
Australia is an important control group because it had minimal Covid prior to Omicron at the end of 2021. Therefore the effects of the vaccine alone on the population can be deduced by what happened there in 2021.
There are two key points to note. Firstly, there was a lack of respiratory deaths in 2020, 2021 and even 2022. Any analysis of excess mortality needs to account for that. Secondly, many of the excess deaths were not included in the major categories of death.
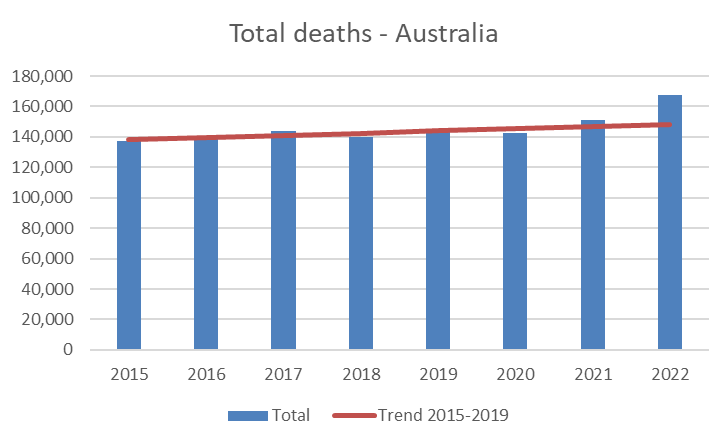
Total deaths
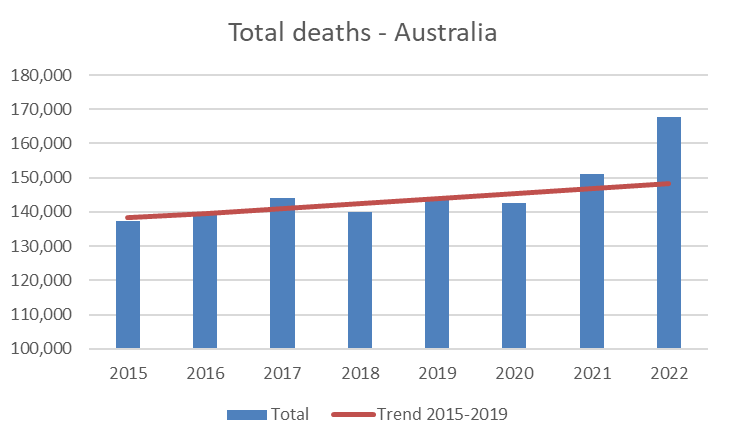
Total mortality was lower in 2020 and higher in 2021 than expected levels (see figure 1). Figure 2 shows the same data with an adjusted y-axis to show that these differences were not insignificant. For 2021, there were 4,145 excess deaths in 2021 whereas there were only 1,224 deaths attributed to Covid.
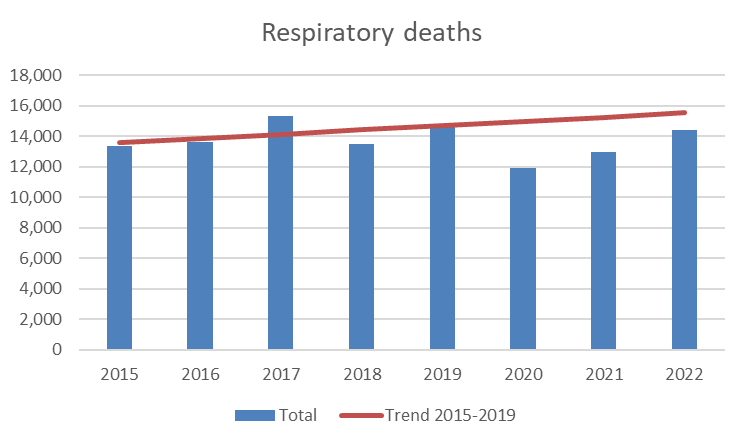
Respiratory Causes of Death
In 2020, deaths from respiratory causes plummeted. This is likely to be because of the disappearance of influenza from 2020. In 2021, the same was true. Clearly, any assessment of excess from other causes needs to account for this deficit. The deficit was 3,078 in 2020, 2,273 in 2021 and 1,130 in 2022. The 4,415 total excess in 2021 is therefore likely to represent a true excess of 6,688 when the deficit in respiratory deaths is taken into account, which would be a 4.5% increase in all deaths and 3.7% excess in non-Covid deaths.
Uncategorised deaths
As always with such datasets, the data of interest are not apparent at first glance. After removing the major categories of cancer, circulatory, respiratory and dementia deaths, the uncategorised non-Covid deaths show a significant increase above expected levels. There were 2,841 such excess deaths in 2021 and 6,238 in 2022. It would be interesting to know how many of these were sudden unexpected deaths. In England and Wales, such deaths are categorised as “symptoms, signs and ill defined conditions” and accounted for the largest group of non-Covid excess deaths from March 2020 to June 2022.
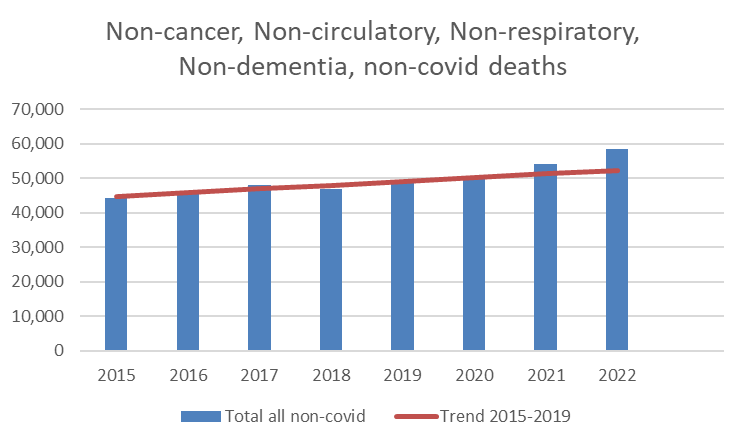
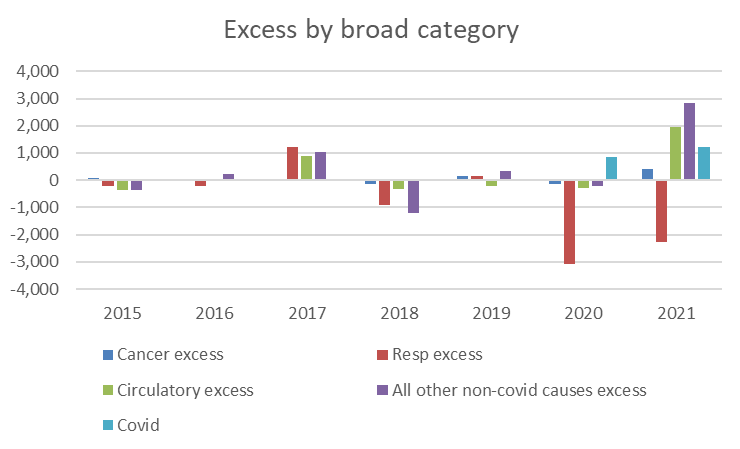
Figure 5 shows that in 2021, the 1,224 deaths attributed to Covid were far fewer than the deficit in respiratory deaths from other causes. In the meantime, circulatory deaths and ‘other’ deaths were substantially higher, amounting to a combined excess of 4,776.
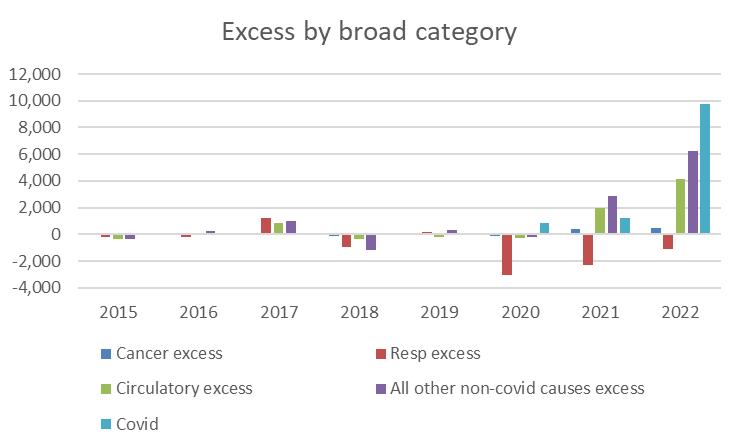
In 2022, deaths attributed to Covid reached 9,735 while these circulatory and ‘other’ deaths escalated further accounting for 10,403 deaths. Taken together, there were four excess circulatory and other non-Covid causes of death for every death attributed to Covid in 2021, whereas in 2022 these were of equal magnitude. Anyone wanting to dismiss these deaths as under-diagnosed Covid needs to explain, first, why diagnosis failed and secondly why this ratio was so dramatically different in 2021 to 2022.
Major causes of death
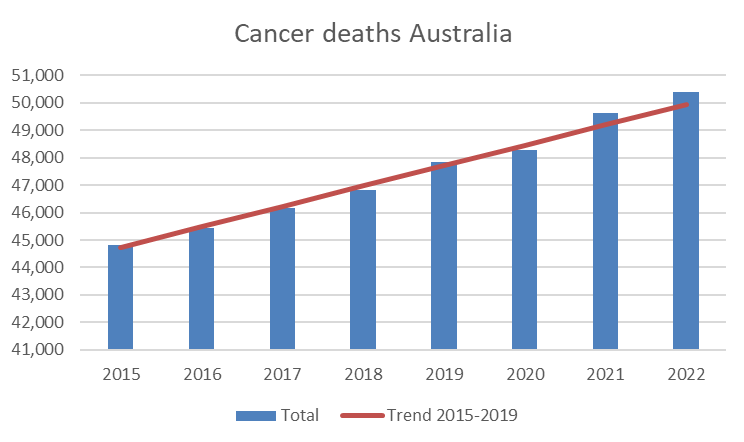
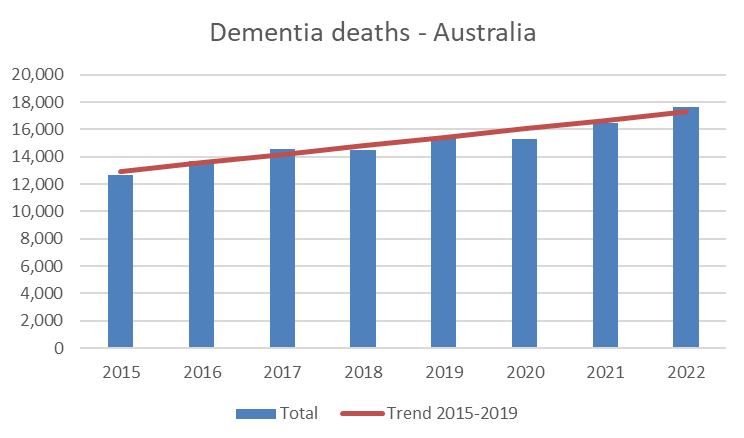
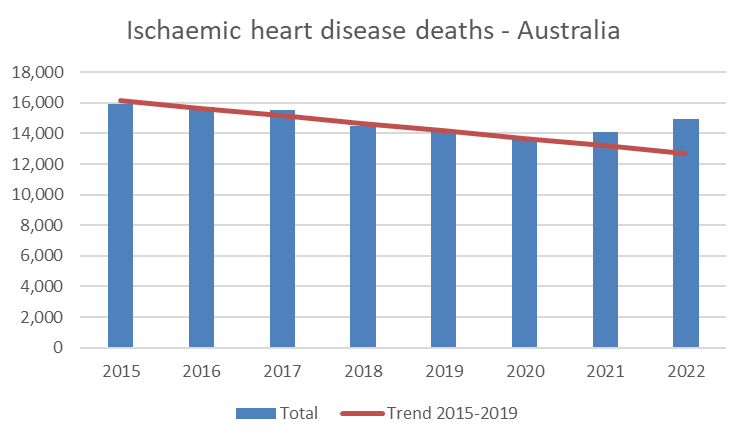
The 2015-2019 trendline provides a very accurate prediction for deaths from cancer (figure 3) and deaths from dementia (figure 4) indicating that it is a reasonable method to use for assuming a baseline.
Ischaemic heart disease deaths were in excess of expected levels, with 876 extra deaths. (Remember there were only 1,224 deaths attributed to Covid.)
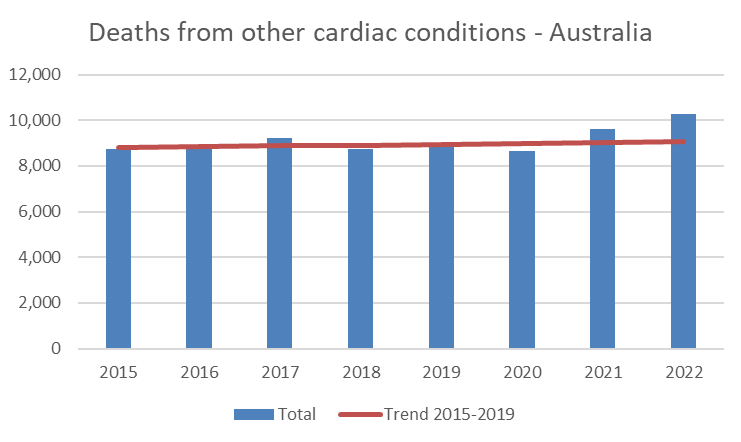
Similarly, deaths from other cardiac conditions were also in excess, with 583 extra deaths in 2021.
Unlike other causes of death, deaths from strokes showed a declining trend until 2021, when there was an excess of 476 deaths.

Deaths in Australia exceeded expected levels from 2021, well in excess of what could be attributed to Covid. The excess was part circulatory disease, while many deaths did not fall into the main categories of deaths.
These data from the Australian ‘control’ group, where Covid was not a major factor until 2022, underline concerns about the role Covid vaccines may be playing in global trends in excess deaths.
Dr. Clare Craig is a diagnostic pathologist and Co-Chair of the HART group, where this article first appeared. She is the author of Expired – Covid the untold story.












To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
I interpret The Australian statistics of mortality as follows. The initial wave of Covid 19 was not responsible for excessive deaths and I would suggest that the Vitamin D status of The Australian population could have been the reason . Subsequent mortality did increase coinciding with the introduction of the vaccines and increases in mortality by heart and circulatory failure might therefore be due to either , Covid 19 infection or vaccine damage . We in Britain saw an upsurge in deaths in 2021 . The expectation of vaccination would be that deaths should decline . We observed the opposite . It might therefore be logical to conclude that vaccination was promoting mortality .
The other reason for deaths to be reasonably expected to decline in 2021 was those pulled forward by Covid among the vulnerable. Double reason to expect fewer, not more.
And the fact it was a seasonal virus, so its activity would naturally fall away February/March as it did in 2020 and other respiratory viruses, like ‘flu, do.
However, once vaccination had reached a significant number, it lost its seasonal nature and became year round. That was the direct result of the mRNA juice.
This is where the skeptics get it wrong.
To believe in Covid you have to accept absurdities. Like believing that this virus couldn’t be bothered with Australia in 2020, that this virus can detect skin colour, that this virus can tell if you’re swedish, that it can observe national borders, that following arrows on the floor is protection and that flu (an illness 100% identical to Covid) was replaced by Covid (an illness 100% identical to Flu).
There is a very simple explanation for these absurdities: Covid never existed. The only place it does exist, is in the mind.
Continue to accept the absurdities of Covid 19 and the criminals will bog the skeptics down in trench warfare for centuries to come.
The skeptics are going to have to swallow their pride (that they believed it too) and understand that these excess deaths would look unambiguously catastrophic, and undeniable, if Covid was taken out of the equation.
The lack of flu deaths in 2020/21 in itself is interesting. Was it genuinely an extremely mild flu year, or where flu deaths misattributed to Covid-19?
Nearly all deaths were misattributed to the coof.
Following an overly sensitive PCR test (40+ cycles) any death within 28 days was recorded on that ominous death-ticker shown on every (so-called) news program.
Nosocomial ‘cases’ – caught or testing positive in hospital.
Iatrogenic deaths – caused by medical treatment, such as excessive use of ventilation.
People still think 160k or more dropped dead from coof. It was far, far fewer.
Or, as a contributor on here mentioned at the time, was covid a cure for the flu?!!
“This is likely to be because of the disappearance of influenza from 2020. In 2021, the same was true. “
Oh?
The proferred explanation for the alleged absence of influenza was competition from CoV 2, but if the latter was absent from Australia in 2020 until the end of 2021, then whilst that explanation could be the case elsewhere, it cannot apply in Australia.
Explanation needed please.
Could the truth be influenza did not disappear, but testing for it stopped, replaced by the obsession for testing for CoV 2 ?
In fact on this site… https://www.worldlifeexpectancy.com/selected-deaths-vs-covid-19-australia
… it is showing over 9 000 deaths from influenza and pneumonia (respiratory diseases) 2020 to end 2021.
The same site shows over 80 000 ‘flu & pneumonia deaths 2020 to end 2021 in the UK when supposedly there were none.
Somebody is telling porkies it seems.
Worth remembering all respiratory deaths end up as pneumonia.
I can’t bring myself to care about excess mortality especially if it’s caused by the covid jabs.
The way I see it is that people made their decisions and that’s it. Those who didn’t take the jabs paid for the consequences at the time, those who did may have to pay for the consequences after.
We all have to live with the consequences of our decisions.
I will just say “informed consent” and “coercion”.
It’s one thing to decide for yourself on the known evidence, it’s entirely another to feel that you must comply with what effectively became an instruction to have the Covid-19 mRNA experimental gene therapy or lose your job.
Standing up for oneself isn’t always easy.
I saw plenty of images of people sacrificing their jobs to defend their personal and physical integrity. And of course it must have been a very hard thing to do. Which would have been made a lot easier if the majority would have done the same, or even just stood up for them.
When I watched images of doctors and nurses being escorted out of hospitals for refusing covid jabs, the whole thing had a whiff of the Jews being marched out of their apartments while their longtime neighbours looked on passively.
I realise it’s a bummer for people who are jabbed each time an article like this comes up. It must be pretty uncomfortable. I’m not happy for them. But I’d lie if I said I had much sympathy either.
Are these worldwide excess deaths significant enough to make a difference in policy and business decisions by governments and insurers, for example? Are they willfully being ignorant when it comes to mortality tables and pension shortfalls (or maybe gains)? It seems that excess deaths would make some difference but maybe with increased migration the effects are not as evident, say in housing or purchases normally made by middle-class people who took the jabs to keep their jobs?
It could be on the agenda for those who do actuarial assessments for pension schemes. In recent years, they have been concerned about rising life expectancy figures, leading to requirements for increased contributions to achieve agreed benefits etc.
Is Australia also seeing increased disability claims that other nations are seeing? Do increased disability claims, with government payments to claimants and decreased taxes paid into the system, counteract decreased pensions due to excess deaths? Increased disabilities often mean that family members will need to quit working or retire to provide care, so that’s even fewer tax monies into the system.
Thank you for all your hard work and honesty in the insanity of the last almost 4 years.
I wonder why you’re no longer on the BBC?. Lol.
Please keep going and thanks for the book.
One of several differences between UK and Australian Covid statistics, is surely the fact that Australia has a pretty good idea what the denominator (total population) was and is.
In the UK, the quoted figures for the size of the population varies wildly, for reasons that are absolutely clear.
“…[Australia] had minimal Covid prior to Omicron at the end of 2021…”
Everywhere had minimal COVID. That is, the symptoms of SARS-COV-2 infection.