I recently watched a documentary, Idiocracy, that described how evolutionary processes might introduce negative effects to the population over the longer term, given selection for certain behaviours and cognitive abilities. One particular theme in the documentary was centred around the characteristics of an isotonic sports drink, Brawndo, and the failure of crops to grow when watered only with this drink. Many appeared to believe that Brawndo would be good for plants because it had what plants crave, electrolytes. This argument appeared to be based on marketing material for the drink, and it was apparent that none of the advocates for the use of Brawndo had any idea of what electrolytes were other than it being something that plants crave. The full nature of the requirements of their crops was completely missing from their considerations.
I mention this only because it reminded me of the cries of ‘antibodies!’ that I’ve heard in reporting on Covid by Government and the media from mid-2020 through to the present. This top-down information campaign resulted in ‘antibodies!’ being discussed in casual conversation up and down the country. It appeared that ‘antibodies!’ were simply what viruses loathe, and that was the end of the discussion. I found this confusing because antibodies are only one part of the immune response to a viral infection and it is important to consider all aspects of the immune response when attempting to protect from infection or treat disease. Indeed, there was plenty of evidence prior to 2020 that coronavirus infections generated only a short term antibody response and that recovery and longer term protection from disease was mediated by T-cells and the innate immune system.
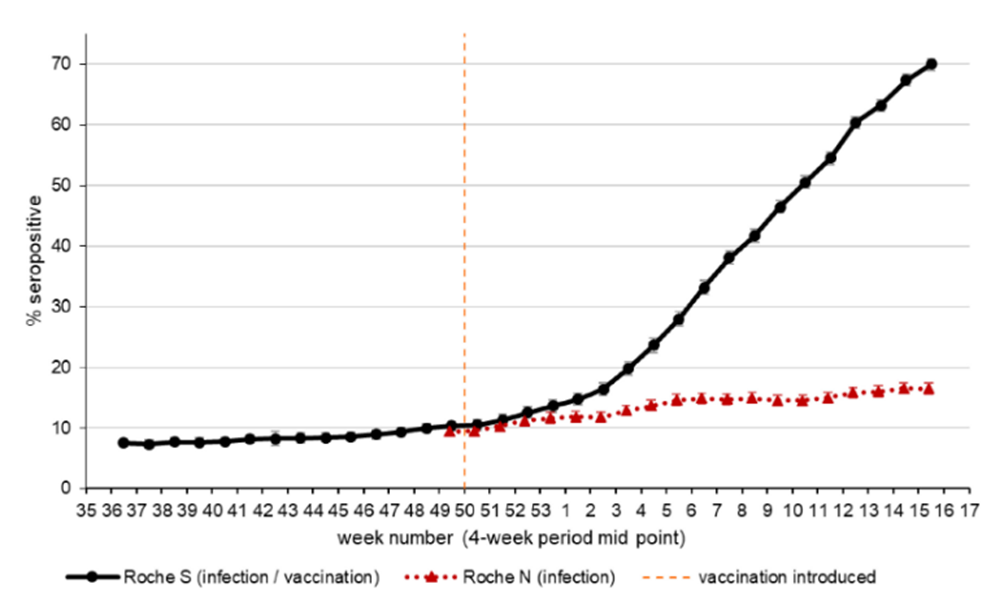
The UKHSA was no exception in its fascination for reporting only antibody levels, devoting four pages (out of 19) to this single aspect of immunity in the first Vaccine Surveillance Report. In those four pages it presented the unsurprising finding that the advent of the vaccines resulted in a dramatic increase in the proportion of the population with antibodies to the spike protein. This was to be expected as the vaccines result in only the spike (or S-protein) being presented to the immune system. Antibodies to the nucleocapsid (or N-protein) remained unaffected by the 2021 vaccination drive and continued their trend seen during pre-vaccine 2020, with a slowly increasing incidence of such antibodies reflecting the proportion of the population that had been infected with Covid. This effect was presented to the public in that first report in a graph of those positive for antibodies to the N-protein versus S-protein found in surveillance of donated blood.
The interesting thing about the details of population antibody levels (serology) in the Vaccine Surveillance Report is that it only mentioned the presence of IgG antibodies in the blood and there was no reporting of the at-least-as-important IgA antibodies (present in the respiratory tract and gut). That is, not only did the report ignore non-antibody immune mechanisms but it also limited itself to a subset of the antibody response that is arguably of less importance for respiratory infections. In defence of the UKHSA, it could have simply meant that the strength of the immune response in general is often correlated with the levels of IgG antibodies found in blood serum, and thus that its reporting of the serology was generally useful. If it had meant this it would have helped if it had told us this at the time.
Regardless, despite very high antibody levels in the population to the spike protein, and relatively high levels to the N-protein, Covid waves keep on coming. This suggests that the original faith in ‘herd immunity’ through the generation of IgG antibodies was desperately misplaced. Not that anyone is telling us this – as far as our authorities are concerned there have been no mistakes, other than the facile ‘we didn’t do enough of whatever we did’. Of course, this is what politicians always say – that everything would have been fine if they’d have been allowed more freedom to enact their favourite policies.
What is so odd is that the vaccines targeted the spike protein in the first place. Sure, this approach results in the generation of antibodies capable of neutralising Covid’s spike protein. But this doesn’t appear to be the mechanism adopted by the body following natural infection. Studies suggest that the cellular immune response is important for offering long term protection from infection with coronaviruses (including Covid), and that this cellular immune response targets the N-protein not the spike protein. As Dr. John Campbell says in an informative video recently discussing this paper:
In that case you might think it would be better to make vaccines based on nucleocapsid proteins rather than spike proteins, and if you thought that I’d tend to agree with you, and so would these researchers…
It’s not the spike protein bit that’s working best, yet the vaccines are based on the spike protein – I really want to know why the drug companies chose the spike protein to make all the vaccines against [Covid], apart from the Chinese [vaccine].
As an aside, I note that it was the Chinese authorities that sent the RNA code for the spike protein to the West, which was then used to ultra-rapidly develop the vaccines that we have today.
It is also worthy of note that although the early vaccine trials were based on there being an actual reduction in symptomatic infections in the vaccinated (albeit only over the short term), since then the pharmacological companies have negotiated with medical regulatory bodies that they only have to show serological evidence that their updated vaccines have induced an antibody response (which will, of course, be limited only to antibodies to the spike protein). Indeed, the recent bivalent boosters were only required to induce an anti-spike antibody response in (six) mice before they were released to the public. I suppose we’ll find out in time if they actually work.
One potential problem related to antibody-based immunity is the role of anti-idiotype antibodies, that is, the generation of antibodies that attack the body instead of the pathogen. While much has been made of the role of ‘neutralising antibodies’ in the generation of protective immunity, this is only one way in which antibodies function. Neutralising antibodies work by the antibody attaching itself to a important part of the pathogen, impairing its ability to function – in the case of Covid these neutralising antibodies attach themselves to the spike protein and stop the spike from binding to the ACE2 receptors present on many human cells and thus stop the virus from entering the cell and replicating. However, another role for antibodies is to signal to other immune mechanisms that a foreign body is present. One part of the antibody binds to its target and, once bound, another part of the antibody indicates to the immune system that whatever it is that it is attached to needs to be dealt with (using a variety of mechanisms). However, it has been known for decades that an unavoidable part of the immune system is the generation of at least some antibodies that mimic the original antigens found on the pathogen. In the case of Covid, as the target antigen is the spike protein the ‘mimic’ antibodies will themselves resemble (parts of) the spike protein – and as the spike protein itself is capable of attaching to ACE2 receptors on cells it is likely that there will be at least some antibodies generated that are also capable of attaching to ACE2 receptors on cells. Unfortunately, the ‘other end’ of the antibody will at this point signal that ‘the thing that it is attached to is foreign’ and this will lead the cell being targeted by the immune system, resulting in to the usual immune response to cells that are identified as ‘infected’ for ‘foreign’ by the immune system, including inflammation and the destruction of ‘infected/foreign’ cells. Normally this damaging autoimmune response is muted and doesn’t cause a significant impact (except in relatively rare cases where the immune response is abnormal). However, there is evidence that the very high antibody levels developed after severe Covid have induced relatively high levels of these unhelpful autoantibodies, leading to a pathogenic response. These autoantibodies have also been suggested as at least contributing to the mysterious ‘long Covid’. Note that the Covid vaccines were designed to induce rather high antibody responses by the immune system similar to, or even exceeding, those normally found only after severe Covid. Indeed, these very high antibody levels have been reported as being one of the triumphs of the vaccines (applying a simplistic ‘more is better’ approach to the immune system). It remains to be seen if autoantibody problems also occur after vaccination, leading to cardiac, neurological or other effects. Indeed, if there is ‘original antigenic sin’ occurring then it is possible that each subsequent Covid infection would also produce these autoantibodies in meaningful numbers, leading to longer term post-vaccine complications (exhibiting itself as a higher risk of targeted autoimmune inflammation in each post-infection period, even if the infection itself had presented with mild symptoms).
Another potential problem related to the highly immunogenetic nature of the Covid vaccines is that of ‘high zone tolerance’. Our immune system is designed to attack ‘things that shouldn’t be there’ and most definitely not ‘things that should be there’ (i.e., the self). However, repeated exposures to ‘things that shouldn’t be there’ at relatively high levels trains the immune system to treat those things as part of the self and suppresses the normal immune response. This mechanism is important not just to avoid our immune system from attacking ourselves, but also to mute the immune response to ‘foreign stuff’ that we encounter every day, such as food (in our gut, with ‘digested bits’ eventually reaching our bloodstream) or pollen (in our respiratory tract). If we didn’t have this tolerance mechanism then we’d have a significant immune response every time we ate a meal or went for a walk. Indeed, it is of fundamental importance that we’re tolerant to the symbiotic bacteria in our gut that we use as part of our digestive process. It is very possible that the significant levels of spike protein produced after vaccination, coupled with frequent boosters, has resulted in a level of immune tolerance being generated in some individuals. If this is the case we might expect to see higher infection rates (lower immune response on infection) and lower hospitalisation rates with severe Covid (as this is due to a hyperactive immune response), but higher rates of problems associated with the viral infection itself as the immune suppression would lead to higher viral loads (this is likely to include pathologies associated with the spike protein itself, such as has been proposed for myocarditis).
The Vaccine Surveillance Report for late October 2021 contained a rather worrying statement, presented as a throwaway sentence deep in the text:
Recent observations from U.K. Health Security Agency (UKHSA) surveillance data [show] that N antibody levels appear to be lower in individuals who acquire infection following two doses of vaccination.
This finding was important because, while there are several potential reasons for it to occur, one important potential mechanism is original antigenic sin (OAS, also known by the more prosaic term ‘immunological imprinting’). OAS occurs when the first exposure to a particular pathogen primes the immune system, and all subsequent exposures result in a response biased as though it was the original infection even if in the subsequent exposures the pathogen has changed slightly (possibly via evolution targeting immune escape) and requires the immune system to have recognised this change for an optimal immune response. In the case of the vaccines, the first immune exposure is only to the spike protein (produced by the vaccines) and thus if OAS occurs then the immune response following infection will be biased towards strengthening the level of antibodies to the vaccine spike protein (i.e., those present following vaccination) rather than the N-protein of the virus (which will be absent following vaccination).
This innocent sounding sentence in the report wasn’t proof of OAS, but it was suggestive of a potential problem. Yet there appeared to be no follow up to this finding and the sentence merely came back in every week’s Vaccine Surveillance Report, pointing out that something that sounded worrying to the right eyes was simply being ignored.
Fortunately, N-protein antibody levels appear to have risen significantly since Omicron variant came onto the scene in late 2021.
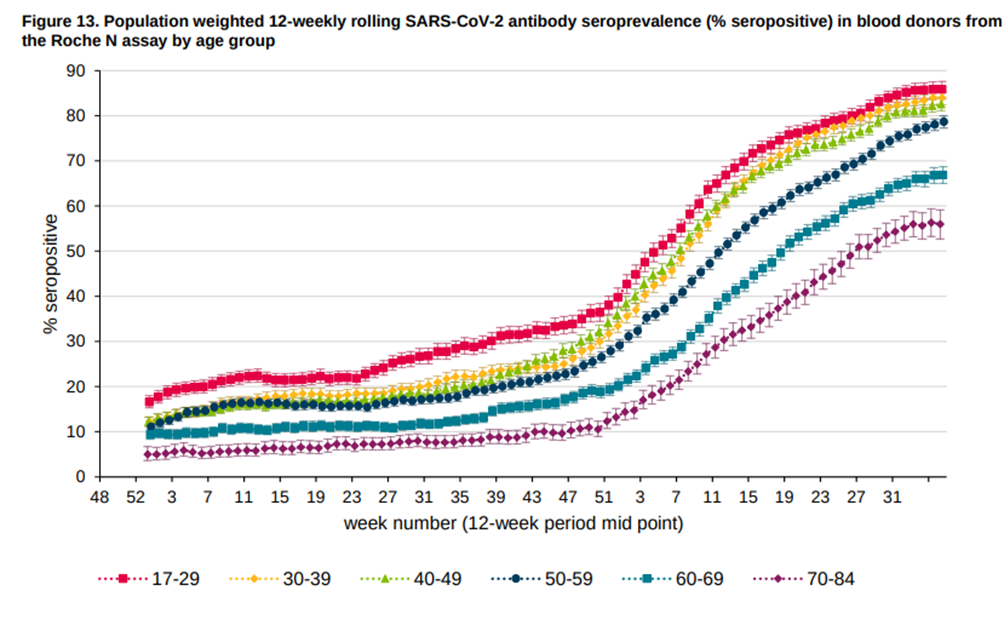
The rapid rise in N-protein antibodies across the population at the start of 2021 might simply reflect the relatively high infection rates seen with the Omicron variants compared with prior variants, although it might also be important that Omicron is rather dissimilar to prior variants and this might reduce the impact of any OAS that is present.
The reason for the lower levels of N-protein antibodies found in older individuals despite huge infection levels in the population isn’t clear. This might reflect some risk of OAS in those with older immune systems, but could also reflect some continuing restraint in terms of social behaviour or reflect the fact that the immune function in older individuals is less liable to produce antibodies after natural infection (immunosenescence – note that this would also make the immune system in older individuals less likely to produce antibodies after vaccination). It would be useful to know more about this effect, because a full understanding of the potential for OAS is crucial to inform our public health response towards the protection of vulnerable individuals from Covid.
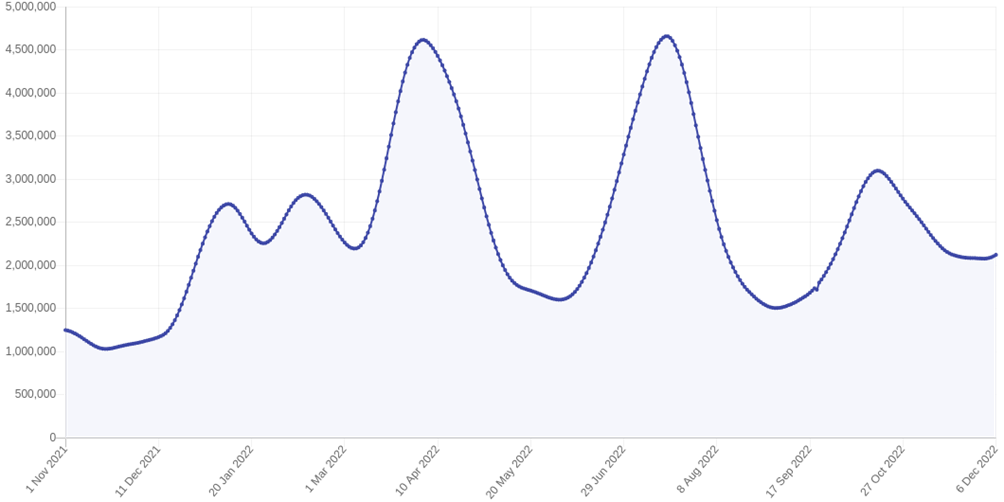
Whether or not OAS is occurring, I note that the high levels of Covid antibodies in the population doesn’t seem to have prevented the up-tick in new infections that we’re currently seeing in the U.K., from the rather high levels (over 2 million concurrent infections) that we’ve had since the end of the previous Covid wave in November. If it is a new wave then I imagine that we’ll see it peak in mid January, with sufficient cases in about 10-14 days’ time for there to be calls to ‘cancel Christmas’ from the usual suspects. Hopefully few will heed this ‘advice’.
I’m sure that the above will result in a few murmurs of ‘variants’. As I’ve mentioned previously, it is important to note that mutations in the N-protein are somewhat less likely than in the spike protein. While it is the case that each of the nucleotides in the RNA is equally likely to mutate, some parts of the RNA are more likely to result in a viable virus than others. The spike protein is known to be particularly ‘mutable’ (mutations are more likely to result in a viable virus) whereas the N-protein is relatively conserved (mutations are less likely to result in a viable virus). Thus it is likely that immune mechanisms targeting the N-protein will continue to work to control infection to some extent even in the face of viral evolution, compared with the immune response to the spike protein, which is more liable to be evaded by the virus. Which brings us back to the question as to why the highly mutable spike protein was selected as the target for the gene based vaccines in the first place.
Next time I’ll discuss a part of the Vaccine Surveillance Report that should be of great interest to many people – the section on the impact of the vaccines on pregnancy.
Amanuensis is an ex-academic and senior Government scientist. He blogs at Bartram’s Folly – subscribe here.












To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
Referring to para 2, a while back it seemed to me that the obsession with antibodies, especially re the product on offer, looked like an advertising tactic, not proper science. More like deliberate avoidance of comprehensive education on the topic.
About a year ago, via this site (or maybe it’s predecessor), I came across organisations that can (at a fee) perform T-cell assessments related to SARS-Cov-2, which I became interested in on the basis that it was well over a year since I had some kind of respiratory attack (traditionally called common colds) around the time that C-19 emerged. Not advertising, but the firm used was based in Abingdon. The result of that was inconclusive, so it was probably caused by one of the hundreds of other viruses. I had a go at this, because it was obvious that it would be pretty unlikely for any relevant antibodies to be on board after 12 months or more.
Looking on the bright side, it has turned out to be educational about the mechanics of our immune system. On the other side, I’d better not say too much!
Incidentally, I endorse John Campbell’s channel; useful and reassuring to a large extent.
Very interesting (as always).
I’m afraid there has been so much lying that my default assumption now is that any covid related output from “official” bodies is not based on incorrect assumptions or innocent mistakes but on expediency, greed, lust for power, arse-covering. So rather than that concluding that “vaccines” were “effective” because antibodies, the conversation was more like “what plausible story can we cook up that sounds like these vaccines are effective”.
Yes indeed. Why choose the spike protein for the covid vaccine :-
https://hillmd.substack.com/p/spike-proteins-choice-by-competing
Yeadon may be being a little over dramatic by describing the vax as bio weapon, but for a more nuanced view :-
https://dpbh.nv.gov/uploadedFiles/dpbhnvgov/content/Boards/BOH/Meetings/2021/SENEFF~1.PDF
I’ve yet to see any scientific rebuttal of the dangers raised in the paper (and the earlier one with Antony M. Kyriakopoulos).
The immune system is incredibly complex and poorly understood, and even worse often misunderstood, especially by the genetic engineers behind mRNA whose only brief nod to the immune system, seems to have been how to avoid their product being destroyed by it.
What could possibly go wrong.
I don’t think Yeadon is being over dramatic at all. These products are referred to as ”countermeasures”, and Katherine Watt elaborates further;
“NUTSHELL: US Government since 1969 has incrementally transferred/hidden the joint DOD+HHS Chemical and Biological Warfare Program (50 USC 32) in the Public Health Service Act (42 USC 201) and Food Drug and Cosmetics Act (21 USC 9), such that federally-funded, federally-directed public health programs and products are actually bioterrorism programs and biological and chemical weapon attacks.
21 USC 360bbb-3, Authorization for medical products for use in emergencies, is one of the key pseudo-laws enabling the bioweapon attacks under the Covid-19 national emergency pretext.
We now know that there is no stopping condition, because use of the products “shall not be considered to constitute a clinical investigation.” If there is no regulated investigation, then there is no stopping role for a regulatory agency to perform, and the products are not medicinal drugs or devices: they are weapons.”
https://bailiwicknews.substack.com/p/stopping-conditions
“I recently watched a documentary, Idiocracy” – thanks for that, this really did make me laugh out loud. I guess this is the film Hancock should have watched rather than the fictional disaster movie Contagion 😉
Yes, a very good question as to why they chose the spike protein for the vaxxes, particularly as there were doctors warning in December 2020/January 2021 that the spike protein was already being seen as the pathogenic part of the virus. I remember reading quite a few items on Children’s Health Defense about that. I also remember reading about a study that had shown the spike protein had caused damage in different organs, without any trace of the virus being found. They can’t claim there was no knowledge, when even I had heard that the spike protein was in itself harmful prior to the vaxx rollout. It could be as simple as Fauci et al. long knowing what the problem was, what part of the virus they felt needed to be eliminated and had started brewing their poison some time around October/November 2019.
Another very good question is why “scientists” across the world decided to fixate on antibodies. It’s one thing saying that the health authorities in the US or the UK decided on a certain course of action and that was that, but why did every other country on earth decide to follow suit? The real pandemic was the “stupid” bug that invaded most people’s brains.
Looking forward to your article on pregnancy and the vaxxes.
I’ve learnt a lot these past couple of years not only about our fake democracy or rNHS not being the envy of the world, or the government who’s job it is to protect this country and its inhabitants but does not, but how wonderful our own bodies are, our immune systems are nothing short of miraculous, provided we take care of it and not bombard it with toxic chemicals. I question everything now! We only have one life and I am not entrusting it to anyone particularly the government or its health agencies.
Idiocracy is the name of a film about the human race regressing to stupidity! Very apt!
‘Regressing’ – I think we are beyond present continuous and have arrived at past perfect.
We have had a pandemic of stupid which started in 1945 when the Nation went nuts and overdosed on the Cradle-to-the-Grave, lots of free stuff elixir doled out by Labour.
Stupid is now endemic, taught in schools, and there is no cure. Only a minority have immunity.
Instructional, well balanced and argued. Thanks.
At the very least, the OAS theory is much too simplistic: Influenza (and common colds) are recurring infections most people survive without even getting seriously sick. This implies that people becoming reinfected with it will have an immune system supposedly imprinted by the previous version of it. Nevertheless, the immune system must be capable of updating itself quickly in the overwhelming majority of cases.
Forgive me, Amanuensis, until I reached “…..and this will lead the cell being targeted by the immune system, resulting in to the usual immune response to cells …….” I was following your explanation beautifully, but then lost the thread. Sorry to be a pain, but there appears to be a typo in the extract above. Could you please amend. Many thanks, and for your excellent articles generally.
“The rapid rise in N-protein antibodies across the population at the start of 2021 might simply reflect the relatively high infection rates seen with the Omicron variants compared with prior variants, although it might also be important that Omicron is rather dissimilar to prior variants and this might reduce the impact of any OAS that is present.”
I think you mean 2022, not 2021.