
Downplaying. That has been a handy weapon against anything that threatened the official Covid narrative. Downplaying sceptical voices, downplaying uncertainties, downplaying contradictory data.
I recently described a typical example of the latter from Denmark. Here is another one, from Israel, which gives us a dual opportunity: first, to look at the rate of significant adverse events after the booster dose, as reported in a Government-initiated survey. Second, to observe the language the anonymous authors used to describe the data. Released long ago but not published in a medical journal (yet?), the summary was written in Hebrew and contained 26 slides. I have tried to offer below a precise translation of the text.
The topic of the survey is called “reported phenomena”, which is not a complete phrase for “reported side-effects”, since, just like in English, an adjective is usually added to indicate the presumed link to a drug or a vaccine.
The authors are aware of under-reporting of side-effects, since they state “it appears that there is under-reporting”, though it is not clear how they infer that from reported data.
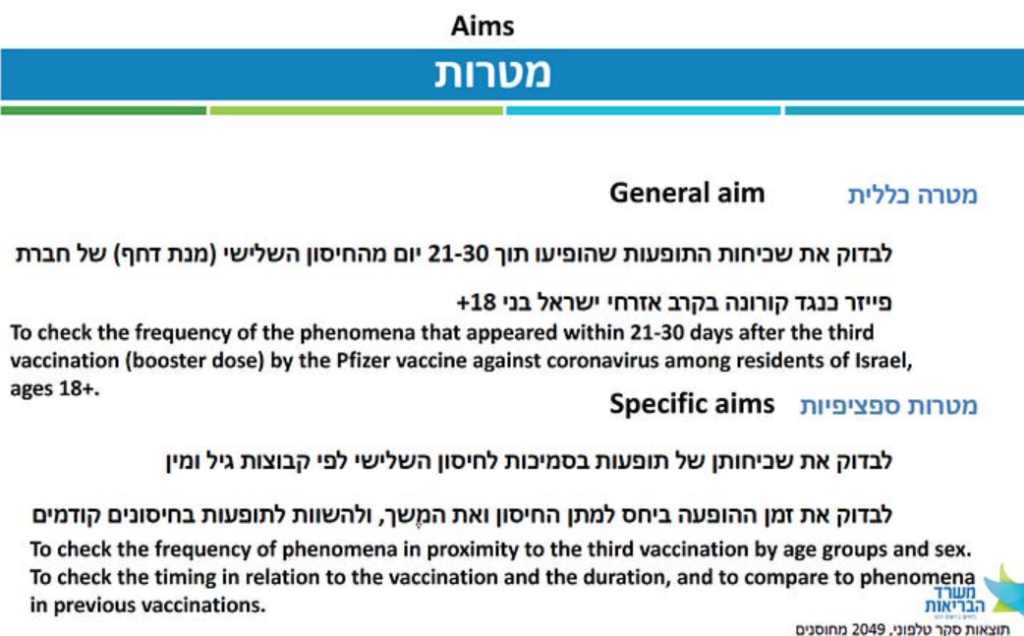
The aims of the survey are clearly stated (Figure 1). In brief, it was a random sample from the database of the Ministry of Health, excluding people without a listed phone number (understandable) and those who had had Covid (why?). Participants were vaccinated 21-30 days before a structured phone interview, conducted 2-3 months into the booster campaign.
Slightly over 2,000 people completed the interview, evenly split by sex. I am not sure why the sample size was not much larger, say, 20,000, closer to the vaccine trials. Lack of importance of the topic? Lack of resources in a country that served as a Pfizer laboratory? Downplaying unfavourable rates as imprecise (due to a small sample)?
Sampling ensured three equal-size age groups, which means that the age distribution of the sample did not necessarily match the age distribution of the vaccinated population. Although age-specific rates were sometimes presented, a weighted rate for the entire population was not.
Two to three months later, a follow up interview was conducted with 45 of 59 women who reported changes in menstruation after the booster. We’ll return to this part later.
Survey results are influenced not only by reporting accuracy but also by the response rate, which can be defined in more than one way. It was around 50% by one definition.
To estimate a range for the rate of selected side-effects, I will make two opposite assumptions about non-participants, which favour the vaccine. The first one is extreme.
- No side-effects would have been reported by non-participants, so any observed frequency should be divided by 2. You may also view this ‘correction’ as accounting for coincidental events.
- Unobserved rates in non-participants would have been identical, so any observed frequency is correct.
I am excluding the possibility that non-participants would have reported side effects at higher frequency than participants, again to favour the vaccine (a conservative approach).
A short preamble before showing data: vaccines are given to mostly healthy people who do not present themselves as care-seeking patients. Therefore, the standards for ‘safe’ are much more stringent than those for treatment of sick patients. In either case, Primum non nocere (first, do no harm) should be a governing principle.
Now, the data.
First, a vaccinee should have been lucky to escape side-effects – two-thirds reported at least one (Figure 2) – some of which have been classified by official voices as reactogenicity. Occasionally, that was a promotional public health message for Covid vaccines: the side-effects mean that the vaccine is working! For some reason, it has never been a promotional message for the flu vaccine.
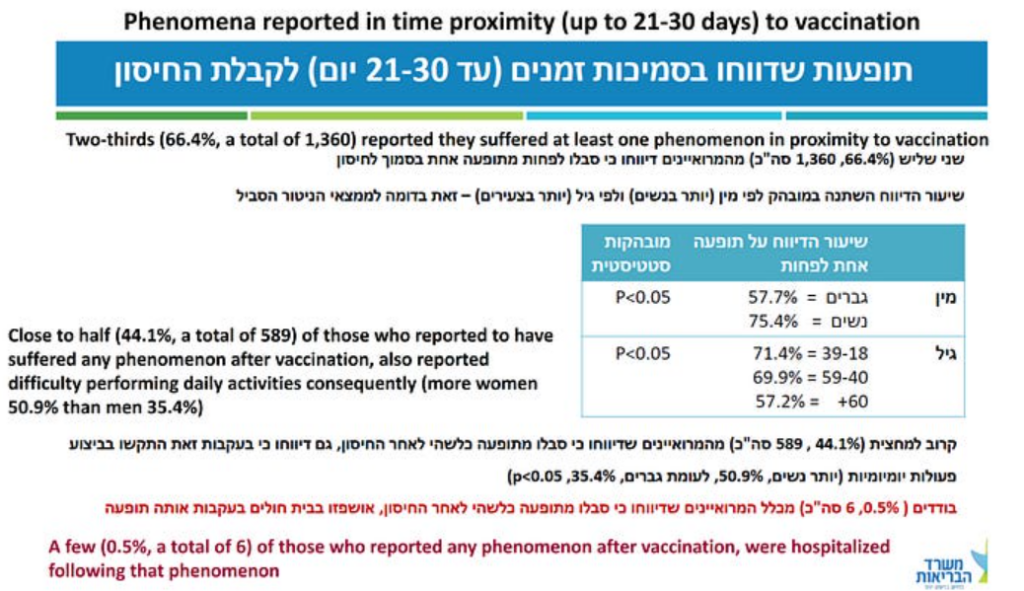
In almost 30% of the sample (589 out of 2,049), or about 15% under the most conservative assumption, the side-effect was severe enough to have caused difficulty in daily activities. Read the last sentence again and imagine that the culprit was a new mRNA-based shot for flu rather than Covid. Going grocery shopping? Get your flu shot here for free and a good chance to spend a few days in bed, or off work!
More important, hospitalisation after vaccination should be extremely rare, perhaps in the single-digit range per million or so, or no more than one per 100,000. That used to be called a safe vaccine. The rate in this sample was six per 2,049 or 150-300 per 100,000 (my conservative range) – hundreds of times higher than for a safe vaccine.
How good is this small-sample estimate?
Since hospitalisation follows a serious adverse event, we may check concurrence with the latter. A solid analysis of the randomised trial of the Pfizer vaccine estimated 18 serious adverse events per 10,000 (180 per 100,000) above the placebo group. By and large, 150-300 hospitalisations per 100,000 is a comparable range.
To grasp the magnitude of these rates, consider 7,000-15,000 hospitalisations in Israel after the first booster; 60,000-120,000 in the U.K.; and 200,000-400,000 in the U.S.
That does not fit the standards for a safe vaccine, even before considering vaccine-related deaths. And there were deaths, unless one assumes that all reported fatalities in every monitoring system are false. In Israel, the (short-term) booster fatality rate was estimated at 8 to 17 per 100,000, perhaps 200 to 400 deaths.
How do the authors report the hospitalisation data (Figure 2 above)?
A few (0.5%, a total of 6) of those who reported any phenomenon after vaccination were hospitalised following that phenomenon.
It is unclear if the red font was used to emphasise reassurance or concern. I translated the first Hebrew word to “a few” (neutral) but it might be closer to “few” (reassurance).
Either way, the truth is simple: if the vaccine were safe, we should not have observed any related hospitalisation in a sample of 2,000. To observe six instead of none, by the play of chance, is a fictional proposition.
Adverse events were divided between local, at the injection site, and “general” (exact translation), some of which should be called ‘systemic’. About half of the respondents reported at least one general side-effect, the most common of which were weakness or fatigue (42%), headache (26%), muscle or joint pain (25%) and fever above 38.0°C (15%). Of note, 5% reported chest pain. These are significant percentages even if divided by two.
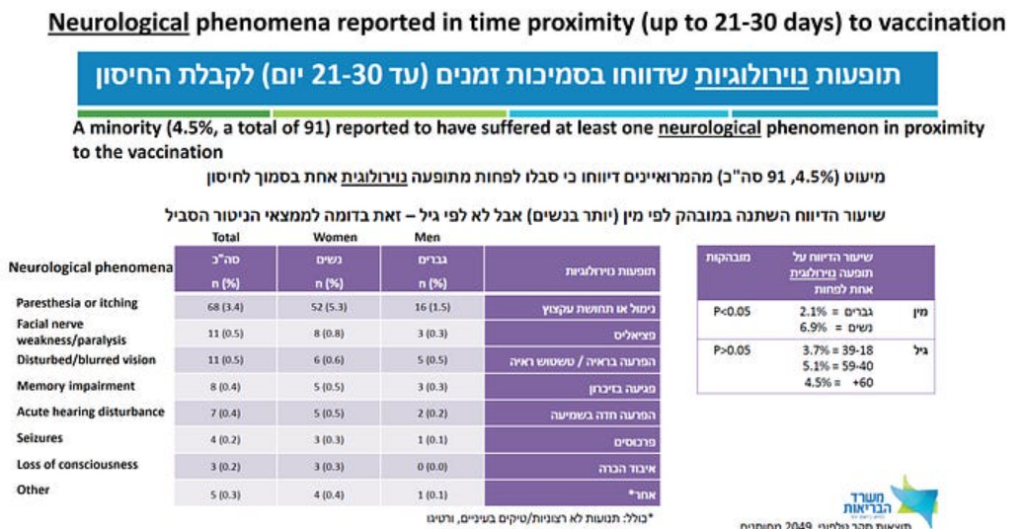
The authors reassuringly tell us that “a minority (4.5%, a total of 91) reported to have suffered at least one neurological phenomenon in proximity to the vaccination” (Figure 3). That it was not a majority is good news, but this minority corresponds to 2-5 vaccinees per 100, under my conservative assumptions. In almost half of the cases, the side-effect was still present on the date of the interview.
It is impossible to understand the mindset of public health officials who consider such frequencies acceptable for mass vaccination of healthy populations against a disease that is about as risky as the flu until around age 60, and in the healthy elderly. Perhaps coronaphobia has not spared them either.
Three slides present data on changes in menstruation. I still remember how this worrisome side effect — indicating altered hormonal status and systemic dissemination of mRNA-containing lipid nanoparticles — was downplayed at the beginning. Early anecdotes, mostly reported on social media, have sent a clear message: pregnant women should not be vaccinated. It was ignored.
Evidently, the risk in pregnancy was well understood by those who quickly launched post hoc reassurance research, which has no merit. Nothing can assure a logical-moral mind that interference with hormones during a normal pregnancy meets the criteria of safe and ethical conduct.
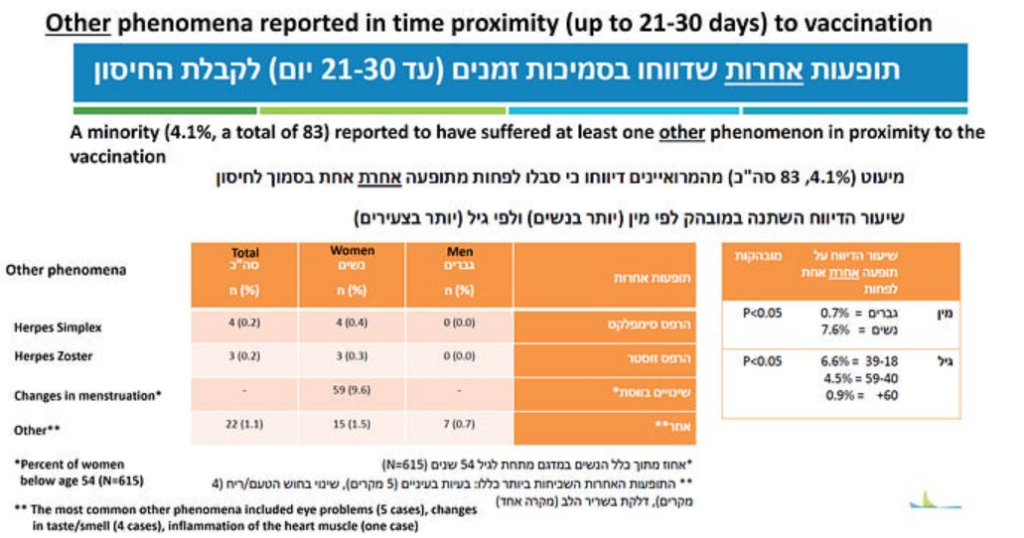
The frequency of changes in menstruation was computed from a sample of 615 women ages 18-53 (Figure 4). About 10% of the women (5-10% under my conservative range) reported some abnormality. Almost 90% of those who reported abnormality reported regular menstruation before vaccination, which means that in most cases it was not misattributed. In half of the women, the abnormality persisted at the time of the follow up interview. Perhaps they will have another follow up to tell us the frequency of prolonged or permanent abnormality after a third dose. Perhaps not.
There is a wider, troubling perspective of these data. We can be certain that the vaccine reached the ovaries and disturbed a delicate balance of female hormones because the clinical consequences were immediate. What about other organs? There is no reason to assume that mRNA-containing lipid nanoparticles spared all other organs, and if so, what might be the long-term consequences? That they can damage blood vessel walls is already known.
Last but not least, there was one reported case of myocarditis (Figure 4, footnote), which might have been one of those six hospitalisations. Not every case of myocarditis is diagnosed, so we cannot exclude one or more subclinical cases in the sample. If the vaccine were safe, we should not have observed any case of myocarditis in a sample of 2,000. Anyway, by now it is a widely accepted side-effect, downplayed by claims about Covid-related myocarditis.
Five conclusions were listed on the last slide. Let me end with a translation of the last one, often considered the take-home message:
In the majority of those who reported phenomena of any kind, the presentation after the third dose was not more severe in comparison with previous vaccinations.
I contemplated several responses to this reassuring message, but perhaps none is needed.
Dr. Eyal Shahar is Professor Emeritus of Public Health at the University of Arizona. This article first appeared on Medium.















To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
“Monkeypox lasts after scabs…” (Telegraph) Comments now closed, but some good robust views. The virus would be detectable after infection – that is immunity!
Also noted in the same article there were ‘surging case numbers’ LOL…I think there’s around 100 worldwide. They just can’t help themselves!
wonder when it is going to become “exponential”.
I haven’t heard it for ages now. I kind of miss “exponential”
Roll up those sleeves, dronebeings!
A Commonwealth-funded $200 million quarantine facility in Perth’s north looms as an expensive white elephant with Premier Mark McGowan admitting he is unsure what to do with the compound once construction is complete in the middle of the year.
Fill it with the evil politicians and ‘health officials’ and big pharma bootlickers. And use up that stockpile of vaccines – three shots a day, before meals.
They bought it. They own it!
They will keep it mothballed ready for the new WHO pandemic treaty.
Then any future vax refusers can be imprisoned in these 21st Century gulags.
Monkeypox deniers down under beware
Things have changed since they greenlit this. A lot more vax resisters and vax-remorseful now.
That’s one reason why the next shock that the rulers impose won’t be a rerun of the last one.
“Vaccination” only started about 9 months after the first lockdown. There has been far more resistance to “vaccination” than to lockdown.
They should be treated humanely (but locked down, of course), and allowed visitors: anyone who wants to speak to them about what they did to our lives.
And a televised draw every day for the honour of giving them their shame-to-waste-it shot. Something like this.
https://www.youtube.com/watch?v=j5EzLJzimZ0
The way prime minister Mark McGowan talks about this! That guy is seriously taking the p*ss.
Only in the state sector!
It’s basically a large number of portakabins with lots of extractor fans and barbed wire.
Is that a railway line running to it?
https://www.multiplex.global/projects/centre-for-national-resilience-perth/
Good question. There is a rail line through Bullsbrook, unfortunately there aren’t specific enough details as to where this facility is located. Google Maps doesn’t give much away.
LOVE the solar panels on the roofs, though. Internees will be happier just knowing their carbon footprint has been reduced.
‘Stonewall accused him of “making fun of trans people” in his new SuperNature special, reports MailOnline.’
He’s a comedian you demented perverts, making fun of people is what he does.
If he refused to make fun of trannies you would probably accuse him of excluding trannies and condemn him for that.
No they wouldn’t It is called touching a nerve. We seem to have forgotten in our new politically correct era that the anguished are often triggered by observations that get too close to the truth.
Most of us view transgenderism as mental illness. Six-foot men in frocks aren’t women. The literature (rarely quoted now) is quite clear; most suffer from a paraphilia, a fetish. They become sexually excited at the thought of themselves as women. Talk of them being women trapped in mens bodies is exactly that, talk. Some people are convinced they are Napoleon but it doesn’t make it so. The sexual link has always been clearly understood as unhealthy.
Instead of classifying this as a sexual fetish as they used to do, and working on reducing its hold over the individual, we have allowed the fetishists themselves to dictate terms. We must treat those masculine creatures as women. This is absurd and we all know it.
The exceptional sensitivity to all this is a clear sign all is not as the narrative would have us believe. Perhaps the way out is more awareness of the fate of those who transition. As we all know they tinker with some superficial aspects of the body; oestrogen injections do have some effect, and breast augmentation adds more. Wearing women’s clothes, a wig and makeup all add something. Except the most important thing, they don’t solve the actual problem. They aren’t women. They are men with mental health issues.
All this is known by psychiatrists. Surely at some point we must all get fed up assisting mentally ill people in a delusion that is destroying their lives?
Gervais probably gets too close the ridiculousness of this topic. A mortal sin for the thin skinned.
I don’t care a jot if their delusions destroy their lives. It’s allowing them to destroy other people’s lives that I object to.
A good synopsis
I watched it last night. Absolutely hilarious, but only because it approaches comedy from kind of a 1970’s perspective. Not quite though.
While the initial reaction to a comedian even mentioning trans is a bit of hand rubbing and “this could be good” what he actually articulates isn’t transphobic. But it’s funny and whilst trans is the subject matter, trans people are not the butt of the joke, so called TERFS are.
I was never a Gervaise fan until I watched his Oscar’s spot. What he does with his Netflix show is highlight the absurdity of every ‘phobic’ subject, even hurty words.
https://www.youtube.com/watch?v=ceS_jkKjIgo
I did think his series After Life was very funny though. All characters were fab but I think my fave was the skanky guy with glasses who’s wife left him for a gypsy. Cringey but funny with an undercurrent of pathos.
Good to see conservatives ( in name only) preparing for another cash handout into the highest inflationary environment for 40+ years.
“More money off energy bills for every household under Rishi Sunak rescue plan” – rubbish, he’s taxing business for making a profit and leaving green taxes in place, the Communist troll.
Yes, why not suspend the ‘Green Levy’ for a few years, keeping that and robbing tax payers again is not on
they aren’t giving up on any taxation rates and to even have tax on home heating fuel is disgusting
and to even have tax on home heating fuel is disgusting
By a few, you mean about five million and by suspend, you mean shove up the arse of Kim Jong Johnson….
Bet my household is excluded yet again
Left-wing parties will oust the tories and wreck Britain?
They’re too.late. The tories have spent the last two years wrecking Britain and have more or less finished the job.
I think we all sense there is some remnant within the Tories that does prevent the full spectrum destruction the modern Labour Party would unleash.
That would be a swift descent. Look at Scotland. The SNP are a hard left party now in bed with the Greens, who are outright communists. They openly talk about “New Scots” whom they want to invite to the UK. Many Scottish Government job adverts state explicitly “We welcome applications from individuals who require a visa to work in the UK.”
Their absolute hatred of us – their own people and the culture we created – is very obvious. At least some of the conservatives are against that. It isn’t much but it is something.
Agree there is a small remnant. If only they’d leave the Tory party and form something that represents the values that many of us have. It will be a great shame that they almost certainly won’t as the few decent ones are pretty much bound to lose their seats in the next election as the Tories are destroyed and who will we get instead?
I am not so sure. Labour don’t seem at all credible. So it is difficult to say.
Now would be the time for them to do it. To form a genuine conservative party given the disappointment of the last few years. A zero immigration policy alone would probably trigger a landslide in my view.
That hundred of them who rebelled against the vaccine passports would be a good start of a party – they could form a kind of alliance voting or bloc with perhaps the DUP who were fairly opposed to most of covid lockdown BS and maybe others. Would make it damned difficult for Johnson to ramrod anything else destructive through without his big 80 seat majority if nothing else. And if they went now they have the interim period between now and next gen election to try to grow.
There will be no salvation via the ballot box. That pseudo politics is gone for good.
Yes, there is still a remnant of non-leftism left in some parts of the Conservative party but Kim Jong Johnson has essentially destroyed the party.
They aren’t even Tories, they are Blairites, continuing the dismantling of the UK
Compulsory vaccination of children in the Netherlands failed.It was said that this proposal was aiming to make childcare centres safer for children’s health.
This was not just about any Covid vaxx.
So if a child is vaxxed against common diseases, why are the childcare industry scared of an unvaxxed one?
https://nltimes.nl/2022/05/25/childcare-sector-upset-cant-mandate-vaccine-use-senate-vote
“Compulsory vaccination of children in the Netherlands failed.”
But when they get to a certain age they will need to be ‘vaccinated for Covid’ to receive their EU Vaxx Pass if they want to travel anywhere, and be able to re-enter the Netherlands.
Down voted you for your defeatist attitude in your reply without even acknowledging the small win that Encierro informed us about.
Thank you.
“and be able to re-enter the Netherlands” Please cite examples of EU countries refusing entry to their own citizens/residents.
How about the UK? Entry was forbidden unless you could provide a Passenger Locator Form, and proof of being ‘vaccinated for Covid’, or a ‘negative result from a test’. Plus you needed to show you had paid for two PCR tests (sold by some shady character with a foreign name)… and also spend 10 days in ‘self-isolation’.
Many countries in the EU had similar demands of their own citizens.
How quickly we have forgotten!
Your memory fails you. The UK is not in the EU:
You are posting false information.
Dr. Naomi Wolf Proven Right On ‘Global Vaccine Passports’
https://rumble.com/v164s83-dr.-naomi-wolf-proven-right-on-global-vaccine-passports.html
Bannons War Room
Stand for freedom with our Yellow Boards By The Road next events
Saturday 28th May 3pm to 5pm
Yellow Boards LONDON
Junction Buckingham Palace Road/Victoria St,
London SW1E 5LB
Tuesday 31st May 2022 11am to 12pm
Yellow Boards
High St
(between Marlow Bridge & Pound Lane)
Marlow SL7 2AA
Stand in the Park Sundays from 10am – make friends & keep sane
Wokingham
Howard Palmer Gardens
(Cockpit Path car park free on Sunday)
Sturges Rd RG40 2HD
Bracknell
South Hill Park, Rear Lawn, RG12 7PA
Telegram http://t.me/astandintheparkbracknell
…..
““ESG’s power grows as banker is canceled for talking sense on climate change” – Rupert Darwall says in the New York Post that Stuart Kirk should not have been cancelled for talking sense about big banks’ ludicrous obsession with climate change.”
Best thing that could have happened. Kirk has had great publicity from this and had plenty of support from other bank bosses. The BoE also being slammed for their obsession.
Rumpelstiltskin syndrome. People yawning and rubbing their eyes as they emerge from a generation of slumber.
I think the COMMservative scumbags have done a pretty good job of “devastating the UK”. There is no coming back from this. They have committed treason on a grand scale and are guilty of carrying out the most serious crimes it is possible to commit on an industrial scale. They have got this far without being asked a single difficult question. That is a measure of how dishonest our society is, it literally cannot bring itself to even contemplate the truth, let alone handle it.
We now need to form a NEW POLITICAL MOVEMENT, with good people at the centre of it, not the lying criminal selfish greedy corporatised terrorist scum we have currently got. The UK is ripe for big change, we now have a golden opportunity to finally rid our democracy of these vile people and their twisted ideas about what is ok and not ok.
Theres six hundred and fifty of them and sixty eight million of us. We can do this.
Thanks for that CTR. I was beginning to think I was a loner.
On DS!
““DAN WOOTTON: Sue Gray delivered a damp squib Partygate investigation” – The GB News presenter and MailOnline columnist says it will take more than Sue Gray’s report to topple BoJo.”
Dan Wooton is wrong. Partygate was never about parties, we could all have dealt with work/social events, albeit grudgingly.
It was the barefaced lying by our PM and his habit of hanging others out to dry as a sacrifice to the public that’s objectionable.
It was the barefaced locking down, repeatedly and with accompanying propaganda from Pyongyang.
Dan is completely wrong on this. I cannot for the life of me understand why he goes as far as he does to DEFEND Johnson.
The other evening I was in the very very odd position where I found myself, possibly for the only time ever, actively agreeing with Benjamin Butterworth.
Have said elsewhere on this site that Dan Wootton needs to scan some of these posts on this site to see what his viewers really think before he continues with his “move on draw a line under this” patter.
The irony of this comment is that Partygate is a big distraction from the actual crimes the government has committed over the last two years, and their ongoing destruction of British democracy and sovereignty.
“Analysis from NHS doctors …”: are these the same doctors who lied their way through the last couple of years, or different NHS doctors? How are laymen meant to be able to distinguish one mob from the other?
From British government radio a few minutes ago I learnt that Mary Magdalene has been “slut shamed” for all these years.
Every gob in the studio agreed. “Slut shamed”, “slut shamed”, they all echoed. The term “sex work” was also heard.
So it will be no Easter eggs for them!
But I doubt even a single one of the idiots on the radio programme, or its producer, would understand that joke. They’d have to know more than a tiny amount about Mary Magdalene to begin to.
Clearly we live in uber-sensible times, when fashionable lingo thought up by independent thinker geniuses during the past five minutes, standing so impressively on the shoulders of giants, finally explains thousands of years of history and culture and religion.
Either that…or well maybe another take on what’s happening can be made to stand up better?
PS Did nobody tell these idiots the difference between a “whore” and a “slut”?
Boris Johnson may be a pathological liar in the true sense of that term, lying even when he isn’t close to being obliged to lie to maintain his position.
We’ve enjoyed the photos. Next can we have some audio please? And then perhaps a “What happened to the missing tapes?” inquiry if you must.
Surely surely he’s got it coming to him? The senior civil service must detest him. The Commons Speaker’s office probably aren’t too keen on him either. His friends include the London Metropolitan Police, officials of one or two foreign powers in London, and … ?? … Has he got one or two mates left at the Spectator? He doesn’t seem like the kind of person many people would bend over backwards to be loyal to.