When did the coronavirus first appear and begin spreading? Did it emerge in December in the Huanan wet market, or did it leak from the Wuhan Institute of Virology in November, or was it intentionally released at the World Military Games in October? Was it spreading internationally during autumn 2019? Has it been around for years?
Here I’ll present evidence that the coronavirus appeared at some point in the second half of 2019 and was spreading globally during that autumn and winter.
There have been a number of studies that have gone back and tested stored samples for evidence of the coronavirus, either antibodies or viral RNA. One of the most intriguing is a study from Lombardy in northern Italy by measles researchers (Amendola et al.) who had spotted that Covid could cause a measles-like syndrome (though the evidence on this claim is not fully clear and a measles-like rash was not a widely publicised symptom of the disease). The researchers tested hundreds of stored samples taken during 2018-20 for both antibodies and viral RNA. Eleven of the samples were positive for viral RNA from August 2019 to February 2020, including one from September, five from October, one from November and two from December. Four of these were also positive for antibodies, including the earliest sample from September 12th 2019 (both IgG and IgM). A striking 25% of the samples from September to December were positive for viral RNA, which seems on the high side even considering these were samples from people visiting hospital with measles symptoms; the percentage positive then oddly dropped to 16.7% in January and February 2020. The positive samples were genetically sequenced to reveal mutation information, reducing the chances of them being false positives – though it should be noted that the positives were of partial sequences, not complete ones, so cross-reaction remains a possibility. In addition, none of the samples tested positive on a SARS-CoV-2 PCR test and the first to be positive on more than one RNA component – the first strong evidence of true infection – was from December 15th in Milan. Comparison was made with a control group of 100 samples from August 2018 to August 2019, none of which were positive on any RNA fragment, though 12 were positive for at least one antibody, a result which the researchers called “inconclusive”. Their results led them to estimate that the virus emerged around July 2019.
A separate study in northern Italy tested waste water from 2019 for viral RNA and found samples in Milan and Turin positive from December 18th, though negative prior to that, which is in contrast to the results of the first study – though in line with when the first strong positive turned up in Milan. The samples were again genetically sequenced, adding to their reliability.
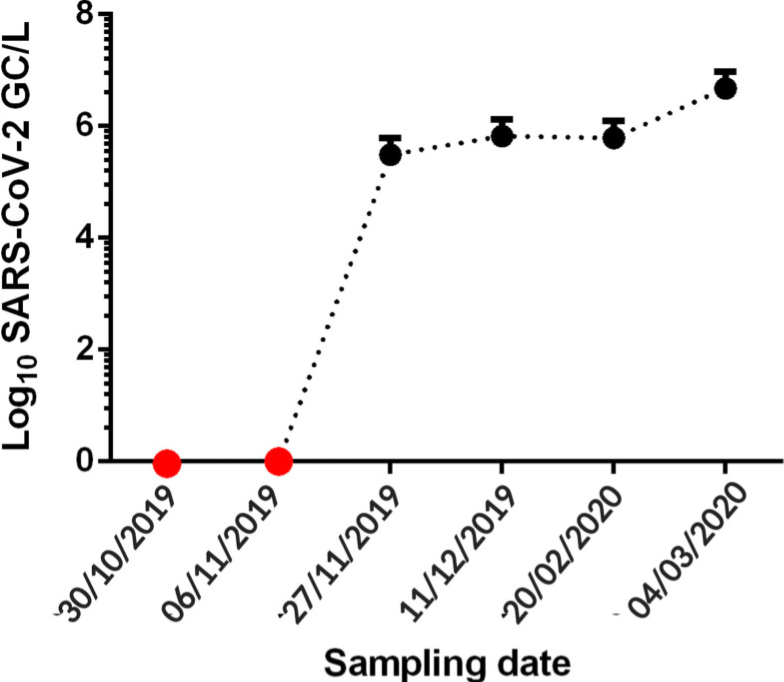
A Brazilian sewage study found SARS-CoV-2 RNA in samples from late November and December 2019, but not in two earlier samples from October and early November. The samples were taken from one site in the southern Brazilian city of Florianópolis and were genetically sequenced for confirmation.
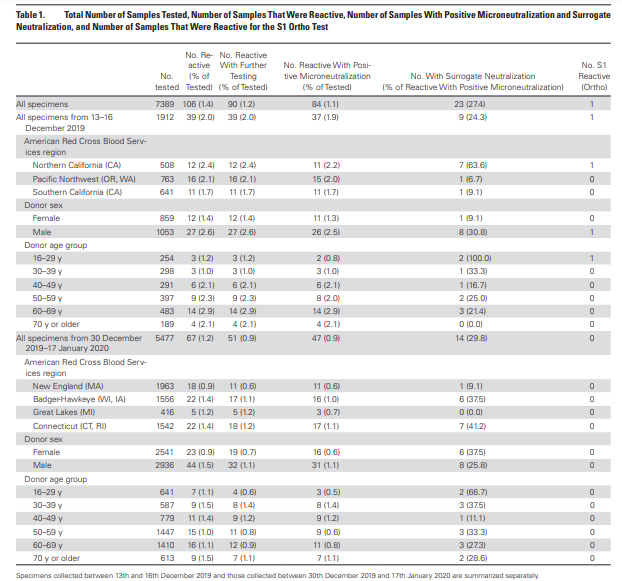
An antibody study of archived Red Cross blood conducted by the U.S. CDC found 39 antibody-positive serum samples collected December 13th-16th 2019 in California, Washington and Oregon. Overall, 2% of blood samples collected from these states on these dates tested positive for antibodies. The full results can be viewed in the table below. A 2% antibody prevalence in mid-December suggests significant community spread across America during November 2019. However, there were no earlier samples for comparison and no testing or sequencing of viral RNA for confirmation.
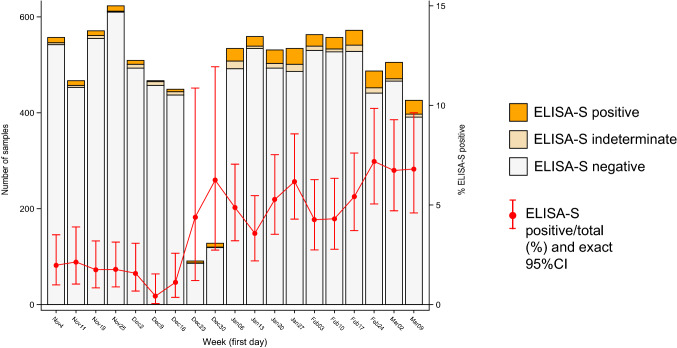
A study of stored blood samples in France examined hundreds of routinely collected samples in a population cohort and found around 2% prevalence of antibodies in November, rising prevalence in December and around 5% prevalence in January. These figures do seem on the high side when compared to the above studies, and the lack of testing and sequencing of viral RNA and the absence of samples from earlier periods suggest this may be less reliable evidence.
Another Italian study (Apolone et al.) tested blood samples from lung cancer screening for SARS-CoV-2 antibodies and found 14% of those from September 2019 were positive for SARS-CoV-2 antibodies, rising to 16% in October though oddly dropping back to 3% in January 2020. These pre-pandemic results are again on the high side and lack testing and sequencing of viral RNA as well as negative controls from earlier periods, meaning they may be cross-reacting. A Spanish study detected SARS-CoV-2 viral RNA in a sample of waste water from Barcelona on March 12th 2019; however, all the other historic samples up to January 2020 were negative and it is suspected that this is a false positive due to contamination or cross-reaction (the sample wasn’t sequenced).
What about early spread in China? It’s hard to get reliable data for this country. However, a leaked Chinese Government report found hospital patients (recognised retrospectively) admitted in Wuhan from November 17th 2019, suggesting the virus was spreading there during November and probably October.
A molecular clock study estimating the date at which the common ancestor of early viral samples was around put the emergence of SARS-CoV-2 as early as July, in China. A separate molecular clock study estimated the emergence between mid-October and mid-November in Hubei province, China; another put the emergence between early October and early December and reviewed other studies which found similar. A fourth estimated an emergence in late October with global spread occurring throughout the winter.
There is considerable evidence, then, that the virus was circulating both in China and internationally by November 2019 at the latest. We can also say with strong confidence that it was not circulating prior to July 2019, and it may not have been around before October 2019, depending on how reliable the European data from the early autumn are.
Some argue that all this evidence of early spread – despite coming from multiple sources and using robust validation methods such as sequencing – must be faulty in some way, as the lack of excess deaths prior to March 2020 makes it impossible for the virus to have been spreading widely over the autumn and winter.
My view is that this argument is insufficient to overcome the clear evidence of early spread. I don’t deny that there is something of a ‘mystery‘ that must be resolved insofar as the waves of excess deaths did not begin until March 2020. Some sceptics resolve this ‘mystery’ by arguing that the virus must therefore be no more deadly than other similar viruses, and thus that any excess deaths since March 2020 must all have been caused by interventions such as lockdowns, faulty treatment protocols and vaccines. However, I agree with Dr. Pierre Kory that we have undeniable evidence of waves of severe pneumonia with a common clinical profile that began in March 2020 and that are best explained by the novel respiratory virus to which most of the deceased tested positive. While some of the excess deaths will be due to interventions, and some of the Covid deaths will be misclassified, the majority of additional deaths from a respiratory cause will be due to the virus. Professor John Ioannidis used antibody data to estimate that the infection fatality rate in the Americas and Europe in the first wave was around 0.3-0.4% (higher in hot spots), which is several-fold higher than flu, usually estimated at around 0.1%.
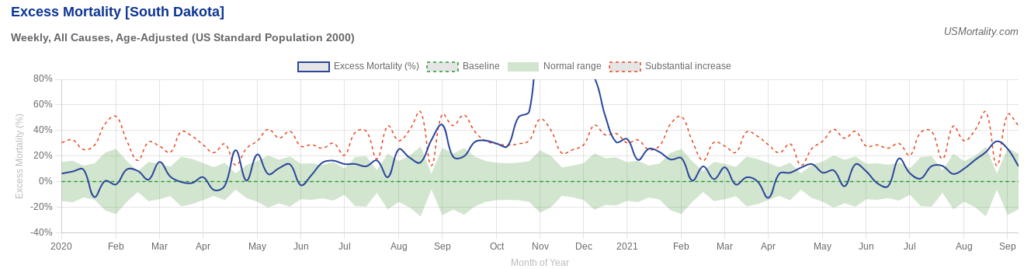
A good counterexample to the claim that all the excess deaths in the pandemic were caused by interventions and not the virus is South Dakota, which imposed very few interventions. Despite this laissez-faire approach it had a mild spring wave; yet then had a massive summer wave that resulted in greatly elevated deaths during the autumn. These deaths certainly can’t be put down to sudden panic: the state was so relaxed during its summer outbreak that it held a massive motorcycle rally.
So how to explain the lack of excess deaths during the autumn and winter of 2019-20? The most important point to be made is that while SARS-CoV-2 was clearly circulating during that winter, it does not appear to have been the dominant virus either in the community or in care homes and hospitals. Thus while, say, 2% of the population may have contracted the virus during the winter, because it was competing with other, milder viruses and wasn’t running rampant among the high risk population, its impact was limited and it did not cause noticeable excess deaths.
The early-spread-sceptic’s objection to this point is that the virus is clearly highly infectious so if it was present and circulating it’s simply not possible for it to have remained at a low level and not run rampant in, say, care homes, causing havoc.
But is it really true that the virus always causes a large wave of infections and deaths whenever it is present, and as soon as it arrives? The evidence suggests not. Just look at how it failed to take off in many places in spring 2020, not just South Dakota, but Japan, South Korea, Germany, Eastern Europe and large parts of the U.S. India notably wasn’t hit hard till Delta in 2021, and East Asia not until Omicron. In other words, the virus doesn’t always do what we’d expect, and in particular it doesn’t always cause a large, deadly wave as soon as it is present.
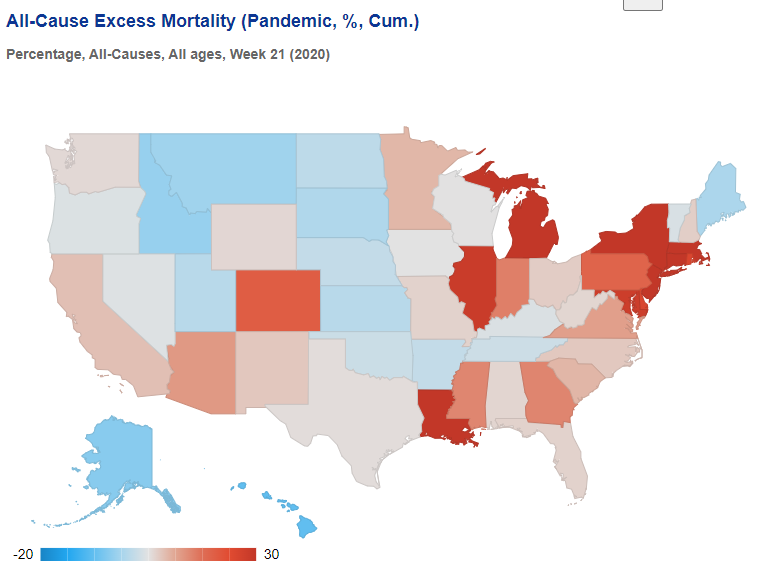
To illustrate, here’s the picture in the U.S. at the end of May 2020, after the initial wave. It’s a real patchwork, with clear concentrations of excess deaths around New York and around Michigan, Illinois and Indiana, plus Louisiana and one or two other states. Many other states had very few excess deaths during the spring. Yet we know the virus was circulating widely in every state.
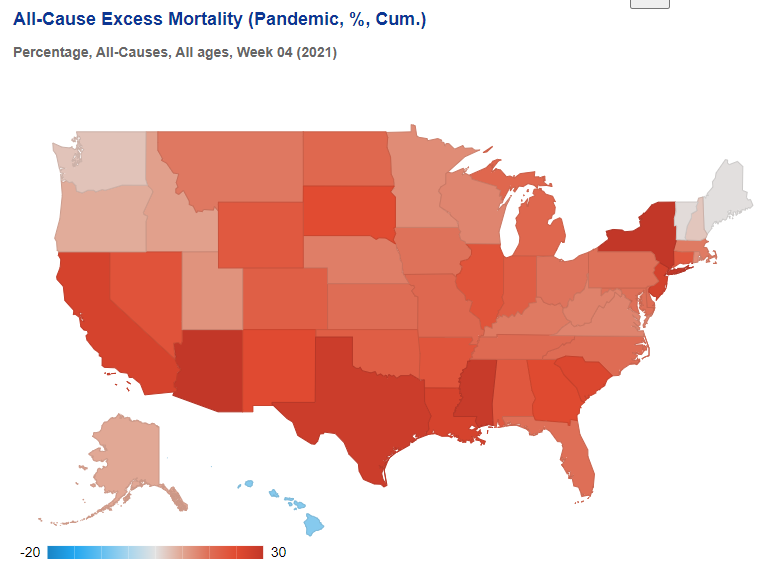
Then, by the following winter, excess deaths were high almost everywhere, meaning specific local treatment protocols or policy responses cannot be credited either with causing the deaths or averting them.
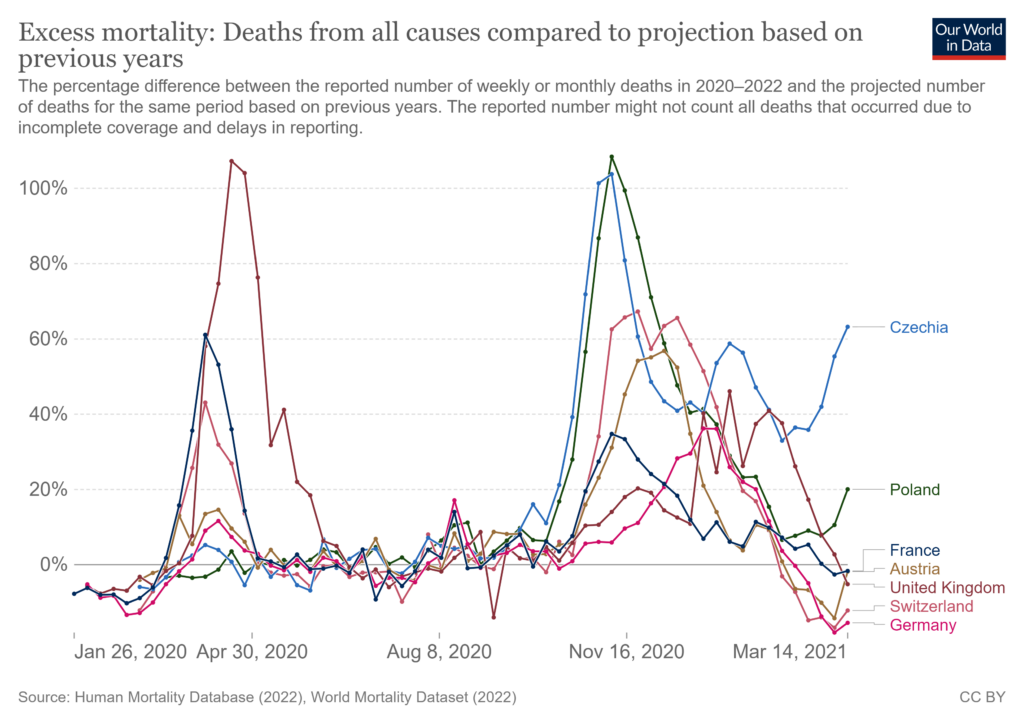
In Europe, too, there was huge variation in the impact during the initial spring wave, even though the virus was circulating everywhere.
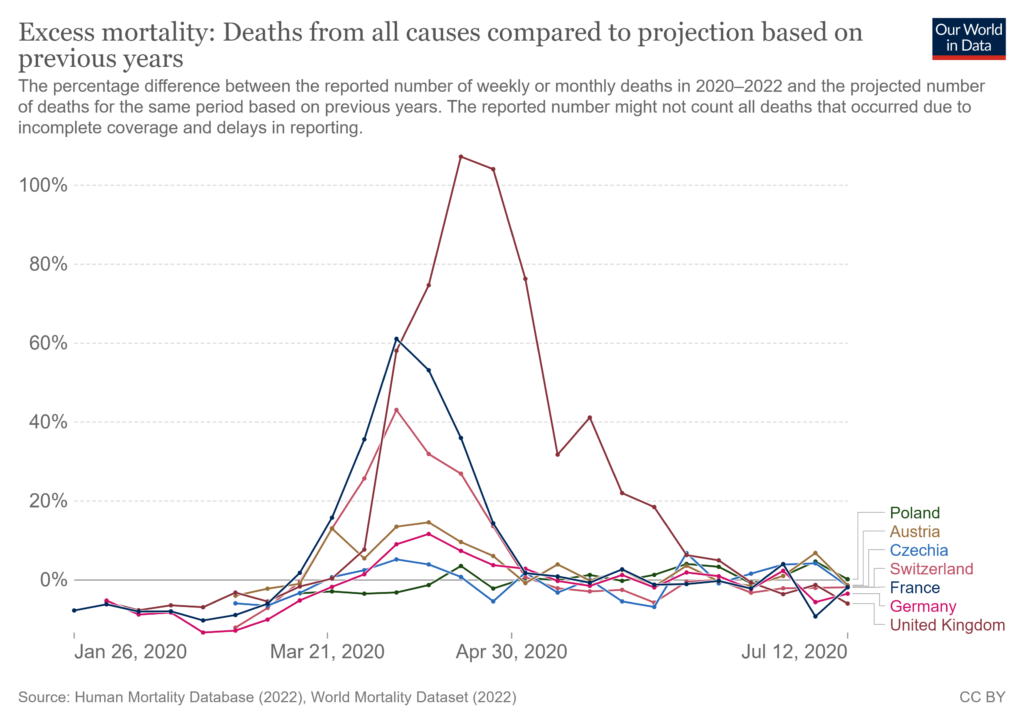
This wasn’t owing to policy responses, as shown by the very different outcomes the following winter.
In line with these inconsistent outcomes, numerous studies have shown that outcomes during the first wave weren’t explained by policy responses. But they also aren’t explained by whether or not the virus was circulating, as it was circulating everywhere.
The evidence we have, then, from multiple studies with strong validation methods – including genetic sequencing of viral RNA – shows that the virus was circulating globally since November 2019 at the latest, with some evidence of its presence as far back as July, though not earlier than that.
The most likely reason there was not an explosive, deadly outbreak prior to March 2020 (or even later in many places) is that the virus was still in competition with other winter viruses so was not dominant or running rampant in hospitals and care homes. The large outbreaks from spring onwards may have been assisted by the emergence of new, more infectious (and possibly more deadly) variants. A winter Covid prevalence of around 2% largely among the low risk could easily go unnoticed among the usual winter diseases without triggering noticeable surges in hospital admissions and deaths.
On this evidence, then, it seems we can definitively rule out both an emergence before July 2019 (too many negatives and just one questionable positive) and after November 2019 (too many positives in a number of countries). The evidence is not currently consistent or robust enough to be able to pin it down more definitively than that.
There should, of course, be much more evidence on early spread. The World Health Organisation in June 2020 called for early spread to be properly investigated. However, very little has been done, and particularly in the United States, the various Government agencies have made no efforts to investigate early spread as part of their general neglect and squashing of all investigations into Covid origins.
Such silence and obfuscation only raises suspicions. And there is no shortage of reasons to be suspicious. The lack of genetic diversity in early samples, the high degree of adaption to humans from the outset, the absence of animal reservoirs and the presence of unique features that make the virus highly infectious among humans suggest that it was not natural but engineered, and thus either leaked from a lab or was released. Who was involved in the research that created the virus and the course of events that led to its getting into the human population is therefore a question of great importance that must continue to be pursued.













To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
Aren’t these the people who have already decided that social distancing and forced face masking will continue for their victims no matter what?
Chances are that most new students will have had much more independence at home, before they were locked away into substandard bedsits and behaviour-policed by private security guards behind grid fences, all in the name of not posing an inacceptable risk to staff.
social distancing and forced face masking – evil – look at Australia
SPEECHLESS Australia OUT OF CONTROL
Alex Belfield – THE VOICE OF REASON – (I don’t agree with everything Alex say he, but I am willing to forgive him)
https://www.youtube.com/watch?v=QIdta7AA2IY
Stand in South Hill Park Bracknell every Sunday from 10am meet fellow anti lockdown freedom lovers, keep yourself sane, make new friends and have a laugh.
(also Wednesdays from 2pm)
Join our Stand in the Park – Bracknell – Telegram Group
http://t.me/astandintheparkbracknell
“Aren’t these the people who have already decided that social distancing and forced face masking will continue for their victims no matter what?”
Exactly. As with every other body that is meant to stand up for those it represents, the suggested solution to the ills caused by coronamadness is not to question the madness or push back against it, but to ask for more help in mitigating the disastrous results.
I wish these students all the best in their coming University life, young people have been treated appallingly by this disgraceful government.
If institutions, at some point over the next year, have to go “on-line” for some reason or other ..these same students should demand refunds.
Saint Boris must remember that HE is responsible for the destruction of these young people’s futures, with his cruel and pointless lockdowns. He must also remember that they are the voters of the future, and they will remember how he totally threw them to the bottom of the pile.
But they may realise that Sneer Smarmer would have locked them up even harder and more cruelly.
I wouldn’t blame them for spoiling their ballot papers, big time.
Boomer here. I’ll have much the same thoughts next time I vote ……
It beggars belief that young people are still taking the decision to burden themselves with huge debt for the costs of university fees. Especially so now that the government has made them a target group for ‘vaccine’ coercion. The pressures they will be faced with is immense and any good parent would guide their child away from the debt slavery towards apprenticeship if at all possible.
So let’s force them to wear masks all the time, exclude them from the Student Union unless they have the jabs, and test them to remind them that they might be biohazards, that’ll definitely help.
So my employers HR came knocking asking for everyone to submit their vaccination status. Me being me, I decided to get mine in first.
I’m posting my email here if anyone wants to reuse it when their time comes. On my lunch break so no idea if I will be still employed this afternoon lol
Thanks for your email regards our return to the office.
Could you please explain to me why an individuals vaccinations status is actually important when by looking at the latest data in the PHE Variants of Concern Technical Briefings (number 21) we can see clearly see that vaccinations have neither prevented infection or reduced transmission of the virus? I have no doubt that you and many others will dispute my assertion but it’s all there to see on page 21 of the document for HM Gov below should anyone care to look.
SARS-CoV-2 variants of concern and variants under investigation (publishing.service.gov.uk)
Whilst I don’t doubt that some individuals within the company may sadly relish the opportunities for discrimination that the sharing of such private health related information presents, I for one find the request for this personal information deeply disturbing.
I appreciate that some vaccinated individuals within the company have strong reservations and concerns about their return to office and even returning to public life in general but I fail to see how an individual’s vaccination status is of any relevance given the above.
Is the company going to provide the unvaccinated and those who refuse to disclose with their own desks in an hermetically sealed room of their own perhaps or maybe just adorn them with yellow stars instead? Outside of such or similar measures I can see little or no use for the company knowing an individual’s private medical information.
Regards
Ask them, while they are requesting confidential medical information if they are requesting the HIV status of other staff members and if so why not?
Love it, not sure you’ll still be employed by the end of the day, do you have an HGV license by any chance?
I’m not sure all teenagers have been cooped up for 18 months, possibly those whose parents are sheep (possibly the same teenagers I now see muzzled) , but I’m happy to say we’ve had loads of them meeting up in groups throughout the whole debacle
Every time I see a group of teenagers showing total disregard for social restrictions, I think: good on you.
Not just the young ‘uns.
Last week I traipsed round my own small seaside town. Unprompted, the keepers of three businesses told me that by and large, this year’s tourists have been uncommunicative if not downright rude.
Fear does that to people.
I suspect they are the ones that normally go to the Algarve for tapas.
This year they have been grumpily tramping around tourist towns in the UK.
Teenagers don’t need help. They need to ‘do gooders’ to get out of their life – permanently.
Let us all hope that people remember all of this when the next election comes around and refuse to vote for the current incumbents of the House of Parliament. We have to change the system or we will continue to get “being locked down for almost two years, to something like as much freedom as you’re ever likely to get.” . Is that the “Freedom” you want? Let us not forget that Starmers Opposition was no Opposition at all. Those bastards took our lives and our freedoms, now we take their positions.
“The source said universities would have to address “socialisation issues” as well as academic study. “
I’m sure that the universities are doing all they can to minimize these socialization issues by enforcing such social activities as mask-wearing, antisocial distancing and enforcing inoculation with drugs of unknown effect.
You couldn’t f.ing make it up.
Another one bites the dust:
Rapper who mocked lockdown protesters dies of heart attack after having the Pfizer Covid-19 injection
https://dailyexpose.co.uk/2021/08/24/rapper-who-mocked-lockdown-protesters-dies-of-heart-attack-after-having-the-pfizer-covid-19-injection/
“…some concern students may overindulge after two school years in which socializing was strictly limited.”
Because students never overindulged before.
This is presumably code language for concern that students might do something other than sitting – fully masked, vaccinated and alone – in cupboards while shivering with fear because of The Terrible Virus[tm].
Students need people who taught them only a very few things. But taught them how to think. Good learning starts with how to separate the shaft from the wheat.
Mr Dalton was receive by a University when aged10.
Don’t comply. Ditch the masks. – FIGHT BACK BETTER – Updated information, resources and links: https://www.LCAHub.org/