
How might Covid vaccines reduce mortality?
There are two possible mechanisms, thoughtfully explained in a thorough review and a recent article on Brownstone: Covid vaccines might reduce the risk of infection, or reduce the risk of death — if infected, or both. We can explain the mechanisms in words, with reference to ‘marginal and conditional probabilities’, or we can depict them in a causal diagram — a powerful methodological tool.
The first mechanism is simple: If a Covid vaccine reduces the risk of infection, it will also reduce the risk of death, because there is no doubt that getting infected increases the risk of death. Theoretical exceptions aside, if A affects B, and B affects C, then A affects C.
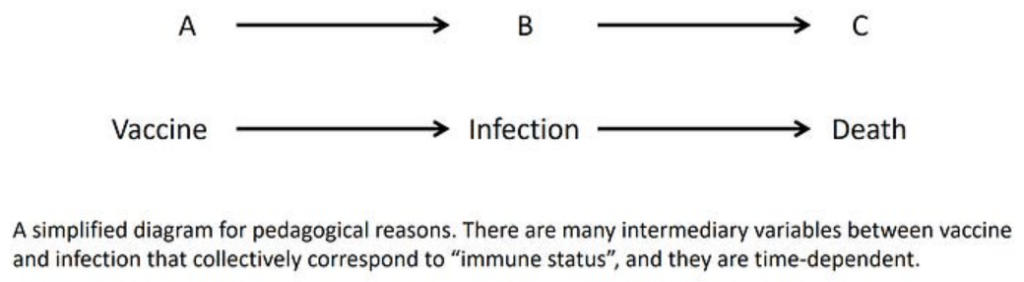
What if A does not affect B? What if a Covid vaccine does not reduce the risk of infection? Then it cannot reduce the risk of death through this mechanism. The causal chain does not exist. A link is broken.
By now we know that Covid vaccines appear temporarily to increase the risk of infection, and any subsequent benefit is nullified within months, if not turned again into harm (negative vaccine effectiveness). Therefore, according to the first mechanism, there is a short period when a Covid vaccine increases the risk of death, a limited period (a few months) when it decreases the risk of death, and a later period when the effect is null at best.
The second mechanism is more complicated. One aspect was explained in the Brownstone article and is related to a causal concept called ‘effect modification’. Like numerous epidemiological concepts, there are layers of complexity below superficial simplicity. I will keep it simple.
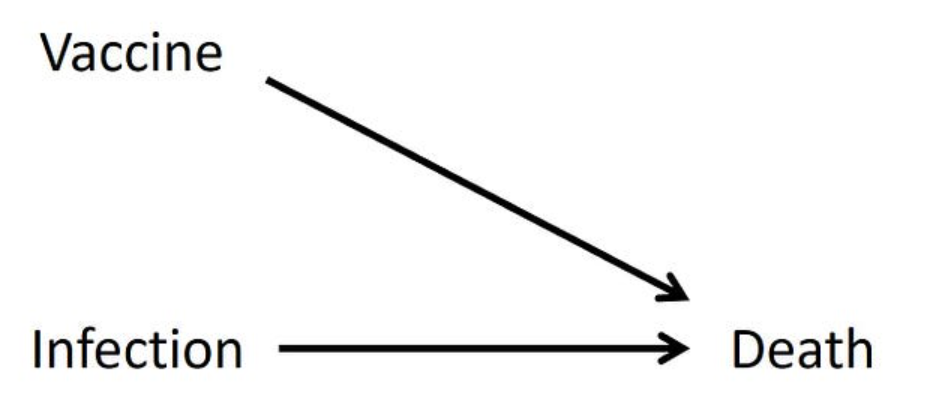
When two causes — Covid vaccine and Covid infection — operate on a single outcome (death), we may ask two causal questions:
- What is the effect of a Covid vaccine on the risk of death — if infected?
- What is the effect of a Covid vaccine on the risk of death — if not infected?
The second question is asking about vaccine-related death, the worst adverse effect. (A vaccine can be a cause of death even when someone is infected, but that’s another issue.)
Theoretically, the two types of effect could be different, in any possible way: magnitude and direction. Both might be harmful effects, yet of different magnitude. One might be beneficial and the other null, and so on. Add to that complexity time-varying effects, as noted earlier, and you can see how complicated causal reality might be.
Coincidentally, I encountered a relevant study at about the same time that I read the Brownstone article. That study provides insight into the two mechanisms by which Covid vaccines might reduce the risk of death, although the authors missed one aspect of their data (regarding reduced infections) and stopped short of the computation for the other (reduced mortality, if infected).
That’s not surprising. At times of biased media and biased science, we sometimes find insight from narrative-matched publications that missed interesting inference from the data.
Published as a ‘research letter‘, the study compared Covid mortality with mortality from seasonal flu. Using databases of the U.S. Department of Veterans Affairs (VA), the researchers identified patients who were hospitalised with an admission diagnosis of Covid or influenza and ascertained deaths. Most patients were elderly, the age group where Covid mortality is concentrated and effective vaccines are needed.
Did Covid vaccines reduce infections? Although the design was a classical retrospective cohort, the baseline data in the first table may be viewed as data from a hospital-based case-control study. (I cannot get into a technical explanation of ‘propensity score weighting’, but it can be ignored for a basic case-control analysis.)
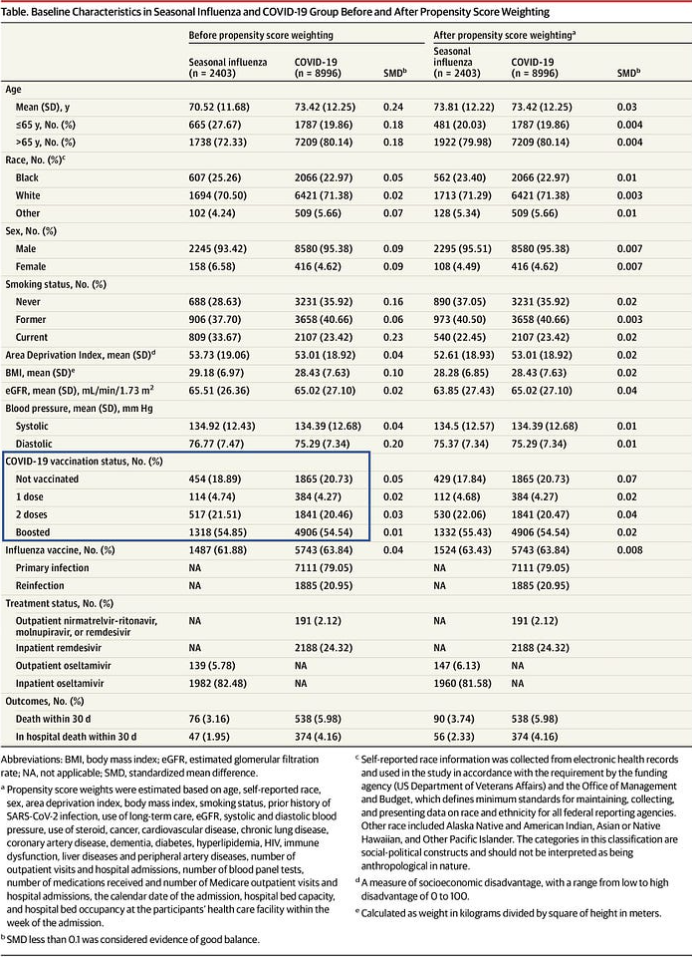
We may consider Covid patients as cases (numbering 8,996) and seasonal influenza patients as controls (there are 2,403). In a typical hospital-based case-control study, controls are selected from multiple disease categories, but I don’t see a major problem with this control group, and perhaps there are referral-related advantages.
Many complicated issues arise from a case-control study. Nonetheless, the basic analysis is simple. We visually compare the distribution of the suspected causal variable (Covid vaccination status) in cases and controls and compute odds ratios. If the vaccines meaningfully reduced the risk of infection, we should get odds ratios much smaller than 1.
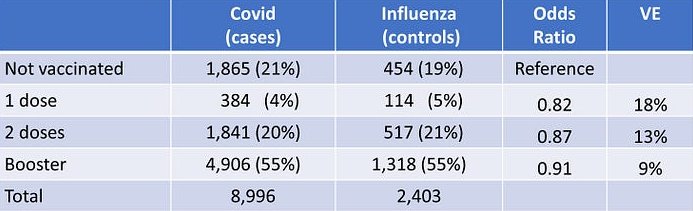
We have no such evidence in these data. The odds ratios are close to 1 (close to zero vaccine effectiveness) and they line up in the ‘wrong’ (unexpected) order of magnitude: the larger the number of doses, the weaker the apparent effect. The causal chain from vaccination to reduced mortality through reduced Covid infections is not corroborated.
Interestingly, we may also view influenza patients as cases and Covid patients as controls and compare the distribution of flu vaccination status in the two groups. Check their table above. There is no meaningful association either.
Might biases account for near-null associations? Biasing paths typically lead to a statistical association when there is no real cause-and-effect relation. Random error aside, it is unusual for biases to turn strong effects into near-null associations.
Did Covid vaccines reduce mortality, if infected? We turn next to the second mechanism by which a Covid vaccine might reduce mortality: reducing the risk of death, if infected. That part was addressed in the original design. Every member of the cohort was infected, either by SARS-Cov-2 or by influenza.
The authors have focused on a comparison of Covid mortality with flu mortality, but they added a secondary conclusion:
The increased risk of death was greater among unvaccinated individuals compared with those vaccinated or boosted — findings that highlight the importance of vaccination in reducing risk of COVID-19 death.
How important is vaccination? What was the vaccine effectiveness — if infected? They don’t say.
If Covid vaccines no longer reduce the risk of infection, that’s the only source of vaccine effectiveness (VE) against death.
Below you will find their table and my computation:
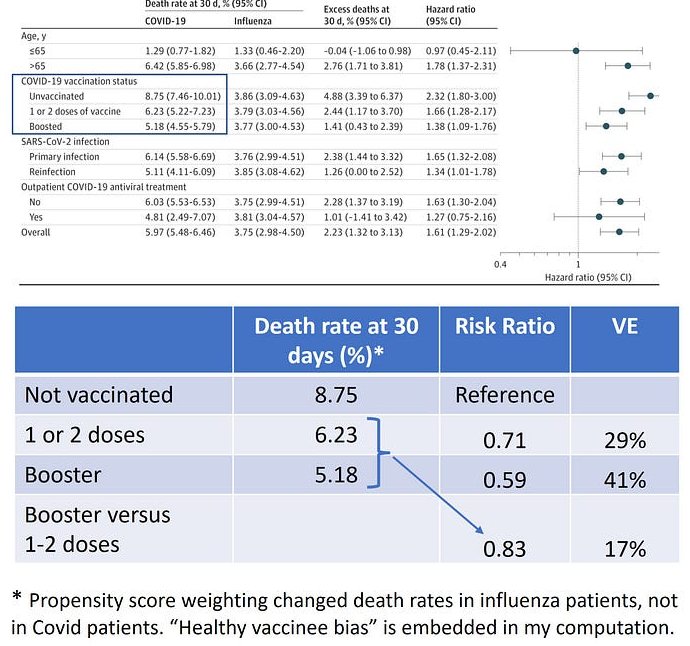
VE of 30% or 40% in the vulnerable population is far from ‘highly effective’, a perpetuated claim. The incremental benefit of booster vaccine (one or more doses, per supplementary material) was even smaller (risk ratio 0.83, VE 17%).
Moreover, 30% to 40% is not necessarily the true effectiveness. We have clear evidence of ‘healthy vaccinee bias‘, a type of confounding bias, in both the U.S. and the U.K.. People of the same age who were vaccinated against Covid were healthier, on average, than their unvaccinated counterparts, as evident by lower non-Covid mortality. Therefore, the unbiased VE should be smaller. For example, a modest bias correction factor around 1.5 would drive VE of 40% close to zero.
Billions have been vaccinated under the slogan ”safe and effective’.
It was neither.
Dr. Eyal Shahar is Professor Emeritus of Public Health at the University of Arizona. This article first appeared on Medium.












To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
This was in your “News Round-Up” section this morning and worthy of an article here.
Not that us unjabbed needed any convincing that we made the right decision.
Well-said
When the authorities tell me they have the solution for a problem they invented and that I must participate, I already know I want nothing to do with it.
Imagine a vaccine so safe I must be forced to take it, to protect me from a virus so deadly I must be tested to find out if I have it.
‘The Science’ said on ITV and elsewhere that you would not die from anything….funny that. 92% of the dead in the UK since the Dec 2020 stab campaign were all jagged. The deaths spike post every stab program. That is all you need to know. The stab IFR was 4-5x worse than the flu-scamdemic.
I think any rational person would agree with the author, including Joel Smalley, looking here at the South Korean data;
”Based on the evidence, and a massive dose of logic (and no censorship because I’m not beholden to any indoctrination education establishment or publishing in any controlled “medical” journals, I consider the COVID deaths to be jab deaths, as well as all the other excess deaths – unless you really think that “lockdown” deaths only coincidentally occur after jabs, naturally…).
So, that’s roughly 70,000 jab deaths on a vaccinated population of around 38.7 million. In other words, a jab fatality rate of 0.18% which is pretty consistent with quite a few other studies, including the infamous Skidmore one retracted involuntarily.
If we extrapolate that across the whole “vaccinated” world (5.57 billion according to OWID), I estimate just over 10 million people have been killed by the jab. That compares to 6.9 million “COVID” deaths (which includes a whole load that are actually jab deaths as I have set out above), i.e. at least 150%.
I know it’s a collective effort but that would put all the world “leaders” who sanctioned the democide in their countries at 4th spot in the table of most murderous dictators, behind Hitler (17 million), Stalin (23 million) and Mao Zedong (50+ million).”
https://metatron.substack.com/p/the-jab-has-killed-more-than-50-more
There is another mechanism which seems to be steadfastly overlooked.
What if (viral) infection does not increase the risk of death, because the major risk arises from other factors, age, decrepitude which which will cause death anyway.
If you have just got out of the swimming pool, how much wetter do you get if it is raining? Would you be drier without the rain? If your house is a raging inferno, would throwing a fire-lighter on it make it worse?
Therefore the vaxxed die anyway even if not from the vaccine nor the infection.
What would be interesting is some data on date and health status of the ever vaxxed, then date of death. Exclude deaths from CoVid. My thinking is the interval from vax to death in the ‘vulnerable’ cohort will be no different to that of the unvaxxed within the same cohort.
Average age at death of alleged CoVid victims, 82 years, 95% of whom with one or more comorbidities. (Average life expectancy is 81.)
So what killed them and would they have lived without CoVid and for how long?
Average life expectancy is 81.
When the “vaccines” came out, I looked at my chances of dying based on govt stats over past few years compared to during the “pandemic” and the difference was miniscule. I decided that taking a “vaccine” that had not been subject to normal testing and approval protocols, and that used a novel approach, to supposedly reduce my chances of dying by some tiny percentage, was daft.
True, but many, many people weren’t given the choice of making their own minds up. It was jab or job.. And anyway. They wouldn’t give us something patently unsafe, would they…
One person I know got jabbed because of the job – care home worker. Everyone else believed in it or wanted to travel or felt pressured by family.
AFAIK it was just care home workers who were legally forced, and threat to NHS workers.
Nobody in this country was legally forced. Fact. Too late for many to accept this, though…
Initially (I even made a comment about this some years back), I was perfectly willing to get vaccinated against COVID despite I considered this a usless exercise (IMO, the chance that anbody managed to avoid exposure to Sars-CoV2 until vaccination became available in December 2020 was zero and I certainly didn’t manage myself) as quid pro quo deal with Corona’s witnesses: I’m willing to accept this injection just because you want me to do that if this means I’ll get my life back afterwards as the reason for your virus paranoia is now gone. I changed my opinion on this when it became clear that the Sars-CoV2 apostles weren’t the least bit willing to keep their part of the bargain but just regarded eternal repeat-covaxxing as another integral part of their new normal.
With the benefit of hindsight, my position on this is now that Sars-CoV2 is (as always) an unavoidable health risk and getting covaxxed an avoidable one. Hence, it is to be avoided.
I’m a hypochondriac with history of autoimmune disorders so I was always going to be wary of an untested treatment. I guess a lot of people thought it was risk-free so just went ahead.
I didn’t get jabbed because I couldn’t think of a benign explanation for the government’s desire to jab us all with experimental gunk, produced by known crooks, that couldn’t possibly have been properly tested, in response to something that posed a trivial threat to the vast majority of the population.
That was my position as well Nearhorburian. Since the jabs had been rushed through an obviously defective testing regime (they couldn’t possibly condense 10 years into one year) and there was no medium to long-term adverse effects data, I checked the details of the Government’s compensation scheme. This was particularly important since we knew Big Pharma had been indemnified against claims.
It was obvious that the Vaccine Damage Compensation Scheme was inadequate. £120,000 for death or 60% disablement, IF you qualified, was far, far too little. I live alone, if I was injured that amount of money wouldn’t cover the cost of care for a year let alone the rest of my life. And you had to prove your claim. So who was going to do that, if I was severely incapacitated?
If I was severely injured it wouldn’t just ruin my life, it would have ruined my sons’ lives as well since they would have had to take care of me.
I knew I wasn’t at risk from the virus. I knew the jabs didn’t stop you getting it. I knew the safety data wasn’t there. I knew the testing regime was defective. And I knew the compensation scheme was inadequate and hard to claim.
It was a no brainer …….
30 years ago I read a book called Nature’s Child by Leslie Kenton. She mentioned that her unvaccinated children were healthier than her vaccinated children. This piqued my curiosity – my first child had just been born. The health visitor said “if you have any vaccine concerns discuss them with me” I said I had none, she then repeated the line about vaccine concerns. I started reading and researching around vaccines and since then have been avoiding them where possible and keeping my 3 children vaccine free for as long as I could.
( I am also trying to keep my animals vaccine free. So much money to be made by jabbing pets and livestock.)
There are many questions about the contents of the products, thimersol, PEG, SV40, what were those scientists doing in the early 20th century in Africa with monkeys? The more you look at it the more it appears to be sorcery, “double double toil and trouble …eye of newt and toe of frog…” and that was before I read the book Dissolving Illusions | Disease, Vaccines, and the Forgotten History – Dissolving Illusions details facts and figures from long-overlooked medical journals, books, newspapers, and other sources. Using myth-shattering graphs, this book shows that vaccines, antibiotics, and other medical interventions are not responsible for the increase in lifespan and the decline in mortality from infectious diseases.
And finally one needs to be aware of the indemnity offered by governments to pharma and then like all or most of you one realised that this was not what the authorities claimed it was.
What I thought earlier though was why not jab everyone with saline and then everyone would be lulled into a false sense of safety and fortunes could be made with no collateral damage? The “product” would be safe and it would have made no difference to the mortality figures.
My conclusion is that we are being treated as lab rats.
Whilst trying to avoid falling into linguistic errors (no shortage of those by the usual suspects), it’s worth noting that the early 2021 pamphlets promoting the use of the jabs did not promise that they could protect against infection – only that it would reduce the severity of it. So, they knew that A does not cause B.
Thus we are into the complexity of the real world, with a mixture of different cause and effect combinations. The jury is still out as to whether the products that have been promoted actually delivered any direct biological benefit to anyone. However, I’m glad that when offered it in March 2021, I’m glad I said “no, not yet, until it becomes an established product”. I haven’t changed my mind yet.
More understandable than Igor Chudov’s take on the same data and well worth a separate space ATL.
In that context, I very much recommend a look this piece as well:
https://www.unz.com/article/how-effective-are-the-covid-vaccines/
It also shows that the trials already demonstrated that the very opposite was true.
The stunning piece by Madhava Setty linked to at the News Roundup today mentions the very same, as its author has analysed in detail in prior articles, as well as exposes the ignorance about it among ‘vaccinators’.
https://madhavasetty.substack.com/p/from-the-belly-of-the-beast?r=gs9pw&utm_campaign=post&utm_medium=email
I concur with JayBee that the article, ‘From The Belly Of The Beast, by Madhava Setty, is a wonderfully written piece, very well worth reading.
I noticed throughout how vaccine zealotry is very much like a religious cult.
Remember this?
https://www.youtube.com/watch?v=5s0BDxL6LA0&t=9s
Bill Gates: ‘It Looks Like Almost All The Vaccines Are Going To Succeed’ | TODAY
In this Gates also says that wearing masks is very important.
With an absolute risk reduction in the range of 0.85, from the Pfizer vaccine….and, according to John Ioannidis an IFR of 0.095 in my age range…exactly how effective could the vaccine ever have been for, not only me, but huge swathes of the general public……..Or am I missing something?
Serious illness from SARS-CoV-2 results from how the body reacts to infection. The hyperimmune syndrome or cytokine storm, COVID-19, can be mimicked, at least in some respects, by the vaccines which are derived from the spike protein. It is not the virus that kills. Reducing the death rate is only possible if (1) the virus mutates so it is less likely to provoke a hyperimmune response – which has happened – or (2) if the correct treatment for the cytokine storm is deployed. Though this latter was unnecessarily delayed, as I have repeatedly pointed out, it has happened. So – vaccinination cannot stop infection, and the reduction in death risk is due to other factors, which have been ignored in official accounts of vaccination efficacy. Which of course begs the question of why myocarditis and thrombocytopenia following vaccination have not been treated in a timely fashion.
I believe Peter McCullough said myocarditis cannot be treated, only managed. It is irreversible damage. Does anyone know differently?
“If Covid vaccines no longer reduce the risk of infection, that’s the only source of vaccine effectiveness (VE) against death.”
What about the claim that vaccines reduce symptoms? By looking at people already in hospital, you have removed people whose symptoms were reduced and so did not enter hospital.