration of a pandemic to vaccine rollout), Rancourt writes, “We attribute this [mortality] variability in the pre-vaccination period to large country-to-country differences in aggressive medical and government measures, convoluted with underlying population structures of fragile individuals, similarly to the large state-to-state differences in the USA …”. As in UK and many other countries, governments emptied hospitals, cancelled operations, locked residents in care homes, etc., which is clearly not beneficial to prolonged health.
Then, “By comparison, the patterns and magnitudes of ACM by time are relatively consistent, from country to country, in the vaccination period (Figure 6): all 17 countries have significant excess ACM in the vaccination period, virtually all 17 countries have large peaks of excess ACM in early-2021 when the COVID-19 vaccines are first rolled out, followed by a peak in excess ACM in early-2022 (the nominally January-February 2022 peak) when boosters are rolled out.”
In summary, “We attribute this relative constancy from country to country of excess ACM by time of the vaccination period as being due to the large uniformity in timing of COVID-19 vaccine and booster rollouts across the 17 countries; whereas medical and government measures were generally more disparate in the pre-vaccination period.”
The possibly two main points of Rancourt’s 180-page paper are:
(1) Absence of excess mortality until the COVID-19 vaccines are rolled out and
(2) The COVID-19 vaccines did not save lives and appear to be lethal toxic agents.
The first point is repeated in all his papers, i.e. that mortality comparisons between neighbouring countries, states and provinces repeatedly show THERE WAS NO PANDEMIC.
His second point is, I think, expressed lightly!
Thank you for doing this. It is e trembly important to get the facts. Confirmation bias on both sides is a huge problem.
Terribly important
Dennis Rancourt has now replied to Hoeg’s criticism.
https://denisrancourt.substack.com/p/my-response-to-tracy-beth-hoegs-criticisms?publication_id=1767404&post_id=141020553&isFreemail=true&r=1ninci