
During the 24 weeks from March 24th 2023 to September 1st 2023 there were 32,130 registered deaths due to heart failure in England. In 2020 we had expected 25,512 heart failure deaths during the corresponding weeks, a difference of 6,618. If we extrapolate to 52 weeks then, at the prevailing rate, we’ll see 14,339 more deaths from heart failure in 2023 than we expected in 2020. To put this in some kind of perspective, that’s equivalent to the total number of deaths from all causes in Lancashire in any single year, or, if you’re not familiar with Lancashire, it’s about the same as the total number of deaths in Devon and Cornwall in a single year.
Deaths from heart failure over the past 24 weeks have been 26% higher than the expected level in 2020. The source of this rather alarming statistic is the latest report from the Department for Health Improvement and Disparities.
However, it doesn’t report it in quite the same way. It compares heart failure deaths in 2023 with ‘expected’ heart failure deaths for 2023, without mentioning that ‘expected’ heart failure deaths in 2023 are 8% higher than in 2020. Inflation affects heart failure deaths just as much as it does the pound in your pocket, it seems!
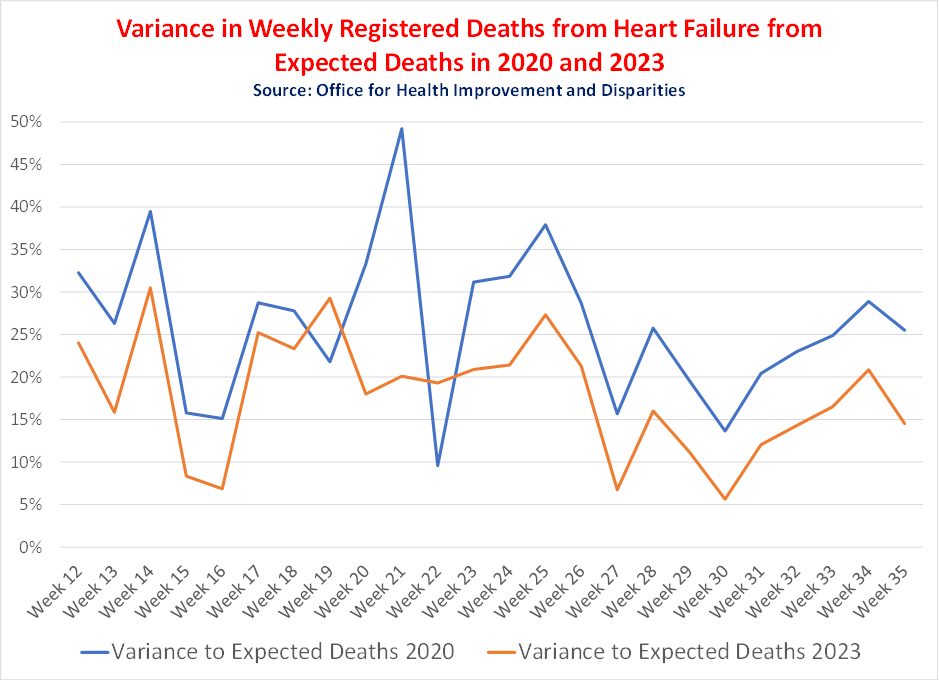
Figure 1 shows the level of registered heart failure deaths in 2023 measured against the ‘expected’ level for 2020 and 2023. These are shocking figures. But what’s the cause?
Chief Medical Officer Professor Chris Whitty offered up ‘delays to the prescription of statins’, before this theory was thoroughly debunked by Carl Heneghan and Tom Jefferson in a Substack post, subsequently reprinted by the Daily Sceptic.
Some cardiologists, such as Drs. Aseem Malhotra and Peter McCullough have pointed the finger at the mRNA vaccines.
Others blame the tendency of the lockdowns to reduce activity levels and force us into unhealthy lifestyles.
For me, two chance meetings at a riverside pub garden encapsulates the role of pharma and non-pharma interventions in this sorry state of affairs. Which of these paths bears the greater burden of responsibility, I leave it up to you to decide.
Picture the scene: a warm summer evening during the recent fine weather, a pleasant pub garden, boats and paddleboarders drifting by. A friend came over. He’d been a zealous masker and social distancer. He had fallen out with various people over his over-zealous compliance with the whole Covid theatre. But surprisingly his opening words were to inform me that the 43 year-old girlfriend of a mutual acquaintance had just dropped dead and, amazingly to me, he blamed the vaccine. He then went on to tell me about John Campbell, adverse reactions and the dangers of spike proteins. I agreed that it wouldn’t be a surprise if the vaccine had been a contributing factor.
We hear this story again and again. Vaccine injuries and deaths are a real thing. The real-world benefits of mRNA vaccines are very debatable. ‘Cases’ peaked in January 2022 at three times their previous peak and after 90% of the population were vaccinated. According to Euromomo, excess deaths across most of Europe in post-vaccine roll-out 2022 were 7% higher than in 2021 and only 2.7% lower than in pandemic ravaged 2020.
As my first friend was leaving, a second old friend came along. He used to regularly cycle in the same group as me but hadn’t been since the lockdowns. Now, here he was, 10 kilos (1½ stone and 3.2 points on the BMI scale) heavier, explaining that he’d never really got back into cycling after the lockdowns and now he felt he’d be so far off the pace he’d struggle to keep up and where’s the fun in that? He then went on to say that, the end of cycling aside, the first lockdown had been the happiest period in his family life. He’s a bit of a Lefty, and, true to form, made an abrupt Left turn and went into the merits of UBI (universal basic income), how wonderful if everyone could frisk in their garden in late spring sunshine and to hell with work. Lounging on the riverbank in the late summer sunshine I could have easily been persuaded that he had a point!
As seductive as this notion may seem, I was reminded of a fascinating paper produced by the ZOE group back in July 2020. (You can see the study here, though perhaps the video is more easily digestible.)
The study looked at the lifestyle impact of the first lockdown across a number of factors, one of which was weight. The results across all the factors were bi-directional, meaning that some people put on weight and some people lost weight. Likewise, some people increased their activity levels while others reduced theirs. Some snacked more, some snacked less.
Figure 2 shows the impact on weight. With over 200,000 participants this was a huge study. Participants were divided into two groups: low DI and high DI. DI stands for ‘disruption index’; it indicates the degree to which someone’s lifestyle was impacted by the lockdown.
Body weight change was highly variable among individuals. In the Low DI group, 33% of participants lost a mean of 4.4 kg and 34% gained a mean of 3.7 kg. Amongst the High DI group, 33% lost an average of 5.5 kg, while 34% put on an average 4.2 kg.
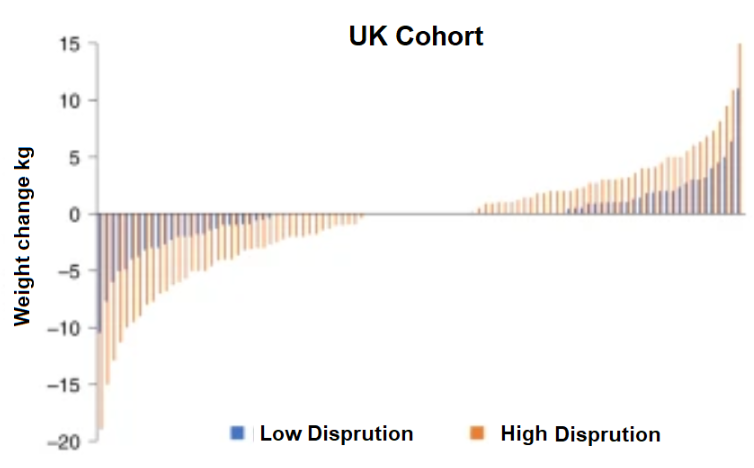
The change for the population as a whole was about zero, but this masked big variances at the individual and sub-group level. There were many examples where people were spurred on to change their lifestyles, but as a general rule the fit got fitter and the fat got fatter. This friend, having gained a few kilos in the first lockdown, was now distinctly overweight and compounding the problem year after year.
I would argue that the picture unearthed by the ZOE lockdown study is probably indicative of what would happen if UBI allowed people to absent themselves from the workforce. I suspect WFH (working from home) for some people also emulates a less extreme form of lockdown, leaving more time for both strenuous activity or sloth.
It’s perhaps worth just reminding ourselves of the degree to which the U.K. has become a nation of fatties. Figure 3 shows the proportion of overweight and obese over 18 years-olds by English region.
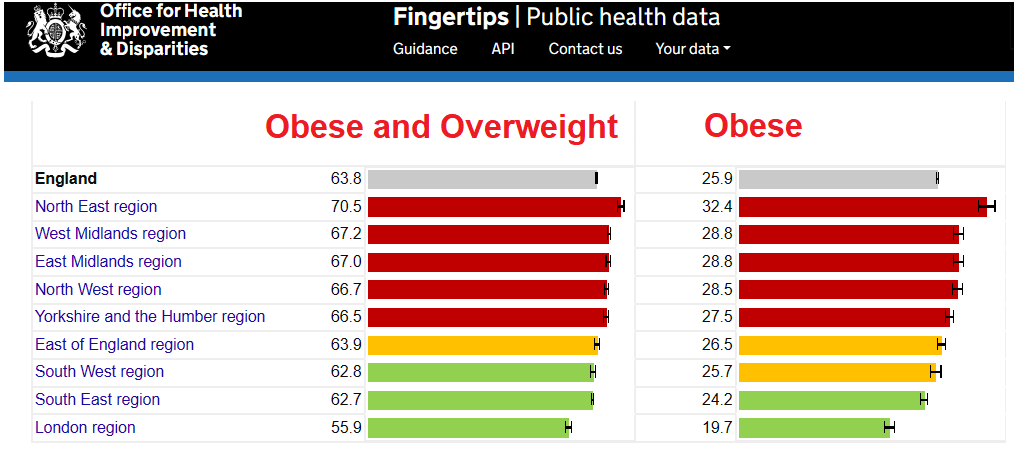
It’s a sorry tale.
But it’s not only some adults who displayed a tendency to put on weight during the lockdown. More worryingly still, children followed the same path.
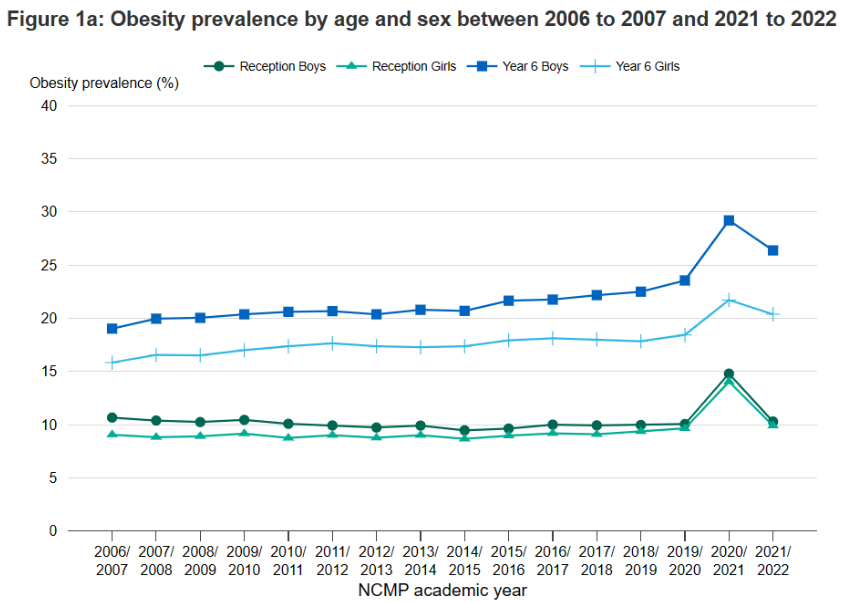
Figure 4 illustrates the degree to which reception age and year 6 boys and girls saw obesity levels accelerate dramatically in 2020-21. While the ‘reception age’ kids’ mean weight went back to its pre-pandemic levels the mean weight for year 6 kids didn’t, showing about a three percentage point increase.
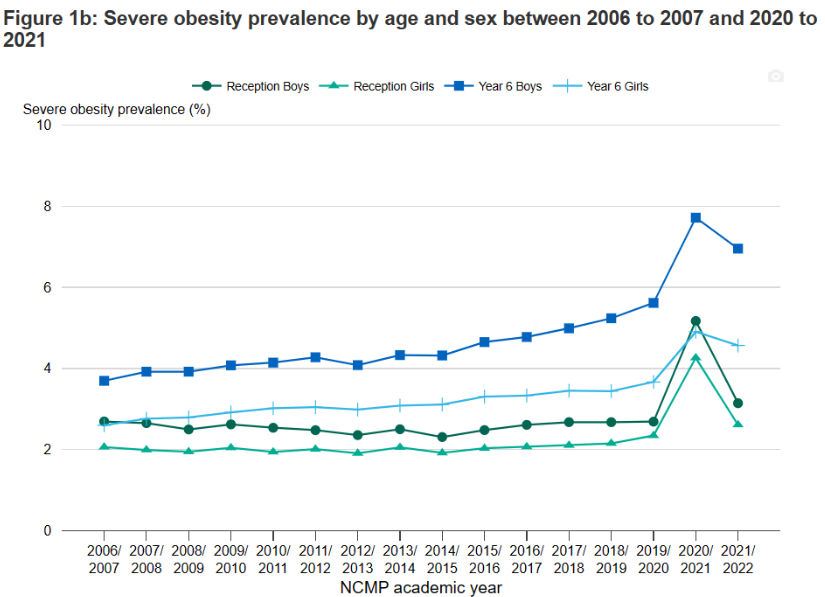
Among the ‘severely obese’, the impact of the lockdowns is even more dramatic, as shown in figure 5. Among year 6 boys there’s been an increase of about a a third in the number of the severely obese.
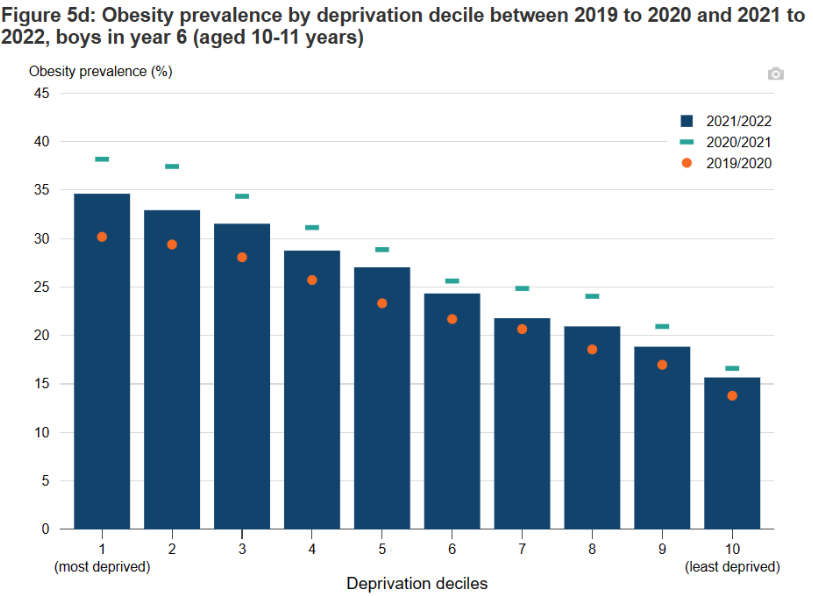
All too predictably, these increases in obesity tend to follow levels of family deprivation. Figure 6 shows that the most deprived kids are about twice as likely as the least deprived kids to be obese. In addition it shows that during 2020-21 the kids from the poorest homes were about three times as likely to become obese as kids from the better off homes.
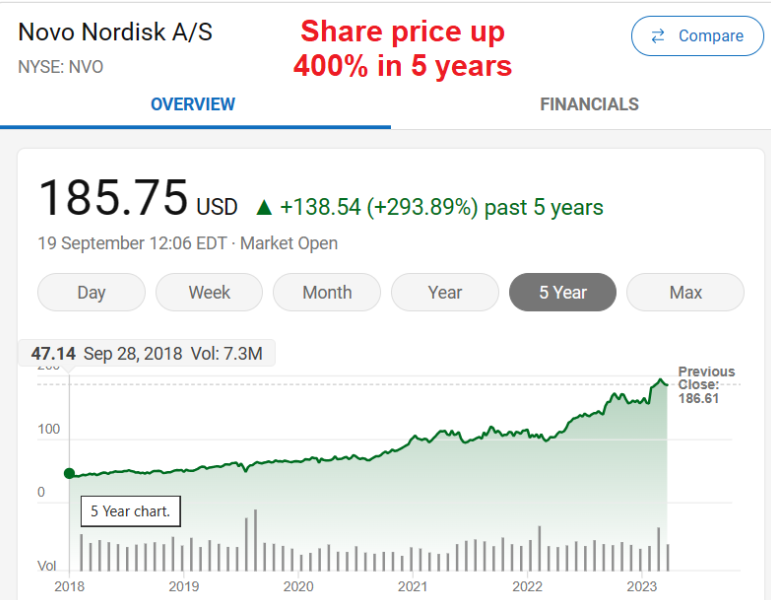
Of course, the solution for my cycling-lapsed friend is, in the Tebbit tradition, to get on his bike. The same goes for just about everyone else. But that’s not how the health professionals seem to see it. Rather than take responsibility for your own health, the taxpayer is going to be landed with a bill for ‘Wegovy’, the brand name of ‘semaglutide’, a drug that NICE claims could help people reduce their weight by over 10%, if implemented alongside nutrition and lifestyle changes.
Wegovy is made by pharmaceutical company Novo Nordisk. Its share price has doubled in the last 12 months and went up 400% over the past five years. It’s been a good time to be big in obesity!
Let’s roll forward 10 years. The NHS has been spending countless millions of taxpayers money on Wegovy, what’s the result? More obesity, the same level of obesity or less obesity? My money’s on more. What’s more, Wegovy comes with its own fair share of side-effects. Stop taking it and your weight tends to pile back on.
The story with Covid was clear: look after your health and there’s nothing much to worry about; pharma and non-pharma interventions simply weren’t required. Exactly the same is true with regard to weight and general health. But how do we help people realise that salvation doesn’t reside with Big Pharma?











To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
If you like data and are partial to a graph then this substack will knock your socks off. Excellent work by this author;
”Occam’s razor (also spelled Ockham’s razor or Ocham’s razor; Latin: novacula Occami) is the problem-solving principle that recommends searching for explanations constructed with the smallest possible set of elements.
For the First time we have Synchronized data from England where we have
a) All-Cause Death by Vaccine Status – Separated into Age Groups
b) Vaccine Uptake Data – Separated into Age Groups
The Sets of Data are for the Same Time Lines and the Same Populations.
Why on earth the England Health Authorities failed to (or would not) provide the following Essential Public Health Assessment is something deserving of an inquiry if not prosecutions; given record Excess Deaths in the UK have followed the roll out of uncontrolled Biodistribution Lipid Nano Particle Synthetic Messenger RNA Genetic Instruction “Vaccines”.
To all those defending the Vaccines in the face of this Data, you are now party to continued an unnecessary death … and untold suffering; The extra all-cause deaths represent a mere fraction of the number of people likely harmed, the devasted number of family members either grieving or struggling to carry extra burdens brought about by pure and reckless greed and reckless virtue signaling or defense of an indefensible reckless and greedy vaccine stakeholder position.”
https://thenobodywhoknowseverybody.substack.com/p/england-annus-horribilis
By a long way, the most evil thing inflicted by government on people in my lifetime. (I’m 72).
I’ve had a quick read but it’s not obvious how they control for the uncertainty in the population figures. This is the big problem. Statisticians have the data for how many people had at least one dose to a pretty high accuracy, but the perennial problem which clouds the analysis is that there is no single source of truth for the total population figure or the numbers in each age strata.
And what’s the No1 risk factor of DEATH from Covid 19?
Obesity!
This study from the CDC shows that being obese and being admitted to hospital with Covid 19 gave a person a whooping 30% increased risk of dying from Covid.
So while they locked us down they were unwittingly INCREASING our chance of dying from Covid.
You couldn’t make it up.
If you dont think it can get anymore absurd have a guess what the No2 risk of dying from Covid 19 is?
Asthma, Chronic obstructive pulmonary disease (COPD), Emphysema, Pneumonia?
Wrong!
The number 2 risk of dying from this airborne virus is………..errrr ANXIETY.
Yes, you read it right, Anxiety.
And with another whooping 28% increased risk.
And understand that this is not anxiety AFTER catching Covid but people who have a long past medical history of Anxiety.
Apparently this virus actually knows who suffers from this mental condition, targets them and kills them!
Anyone care to explain this bizarre finding?.
https://www.cdc.gov/pcd/issues/2021/21_0123.htm
Perhaps people with anxiety are less able to exercise and eat healthily? Either way, stress, anxiety, depression and the like are known to affect the immune system I believe. This initially worried me as I’ve been anxious all my life but luckily I managed to survive the ‘vid in 2022. Most likely it’s a false correlation, there’s a whole website dedicated to such things somewhere – the more butter you eat, the more likely you are to get divorced etc etc. Presumably they corrected for the possibility that such people had long term anxiety because they had other chronic health conditions, but who knows.
I know. I’ve known all along what this means because I’m a Paramedic and seen literally hundreds of patients with severe breathing difficulties.
The problem is, it’s such a simple explanation that no one believes me.
Here’s how it works:
Imagine you have a history of anxiety and test positive in 2020 for this new unknown virus.
You’re in a hospital bed surrounded by doctors in Hazmat suits and respirators telling you you’re going to die because the bad news is you have this deadly virus inside you.
If you’re an anxious person then you may start to get worried and even start to have a panic attack and the main symptom of a panic attack is…… HYPERVENTILATION.
To a bunch of hysterical doctors (relying on confirmation bias) you would appear to be having severe breathing difficulties, a sure sign of Covid ARDS (Acute Respiratory Distress Syndrome)
And so on the ventilator you’d go and almost certainly die because they’d crank up the pressure until your lungs exploded.
As for the low saturations that the Doctors give as ‘proof’ of Covid, desaturation is actually also a consequence of severe hyperventilation.
That’s why Anxiety is the No2 risk factor and why the medical profession is terrified anyone will work it out.
Makes sense, but wouldn’t anxiety after catching covid have the same effect?
You’d really think that a doctor could differentiate between panic and an actual problem – wouldn’t the O2 sats give it away?? Panic shouldn’t cause them to drop surely?
As I said this was people with a PAST medical history of anxiety not anxiety diagnosed after catching Covid.
The records were combed for all those who died in hospital and it was found that these people had been diagnosed or treated for anxiety prior to Covid.
As for oxygen desaturation this paper (link below) clearly shows that hyperventilation can cause oxygen desaturation.
This would also explain why these people were called the ‘happy hypoxics’ believed at the time to be a unique feature of severe Covid infection. Low saturations to the point of clinical hypoxia but with no fever and still able to walk and talk.
https://pubmed.ncbi.nlm.nih.gov/8118644/
I remember reading/hearing that info ages ago. Think it was Chris Martenson on one of his Peak Prosperity videos. I agree, it does sound absolutely absurd. It sounds even more absurd with the benefit of hindsight and all of the data that has emerged during all of the time that has elapsed. I mean, it’s not like the flu ever singled out the obese and anxious as a special class of people to target, nor any other respiratory virus come to that. It sounds like complete and utter bollocks to be honest. The one thing that cannot be disputed is that this ‘PsyOp19’ was far and away, disproportionately a real danger to the elderly and frail. Just the same as other respiratory viruses and illness, as it happens. Factor in the withdrawal of early medical intervention and meds such as antibiotics and the numbers just increase.
In fact, it’s so ridiculous to believe that a resp virus can select for fat people and target them that we’d expect the ‘obesity epidemic’ to be over and done with but it would appear that the UK is still holding the unfortunate title of ‘Europe’s Fattest Nation’ in 2023, according to the table on this site;
https://worldpopulationreview.com/country-rankings/obesity-rates-by-country
Good morning!
Obesity is a real problem increasing a person’s risk for multiple diseases. Fat is not an inert tissue as was previously thought. Obesity does negatively affect the immune system, so I am not surprised regarding increased susceptibility to infections.
On an aside, a study in the USA showed that lockdowns increased levels of obesity in obese people, not significantly in people with a normal BMI.
Yes it was Chris martenson and he was also scratching his head. I’ve found no other discussion on the topic despite this being a massive study of 540,000 people and the conclusions clear.
Did the CDC suspect what anxiety really meant? That deranged doctors were venting panic attacks in the tragically mistaken belief they were seeing Covid ARDS?
In subsequent guidance to frontline doctors Obesity and Diabetes were given as the highest risk factors for death but Anxiety was completely airbrushed. Very strange. (link below)
As for obesity and diabetes these people are always a high proportion of the hospital population.and human psychology would simply have chosen the most unsympathetic victims (the obese) as being first in line for the ventilator.
And that’s what we’re really talking about with these deaths, ventilator deaths combined with dubious natural deaths, mistakenly diagnosed as Covid, and Covid being put on the death certificate.
Was it murder? No, These doctors were temporarily insane (Mass Hysteria) and making decisions using confirmation bias not logic. The most we could expect would be manslaughter through diminished responsibility.
There was one incident though where the doctors crossed the line, I believe, and that was the deaths (link below) of 5 conservative anti vax radio show hosts who all died (I believe 4 out of the 5 were ventilated), apparently of Covid.
Putting aside the staggering statistical improbability that a cluster of radio show hosts would all die together in a short period these deaths were simply due to the Doctors, faced with vaccine hesitancy, having to find people to make examples of.
I’ve got a strong suspicion that these people would have been persuaded by the doctors that, once again, they had a deadly virus time bomb inside them and their only hope was to go on the vent. They may have been vaccine skeptics but the unquestioning trust in doctors goes so deep that, even for them and their families, they wouldn’t have been too hard to convince that only the Doctors could save them now.
Once dead their heads could be held high by the Doctors to push the uncompromising message they wanted to send to the public “see what happens when you don’t take the vax?”
https://pubmed.ncbi.nlm.nih.gov/8118644/
https://www.cdc.gov/coronavirus/2019-ncov/hcp/clinical-care/underlyingconditions.html
(see diagram at bottom of page RR and comorbidities)
https://www.vanityfair.com/news/2021/09/anti-vax-radio-hosts-dying-covid
I think overweight people do worse with lots of bugs, including flu, they just weren’t really told about it like they have been with covid.
It is a difficult area as it is too late for the people to regret their decisions and have the stuff sucked out of their body.
In the next Plandemic there will be no refusal of the jab and this scares me as WHO are ramping up their control.
The more encouraging news is that more people are refusing any sort of jab, as I would not put it past the suppliers shoving ‘left over mrna mix’ into anything.
Spot on. mRNA in the food, water, the air, who knows. Robots and Police going door to door. The Klimat-Mongoose Flu scariant. Followed by countless others being cooked up in the 300 US biolabs worldwide. Just a cockup.
Why do you say, ”In the next Plandemic there will be no refusal of the jab..”? The data clearly show that for every new death shot released there are less and less daft enough to rock up and take it. Therefore, with a foresight marginally more accurate than Tosspot Ferguson, I’m going to go out on a limb and predict that whatever sh*t sandwich they plan on serving us next there will be uptake of the mRNA ‘vaccine’ bioweapon ( because it’s bound to be, isn’t it? ) which is at an all-time low, reflecting perfectly just how awake and distrustful the masses have become off the back of ‘PsyOp19’.
I would love to agree with you and hope you are right. However, the last Plandemic propaganda pushed the mandatory jabs & people in the U.K. were already saying no jab, no NHS care, no job.
Seeing how quickly they can defund & debank detractors, it does not fill me with hope.
Unlike you, I am surrounded by jabbers and have only met two people with my views.
I hope you are right Mogs.
Don’t forget that in the UK we are pretty close to a General Election (next Spring?). The Conservative conference is next week. Almost everything significant should be seen in that context. In particular, they will be selective of what is published via the usual media.
A very good piece, thank you.
Exactly – food is comfort. Obesity is largely due to comfort seeking.
Thus the underlying reason for obesity is stress, and more specifically the inability of most people to cope with stress. The issue here is a lack of skill to handle our natural emotions: stress comes in a spectrum and is vital for a balanced life (it makes us alert).
But the western approach of ‘making it go away’ is utterly wrong.
And who ever taught us how to handle our emotions in formal schooling?
The way out of this spiral of inability is to become more skillful in handling our emotions, and the best way to do this is to train in mindfulness and meditation.
“But how do we help people realise that salvation doesn’t reside with Big Pharma?”
My wife and I went carnivore some months before Covid hit. My wife lost a lot of weight, I, 6’5″ and 14 stones (had been for years, well within BMI boundaries), energetic and fit, lost 20lbs in 6 weeks, and have now settled at around 12 stone 10 lbs.
The fat lost was visceral fat. The fat you don’t need, the fat that is piled on by the appalling shit people eat. Read up on the Randle Cycle, which explains how a diet of carbs and fat (including the filth that is seed oil, industrial waste in reality) PILES on the pounds.
Dump carbs and sugar, and you’d be fine. And it’s easier than you might think, tho’ carbs are addictive as they don’t fill you up, rather make you crave more
But says the Climate Retard, ‘doesn’t the cow and pig kill Gaia…my earthly mommy?…’ (tears, sagging shoulders)
Answer – No!
Arable framing is responsible for the death of the countryside. Soil poisoned, hedges destroyed, animals, flora and insects exterminated on a massive scale, as anyone of my age (72) can attest to.
Livestock farming done properly replenishes the soil with animal shit. It can also take place where you cannot grow arable.
My wife and I went Carnivore over three years ago. We eat, and cook with animal produce alone. Our (grass fed) meat comes from a local farm shop and our local butcher. Our food miles are minimal – the only food I regularly buy from our local Sainos is tea and coffee. Similarly our food waste is non-existent. Any fat too gnarly the dog gets, teabags and egg shells go into the compost. We gave back our food recycling bin.
A good read on this matter is “English Pastoral” by James Rebank. Regenerative farming is also taking place all over the USA, on livestock ranches. Our farm shop (we’ve known the farmer for nigh on 20 years) farm a patch of land in Somerset that they have farmed for over 300 years. They have always practised what is now called “regenerative” farming, rotating livestock and arable and feeding the earth with animal shit. I love the smell of slurry in the morning 😁
Oh and for the climate crazies – their farm has been declared carbon neutral.
And if you are ever there – https://www.kimbersfarmshop.co.uk/ – be sure to talk to the farmer about Vegans 🤣🤣
https://web.archive.org/web/20230327065009/https://www.netzerowatch.com/agriculture-may-already-by-climate-neutral/
This organisation might be of interest: https://www.soilassociation.org/ if you are not already a member.
Yes – tho’ their origins are murky!
https://thecritic.co.uk/issues/august-september-2022/blood-and-soil-the-greens-fascist-roots/
Of course, the Nazis were the original Greens… and current Greens very similar, in that they believe that the end justifies the means; such as, polluting vast areas of the Third World mining rare earth, sickening many and wrecking lives and childhoods, so that we can have “clean” energy
“Fascist Ecology: The “Green Wing” of the Nazi Party and its Historical Antecedents”
https://epublications.marquette.edu/cgi/viewcontent.cgi?article=1155&context=hist_fac
Green Tyranny
Exposing the Totalitarian Roots of the Climate Industrial Complex
By Rupert Darwall
https://www.independent.org/publications/tir/article.asp?id=1363
I wasn’t aware that the Soil Association was allegedly founded by some of the 1930’s fascists, until I read the “thecritic” article. However, their summary “It is a tragedy that the radical politicisation of environmentalism has led to the majority of those who occupy the political middle-ground recoiling from the real issues of biodiversity loss and climate change. It could be argued that until this green extremism disappears, the chances of us finding consensus on how we combat the evolving environmental crisis is, like Tarka, dead in the water.” suggests that they actually believe in a current “environmental crisis” related to “climate change”. Looks a bit oxymoronic.
Thanks for the adverts for some in-depth books! It’s wise to be sceptical about all the industrial complexes, including the chemical industry and the others.
I’ve increased my quality red meat consumption a lot in the last 6 months, from almost no red meat to at least twice a day. (Hey, if they say it’s bad for you, it’s probably really good.) I notice I feel very content every day. I put it down to the red meat.
Beware alpha gal syndrome, which is an allergy to mammal meat and products. I wouldn’t be surprised at all if the meat allergy and infected ticks came from a biolab. My husband and I were both diagnosed a decade apart. I had anaphylaxis requiring hospitalization and he had hives. We live in the eastern half of the US, where cases are increasing. UK has some cases and Australia has quite a few. Weird that different tick species are causing similar reactions across the world, right? Eating low carb with red meat made me lose weight and feel great. Eating well is much harder with just poultry and fish (and tofu and beans) on the plate.
I’m no medic but suspect this is the thin end of the wedge for cardiac deaths as the spike begins to bite.
A whole generation has been cursed by the politicians.
Time for change and retribution.
I think the words poverty and deprivation now mean something quite different to what they used to.
If you are fat (and almost certainly have a mobile phone) and a place to lay your head, I refuse to accept you are poor. And you may be deprived of many things but certainly not sustenance.
I’m not judging. I’m just saying that isn’t poverty in my books.
If poverty is “relative” then there will always be poverty… unless we have a society where everyone has the same. Is poverty another word that has been corrupted by lefty collectivists to advance a political agenda? Yet again?
Indeed. It’s quite plausible IMO that the correlation between “relative poverty” or “relative deprivation” or what is in truth just “the lower part of the socioeconomic spectrum” (people who earn less and are less educated) and fatness and health is not evidence of causation. “Poor” people don’t eat badly because they are sad but they eat badly because they make bad life choices in general, as evidenced by them being poorer and less educated than average.
That’s harsh tof.
Not intended to be harsh. Of course luck plays a part – who your parents are, where you are born, what happens to you in life that is outside your control, and of course the capacities you are born with. I would love for people to eat better food and live more healthily, and when I come across people in my daily life I encourage them to do this, while trying not to get too preachy. I guess these days I am just paranoid about anything that seems to assume equal outcomes are natural or achievable. Of course people sometimes eat badly because they are sad, but perhaps they are sad because they are just not as good at the game of life as others.
Yes – poverty shouldn’t mean being able to buy enough food, even cheap and nasty food, to become seriously overweight.
The Road to Nab End – William Woodruff – https://www.williamwoodruff.com/the_road_to_nab_end__an_extraordinary_northern_childhood__29442.htm
And many similar instances were part of my grandparents growing up.
It’s a brilliant book.
I’ll check it out.
To be clear though, I’m not saying poverty never existed.
I could be wrong but I am guessing that the poor in Lancashire in the 1930s were not overweight. I just don’t think people who struggle to feed themselves can be overweight.
So this Wegovy rubbish leads to weight loss alongside lifestyle and nutrition changes? Are they sure it’s not just the lifestyle and nutrition changes that are leading to the weight loss? If you can make those changes alongside this miracle drug, why not just make the changes and not bother with the drug?
I often wonder how bad it has to get before the RPTB/bigpharma/governments etc. get nailed over this.
The next few years are going to be very interesting. The RPTB have a huge investment in mRNA jabs – vast amounts of money depend on the success of such gene therapies. Vax passports/digital ID being the ultiate aim of course “for your safety”.
Hopefully we are near a tipping point, people are beginning to question the narrative eg look at the diminishing jab uptake – I’d say because a vast number of people know of someone close whose health has been badly affected or worse.
All empires fall, most very slowly then very quickly.Think bigtobacco.
One important point re statistics and particularly the ONS. There seems little doubt that the ONS, and I’m being kind, bends to the will of its political masters. Just in case anyone from there reads this, just remember that your masters ie the government, are immune from prosecution. You’re not – and it will be of no use saying you were just following orders.
I’d love to see a reality TV show in which a group of obese people (who aren’t on any medication that causes weight gain) volunteer to remain in a controlled environment where they are fed only healthy food, in normal reasonable amounts, no junk food and no overeating allowed, with exercise-based tasks for non-food rewards, for about 10 or 12 weeks, to see if their obesity is due to their genes or their lifestyle.
I’m sure it would be a ratings winner.
In discussions about obesity, I rarely hear any mention of the fact that antidepressants and other psychiatric medication, and various non-psychiatric medication, can cause weight gain in many people, with a very high proportion of the population taking some type of long-term medication.
I’ve definitely seen such a thing ages ago. Probably back in the day when I watched BBC, or TV in general. I just can’t remember the name of the shows now. Do you remember that one ( don’t know if it was Channel 4 or BBC ) where there was 2 people living in a house, one was obese and super unhealthy and the other was always underweight. It was that buff blonde guy who was a doctor who hosted it. They had to swap diets for a week I think, so at every meal they’d have to sit together and eat what each other would normally eat ( or not ) for that meal. I always enjoyed that show because it was a rude awakening for both participants, who were at polar opposite ends of the ‘fat/skinny’ spectrum, and it demonstrated the huge influence that psychology plays in determining what and how much we eat, plus exercise of course. There was also a one hosted by that chef who’d lost a load of weight, from Gloucester, and the participants also lost weight on that one. ”Fat Families” ( I think ), hosted by that guy in the glasses, was also another entertaining show.
Yes, I remember that programme, Mogwai, it was ‘Supersize v Superskinny’, on Channel 4, with Dr Christian Jensen. They only swapped diets for 5 days (later 2 days) , according to Wikipedia, and the overweight person’s diet for those 5 days wasn’t necessarily a healthy diet.
Fear not! Annie has her mask; crisis averted!
Wonder what the correlation coefficient is between increased obesity and increased obesity in big Pharma’s bank accounts? 1 would be my guess.
Nahhhhh …. It’s another conspiracy! no?