
New York City’s death toll in the first Covid wave was unusually high. By the end of June the city had suffered excess deaths of 183 per 100,000 people. For comparison, nearby Maryland suffered 60 per 100,000 in the same period.
The reason so many people died in New York that spring has been speculated on since the start. One popular theory is that it was the mania for mechanical ventilators that was chiefly to blame. For instance, Michael Senger writes:
The outsized number of excess deaths in the area around New York is better explained by the particular hysteria in that region for mechanical ventilators which decreased the survival rate for patients over age 65 by 26-fold.
While Senger elsewhere allows that “other iatrogenesis” may have played a role, he takes the main culprit to be ventilators, as the above quote indicates. He is far from alone in this view.
However, it is straightforward to show from public data that mechanical ventilation cannot be responsible for more than 20% – or a fifth – of the Covid deaths in NYC that spring.
The first salient fact is that just 12% of NYC hospitalised patients were on mechanical ventilation as of April 4th 2020, according to a study in JAMA. The same study shows that the death rate for intubated Covid patients was 88%.
According to the CDC, 32% of NYC Covid hospital patients died during the first wave. (The CDC notes this rate was similar to the U.K. rate of 33%.)
If we assume that the 88% ventilator mortality rate continued after April 4th then ventilator deaths would account for 11% of all hospital patients and thus 34% of all hospital deaths (i.e., 11% ÷ 32%).
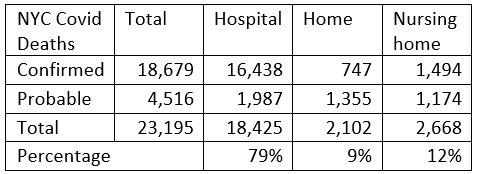
Hospital deaths were 79% of total NYC first wave deaths, again according to the CDC (this is assuming that deaths not at home or in a nursing home were in hospital).
This means that deaths of intubated patients accounted for 27% of total NYC first wave deaths (i.e., 34% × 79%). The normal death rate for patients on mechanical ventilation suffering from viral pneumonia is 22%, according to a study from Atlanta. So if we (conservatively) assume that all Covid ventilator deaths above that level were avoidable, preventing those would cut the NYC Covid death toll by 20% (i.e., 75% of 27%, where 75% is 100%–(22% ÷ 88%)). The NYC ventilator panic cannot be blamed for more than that.
It might be suggested that NYC simply intubated too many people unnecessarily and should have intubated far fewer. However, 12% of hospital patients being on mechanical ventilation is relatively low compared to, for example, England in its various Covid waves. The proportion of hospital patients on mechanical ventilation in NYC was not unusually high.
Why was the NYC ventilator mortality rate so high? The Atlanta study compares it to the rates for other states and finds it at the top end.
In some of the earliest reports of COVID-19 from Wuhan, mortality rates among those admitted to ICUs ranged from 52-62%, and increased to 86-97% among those requiring invasive mechanical ventilation. In more recent data from the United Kingdom, 67% of those who had received mechanical ventilation died, as compared to 22% of patients intubated with viral pneumonia in the preceding three years. Early reports of smaller cohorts from Seattle, where some of the first COVID-19 outbreaks occurred in the United States, indicated that 50-67% of patients admitted to the ICU and 71-75% of those receiving invasive mechanical ventilation died. A recently published report from New York also found high mortality of 88.1% among those who required mechanical ventilation.
For Atlanta, the study found a rate of 47% (49 died, 55 discharged), which the authors attempt to explain by suggesting that a policy of early intubation helped lower the death rate: “Our internal guidelines emphasised early intubation and standard lung-protective ventilation strategies.”
If Atlanta was intubating more readily while NYC was prioritising sicker patients, that could explain the difference. However, that would be the opposite of the iatrogenic theory, which argues that early intubation is what was killing people.
In any case, with intubated patients accounting for just 12% of hospital patients and 34% of hospital deaths, and hospital deaths making up 79% of all deaths, ventilators cannot be held responsible for more than a fifth of NYC first wave deaths.
The New York nursing home policy of discharging Covid positive patients into the homes has also been blamed for killing large numbers of older people unnecessarily. However, with only 12% of NYC Covid deaths occurring in nursing homes, there is a clear limit to how much that can explain as well.
Wrongheaded policies and treatment protocols certainly contributed to excess deaths during the pandemic. However, there can be little doubt that most of the excess deaths during Covid waves were due to the virus. That’s why they invariably closely track the other epidemiological measures. Symptoms, PCR test positivity, LFT positivity, genetic sequencing of variants, hospitalisations and antibodies all rise and fall together as waves pass through. A review in the Lancet of all 1,095 autopsies of Covid-positive patients in Germany found that 86% died directly due to the virus and 14% died with the virus as a secondary cause (or incidentally present).
Lockdown scepticism doesn’t rest on proving that COVID-19 is no more severe than the flu. Flu is generally understood to have a 0.1% fatality rate. Professor John Ioannidis estimated the fatality rate of Covid in the first wave to be around 0.4% in Europe and the Americas (note that NYC’s overall excess mortality, after three years, no longer stands out). The slightly higher fatality rate is not unexpected for a virus slightly more severe than influenza. Lockdown scepticism does not depend on convincing people that that 0.4% is really 0.1%. Rather, it depends on convincing people that our freedoms, prosperity and way of life should not be sacrificed in order to try to suppress or contain a virus with a mortality rate well below 1%.
Of course, we should also try to identify policies and treatment protocols that were harmful in order not to repeat them. And pointing out that interventions aren’t actually anywhere near as effective as claimed is always worthwhile. But the most important goal is to establish the priority of freedom over cowering in fear from a not-so-deadly virus.













To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
I guess, like most that come here, I am thoroughly sick of what’s happening in this country (& the planet, really) and increasingly alarmed about the future!
This is a request to the administrators of this site, please focus more on the morality & human rights affected by this pandemic. Each & every one of us has the right to live our lives, no one should be expected to sacrifice their lives for the greater good, someone else’s granny or Johnson’s poll ratings.
Following Science is all well & good, but science is just a tool to allow us to learn the best way of doing things, NOT necessarily the right way of doing things. It’s ludicrous to expect one generation to sacrifice its present & future for another, especially when those we are throwing our lives away for, have already lived theirs.
Let’s start seeing more moral & human rights arguments against pandemic mitigation measures! Science isn’t everything & the other side have no interest in facts & logic. Tip toeing around socialist values & “let it rip” accusations because you don’t want to be labelled callous, is surrendering the truth & science, never lose sight applied science is subjective & emotive.
There’s more to life than the science.
No one should be expected to sacrifice their lives for the greater good?
I presume you ignore Remembrance Sunday, then? And feel no gratitude to those who, over the centuries, have made that supreme sacrifice for the good of others?
Say, rather, that nobody should be expected to turn himself into a grovelling slave because lying tyrants tell him to. Just because almost everybody in Britain nowadays is a selfish coward, that doesn’t mean there is no such thing as self-sacrificing heroism.
Debate ‘This site would not fight for Queen & Country’.
I was born 12 years after the end of WW2 although that seemed ancient history to an infant.
I remain acutely aware that for the whole extent of my life this country has not been involved in an existential war (of the conventional sort), uniquely in our history I believe.
I might have been prepared to sacrifice my life for the country I grew up in, not that I would have been much use as a soldier.
That country is now in another place, the past (can’t remember whose words I reversed there) and I am not prepared to sacrifice anything for the entity that has replaced it.
“The past is another country. They do things differently there.” LP Hartley Opening of The Go Between
Thank you,
I have it on a freebie DVD. My main interest was the Michel Legrand soundtrack but it is a good film.
I think the boy repeats the phrase at the end as he looks back as an old man.
The idea that UK participation in either WW1 or WW2 was about “the greater good” is simply laughable.
WW1 seemed like folly and people went into it probably out of some misplaced loyalty
WW2 the motivations of our leaders may or may not have been honest but I think people believed they were fighting for their freedom, that there was an existential threat to our future – that’s not an unreasonable view, given that most of Europe had been conquered by the Germans.
.. a Germany actively funded by the American armaments industry, among others, and a leader, Hitler, promoted and supported by various individuals in Europe and the USA with an interest in having another even bigger world war, having found the previous one very profitable. … Some of the earliest soldier-sign-ups may have been motivated by altruism based on the propaganda and advertising which encouraged that attitude, but most were very soon conscripts.
No, I mean’t what I said & what I said, is what I mean’t.
The problem in debating this with you, of all people, is your establishment indoctrination. I don’t believe everything written in history books, it’s mostly myths & lies.
I remember the many who were executed for bravely saying no to establishment wars. Courage is knowing when to stand up against bullies, going against the flow for what’s right, not what you’re told is right by others.
This situation should never have been tolerated, government had no right to take yours or my freedoms, people should have said no from day one, by capitulating we empowered government to take more & do more & more. If non-compliance mean’t braking the law so be it, if it meant confrontation with the authorities so be it.
The state gives itself the right to use reasonable force, or even murder its citizens to defend itself, our government has instigated, facilitated & encouraged far greater violence in the name of freedom & democracy all over the world, it’s only right we have the moral & constitutional right to defend our own freedoms against tyrannical government!
Emotional blackmail doesn’t work on me. Let me be clear I am not condoning violence, I abhor any violent act, especially state violence, but as you point out self defence is self-preservation.
There has been a lack of any legal/moral opposition to government over-reach, where are all the human rights lawyers? Where are the intellectuals & academics? Where are the historians? Cowering under their beds in fear of losing their well-paid jobs, keeping them in comfortable lifestyles.
Don’t ever lecture me on bravery & courage in doing the right thing! I’ve been a lone voice on stating the fact government had no right to take your freedoms, collectivists had no right to take your freedoms, no one has the right to expect you to give your life for theirs! I’ve always gone against the grain when I believed it was right,
I, like many others, trusted my freedom to the government for two weeks to flatten the curve of what was being presented as a possible existential medical threat, the likes of which I knew to have appeared on rare occasions in the past.
Ever since it became screamingly obvious that Covid was no such thing the government has betrayed that trust.
I had the advantage of being out and about as a key worker, not in lockdown, able to use my eyes to see and to talk to frontline health practitioners who told me so but who were not given a voice by the corrupted media and who were threatened into public silence by their own management.
Great ‘Green’ Job Hoax: Only China Profits From Making Wind Turbines & Solar Panels
https://stopthesethings.com/2021/10/24/great-green-job-hoax-only-china-profits-from-making-wind-turbines-solar-panels/
China itself is building nuclear power plants and hundreds more coal-fired power plants, as if its economic livelihood depends on it.
….. join the peaceful resistance …..
Wednesday 27th October 11:30am
Yellow Boards Event – Stand by the Road
(If we start at 11:30am some people might join on their lunch break.)
Tesco Superstore
17 County Ln, Warfield, Bracknell RG42 3JP
Saturday 30th October 2pm
SPECIAL STAND WINDSOR with Yellow Boards
Alexander Park (near Bandstand) Stand in the Park
Barry Rd/Goswell Rd
Windsor SL4 1QY
Meet in the Park 2pm followed by walk to
Stand in the Town Centre By the Castle
About 2 hours in total.
Stand in the Park Wokingham Sundays 10am
Make friends – keep sane – talk freedom and have a laugh
Howard Palmer Gardens Wokingham RG40 2HD
behind the Cockpit Path car park in the centre of the town
JOIN Telegram http://t.me/astandintheparkbracknell
The ills of our society (in this area) won’t be cured until we relearn that personal and therefore population health is not a matter for government, but solely for personal responsibility and for genuine charity (not the coerced “charity” that is tax-funded expenditure).
The NHS is just the particular UK 1940s state socialist manifestation of this general social sickness of all modern societies.
It was heading this way some years ago when the NHSs concern for a patients individual health was replaced by prioritising Public Health (delivered via local authorities somehow).
Public Health means coercion of the individual for the greater good.
See todays opening comment by Anti_socialist above.
Public Health gave us effective sewage disposal, clean water, clean air and pest control, all of which are beneficial to all, it is when it crept into making demands on the healthy that things took a turn for the worse.
Agreed but I wasn’t thinking of those sort of essential services, rather medicinal ones as supplied by the NHS.
Public health these days seems to be little more than the debate about how many people you push in front of the train, to save people further down the track. When we have no idea whether pushing people in front of a train can stop it.
Exactly. This is about limits, not some airy-fairy absolutism.
You doubtless understand why it’s necessary to argue for absolutism in response to absolutism on the other side, in order to achieve a sensible resolution.
The absolutism that predominates, largely unquestioned, in our society is the idea that the state being responsible for public health is unquestionably good and necessary.
ITEM: “Criticism of Newcastle fans over Arab-clothing shows double standards”
I’ll piggyback the latest development on Novak Djokovic and the Australian Open (see Fox Sports) here because they’re both about sport.
After the federal government appeared to have slammed shut the gate on allowing Novak to even enter Australia by not granting visas to any unjabbed, a leaked email from Australia’s peak tennis governing body (Tennis Australia) to the world governing body for women professionals (the Women’s Tennis Association) suggests that unvaccinated players will be allowed into the country after all (and can play after two weeks hotel quarantine and regular PCR testing). Such an email would not have been allowed without serious behind-the-scenes consultation between the tennis body and the federal and Victorian state governments. So, Novak, by standing firm on not revealing his vaxx status to Australian political and tennis authorities, is causing them to wobble on their hard-line Vaxx Passport stance.
So there we have it. Tennis Australia mandates the Covid vaccine. The federal government huffs about not granting visas to he unvaxxed. The Victorian government, run by the evil gnome, Daniel Andrews, puffs about No Jab No Play at the Rod Laver Arena in Melbourne. Novak steadfastly returns serve to all of them and an email is conveniently leaked to find a way out of the acute embarrassment to the authorities of potentially blocking the star men’s attraction at the Oz Open.
There is still a fair bit of baseline rallying to go on all this before the Open in January but if Novak can win his vaxx passport battle, it will be a win for all others who face vaxx discrimination but lack his profile and social clout.
Thanks for the update, Phil.
Many more like Novak are desperately needed.
Good for him.
Wimbledon btw was one of the few major sporting events that had insured against losses caused a Pandemic for 2020. Not sure if they were allowed to cover this year as well.
I would hope he would still refuse to go on the grounds of the discriminatory hotel quarantine policy.
The hypocrisy over the Newcastle United takeover has been breathtaking.
I truly hope that Novak Djokovic will HOLD THE LINE.
Let’s go, NHS.
We’ve spent decades being harassed and nagged by campaigning homosexuals. Now the boot is on the other foot :
“Gay & lesbian NHS staff say they feel ‘unsafe’ and ‘scared’ by organisation’s pro-trans stance, LGB Alliance warns.”
https://www.rt.com/uk/538084-gay-lesbian-nhs-trans/
Dear me.
Nurses in crisp white dresses, but without cervixes. How does that make patients feel, I wonder? Supposing anybody ever bothers to ask the patients anything?
Stonewall and other LGBT groups, having won their campaigns for gay rights, have been infiltrated and taken over by trans entryists in the same way that ‘militant’ and Corbyns lot tried with the Labour party.
BBC Ulster have produced (broadcast?) a 10 part documentary about this and how Stonewall has become a protection racket demanding £2,500pa from public and private entities, great and small, for the privilege of being investigated and then graded depending on how low they bow before the altar of Trans Rights.
Trans Rights people enjoy being wined and dined in the corridors of power including Whitehall and Embassies but they came unstuck in that documentary when one of their leaders was unable to say what ‘twin spirit’ actually meant, likewise ‘gender-queer.’.
I read about this last week (UnHerd/Spiked?). It is remarkable that the BBC would allow such a thing to be produced as is a growing trend from entities within the wider grievance culture to tell Stonewall to sling their hook.
Similar action by public bodies like the Met Police or the BBC itself would allow the private sector and ‘third way’ to follow suit.
“Stonewall and other LGBT groups, having won their campaigns for gay rights, have been infiltrated and taken over by trans entryists in the same way that ‘militant’ and Corbyns lot tried with the Labour party.“
This makes it sound as though malignant organisations like Stonewall et al were fine until the evil modern newcomers “infiltrated” them.
In fact what is being done to them is precisely what they themselves did to organisations and people in wider society.
They haven’t become evil as a result of infiltration by evil people. They always were evil, like the other “minority” lobbyist groups. They have also become bloated and corrupt with power and wealth, but that is what always happens to successful political manipulation organisations – look at our political parties.
Agreed but they got worse once their fight was won.
Seeking a reason to believe perhaps or drunk on wealth and power as you say.
I always had a lot of time for Peter Tatchell who I regard as a very brave man. I understand that he walked away from Stonewall some years ago.
“in the same way that ‘militant’ and Corbyns lot tried with the Labour party.”
Your understanding of the dynamics of the Labour Party is a naive zero, as you waffle away in support of Srarmer.
I have never taken an interest in the internal dynamics of the Labour party ever since being in the student common room/bar listening to multiple tiny sects of lefties from mainstream Labour to Moaists and Pol Pot supporters hate and plot against each other rather than ‘fighting the tories’ or, better still, representing the actual interests of students.
Likewise I have never had a positive word to say about Starmer, if that is who you mean.
So tedious and I imagine patients will be way, way down at the bottom of the list of consideration.
The only ‘entertaining’ aspect would be how they navigate the tension between the alphabet people and those favoured ones who request females attended to by females and then an obvious bloke turns up.
We have our eldest and her family down for half term. She has had high anxiety for over year as a result of the propaganda.
This has meant that I have not expressed my concerns to her in detail – until last night as I felt the need to provide her information and to make an informed decision about booster jabs outweighed the risk of increasing her anxiety.
Very interesting to read the items in today’s round up and see that they back up much of what I said last night. Perhaps we are seeing the green shoots of realism beginning to appear in the mainstream.
The Telegraph seems to have prevented comments on the Sarah Knapton piece about model predictions.
Guess the overwhelming flow is critical of The Narrative.
The article is fascinating. She talks about models “finding” the impact of measures such as masks.
No model can “find” anything unless the assumptions are correct.
She calls herself a Science Editor but makes no comment on that.
The level of debate is very poor. These people seriously think everyone is stupid.
Well, they know that almost everybody is stupid..
Yes, Knapton’s articles nearly always expose her incredibly poor understanding of science. The Telegraph should be ashamed to have her on the payroll!
Spectator ‘Will Savid Javid fire unvaxxed health workers’
“Thee years ago those staff who refused to take the (normal) flu vaccine were redeployed to non clinical areas” says the article.
12 months or more ago they did something similar locally, and perhaps eleswhere.
As the NHS Trust became overwhelmed and understaffed by the numbers of employees claiming to be vulnerable to Covid by virtue of their medical background the Trust started to redeploy them away from public facing roles.
Previously, from the beginning of Lockdown, if a member of staff contacted HR saying “Covid might get me because I’m obese”
they were simply sent home on full pay for weeks or months on end.
HR initially imagined that they had no right to examine such claims (cf mask exemptions) until a real staffing crisis almost crashed down on them, only then did they call those people back in and set them to doing something useful.
I do wonder if Javid and Sunak are looking for a major reform of healthcare however, the NHS has a sacred deity status in the UK and so how do you reform it and not commit political suicide? One solution might be to create chaos in the care and health sector but be able to blame it on the selfish un-vaccinated care and health workers. They can then try to recover from the chaos by bringing in their reforms.
The NHS does need reform but I cannot see Javid and Sunak bringing in any reforms that would be anywhere near what I would like to see.
Re:“After Strong Denials, NIH Admits Funded Gain-of-Function Research at Wuhan Lab” – May I recommend the book by Peter McCullough et al., ‘COVID-19 and the Global Predators – We Are The Prey’ and which outlines the role that the likes of Antony Fauci, Bill Gates, the WHO and the CCP have in this tawdry and anti-human affair.
These organisations and characters have to answer for their crimes against humanity.
Thanks for the recommendation but I feel educated enough about Fouci and the rest; his illegal funding of gain of function experimentation is just one of the crimes he needs to atone for.
‘Resist Covid restrictions for the sake of our young ‘. Good article from the Daily Mail citing demands from the NHS Confederation to implement Plan B.
I might be wrong but isn’t the NHS Confederation a body of Trust Managers and accountants that don’t represent the front line at all, just as the CBI does not represent the workforce.
Its very existence demonstrates how unwieldy the NHS has become if they need a Confederation just to keep in touch with each other and present a united front to government and the press.
‘Plan B’ (from Outer Space?) won’t come in until after the climate conference I am sure. It would be very embarrassing for Johnson if new restrictions were brought in when tens of thousands of delegates from around the world are wining, dining and partying in the UK. Once it’s over, anything can happen.
A friend is a bell-ringer in a local church. The diocese management have issued guidelines on CO2 levels for bell ringers and provide a CO2 monitor that can me used during ringing sessions.
My friend reports that the level of CO2 vary tremendously depending where in the room the monitor is placed – I think he left it next to an open window.
I should add that the person who delivered the meter seemed to believe it was a live Covid detector and that the measurement was the actual level of virus particles in the air.
UNBELIEVABLE!!!
‘Cambridge University to slap trigger warnings on classic books’. Daily Mail.
Decades ago I worked in the video distribution industry (legit but C list movies, no porn) which runs in much the way as music distribution.
One of my tasks was to ensure that each film we were promoting to video shops and retailers was properly certificated by the BBFC, sometimes entailing a visit to them in Wardour St. where I would tell them what certificate we wanted.
The marketing people would make sure to keep in every frame of sex, violence and swearing to get as old an age classification as possible.
Should the BBFC bump it down from a 15 rating to a 12 this was a disaster as no self respecting boy (dunno about girls) would want to share a sissy R12 video with his mates.
I imagine much the same with children books ‘flagged’ by Cambridge, kids making a beeline for them hoping to find the good bits.
Own Goal Cambtidge.
Unfortunately the link is broken so we can’t see what the expansion will include, but I bet few on here will have realised that the government questionnaire about the vaxport was altered in the final days before it was whipped away.
They changed it so that following every question on people being forced to be jabbed for covid to do their job was the same question but regarding the flu jab. So even before the questionnaire was allowed to run its cause, they’d already radically shifted the goalposts without most people realising it had happened.
It doesn’t really matter, the BBC are just using Wales to normalise (dreadful word but useful) vax passes before making them compulsory UK wide.
New year fireworks display stopped in London.
Goose fair in Nottingham stopped
Bonfire night displays may or may not go ahead
Don’t go trick or treating
But this happens in Leicester https://www.leicestermercury.co.uk/news/leicester-news/gallery/leicester-lights-up-thousands-celebrate-6107281
Leicester, the most locked down city in the country was in Tier 4 before they invented Tiers because culture innit.
Meanwhile in London the river Thames New Years Eve fireworks have been cancelled but Diwali goes ahead with 35,000 expected to crowd Trafalgar Square. Good luck to them, hope they have a great time but the double standards of our overlordlings is galling.
Public firework events in small to medium towns here in the SW are still going ahead apparently.
Dear God,just when you think that you’ve seen the worst of the maskateers.
Just returned from our Local CO-OP where I witnessed one of the most stomach churning episodes since this whole madness began.
A (I hesitate to use the word) man actually grovelling in front of an embarrassed checkout assistant,apologising that he had forgotten his mask and covering his mouth and nose with his arm and trying to pay at the same time.
Even 20 minutes after it happened, I’m wondering: ” Was I dreaming?” but the terrible truth is, No ,I wasn’t and I know that this is not an isolated incident
Will normality ever return?, I’m beginning to wonder.
Just in:
EcoHealth Throws NIH Under The Bus Over Wuhan Gain-Of-Function Report; Researcher Claims ‘Massive Cover-Up’
https://www.zerohedge.com/political/ecohealth-throws-fauci-under-bus-over-wuhan-gain-function-report-researcher-claims?utm_source=&utm_medium=email&utm_campaign=209
I noticed that Prof. Hugh Montgomery is again writing in the Daily Telegraph: ‘I’m fed up with anti-vaxxers taking up hospital beds’ “What gets him, he says, is that many of the patients he is treating shouldn’t be there. ICU beds, which could be used for cancer patients, or elderly people needing hip replacements, are being taken up by anti-vaxxers and Covid-deniers….”
Back in December 2020 he was telling the BBC that Covid rule-breakers ‘have blood on their hands’ He was telling the BBC back then “We are in a lot of trouble in UK intensive care now.” And here we are, nearly a year later, after lockdowns, mask wearing, jabs, double jabs, booster jabs, and the fallout of business failures, anxiety, lengthened waiting lists, debt, inflation, and yet still it’s people who think the Government has over-reacted to this virus who are being blamed.
The Daily Telegraph tells us “he has just finished a 24-hour shift. He looks knackered and beaten, but not by the hours” but by treating those of us who “shouldn’t be there”. Maybe he’d be less “knackered and beaten” if, after his 24-hour shift, he went to bed and stopped his media interviews.