
What is the evidence that SARS-CoV-2 originated earlier than December 2019 in Wuhan, and what are the implications of that for our understanding of the pandemic?
The purpose of this article is to provoke discussion about the origins of SARS-CoV-2 by collating a range of evidence from countries around the world – the U.K., France, Ireland, Italy, Spain, the U.S., Brazil and China.
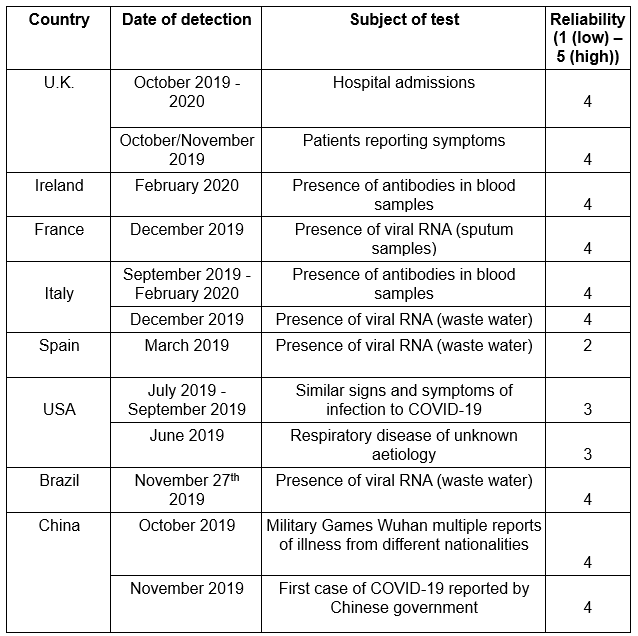
The following table summarises at a glance the information presented in this article. (N.B.: ‘Reliability’ in the right-hand column is an assessment of how likely the evidence is, in this author’s view, to show the presence of SARS-CoV-2.)
The ‘official’ timeline for SARS-CoV-2 (COVID-19) is that physicians in a hospital in Wuhan, China, reported a number of patients with a viral pneumonia of unknown aetiology in December 2019. In January 2020, it was reported that the pathogen was a coronavirus and had been isolated. The coronavirus was designated SARS-CoV-2 and the associated disease COVID-19. After the World Health Organisation declared a pandemic on March 11th 2020, testing for the virus by Reverse Transcriptase Polymerised Chain Reaction (RT-PCR or PCR) was ratcheted up around the world, with countries closing their borders and restricting the activities of their citizens.
Early on, anecdotal accounts started to surface suggesting the virus was actually in circulation some weeks or months earlier than the official timeline. The present article pulls together a number of these anecdotal accounts along with more scientific observations in the form of antigen and antibody testing that appear to corroborate the anecdotal accounts.
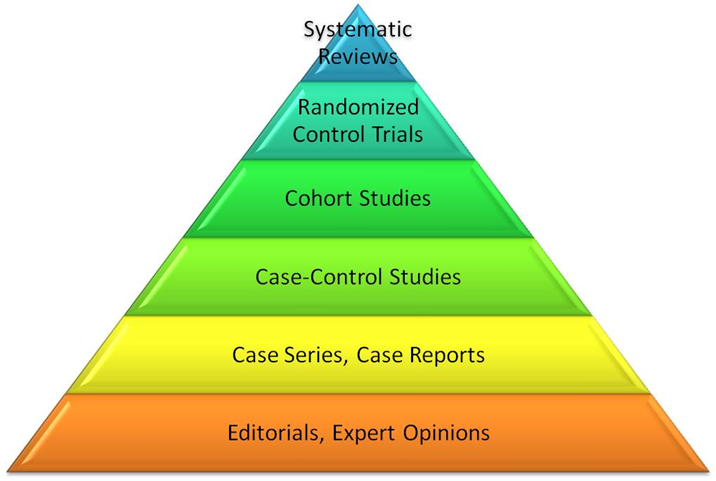
Anecdotal evidence is treated as low grade evidence at level five or six in the evidence pyramid after Sackett (see below); however, that does not mean it is worthless or should be lightly dismissed without investigation to see if it is corroborated by scientific observation.
United Kingdom
In the United Kingdom, I am aware of many people who have reported presenting to an urgent care centre with persistent cough and mild fever in October and November 2019. Some patients reported that the cough had lasted several weeks, up to six in one case. The fever was typically around 37.8-38.0°C. One patient reported a change in taste for seven days after having a cough for the previous five weeks, which resolved itself at the end of the first week in November. General practitioners known to the author working in the same urgent care centre reported parallel experiences from patients in their own practices. Other people from around the country reported similar symptoms around the same time on different websites.
Further evidence from this period comes in the form of hospital admissions for respiratory conditions obtained through freedom of information requests. The data come from the coding added to a patient’s notes after discharge using the International Classification of Disease (ICD; issue 10 was the latest edition at the time).
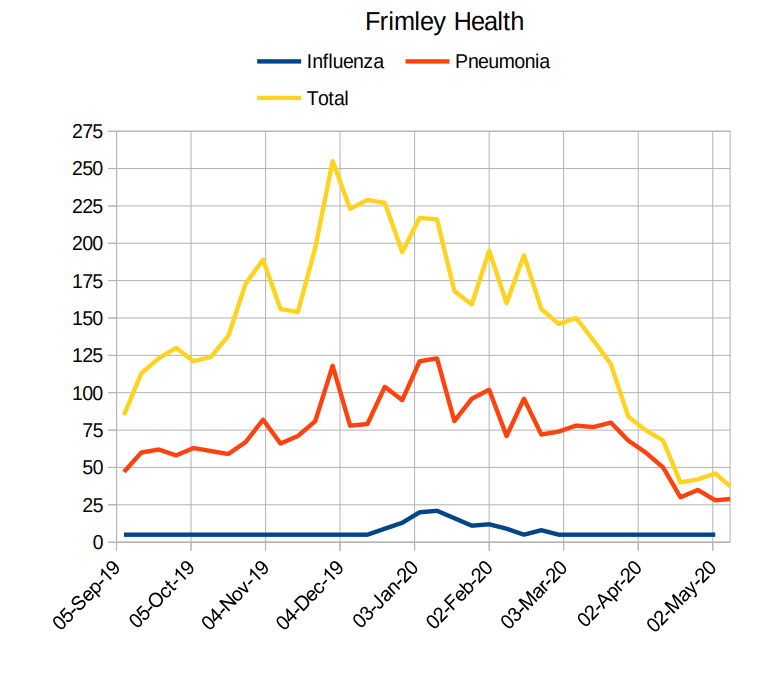
A graphical representation of the data from one trust, Frimley Health NHS Trust in Surrey, is shown below. The orange line represents all the patients admitted and diagnosed with any respiratory condition, the blue line is patients diagnosed with pneumonia, and the yellow line line is the number of patients with a positive SARS-CoV-2 test used as a proxy for COVID-19. When the medics in Wuhan first reported the outbreak they stated that there was pneumonia caused by an as yet unknown pathogen. The Frimley Health graph shows a steady increase in pneumonia diagnoses over the last quarter of 2019, before falling off in early 2020.
If all or most of the SARS-CoV-2 patients had COVID-19, a respiratory disease, then the orange and blue lines should track the yellow line and should not fall substantially below it. This suggests that the number of COVID-19 patients may be predominantly due to positive tests and not diagnosed disease (this assumes those assigning the codes did not routinely omit other ICD classifications such as pneumonia in COVID-19 cases).

This next graph, also from Frimley Health, shows the number of patients coded with respiratory illness as before (yellow), the number of patients with a diagnosis of pneumonia (orange), and the number of patients with a diagnosis of influenza (blue). As may be clearly seen, there was no large winter peak in this trust for influenza in 2020, with cases trending well below the pneumonia and respiratory disease lines. Whether this is significant is unknown – it may again be a classification issue, and without data from earlier years against which to compare it it’s hard to know whether the discrepancy between the disease categories is standard or anomalous.
France
Deslandes and colleagues in 2020 reported on a patient hospitalised in December 2019 in a north Paris Intensive Therapy Unit who was coughing up blood with no diagnosis of cause. The researchers reviewed retrospectively the records of other patients admitted with influenza-like illnesses to ITU between December 2nd 2019 and January 16th 2020. Since every respiratory sample collected in the hospital is frozen and stored for four years, the researchers conducted RT-PCR tests on samples which originated from patients with influenza-like symptoms (temperature above 38.5°C, cough, sore throat, runny nose or muscle pain) or a ground glass appearance on chest radiography. Initially, 124 samples were available; of these, 44 were excluded as they had tested positive for other viruses. Of the remaining 80 samples, 66 were excluded for atypical COVID-19 medical records (though why the researchers didn’t test all of them just in case is not really clear).
Finally, nine samples from December 2019 and five from January 2020 were tested, 14 in all. Of these, one sample from December 2019 was positive for SARS-CoV-2 whilst the remaining 13 were negative.
This patient predates the first official case of COVID-19 in France by approximately four weeks and had had no recent overseas travel or a link with China.
Ireland
Butler and colleagues in 2022 tested 8,509 samples taken from blood donors in the Republic of Ireland between February and September 2020, screening them for SARS-CoV-2 antibodies using multiple testing devices. The first samples that tested positive were those collected on February 17th, some 14 days before the first official notification. Significantly higher antibody presence was identified in Dublin and in donors under 40 years of age. As antibodies last for up to 90 days, the virus could have been circulating as early as the end of November 2019.
Italy
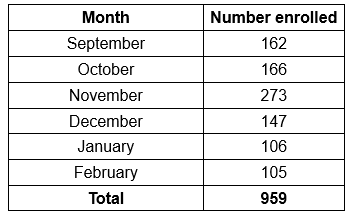
Apolone and colleagues in 2020 reported that between September 2019 and March 2020 in Italy, 959 patients were enrolled on a prospective lung screening trial that involved the taking of blood samples, with the monthly enrolment as shown below.
The first cases of COVID-19 in Italy were identified in January 2020. However, the rapid spread and the number of seriously ill patients suggested to the researchers that the virus may have been circulating several months previously. Samples from the 959 participants were tested for the presence of two types of SARS-CoV-2 antibodies, IgG and IgM. Of the 959 samples, 16 were found to have IgG and 97 were found to have IgM (some had both). The data pertinent to this discussion are presented below.
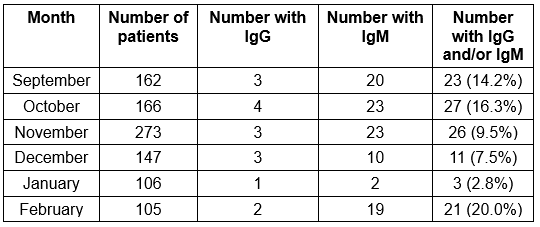
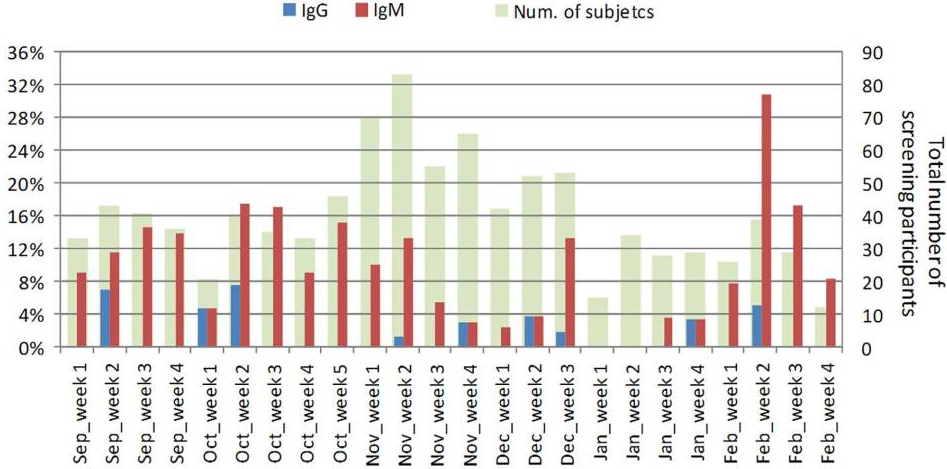
When the weekly data are examined, the researchers show that there are two distinct peaks, one in the second and third weeks of October (18% IgM positive) with the second occurring in the second week in February (30% IgM positive). Between these two dates the number of patients with IgG or IgM antibodies drops significantly.
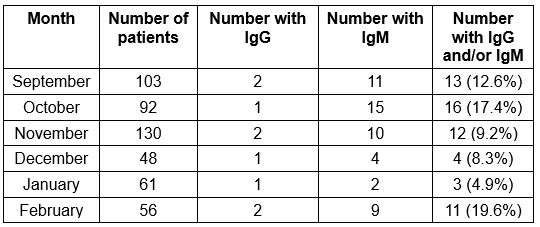
A similar pattern is seen if the Lombardy region is examined in isolation, as shown below. Lombardy is significant as this is the region most affected by the pandemic, according to the Italian Government.
IgM antibodies are significant in that they appear early in the course of infection, reappearing to a lesser extent on further exposure to a pathogen. If IgM antibodies are present in a patient’s serum then he or she has had a recent infection.
IgG antibodies appear after the maturation of the antibody response when B cells switch from creating IgM; thus the presence of IgG demonstrates a later stage in the immune response. Unlike IgM, the presence of IgG is more indicative of a person’s immune status to a given pathogen.
Concern about the possibility of false positive results needs to be addressed. These tests were undertaken using a technique called microneutralisation assay, which according to Manenti and colleagues is the most reliable in terms of the obtained results. However, while the study does not discuss its limitations, other studies have mentioned possible cross-reactivity of antibodies as a limitation. It would also have been reassuring to have seen results for earlier samples, both to see when the antibodies first appeared and as a control.
The authors conclude that SARS-CoV-2 was circulating amongst individuals (asymptomatic at the time of their blood sample, though not necessarily at the time of infection) several months before the first patients were identified in Italy or Wuhan. The first official cases identified in Italy were two Chinese tourists on January 19th 2020.
La Rosa and colleagues in 2021 reported on the testing of waste water samples from five different sites in northern Italy between October 2019 and February 2020, using 24 samples obtained from the same sites between September 2018 and June 2019 as blank controls. Fifteen confirmed positive samples were identified, with the earliest dating back to December 18th 2019 in Milan and Turin and January 29th 2020 in Bologna. The absence of positive samples prior to December is curious given the antibody results above.
Spain
Chavarria-Miró and colleagues in 2020 reported on the testing of waste water in Spain for the presence of SARS-CoV-2. Initially this was for the period April to May 2020, when the virus was known to be active in the country, in an attempt to understand the progression of the virus in Barcelona. These samples were 24-hour aggregations of samples taken from each of two sites that were analysed weekly. Similar assays were undertaken on frozen samples for the first quarter of 2018, the first and last quarters of 2019 and the first quarter of 2020.
The first case of COVID-19 reported in Spain was February 25th 2020. However, analysis of the samples from the first quarter of 2020 showed the presence of SARS-CoV-2 in the sample from January 15th. Of the multiple samples covering 2018 to 2019, only one had a positive result, for March 12th 2019. This could be an anomaly due to cross contamination or it could be genuine.
United States
In 2019 there was an outbreak of severe lung disease in the United Sates that was attributed to the use of e-cigarettes and vaping and is termed EVALI by the CDC. The first cases were reported in July 2019 in Wisconsin and Illinois, spreading to all 50 states and peaking in September 2019. The rates of EVALI reported for the months June to August 2019 in Illinois were twice those for the same months in 2018 (see papers by Layden and Segreto). Of significance are the parallels between EVALI and COVID-19, with a diagnosis of EVALI being one of exclusion (i.e., by process of elimination).
Pitlick and colleagues in 2021 reported on a 34 year-old male who presented with shortness of breath, cough, headaches and other symptoms. A chest X-ray showed abnormalities and he was presumed to have a pneumonia. He was treated with antibiotics but did not improve; in fact, he worsened, requiring supplemental oxygen, and a chest CT scan showed a ground glass appearance. He was treated with further antibiotics without any improvement. He was then treated for EVALI with steroids and he improved, being discharge five days after admission. However, multiple tests for SARS-CoV-2 came back negative. Could this have been COVID-19 instead of EVALI? COVID-19 is a viral infection and hence treatment with antibiotics would be superfluous, whereas steroid treatment would be beneficial. The negative PCR tests count against the possibility, however.
A news report from July 2019 indicates there was a respiratory virus circulating in a retirement community in Fairfax County, Virginia in June 2019, the symptoms of which were cough and fever with pneumonia developing. This was around the same time that the military lab at Fort Detrick was closed after failing a safety inspection; I note that Fort Detrick, MD, is approximately 50km from Fairfax, VA.
Basavaraju and colleagues in 2020 reported on reactive antibodies to SARS-CoV-2 being present in U.S. blood donations in December 2019 and January 2020, when the first reported infection in the USA was reported on January 19th 2020. SARS-CoV-2 reactive antibodies were found in the states of California, Oregon and Washington in samples from mid-December 2019. Antibodies develop after seven to 10 days and may last up to 90 days, thus they could have developed as early as mid-September or as late as the beginning of December 2019. The authors caution that the samples included in the report may not be a true representation of all blood donors and hence their observations should not be taken as a generalisation across all donors in the same time period. Thus, it would be inappropriate to infer the number of infections at a state or national level. Further studies are required to corroborate the findings which are suggestive of the presence of SARS-CoV-2 in the U.S. earlier than officially admitted to.
Brazil
The first official case in Brazil was identified on February 25th 2020. Although SARS-CoV-2 is a respiratory virus, it is known to infect the gut where there are ACE2 receptors; up to 100 million SARS-CoV-2 genome copies are found in each gram of faeces.
Fongaro and colleagues in 2021 tested six samples of raw sewage from Santa Catarina, Brazil. The samples were taken on October 30th 2019, November 6th 2019, November 27th 2019, December 11th 2019, February 20th 2020 and March 4th 2020. SARS-CoV-2 RNA was detected using commercially available RT-qPCR equipment. Negative control tests were performed to ensure sensitivity and specificity. Finally, tests were undertaken in an independent laboratory in a blinded environment using different analysis machinery. These two tests produced similar results, indicating that the samples from October 30th and November 6th were negative, whilst the subsequent samples from November 27th onwards were all positive. This strongly implies that SARS-CoV-2 was in circulation in Brazil some 90 days earlier than reported.
China
In October 2019, 9,000 athletes representing the military from 100 countries attended the Military Games in Wuhan. Several French participants returned from these games with a mystery illness, with one non-participant being admitted to hospital with pneumonia in December 2019. A sample taken from this patient on December 27th tested positive for SARS-CoV-2. Participants from Germany, Italy and Luxembourg all state that they had COVID-19, although the Swedish contingent stated that they tested negative despite being unwell (though which kind of test they are referring to and when they were done is not clear from the press report).
Pekar and colleagues suggest there were cases of COVID-19 as early as November 17th 2019 as recorded by the Chinese Government, although most of the first cluster was associated with a seafood wholesale market in December 2019. Using genome data collected from early cases of COVID-19 and analysed with molecular clock techniques, the time of the most common ancestor to the sequenced genomes is estimated to be late November 2019 (with uncertainty estimates pushing this back possibly to mid-October).
Absent signals
What is missing over this period are reports of excess deaths, which became apparent in the U.K. and some other countries in March and April 2020, when there were significant numbers of admissions to hospitals, usually of older people. Bearing in mind the median age of death with COVID-19 in spring 2020 was 83, one possible explanation for the lack of excess deaths is that the people infected in the last quarter of 2019 were younger and hence less likely to experience severe symptoms or to die. How a circulating infectious respiratory virus would not have reached the older population during the winter is unclear, however.
Conclusion
Although not conclusive proof that SARS-CoV-2 was circulating several months before it was officially recognised, the evidence presented here does give food for thought. It suggests the possibility, for example, that Wuhan was not the original source of the virus but only the place where everything came together. Could it have originated in the USA, bearing in mind that Fort Detrick was closed due to safety concerns in July 2019, or in Europe, with Wuhan simply being where it was first spotted? The apparent artificial origin in ‘gain-of-function’ research needs to be accounted for, of course.
Could it have been the military games that brought the virus into Wuhan in October 2019, as the Chinese Government has suggested? Or could the military games have enhanced its spread from Wuhan across the world?
What does need to be explained is the apparent synchronicity of large numbers of infections in different parts of the world, with significant outbreaks (with large numbers of deaths) occurring within weeks of each other in Italy, Spain, the U.K., France, Sweden and New York, among other places.
It may be significant or it may not be that Frimley Health NHS trust above includes the garrison town of Aldershot in its catchment area.
Some have proposed that the pandemic was a deliberate ploy on the part of the USA or others to besmirch China through a false flag operation. Others have proposed a double bluff by China – noting the financial benefits from, for example, the manufacture of masks, PPE etc. The country’s crippling Zero Covid strategy in recent months would suggest this is an unlikely explanation, however. The standard explanation is that it was something unintended, of course, whether a lab leak or a natural event.
In any case, what does need to be answered is how to prevent the same situation arising in the future, where the actions of one country in imposing draconian public health measures can paralyse most of the world with fear. The WHO carries much of the blame here for becoming an early cheerleader of the Wuhan lockdowns.
What needs to be emphasised is that the information presented here does not mean that the wave of infections reported in March 2020 was non-existent. Many people were clearly experiencing symptoms and reporting them, and they were later found to have antibodies to SARS-CoV-2. Neither should it be presumed that many of the excess deaths reported for March and April 2020 were not due to COVID-19, although data suggest there were a significant number of excess deaths from that time that were not Covid related and are more likely lockdown and policy related.
John Collis is a recently retired nurse practitioner.












To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
I agree with your conclusions in the main. However, in general there appears to be a built-in assumption that there was a unique point of origin. Does nature work like that, or could there have been several of them around the world, in a similar timeframe?
The psychological background to the whole affair might be worth exploring a bit more. E.g. the occurrence of something might be strongly linked to the awareness of it, whereas at other times it might not have been identified. After all, we are discussing respiratory infections that are, in reality, caused by several other coronaviruses, and loads more rhinoviruses, not to mention ‘flu as well.
I’ve actually wondered what would have happened if China officials had NOT reported a new coronavirus to the W.H.O. on December 31, 2019. Is it possible the entire pandemic could have been “missed” and nothing that has happened in the last 27 months would have happened?
One might quickly respond, “no way” because so many deaths occurred beginning in late March 2020 – after all the big ‘hype” had commenced. Still, it’s perhaps possible that most of these deaths were actually caused by faulty medical protocols and/or that the virus had big outbreaks because of people running to hospitals, where the virus no doubt spread, and then got pushed into the nursing homes where about half of the early deaths occurred. It’s also very possible that many cases identified as “Covid” were (and are) not Covid.
The Brownstone Institute recently published an intriguing article, noting that the virus probably was already wide-spread in China either by September 2019 or October 2019 (when the World Military Games took place in Wuhan). Satellite photos shows parking lots at Chinese hospitals that were overflowing and the Chinese military apparently “took over” operation of the Wuhan lab in September 2019. I recently watched a video interview with Robert Kennedy, Jr., who now says it’s “obvious’ the virus was spreading by September or October 2019.
All of this might suggest that the virus was “spreading” widely in either September or October 2019 in China …. and, obviously (if this is true), the whole world “missed” this. If the virus is as contagious as most believe it to be, it would have been spreading all over China … and the world in the early fall of 2019. (However, since the IFR is tiny for the vast majority of people, this does not necessarily mean there would have been conspicuous spikes in deaths).
Based on my own research, I think the virus was spreading (widely) in America by November 2019 … and this wasn’t understood or detected until “latter January 2020”, at least if we believe the statements of CDC officials. I think it’s very possible at least some public health officials KNEW the virus was already spreading in China, America and other countries well before then. If they didn’t know this, they should have known this.
In many past investigations or scandals, a key question is: What did officials know and when did they know it?
The public doesn’t really know the answer to this question … because no reporter has really pursued this line of inquiry. These journalists (and the public) simply accept as incontrovertible the experts’ assertion that the virus was not spreading in America (or the world) until late January 2020.
It’s well past time that someone challenge these assumptions/assertions.
In the early days, there were some news reports about the existence of similar illnesses in Brazil/Brasil as early as Autumn 2019. Some of them were published on YouTube, and might have been mentioned on this site soon after it started. ISTR this was a sewage assessment – rather like what has just been reported in respect of Polio in parts of London today. Thus I think you are right to surmise that it did exist well before it was identified.
As you say, it appears that infections caused by the virus under consideration appear to be relatively benign for most of us – rather like those caused by other coronaviruses, funnily enough. Perhaps adding “SARs” to the name was a mistake, or maybe it was done to ramp up fear; who knows?
If the virus existed and was even half as contagious as we believe … it was spreading. Somebody gave that virus to the 16 people I name in my links and they no doubt gave it to others. Look at the examples cited by the Palm Beach Post and my story on the McCains. Many were married couples that gave the virus to each other – i.e. the virus was spreading. It didn’t just fall out of the air and infect only these few people in “isolation.” I’ve cited examples from Washington, New Jersey, Alabama and Florida. I doubt the virus jumped over, say, Kansas and Nebraska on its way to Sylacauga, Alabama.
I don’t have a degree in epidemiology but most of my conclusions flow from common sense.
Well-said.
I strongly believe there was something around in October/November in the UK.
I had the worse “flu” ever,in my experience in the middle of October 2019 , I am in my 60s and it knocked me for a six for 2 weeks or so.I did not go to the Docs but just got on with it .There seemed to be quite a lot going around in Norfolk at the same time anecdotally.
So if it was the Covid or another similar virus I dont know.
A lot more digging into this should be done .
Dr. Naomi Wolf On New ‘Targeted Gene Editing’
https://rumble.com/v19gqzl-dr.-naomi-wolf-on-new-targeted-gene-editing.html
Bannons War Room
Stand for freedom & make friends with our Yellow Boards By The Road
Thursday 23rd June 4pm to 5pm
Yellow Boards
Junction A321 Yorktown Road/Marshall Rd
Sandhurst GU47 0RT
Stand in the Park Sundays 10.30am to 11.30am – make friends & keep sane
Wokingham
Howard Palmer Gardens Sturges Rd RG40 2HD
Bracknell
South Hill Park, Rear Lawn, RG12 7PA
Henley
Mills Meadows (bandstand) RG9 1DS
Telegram http://t.me/astandintheparkbracknell
I live in a small west country town (UK) which has a large International School in the vicinity, which has mostly Chinese students. I’m generally very fit and healthy. In the 2nd week of November (I can pinpoint the date) I got what I described to friends/colleagues as “a very nasty little virus” which was circulating locally. I felt incredibly tired, had a high temperature and a persistent cough which took about 3 weeks to shift. I took paracetamol for the temperature; whisky for the cough 🙂 and slept a lot…. when I wasn’t at work.
With hindsight, I’m convinced I had Covid. Throughout the past 2 years I’ve lived life as normally as possible and I’m unjabbed. I haven’t officially had Covid, although most of my jabbed friends have, some more than once.
Anecdotal, I know, but I’m sure the virus was circulating long before China alerted the world.
Thats made me think as a good friend of mine works at the UEA and in her department there are a lot of chinese students .I wonder if thats how I got my “flu” ?
It’s the presence of the school which really made me think about it …… I got the bug two weeks after their two-week half-term closure (last two weeks of October 2019). Many would have gone home for two weeks’ holiday and then flown back. Two weeks later the virus was circulating locally.
I cannot put my fingers on the exact timing but we used to meet up regularly for lunch/dinner.Cannot recall her being “ill” with anything though..
At the end of the day, lots of us just don’t know for sure. I did have some kind of respiratory infection in late Dec 2019 – New Year 2020. Reasonably likely that I caught it in the run up to Xmas, and normally would then move on; it wasn’t that bad. However (via this site) I ended up getting some work done privately to see if it might have been caused by SARS-Cov-2. This was done in Jan 2022 using the T-spot technique marketed by a firm in Abingdon, with a blood sample taken by a clinician. Not cheap, and the result was essentially negative – I’m not carrying sufficient T cells that would denote that, so it must have been one of many others that are endemic at that time of year. It would have been interesting if I had proof that I had dealt with the real thing, though.
There’s a big scientific debate, or uncertainty, over how long detectable levels of antibodies persist. I also think the “cutoff values” of all the various antibody tests are worth more serious examination. Also, the decisions on which antibody tests would be “authorized” or “certified” and which were not has grabbed my attention. I think some of the lab results/tests that were no doubt producing higher incidicences of positives were discredited, perhaps intentionally to lessen the “evidence” of early spread?
FWIW, I did get an antibody test in mid May 2020 after experiencing pretty much all the Covid symptoms in early January. This test was “negative.” However, the test results themselves include language to the effect that a negative result does NOT preclude the possibility of earlier infection. Was the fact my antibody test occurred four-plus months after my symptoms perhaps significant?
Personally, based on my research, I think the likelihood of “false negatives” on these tests is greater than the possibility these antibody tests would produce “false positives.”
I think it is significant that Brandie McCain tested positive at least three times, via different antibody tests so the probability her results were a “false positive” are about nil. Michael Melham, the mayor of Belleville, NJ, tested positive twice. The two people who tested positive in Washington State were tested via the “gold standard” antibody assay. Those results were examined by local and state health officials (but apparently never by CDC or national public health officials).
Of course, T and B “memory cells” have more to do with natural immunity than IgG or IgM antibodies.
FWIW, I have never tested positive since I was sick in January 2020. My wife has and I slept next to her every night she had a (mild to moderate) case. It is interesting that my wife didn’t get sick when I was sick … but my two kids were also sick at the same time (their symptoms were not nearly as bad as my own; we all three tested “negative” for influenza at the time) and they’ve never tested positive since either. We’ve all been tested via a PCR test on multiple occasions … and I have taken no precautions against infection.
Thank you to the author and to TDS for publishing this important work. I’m a freelance journalist who’s been investigating the same hypothesis. My degree of confidence this virus was spreading widely around the world before Dec. 31, 2019 is 10 on of a scale where 10 = “convinced beyond a reasonable doubt.”
The following links document 16 almost-certain early cases in America (All 16 tested positive for antibodies).
The first story is about a man in New Jersey – the mayor of Bellville, NJ – who is steadfast in his claim he had COVID on or around November 20, 2019 (The mayor has had two positive antibody test results). The same mayor also reports that several other people became sick at the same conference he first experienced COVID symptoms.
https://www.foxnews.com/world/china-new-jersey-mayor-coronavirus-november
***
This story from The Palm Beach Post identifies 11 people from one small Delray Beach Florida neighborhood who had symptoms in November and December – and all 11 tested positive for COVID antibodies in April. One man, Uf Tokel, was sick in November.
https://www.palmbeachpost.com/news/20200516/coronavirus-florida-antibody-tests-bolster-suggestion-covid-spread-early-in-florida
***
This story from The Seattle Times documents two people who had COVID in December 2019. One of these two people, “Jean,” is a retired nurse from a rural community in Washington state. Local health officials in Washington later said it was “probable” she DID have COVID when she is adamant she did. Still, no official “confirmation” has ever been made about her case and so the date of “Case Zero” in America is still listed as January 2020.
https://www.seattletimes.com/seattle-news/antibody-test-results-of-2-snohomish-county-residents-throw-into-question-timeline-of-coronaviruss-u-s-arrival/
***
This story, which I wrote, documents two people from a small, rural Alabama town (a husband and wife) who almost certainly had COVID in December 2019. The husband nearly died and was in ICU for 24 days in January 2020. The wife has now tested positive for antibodies three times and still had detectable levels of antibodies almost two years later.
Because he was hospitalized and visited medical providers many times, Tim McCain has copious medical records that match all the clinical details of a severe case.
https://uncoverdc.com/2020/06/25/an-alabama-man-nearly-died-from-covid-19-the-first-week-in-january/
SUMMARY: These pieces of journalism identify at least 16 likely early cases in one just country – America. These individuals live in four geographically-dispersed states, an important point as this suggests the virus was not “isolated” in one or two communities. It shows the virus had spread across the country. This figure also doesn’t include the unknown people who infected these 16 people.
Perhaps the most compelling evidence this virus was spreading – widely – before January 2020 is the fact that no employee from the CDC has ever questioned or investigated any of these 16 people.
The U.S. serology study referenced by Mr. Collis was the only one commissioned by the CDC. The CDC (belatedly IMO) tested about 7,400 units of blood collected by the American Red Cross in NINE U.S. states in December 2019 and January 2020. If memory serves, 109 of these samples were positive for Covid antibodies. Two percent of the samples taken in California, Washington and Oregon Dec. 13-16 tested positive for Covid antibodies.
What is interesting to me is that this was this the ONLY study of “archived” blood in America pre- January 2020. Wasn’t there a lot more saved and stored blood officials could have tested? It also took 11 months from blood collection to the results of this study finally being published (in November 2020). Given this was a national emergency, I submit a few thousand units of stored blood could have been tested … in a few days.
There is copious evidence that public health officials either knew – or should have known – this virus had already spread all across America by the end of calendar year 2019 – 105 days before the lockdowns that changed the world.
Needless to say, if the lockdowns were ordered to slow or stop the “spread” of this virus, they happened many months too late.
Yes, they happened many months too late when covid was already on a downward curve – in common with the other two lockdowns. The sad thing is that now covid has been added to the general repertoire of winter ills, it will continue to re-emerge every autumn. If the population had been left alone to get on with things with their own immune systems protecting them, it would just be a general nuisance, and one of those bugs that carries off some of the elderly and infirm each year. However, all this tinkering with dodgy ‘vaccines’ means many more people will get sick (and younger ones too) than would normally be the case, which will encourage even more jabbing (booster 8 or 9 anyone?) and so the merry go round of widespread illness continues ad infinitum.
I agree. I think the “first wave” of the pandemic was completely missed. It probably occurred in November 2019 – March 2020 during the “cold and flu” season – just like the big spikes in the same months the next two years happened.
I think cases were probably on a steep decline by the time the lockdowns were ordered … and that most of the deaths we saw in April 2020 were probably caused by faulty treatment protocols and by so many people being panicked and going to the hospital (at least in some cities) – where the virus spread between people who did have the virus and those who did not. This probably also explains how the virus got into nursing homes so bad and suddenly … and half the April deaths were among nursing home residents.
Like others, I’ve long believed all the Covid narratives are false. But probably the most important false narrative is WHEN the virus began to spread. I think at least some in-the-know officials were probably lying about the pandemic before the official pandemic had even been identified.
I think the same as well. Had the virus never been officially announced, sequenced, and obsessively tested for, people would have simply treated Spring 2020 as a bad flu season, ditto for the following wave in late 2020 and early 2021 as well. They would have adopted the typical “flu strategy” instead of these worse than useless lockdowns, masks, NPIs, panic, and dodgy jabby-jabs. And then it would have been over. Herd immunity would have been fully established before Delta would have even stood a chance. And Omicron may never have even existed as a result too.
People would probably, since they would simply assume it is flu going around and rush out to get the existing seasonal flu jabs, and vulnerable people would probably go get the pneumococcal jab too if they didn’t alread. And through the process of non-specific “trained immunity”, that would have likely still put a bit of damper on the virus (despite it being unrelated) for a time, probably about as effective as the very temporary benefit as the Covid jabs. Beta-glucan supplements could have probably achieved the same thing too, as could thymus gland extract supplements, minus the side effects.
And people would probably take more vitamins and other nutritional supplements than usual as well, as they would during a bad flu season.
So true. All of these dodgy jabby-jabs seem to be only prolonging the pandemic and delaying the inevitable transition to endemicity. Kinda like the worse-than lockdowns did.
*worse-than-useless lockdowns
I worked extremely hard on a feature story I thought was going to be my first national or international “scoop” – a story that presents copious evidence that an Alabama couple almost-certainly had Covid in December 2019.
Well, my big blockbuster story was completely ignored by the mainstream media – and still is to this day.
I came to believe that an even more sinister or depressing story was the FACT that no (national) “public health” officials would even bother to investigate these likely cases. The mainstream press has also completely ignored this line of inquiry (although The Seattle Times and Palm Beach Post did excellent journalism on this topic in May 2020 … since this date, their journalists and editors have completely lost interest in the topic for some reason).
My follow-up piece summarizes some of the evidence of “early spread,” but my theme with this article was that important information regarding the origins and timeline of spread of this virus has been ignored. Readers can reach their own conclusions as to why seemingly very important information was NOT investigated nor reported.
Perhaps this is beginning to change? I’ve since compiled more evidence that supports my hypothesis, which I hope to summarize in a future article.
https://uncoverdc.com/2020/07/13/covid-19-is-a-real-search-for-the-truth-now-taboo/
Here’s an article from NBC News that summarizes statements from CDC officials who said in a press conference in late May 2020 that they could find no evidence of “early spread” in America prior to “latter January 2020.”
https://www.nbcnews.com/health/health-news/coronavirus-started-spreading-u-s-january-cdc-says-n1217766?cid=sm_npd_nn_tw_ma
The author points out the ONE antibody study of blood collected before “latter January” 2020 in the USA. In my opinion, this study provides the most persuasive evidence of “early spread” in America.
This study of Red Cross archived blood found 109 positives out of 7,389 sera tested (which equals or suggest 1.4 percent “prevalence” among these two tranches of blood. The percentage was 2 percent in samples taken from Dec. 13-16 in Washington, Oregon and California).
Collis mentions something that jumped out to me in reading this study multiple times:
“The authors caution that the samples included in the report may not be a true representation of all blood donors and hence their observations should not be taken as a generalisation across all donors in the same time period.”
I think the language of study authors warns that results should not be “generalized” to any population group. My question is why not? The authors don’t provide any convincing reasons WHY we should not generalize these findings to the entire population.
I’m a non-expert layman, but to me, a group of random blood donors is about as good a random sample of Americans as you are likely to find.
If anything, this sample almost-certainly undercounts community prevalence at the time. Blood donors, per the study, are much older than the median age of the population. I think the median age of donors was 52 while the American median age is 39.
Many blood donors are retirees, who do not come in contact with nearly as many people as younger Americans in the workforce. Young people, the most likely to be infected, would be under-represented in a blood-donor cohort.
Furthermore, blood donors are not supposed to donate blood if they have been sick in recent weeks, which would exclude those who might have active or very recent infections.
The study also does not specify which donors tested positive for IgM antibodies (which show “recent” infection) and those that tested positive for IgG antibodies and negative for IgM antibodies (a combination that would show the donor probably had the virus weeks earlier). I have perused many of these antibody studies and am disappointed serology studies from April 2020 or later typically do not give a breakdown on IgM-Positive and IgG-positive results. (The results I would flag in these cases would be those individuals who tested negative for IgM but positive for IgG – suggesting these people had been infected weeks or months before they donated blood).
Finally, the Red Cross Blood study says that donors were “de-personalized” and apparently no interviews were conducted of the individuals who did test positive for antibodies. This is very strange to me. Wouldn’t virus-origin sleuths want to know if and when these people may have experienced Covid symptoms? If I was in charge of this study, I would have rushed to interview these people and also tested their close contacts.
I also want to thank Mr. Collis for publishing the Italy antibody study … which does break-down “positive” antibody results by IgM and IgG categories. I had not seen this study and the results are stunning. This is not a few “positive” results and they date to September 2019. Note also that most are positive for IgM only – which means these were RECENT infections. This study alone should be front-page news in every newspaper in the world IMO. I wonder if contact tracers in Italy made the effort to interview all these positive people about any symptoms they may have experienced.
By itself, this study (if believed) PROVES that this virus was spreading widely well before the Wuhan Outbreak (first reported to the W.H.O on Dec. 31, 2019.)
While readers were warned not to extrapolate or “generalize” the findings of the Red Cross study to the entire population, I went ahead and did this anyway.
To donate blood, you have to be at least age 16. There are approximately 270 million Americans age 16 or older. The results of this antibody sample (from nine states) found that 1.4 percent of Red Cross blood donors had detectable levels of antibodies by mid-January 2020 (the date the second tranche of archived blood was tested).
That would represent 3.78 million Americans who had antibody evidence of Covid by this date (if one DID “generalize” these assay results to the entire adult population). Actually, since it takes about two weeks for antibodies to form, we could say 3.78 million adult Americans might have been infected by the end of 2019 – probably more and earlier than this as people who had been recently symptomatic would not be giving blood. The number would be higher if we included those under the age of 16.
So maybe 4 or 5 million Americans had already been infected by the time the Wuhan Outbreak was first reported. And this is just America.
If this is close to true, and authorities had good reason to suspect this was or might be the case, the fact that they still ordered lockdowns of the entire world would qualify as a crime of epic proportions.
Some might reply that public health officials had no way of knowing this by December 31st, 2019. This might and probably is true. However, they could have known it by, say, the end of January 2020 – which would still be 45 days before our leaders ordered the lockdowns. The first tranche of Red Cross blood was from donors who gave blood Dec. 13-16, 2019. I submit that officials should have tested this or other tranches of blood for antibodies by late January. It would take just a couple of days to get the results. So when CDC officials said they had found no evidence of “early spread” prior to “latter January 2020,” this is only because they weren’t looking. Someone in America’s massive “public health” bureaucracy should have said, “Let’s test some Red Cross blood ASAP.” For some reason, no one said this or thought this or did this.
My husband and I spent 2 weeks in Tenerife at the end of November beginning of December 2019.
Within a few days of returning home (East Midlands), we became unwell with “classic flu symptoms” and coughs that lasted for weeks. I was very poorly and it felt like flu which I have only had once before in my life (I am in my 60s). We had to miss a family wedding held between Christmas and New Year because we felt we could still be infectious with “whatever it was” and also felt completely drained.
It took many weeks before we felt “back to normal”.
BTW my husband is never ill but even he felt pretty crook.
One of our daughters who lives in Loughborough (Which has a big University with a lot of foreign students) was very ill with “flu” in early February 2020.
The symptoms we all had are exactly the same as those listed for Covid.
I started using breath mints (for the first time in my life) after my illness because I could not get rid of the foul taste in my mouth. I still can’t and use them several times a day. Although I have not lost my sense of taste or smell.
It never occurred to us to go to the doctors.
Question: Did you test positive in the year after official Covid? If you really had Covid, you would have developed natural immunity.
I have saved hundreds of anecdotes just like yours. Is everybody who thinks they had Covid in these months wrong? I also think I had Covid in January 2020. I went to the doctor, got a flu test and this test was negative. So our flu-like symptoms were not caused by influenza.
There are MILLIONS of people who had already been infected by this virus by, say, the middle of January 2020. The CDC has said there was no evidence the virus was spreading in America before “latter January” 2020. I don’t believe them. The evidence is overwhelming this was happening … so how did they “miss” it all? Or were they really looking for it?
Throughout this pandemic, the m.o. of public health officials has been to NOT investigate anything they do not want to “confirm.” That’s probably why they didn’t investigate the people who had antibody and symptom evidence they DID have Covid. A real and honest investigation would “confirm” that these people are right … and that the officials were wrong … and/or had been telling fibs all along.
The question that keeps occurring to me is WHY would they lie about this, or refuse to investigate these claims? The only answer I can come up with is that at least some officials KNEW the virus was spreading early – probably in November 2019 or October 2019 or even earlier. Well, how in the world could someone have KNOWN this?
No. I was tested numerous times during 2020 and early 2021 because I come into contact with vulnerable people. I also signed up to Zoe and have had random tests as well.
Not a single positive
Thanks. I also have never tested positive for Covid and I also think I had the disease in January 2020. This is anecdotal “evidence,” but it would fit the hypothesis that many more people were exposed to the virus … before it was even supposed to be spreading.
I have proposed a study of the many people who had Covid-like symptoms before March 2020 (those who tested negative for influenza). Compare this group to a group that did not have Covid symptoms during this period of time. My hypothesis would say that the the people who were sick with “something” between Nov. 2019-March 2020 would have far lower incidences of “testing positive” for Covid in the ensuing 12 months (because, the assumption would go, they developed natural immunity and thus very-possibly DID have Covid in this time frame). If a study found this to be the case, this would support the early spread hypothesis IM0. I of course do not think any such study will ever be commissioned … For reasons obvious to myself.
I know a number of other people in England and Wales who became unwell in late 2020 early 2021. The key similarities between us were in our 60s and 70s and able to take winter sun Holidays and the cough that lasted for weeks.
I suspect we did our bit in helping herd immunity during that time.
I live in Loughborough and my wife worked in the Pilkington library at the university.One whole section of the front facing staff were off in January 2020. It was the urgent care centre in Oadby, south of Leicester where we had the attendances described above. Oadby is home to the University of Leicesters halls of residence. There’s also De Montfort university in Leicester.
About the lack of excess deaths before the official start of the pandemic, another possible explanation (besides the age profile of the patients) is that the variants circulating at this time were less deadly and infectious. They may still have been evolving into a variant with pandemic potential.
It would explain why the pandemic didn’t take off immediately, which seems odd given the R numbers we saw when the virus was isolated – and it is more consistent with a natural origin of the virus, compared to a highly infectious variant appearing out of nowhere. It’s hard to believe in a natural origin without seeing some signs of early evolution of the virus.
My amateur hypothesis would be that the virus has always had a very low IFR (very similar to the influenza for most age groups) and so although some people were obviously dying these deaths were missed or attributed to pneumonia or whatever. The massive spike in deaths basically occurred in one month – April 2020 – and a disproportionate percentage of these occurred in a relatively small number of cities (like New York, New Orleans, Detroit. They also occurred disproportionately in inner-city “public” hospitals that care for the poor). As mentioned, about half were among nursing home residents. So somehow a virus that had not decimated nursing home residents previously suddenly did start to devastate this cohort. Also, as mentioned, many of these deaths were probably caused by faulty treatment protocols … and might have never occurred if these patients had been treated the same as they were before Covid was discovered.
The major objection or reason my “early spread” hypothesis is rejected or dismissed out of hand by many people is that critics say there would have been far too many deaths to have been “missed” if the virus was spreading months earlier than believed.
I welcome and solicit the opinions of better thinkers than myself, opining on how this could perhaps be explained. My focus, though, is not on what didn’t happen, but on all the evidence I think does point to early spread having occurred. That evidence is pretty copious IMO.
I didn’t mention it in my partial evidence summary above, but I have saved scores of articles (and CDC and state health agency ILI weekly reports) that show that the “flu” was both “severe” and “widespread” in most U.S. states in the “flu season” of 2019-2020. I’m not saying everyone who had an Influenza Like Illness definitely had Covid, but I think a fair percentage probably did.
I think this was the real “first wave” of Covid.
In July 2019, on a cruise ship with many Americans, I contracted a severe uri with severe cough, fever, fatigue. Ship doc prescribed antibiotic, cough med, decongestant. Cough lingered. In England saw practice nurse, thought I might have pneumonia. When I asked what I had her response “we are seeing a lot of weird viruses right now”. Many many friends my age had something similar Dec/Jan 2019/20.I am convinced covid 19. Was around much earlier than suggested. Ft. Derrick? We will probably never be told the origin of Cov 19.
You don’t mention Portugal.
My Brother in law lives and works just south of Oporto and was in a management meeting with 11 others on 8 Jan 2020. One of the Directors present had just returned from a tour of Japan, Macau & Taiwan and was coughing a certain amount. By 11 January 8 of them had very high temperatures, extreme tiredness, coughs and though some went back to work within days they were quickly off work again and took 2-3 weeks to fully recover. An antibody test taken later in the year indicated that they had all had Covid. In this business we had one of our younger members of staff who ended up being hospitalised in early February with an “untreatable” respiratory virus which turned to pneumonia. He got better and then went down again a few weeks later. Interestingly despite repeated requests the NHS repeatedly refused to give him an anti body test and say that he definitely did not have Covid, however the symptoms were almost certainly those of Covid.
This is a compelling anecdote. I wonder if I could interview your brother-in-law (Or send him an email for this same info)? You can find my email address at the bottom of my story on Tim and Brandie McCain at uncoverDC.com.
… the anecdote about NOT doing antibody tests is also perhaps important. I’ve found similar stories in my research. It’s like they intentionally tried to keep people from getting antibody tests, especially in the early months of the pandemic.
The main problem in all of this is the manipulation of data.
I refer to all deaths within 28 days of a positive covid test being claimed as due to covid. Also the incentive in the USA to claim a death as covid so the hospitals could profit from this.
The PCR test was never meant as a diagnostic tool on it’s own as per the inventors instructions. I found it stunning the timescale for the ‘roll-out’ of the lateral flow tests which were at best dubious.
Well done BR and others for scouring through and obtaining this data.