
New Zealand is a fascinating country – amazing geography, likeable population, and, unlike its neighbour Australia, most of its wildlife isn’t planning on killing you at the slightest opportunity. It is also fascinating with respect to Covid because its population has a very high vaccination rate across all age groups (well, down to five), but up until recently there has been negligible natural immunity to Covid. Because of these two factors, New Zealand was always going to be of interest as soon as Covid arrived properly, if only to see how its vaccination efforts had protected its population.
For those who missed it, since the end of last year New Zealand has had a succession of Covid waves. These started small, but in the most recent wave, taking place during February and March, infection rates were enormous – if we had these infection rates in the U.K. we’d have peaked at approximately 350,000 cases per day (rather than around 200,000). What’s more, it looks like New Zealand exceeded its testing capacity during that wave, suggesting that peak infections were probably even higher. It is relevant to note that during February and March, New Zealand had over 90% of all the cases it has ever had and most of the rest occurred in January – prior to 2022 New Zealand reported very few Covid infections.
So much for the Covid vaccines protecting against infection – but what do the data look like in detail?
Cases
New Zealand is somewhat helpful in that it does publish daily cases, hospitalisations and deaths by vaccine status; somewhat because it doesn’t allow easy access to anything other than the current day’s report. Thankfully, the Wayback Machine ensures that at least some web pages aren’t forever lost to history. These data were collated for dates since mid February 2022 and smoothed with a seven-day moving average to create a time series of Covid cases by vaccine status.
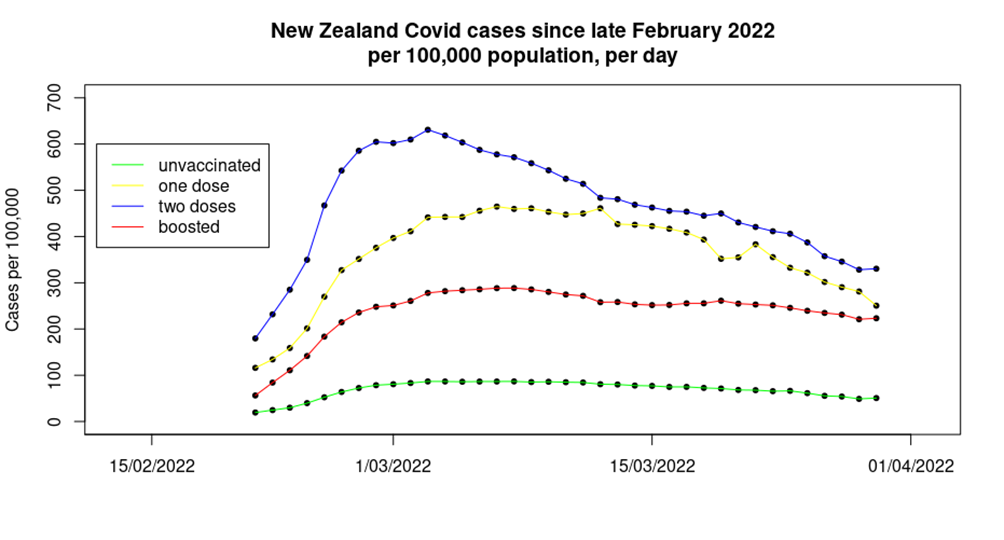
The first time the above graph popped up on my computer screen I had to go and double check all the data sources – and then I triple checked them. The data shown on the graph are notable for several reasons:
- Firstly the obvious one – during the most recent Covid wave there was a much lower infection rate in the unvaccinated, compared with those that had been given one, two or three doses of vaccine. What’s more, this isn’t a small effect – over the period shown approximately:
- 10% of the triple vaccinated in New Zealand were infected.
- 14% of the single vaccinated were infected.
- An astounding 18% of the double vaccinated were infected.
- Yet only 3% of the unvaccinated appear to have been infected.
- The order of the effect is unexpected – for some time in the U.K. the highest case rates have been found in the triple vaccinated, with case rates in the single and double jabbed much lower. In New Zealand the highest rates are seen in the double vaccinated.
- The data for cases in the double dosed appear to have an earlier peak than seen in the data for the unvaccinated, single jabbed and triple jabbed.
- The fall from peak cases to the most recent data point is also interesting. Case rates in the unvaccinated, single dosed and the double dosed have all fallen approximately 45% since their respective peaks, however, case rates in the triple vaccinated have only fallen approximately 20% since their peak. This is rather concerning, as it suggests that we might find that the boosted population maintain a viral reservoir for Covid, ensuring that case rates take much longer to fall to trivial levels and hindering attempts to get society back to a post-Covid normal.
The infections data from New Zealand allow us to estimate the vaccine effectiveness for the Covid vaccines in the absence of natural immunity.

These data are in contrast to recent data from the U.K., which show one and two doses of vaccine to have a VE of minus-50% to minus-100%, and the booster to have a VE of around minus-300%. While this sounds counterintuitive, it is possible that we’re seeing a complex interplay between a waning of the impact of the vaccine and the impact of additional vaccine doses:
- The U.K. vaccinated early, allowing for the impact of those early vaccine doses to have waned significantly for those choosing not to top-up their ‘protection’.
- The Covid vaccines appear to have a period of approximately two to three months where their impact on the immune system is different than in later periods; this is possibly due to the creation of short-lived IgA (mucosal) antibodies. In the U.K., booster vaccinations were given in autumn 2021, and thus most individuals will have been beyond this period when the Omicron variant’s first wave appeared in December.
In New Zealand, the timescales are very different: those given the booster dose will still be in the two-three month period where short-lived immune responses dominate; those given two doses will be in the proposed period of maximal vaccine negative impact; while those that chose not to accept the offer of a second vaccine dose will be in the period where vaccine effects are waning.
There’s one more point to add for cases in New Zealand, and it relates to the U.K. For months, the UKHSA has been telling us that one possible reason for us seeing far fewer cases in the unvaccinated compared with the vaccinated is because the unvaccinated have natural immunity following high infection rates previously (presumably because the unvaccinated are reckless and didn’t follow lockdown rules – I imagine that they also ride motorcycles too quickly, set off fireworks indoors and play with matches while filling up the car). These data from New Zealand, which at the time had very few individuals previously infected with Covid, show lower case rates in the unvaccinated without any significant levels of natural immunity, contradicting the claim of the UKHSA and eliminating one of its reasons for ignoring the alarming data.
Hospitalisations
Analysis of the hospitalisations data offered by the New Zealand authorities is made complex by there being no stratification of the hospitalisations by age group, and the lack of complete vaccinations data by age. However, U.K. data show that in recent weeks approximately 95% of hospitalisations were in those aged over 60; assuming that this will also hold true for the New Zealand population allows us to offer a indicative analysis of the likely impact for that age group of the vaccines on hospitalisations in the country.
The analysis is also hindered by the data on vaccine coverage for those aged over 60 not differentiating between those that have had only one dose of vaccine and those that are unvaccinated. This might in isolation from other data appear to be ‘sensible’ – after all, the single dosed have the ‘least protection’ as well as ‘the longest time for protection to wane’. However, the data shown in the previous section suggest that the unvaccinated and those having taken a single dose of vaccine are in no way comparable, and that considering them as a single group could lead to misleading conclusions. Nevertheless, that’s the hand that’s been dealt for us.
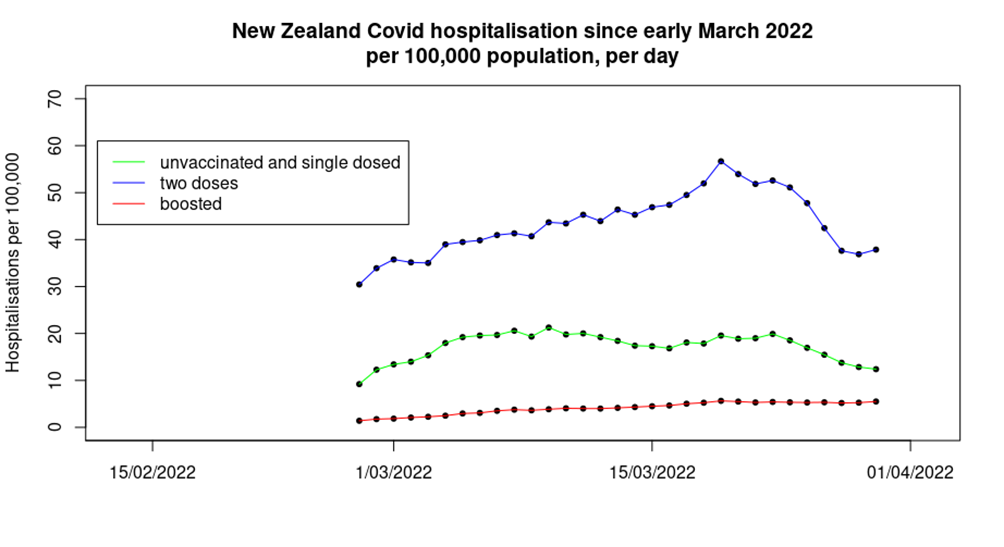
The data are somewhat surprising. While those given a booster dose of vaccine seem to have lower levels of hospitalisations than found in the group containing the unvaccinated and those given only one dose of vaccine – as might be expected – the double dosed have significantly higher hospitalisation rates.
Also interesting is the trend in the data:
- Hospitalisations in the unvaccinated/single-dosed appear to peak earliest – we have also seen this effect in U.K. data, usually in the form of dire warnings early in each Covid wave that the only people being hospitalised are the unvaccinated, only for the warnings to go quiet later in the Covid wave when the data move in the opposite direction.
- Hospitalisations in those given two doses of vaccine appear to peak towards the end of the period shown.
- Hospitalisations in the boosted population appear to show little signs of slowing down, let alone reducing, over the period in question. Note also that this group saw a fourfold increase over the time period shown, whereas the double dose and single-dose/unvaccinated group both saw a 25% increase, albeit with an intermediate period with higher hospitalisation rates.
It was not possible to properly disentangle the hospitalisations data for the unvaccinated, but the data suggest that in aggregate those having taken two or three doses of vaccine (when the two groups are put together) have approximately 45% lower risk of hospitalisation than the unvaccinated/single-dosed. It is worth noting that in the U.K. data we see higher hospitalisation rates in the single vaccinated in those aged over 60, compared with the unvaccinated. It is possible that the same pattern is found in New Zealand, only ‘covered up’ by the co-mingling of the data. If this is the case then the apparent protection offered by the vaccine in the two or three dose individuals will be somewhat lower than 45%.
Deaths
The mortality data from New Zealand are also complicated because the health authorities lump together into one group all the unvaccinated and those having taken a single dose of vaccine. Beyond that complication, deaths data can be tricky to analyse, because there are such huge differences in death rates from (or with) Covid by age. Fortunately, the mortality data offered by the New Zealand authorities do include deaths by age group, which allows a finer analysis than was possible with the infections and hospitalisations data.
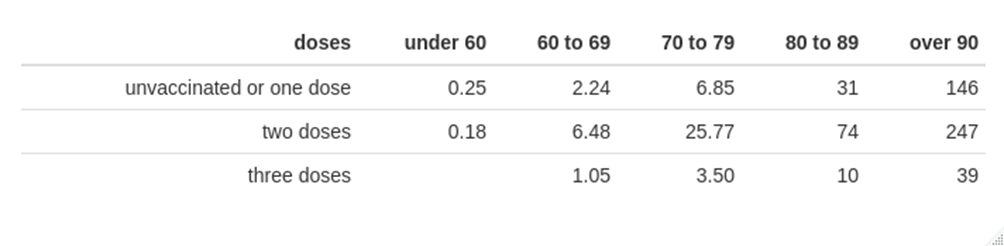
The above table suggests that while those given three doses of vaccine have a decreased risk of death from (or with) Covid compared with the mortality rate in the strange group called ‘unvaccinated or one dose’, the risk of death is greatest in those given two doses of vaccine.
However, it is possible that New Zealand’s data have a similar pattern to that seen in the U.K. (and elsewhere), where dose effects are complicated by the health of those given each vaccine, namely that those closest to death were spared a dose of vaccine, and thus concentrated deaths into the very small number left in the prior dose group. A comparison of the data for ‘unvaccinated or one dose’ with ‘two or three doses’ suggests that the vaccines do still protect against death, but only to a very low degree in younger age groups.
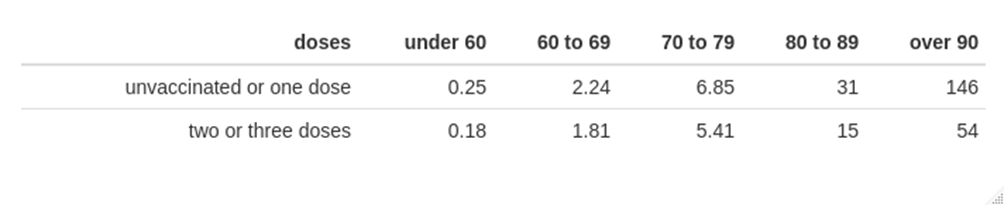
The data above support the use of vaccination to protect against death from (or with) Covid for those aged over 80. On the other hand, the mortality rate in those aged under 60 is very low, and the estimated vaccine effectiveness in protecting against death for those aged under 80 is only approximately 30% – once again, the real-world vaccine effectiveness estimate is rather low. It is also of note that these rather poor figures for the protection offered by the vaccines against mortality come from a country that started vaccination rather late (summer 2021) and where most of the population were only given their booster doses two to three months ago. These data suggest that the vaccines simply do not offer substantive protection against death for newer Covid variants, rather than it simply being a case of waning vaccine protection.
It is also important to note that the data on the benefits of the vaccine in protecting against death shown above should be treated with caution:
- Data on deaths in the unvaccinated and those given a single dose of vaccine are co-mingled; the New Zealand hospitalisation data suggest that death rates might be greater in the single-jabbed.
- The vaccinated appear to have significant increased risk of catching Covid, which contributes to overall risk of serious disease and death.
- These calculations do not include any consideration of the risk of side-effects and complications following vaccination.
Overall mortality
One other aspect of the data coming from New Zealand that is of interest relating to Covid is excess mortality. These data are of interest because New Zealand managed to keep itself more-or-less clear of Covid until the last few months of 2021, and even then case numbers were very low until 2022, with the result that Covid deaths were negligible prior to 2022. With that in mind, its excess death data between the start of 2020 and the end of 2021 are very interesting.
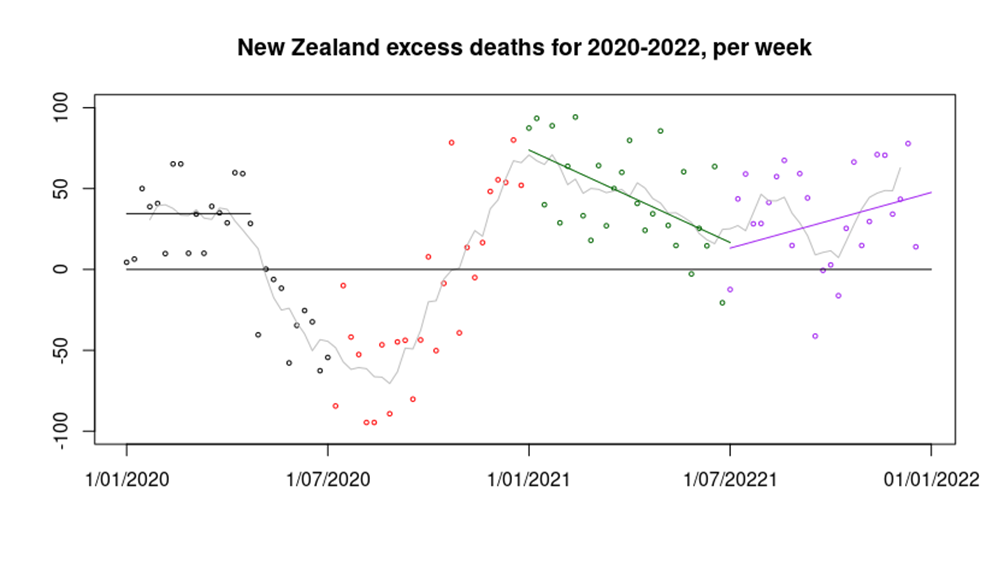
Many countries around the world had a peak in excess deaths in the first quarter of 2020, followed by a significant reduction in deaths into mid 2020. There has been speculation that this pattern was seen because Covid infections in early 2020 killed the most vulnerable, leaving a period in which there were fewer people left to die. However, New Zealand also has this pattern of excess deaths in the first half of 2020 (black data points in the graph above) without Covid infections, suggesting that the reduction in deaths seen in mid 2020 were a result of lockdown. The reason for the excess deaths in New Zealand in the first quarter of 2020 are not at all clear.
Most countries then saw an increase in deaths towards the end of 2020; this has been explained by a resurgence in Covid cases. However, New Zealand saw a similar pattern without Covid infections (red data points). It is possible that this increase was caused by the impact of the reduced healthcare provision during the extreme lockdown – though there are no data to support this supposition. There are reports that the New Zealand healthcare system experienced its busiest summer (January and February) on record with hospitals across the country reaching ‘crisis point’ and several emergency departments at capacity. The cause of this healthcare pressure is unclear, however.
Perhaps the most interesting data in the graph above are seen in 2021. During the first half of 2021 excess deaths slowly reduced from the high seen at the start of 2021 (green data points), perhaps a result of healthcare provision returning to normal. However, around mid-year the trend reversed and excess deaths started to climb again (purple data points). Again, it must be pointed out that there were very few Covid cases in New Zealand at this time, and negligible deaths. Just about the only unusual things occurring in the country at that time were a lack of international travel, restrictions in day-to-day activities for the population and an enormous mass vaccination campaign using novel, under-tested vaccines.
During 2020-2022, there were approximately 2,000 excess deaths in New Zealand, a significant number in a country with a population of five million. We don’t know the proportion that occurred because of lockdown, vaccines or something else; all that we do know is that they weren’t a result of Covid.
Note on data analysis methods. Infection, hospitalisation and mortality data were obtained from the New Zealand Ministry for Health (using Wayback Machine for historical data). Vaccination data were also obtained from the NZ Ministry for Health. Population data were obtained from Stats.govt.nz. Vaccination data were offset by seven days for the infections analysis to account for the Ministry for Health’s definition of vaccine status at infection. An additional seven days offset was applied for hospitalisation, and 14 days for death, to account for the typical timescales of disease progression.
Amanuensis is an ex-academic and senior Government scientist. He blogs at Bartram’s Folly.










To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
If it was designed to work against anything it was against the Wuhan variant, but they got Omicron in NZ. Who knew it was so hard to make vaccines against a mutating coronavirus?
The Wuhan variant being a computer generated composite of RNA taken from one patient.
Now why wouldn’t a vaccine against a computer simulation be medically helpful?
Such are the mysteries of life.
Given that some of the sequences spliced into the virus in the Wuhan lab are identical to those found in Moderna’s own IP, you would think they at least might have had a decent effort at it.
The UK Common Cold Research Unit which gave up in 1980 after 50 years or trying.
They have not made a ‘vaccine’ against the virus – that’s the secret!
Maybe they will learn the lesson in advance of the next virus on its way – iron out those wrinkles.
Excess deaths data is interesting. I don’t buy the “lockdown” and “healthcare” explanations though. For me there are only two possible explanations:
?
Dunno about the specifics, but from general principles you can see why New Zealand might be a choice country for siting some especially unpleasant research. Iceland is another.
So it seems is our New Special Friend – the Ukraine!
We have been lab rats from the beginning. It was blatant. Oh where is that whistleblower who can reveal the unredacted Pfizer contract to us. Some telling signs since The Beginning: strict border controls from 26 March 2020, quinine containing products were unable to be prescribed by doctors from about July 2020, the importation of antibody tests was banned from April 2020, it’s illegal to import ivermectin tablets (suitable for human use), and the Pfizer product was the only one available until recently. I will stand corrected if anything I have said is not correct.
If the virus really was circulating many months prior to the official March 2020 outbreak, then it is hard to believe they would not have imported it already by the time the borders closed. But it is possible that it simply died out on its own with no fresh waves arriving from abroad perhaps?
Then the vaccines have triggered an explosion of cases once the inevitable Omicron wave arrived.
I have wondered if that might be the case.
The sequence might be that each circulating variant produces a covid wave, but that this is self-limiting and infections fall to zero rapidly. A minor mutation then allows the next variant to take hold.
Thus the data in NZ might suggest that they might have had the first variant in autumn 2019, but through their closing the borders they didn’t import the next variant. In addition, the population of NZ was too small to evolve their next variant themselves. Thus covid disappeared until infectious pressure (possibly vaccine related) increased sufficiently to allow an imported case to seed a covid wave.
If this is the case then the massively increased case numbers that we see now (probably a result of vaccination) would produce each new viable mutation more rapidly; it is possible that we’re seeing the consequence of this in a reduction in the time-gap between covid waves (eg, the Zoe data suggests that this might now be as low as 4 weeks, compared with the 12-20 weeks seen in 2020). In addition, the increased level of cases would mean that even a small country like New Zealand might be able to produce home-grown viable mutations even with closed borders.
That makes a lot of sense.
As a result of ‘vaccination’ – yes. But also as a result of obsessive testing (giving many false positives). And they’re not ‘cases’ for the most part.
So if they are following ‘the science’, the jabbing should stop as there’s no point. As there’s no point in jabbing and the incidences post vaccine, it would seem logical
They gave up on science long ago … it’s now just a cult. In 2000 years time they will no doubt be worshipping the prophets who saved them.
Plenty where I am fully masked up. Sun is shining, few of them will know anyone hospitalized or dead. And yet there they are. Cult-like behaviour all around me.
Agreed, it is very cult-like. We who are sceptic should talk more about known cults – ones that are accepted by everyone as being cults. When AIDS was the thing, followers of Bhagwan Shree Rajneesh, also known as sannyasins, had to wear rubber gloves when having sex. Making sure they always walked on the left-hand side of the pavement, though, probably would have been far too fruitcakey for them.
Because virus just thrive in the u/v in sunlight.
Logic and common sense has been missing from all government decisions.
… since forever.
Only if you believe their goal was to help. If instead it was to extend the technocratic agenda and stage manage our lives from cradle to grave then it has been a roaring success.
I agree also with the cult analysis, which when I said that many months ago I got looks as if I was demented. Just yesterday, young niece was ringing around trying to find someone who had a free tester thing as she had a cold and then actually sounded smug when she got a positive result. Apparently most people are saving their free tester things for their holidays!!
We can only assume it is meaningful behaviour for them. Even casual understanding of testing casts doubt on its usefulness. They must get some sense of satisfaction from it.
Well Vaxtastic, COVID (would that I had a font large enough) is the importantest thing in the whole wide world ever – a thing of historic proportions.
How exciting to have it! And if you’ve been jabbed, you’ll go straight to heaven when you die – only you won’t die really, not ever.
There are a few countries that demand negative test results before allowing “vaccinated” Brits to enter. These include the USA and Russia. Not that many Brits plan to go on holiday to Russia this year.
Don’t be daft where would Mr Gates, Fauci and Governments get their money and source of control and power if the injections were stopped.
Canberra signed a contract with Moderna to produce 100 million doses of MRNA. Four shots for every Australian man woman child and [insert current PC term for other genders here].
Maybe they plan to vax the roos and emus too.
The ‘jabbing’ should surely stop anyway – it was only ‘approved for emergency use’, surely? Doesn’t that mean that, since the emergency no longer exists, the drug should be licensed before it can continue to be used?
It’s obviously all the fault of the virus which prompted the manufacture of ineffective vaccines that do more harm than good but someone in authority seems the balance of harms vs risk justifies the risk for something that in most people is like getting a mild cold.
I think I had covid in early March 2020, I was in bed for 1 day, I assumed it was the 2 bottles of red I had the previous day and a heavy cold that slowed me down. I didn’t think it was wuhan flue as I had non of the symptoms apart from a slight headache from the hangover.
i wish I never had those jabs now either, but I needed them for travel.
hopefully more countries will now rescind their travel restrictions.
“I needed them for travel.”
To which country?
Countries that required jabs for entry plus negative pcr tests.
that’s countries like the US and others who pegged their rules to what the US was doing, also Europe.
spain will allow you in if you’ve proof you’ve recovered. Other countries won’t permit that.
some countries allow unvaccinated in but they need to quarantine at authorised facilities at the travellers expense.
it’s all been well publicised.
This is one of the ‘still painful’ aspects of the covid response — within countries there’s popular pressure to remove all of the covid interventions — after all, is is clear that they’re completely pointess.
However, three is much less public pressure when it comes to people crossing borders. I imagine that these non-scientific limits on movements will continue until the pressure becomes too great to support them. I imagine that the main pressure will come from travel for Africans, where vaccination levels are much lower (hence they see lower intensity covid waves) and it could readily be argued that border limitations at borders are racist.
I originally didn’t take the jab on principle: to make the point to those under child bearing age, that it would be criminally irresponsible for them to take an untested jab. I thought I was taking a risk, but it’s now very clear, that even ignoring the additional long term risks from taking the jab, there was more risk from the jab than without it.
And still not a peep in the mainstream. I have one person in my circle aware of this. They visit this website and other related sources.
As for the rest? Complete indifference. I’m now at the post-shock stage. I no longer expect people to really care, and nor am I surprised they are getting their children injected.
It would seem the Behavioural Insights Team have a good grasp of psychology after all. We are the cranks despite our obvious common sense.
For me it was basic caution to hold back on being injected given the speed of development and the obvious propaganda campaign. Seeing people around me fail to invoke a similar sense of caution surprised me at first but now no longer does. A family member recently had his 5yo injected which saddened me, but didn’t surprise me.
I’m trying to avoid asking – I know most people I know have been jabbed, if family members or close friends start telling me they have jabbed their children I’ll probably never be able to think of them in the same way ever again.
I am the same. Permanent damage. I’ve been through multiple rounds of mental gymnastics, giving them the benefit of the doubt. Extreme propaganda, project fear, professional psychologists writing the scripts. But I draw the line at injecting young children with a biological agent that clearly doesn’t work and in many cases failed to protect the parents themselves.
I am assuming unless told otherwise that everyone I know and meet and come in contact with (with a few exceptions who are known to me as having same stance as me) that they are all jabbed to the eyeballs as they are fully on government /MSM messaging. So I don’t bother asking either.
I’d really love to know if any of them are waking up yet!
I’m finding that I’m less and less inclined to bother talking to my stupid ignorant friends at all, which is sad. I shall try to keep some of them and just avoid talking about Covid, but that’s sad too, given the impact it has had on all our lives.
Same here. I occasionally try a tentative exploratory comment/question to see if I get a response but they usually fail/refuse to bite …. so I don’t pursue it. I’m sad at how many friends/acquaintances have had a bad experience but still don’t/won’t make the connection.
Can’t talk about Brexit, can’t talk about Trump, can’t talk about Covid, can’t talk about Ukraine… the polarisation of so many topics where, if you disagree or are even curious, you must automatically be some kind of conspiracist nutjob, is making it difficult to talk with people you know and almost impossible with those you don’t.
Edit: it is interesting though that, once you have estabished their position on one topic, you can pretty much guarantee their stance on the others…
Yes, clustering. I’ve noticed this too. Reluctance to discuss Brexit in a mature fashion guarantees a discussion about the demographic changes suggested by mass immigration is off limits. Just one obvious example.
Difficult to avoid the conclusion it is all cowardice.
Good to know it’s not just me. To me, the Big Lies, as I call them (better not name them but most people here probably know what I mean), define the monstrously corrupt times we are living through. Wilfully ignoring them seems to me to be complicit in the destruction of civilisation. Somehow before the Great Vaccine Lie I managed to put up with people who didn’t want to know what was really going on in the world. Now I can’t. I’m not sure it’s cowardice. Seems more like sheer stupidity to me.
I see it as more of a desire to appear woke and PC and thereby be socially acceptable
Perfect comment summarising my feelings. Basically I am demotivated to talk to anyone about anything anymore.
I actually think this is deliberate on the part of TPTB – stoke up these divisions as a way to a) divide and conquer and b) set one group against each other to promote social unrest.
Going forward I don’t think things are going to be pretty.
Nailed it pjar!!!
I’m in same position and it is sad – like there is a huge, dare I say it, intellectual gulf between us, because it does sort of boil down to intellect, and thinking about things and having an inquiring mind and not taking everything at face value and doing your own research, and a lot of the people I know just don’t do any of that.
You are not alone. I think this describes how many of us are now dealing with our relationships.
I used to think the world was divided into 2 types of people, lager drinkers & bitter drinkers. Lager drinkers lacked a sense of tradition, innate good sense & in their small way each lager they drank was a betrayal. Sadly, having assumed initially that a Venn diagram showing vaccine refuseniks & bitter drinkers would overlap I’ve been mightily disappointed & have had to conclude that my classification model didn’t stand up (as Mike Tyson predicted) to being punched in the face.
The world’s a more complex place than I thought.
I agree, however we still need a heuristic to navigate the world. Your original Venn diagram works fine. I split the world into two, those who will apply critical thinking and those who don’t.
We could speculate on why someone is in the non-critical camp; propaganda, fear, childhood trauma. Who knows? In the end it doesn’t matter. I am not a doctor or epidemiologist and yet I didn’t succumb. All it took was caution, which to me seems reasonable, and then some basic reading. The other camp failed to do this, for whatever reason.
That’s really all it needs. New fangled lager, or traditional beers and ales. It is all the same.
A little publicised fact:
There are 10 kinds of people: Those who understand binary, and those who don’t.
God knows what you’d make of my drinking habits then, which are largely weather and temperature based, I suppose, ranging from a lager drink, to a bitter drink, to a cider drink as someone once nearly sang…
In future years, a lot of people will sing the songs that remind them of the better times, before madness took over the world in 2020
The lumping of unjabbed and single jabbed for hospitalisation and death is highly suspicious, particularly given that they have separated them for infection.
In any case, the persistence of discrimination between jabbed and unjabbed for travel in particular when everyone knows the jabs don’t stop infection and even make it more likely shows that nothing has really changed.
The facts and the evidence regarding the COVID have never really mattered. Two years on It is still being used to drive an agenda.
Exactly. And failure doesn’t stop the agenda. Minor speed bumps. Inconveniences and nothing more.
At least we get to experience what mass hysteria looks like.
Lest we forget, this is what it looked like.
They’ll become very sad Clowns as the years roll by and they succumb to diseases they otherwise wouldn’t have had.
But it will be hard for those of us having to watch it happen to those whom we love.
Quite.
I note that the NZ authorities can actually see the underlying data and so could identify the best way to present the summary data to suit their needs…
And, how do they know? I was in hospital recently for 5 days, and swab tested on admission to A+E (threw up on the nurse when she did the throat), but at no stage was I asked about my vaccine status.
It will be linked to your NHS number.
Thanks, amanuensis.
What is the NZ strategy for conducting tests? Are they conducting randomised tests, or just relying on test results reported by the general population and those conducted in hospitals, surgeries etc?
Is there a breakdown of tests by who conducted the test?
That’s a good question.
As far as we can tell, for the general population the testing approach is like the UK ‘only much more enthusiastic’. Healthcare testing is ‘when people walk through the doors’.
Yes. This is it. Now that we have RAT tests in the country (they were unavailable up until recently, but now they’re ubiquitous) people will test themselves if they have a sniffle and are supposed to then report themselves to the authorities. I would say the vast majority are compliant enough to do this. Some more sensible people just self-regulate their actions and stay home or do not visit vulnerable people. I don’t think testing is standard for attendance at the doctor or dentist, but I would imagine that it is for hospital admission. Some workplaces/organisations require daily RAT tests for either just the unjabbed or for all. A lot of it makes absolutely no sense, but so many are still under the spell.
This interesting article is treating all products as if alike. There is no discussion here of different products, Pfizer, AZ etc which might cause variations, There has also been a lot of talk – perhaps not much published – that different countries and different localities are receiving different versions of products particularly Pfizer. This may be a source of different patterns. I am sadly not surprised that the more injected may be faring worse than the less injected – these products were never designed to prevent infection. You only have to look at this article by the BMJ editor in chief from August ‘20 to see that chaos was expected and predicted
https://www.bmj.com/content/370/bmj.m3258
However, everybody changed the story the minute Trump was run out of office. And as Julian points out the products are no longer even against the original alleged virus.
You’re right about the different vaccine types — I could imagine that there are significant differences in outcome between them — however NZ (and nearly everywhere else) doesn’t provide data on this aspect in their data and so analysis is impossible. If we do get data (from anywhere, frankly) that allows this analysis then we’ll almost certainly write about it.
Thanks.
NZ uses Pfizer almost exclusively. There are a tiny number of AZ, and an even smaller number of Novavax.
‘unlike its neighbour Australia, most of its wildlife isn’t planning on killing you at the slightest opportunity’
All depends what you mean by ‘wildlife’. If you count the dictator Jacinda as wildlife then death chances mirror those of the neighbouring penal colony
And all those rumours of the billionaires buying property in NZ to ride out the reset. Doesn’t inspire confidence.
NZ is the new South America.
Perhaps. But best laid plans and all that.
It puts me in mind of Neville Shute’s book, “On The Beach”, where post-nuclear-war, various people are in, or journey to Australia, which is the last place that the fatal nuclear fallout cloud will arrive (and it does, as I recall). I think there was also a film of the book.
Concerning “wildlife”, my experience is that some horses are eager to lay a damaging hoof on you, and are thus potentially as deadly as many other forms.
There was indeed a film, which starred Ava Gardner. She is reported to have said that Australia was a great place to make a film about the end of the world.
Little did she know.
Apparently the guy who has a stake in Spurs FC has been buying up land in Patagonia (Argentina) to build a resort for the Billionaires – preparations are well underway.
Are we expected to believe she is being vaxxed?
Careful now
Maybe, but I’m interested to know what the white, apparently cylindrical object is between her arm and the syringe. My acquaintance with needles in adult life is limited to a tetanus injection some time ago, and I don’t recall any extra equipment of that sort was involved.
Damn, well spotted. People with experience, please comment? It looks like a little box into which the vaccine is being injected, rather than into the arm. Right in front of our eyes.
It looks to me like a plaster that has been half stuck on ready for afterwards, however never seen it done like this before and suspect it may well be there to hide the fact the needle is not actually puncturing the skin.
It is a plaster. In the original video, we were all surprised to see this in place before the needle went in. The nurse closed the plaster over the wound as soon as the needle came out. To confirm my suspicions that is was a set up, the nurse then fluffs around in the background looking for a plaster to put on, as she ordinarily would, then realises it’s already been done!
I told you so.
And lest one forget, that is not all.
One of, if not the biggest elephant in the room, is the damage that mrna has done and will continue to do (until death) to the immune system.
We already know, courtesy of GVB and others, how the immune system has to be trashed to enable the mrna to deliver its toxic spike cargo.
Longer term “alterations” to the immune system are being seen at a bio molecular level with auto immune disease being the inevitable result. GVB and others again.
There’s certainly a risk that we’ve altered the virus’s evolutionary pressure by vaccinating everyone. This would be seen as an increase in covid’s pathogenicity, particularly for younger individuals. I’d imagine that this would come later in the year; if it comes during summer the usual seasonal dip in coronavirus infections (colds) will mask the effect.
Of course, we might not notice anyway because they’re stopping the publication of raw data (including ‘independent’ sources such as Zoe).
One important sign to watch out for is what happens to case rates after this peak — if they don’t fall to ‘very low’ then something’s up.
Why so?
Because it means that immunity following infection is ineffective in the vaccinated.
Immunity following natural infection is broad and covers many aspects of the virus, so even if our immunity isn’t significantly ‘updated’ for new variants on reinfection (ie, OAS) we’re still likely to have some ability to control additional reinfection. However, immunity in the vaccinated is narrow (spike protein), so if we see OAS it will mean that there’s little protection against newer variants.
Tried to explain this to someone today. As they are brainwashed courtesy of UK govt I didn’t get very far.
The really interesting part is that none of this information will make any difference.
The ‘new normal’ dictates that lockdown is good, masks are good, warp speed gene therapy vacccines are double plus good.
The fact that the actual real world evidence shows that all these things cause far more harm than they do good is heresy and will not be tolerated.
People will learn the hard way as they always do.
Morrison of Oz already said it back in Feb 2022.
11.15 on the video, interesting bit at 11.27
“We’re all responsible for our own health…”
https://rumble.com/vv1cfr-super-bowl-not-black-enough-for-the-blm-mob-and-hiv-covid-vaccine-further-e.html
“Very soon”…. how many times have we heard this? When, exactly?
Meanwhile millions of ‘vaccinated’ are flying around the world, getting on with life.
Just look at flightradar24.com
Exactly. It is a cult. Nothing can get in its way. Remember this from our friend Annie:
I’ve always been confused by the apparent success of crude propaganda techniques used in the past — from anti-catholic (or anti-protestant) rumours spread (deliberately) in the 17th and other centuries, to the ‘baby eating German soldiers’ during WWI.
I’m no longer confused. All you have to do is keep telling the population the same thing over and over again and they’ll simply lap it up. You’d think that people would work this out eventually, and that those with a few years under their belt would explain to the young how it works — but that never happens.
It’s actually quite simple: repeat constantly and suppress opposition.
The key to understanding this is look at the source. It is not as simple as repetition.
Credible scientists have hammered the climate agenda for decades with limited effect. They are not understood as authorities.
Covid propaganda originated from authoritative sources. This worked well, as your comment suggests.
The underlying psychology is the recipients need to have faith in authority and, by extension, the hierarchy implied by authority figures. You’ll note the pushbacks against covid initiatives tend to use ridicule not counterargument. That works with the believers because the need to believe authority is driven by comfort, the need for an authority to be in charge. This absolves them of personal responsibility. Painting critics as cranks reinforces this feeling.
I would argue there will be a strong correlation between sceptics on this site and a whole constellation of positive personality traits like conscientiousness, personal responsibility and common sense.
The propaganda worked because it found a receptive audience who need to be told what to do while maintaining the illusion of free choice. They are slaves and they love their slavery. All this nonsensical talk of liberty and freedom is threatening to that world view as it comes with personal responsibility attached.
The underlying psychology is the recipients need to have faith in authority and, by extension, the hierarchy implied by authority figures.
This is what confounds the left/right hypothesis. So many of the left, although they might deny it, put their faith in authorities – of their own, while believing that it’s the right who “worship” hierarchy and obedience.
They imagine that stroppy words about equality render them immune. But once drilled in loyalty to leaders (for the sake of the cause, comrade), they end up losing the habit of questioning narratives.
I would argue there will be a strong correlation between sceptics on this site and a whole constellation of positive personality traits like conscientiousness, personal responsibility and common sense.
I think the sense of and desire for personal responsibility is very important. I resented (and still resent) mightily the removal of my right to exercise personal responsibility for my health, for example.
Perhaps that’s what is behind some of the more angry of the posts here.
When others have the nerve to assume that responsibility for us (you shouldn’t mix with others, so we’ll close down places where you can; you should wear masks, so we’ll order you; you should take a “vaccine”, so we’ll punish you if you don’t), they are not taking care of us.
They are infantilising and dehumanising us. When I try explain to friends why I am enraged by the lockdowns, masks and mandates that don’t bother them at all, I find myself repeating that “it’s up to me” to decide these matters for myself.
The Will Smith incident in the Oscars gives a really interesting glimpse into the human mind in this respect. (The incident was an inconsequential freak show in most respects but incredibly interesting in this one way.)
After the slapping incident, Smith received the award for best actor and was given a standing ovation. So the people in the room in the moment didn’t think his action had merited censure and just carried on as if it wasn’t a big deal.
Fast forward a few days and the academy – basically those same people – decide to ban him for 10 years.
My question to the people in the room who stood up and clapped him and then decided to ban him would be: if they thought he did so terrible a thing as to ban him for a decade, why did they give him a standing ovation?
The answer of course is that they had in the interim been bombarded by a storm of outrage, real or concocted, that informed them that in fact what he did was reprehensible. They had been incapable of reaching that conclusion by themselves, apparently.
In short, people don’t know how to think and act for themselves. They take their cues on how to think and how to act from those around them. Whatever information we are surrounded by is what most of us believe.
I find it striking that ‘toxic masculinity’ has not been brought into this. Smith assaulted another man in ‘defence of his woman’s honour,’ surely a cast-iron case of ‘toxic masculinity’ according to leftist dogma. Who is Smith to ‘defend’ a woman’s ‘honour’?
But no, as far as I can tell, there’s been no sententious moralising in this case.
Funny that.
Not surprising at all. Woke has a hierarchy, and the ethnic origins of the combatants trumps all in today’s America. Does anyone doubt what would happen if a white actor had assaulted Chris Rock?
It is this aspect we must expose and ridicule.
I agree that it is not surprising, but I disagree that ethnicity trumps all in this hierarchy. If that was a conservative black man or woman who directed the joke at a white leftist who adhered to all of the leftist dogmas, and the white leftist did a Smith, they’d largely be celebrated by the Woke for assaulting the black conservative.
Of course, it would be highly unlikely that an openly conservative black man or woman would be invited to host, but just imagine, say, Candace Owens was invited to host alongside Amy Schumer (just so those running the show could get some perverse enjoyment from the scorn Owens would receive from the Woke ‘celebrities’ present). Imagine the ghastly Schumer did her nauseating little dance while chanting ‘Gay, Gay, Gay…’ (as she did that night), and Owens piped up, ‘Actually, you’re misrepresenting DeSantis, but it’s good to know the left still refuses to pay attention.’ Now imagine Schumer slapped Owens for daring to contradict the narrative. I’d bet good money Schumer would get a standing ovation from every Woke fruitcake in that room, including every black Woke fruitcake.
Black conservatives are particularly loathed by black Woke ideologues in America.
You beat me to it Vaxx
Snap! I have been saying exactly this. The people that were defending Smith did so primarily on the grounds that he was standing up for his wife, in and of itself no big deal.
But he made a big drama of it, committed assault, all while she sat there looking on. There is an increasing trend on tv to have some female character or another bleating on about being talked down to, being oppressed, being sidelined by men, not being treated as fully competent. One would indeed have expected that same crowd to now say how insulting Smith was being to his wife, who I do believe is quite confident and perfectly capable of standing up for herself. Her face when Rock made the joke was more whithering than Smith’s slap.
Toxic masculinity here:
https://www.youtube.com/watch?v=Zzpx9VX9hoI
Excellent observation. Herd thinking in action.
In short, people don’t know how to think and act for themselves. They take their cues on how to think and how to act from those around them.
I wish with all my heart that I didn’t agree with you. I have reluctantly come to the same conclusion, after the experiences of the last two years – except that I’d say “most people” (I suspect that’s what you mean).
For what it’s worth, I was amused rather than appalled by Smith’s slap when I got around to seeing it; and wondered whether it was perhaps staged (it’s show-biz, after all). Apparently not.
The “storm of outrage” was predictable. People do love being outraged by individual naughtiness, while being completely relaxed about grotesque authoritarian over-reach. In fact, they end up demanding that over-reach: perhaps to prove their vigilance to those who have the power to ban others.
God, how depressing. I can only hope that at least some of those who gave Smith a standing ovation think the Academy was wrong to issue its ridiculous ban. Having the guts to say so is another matter entirely.
2In short, people don’t know how to think and act for themselves. They take their cues on how to think and how to act from those around them. Whatever information we are surrounded by is what most of us believe.”
I take your point – however I have been surrounded by the same information bombardment as everyone else I know and I have not only not believed it but also won’t act on it. So what is it about me that separates me from the majority who do believe it and who will act in accordance with it?
As for the Will Smith thing – you have to remember that his speech invoked a lot of emotional resonance which would appeal to the artistic (bit woke) community – references to God, the fact that he is a man of colour (BLM) etc etc – there was a lot of virtue signalling going on in that standing ovation.
I think fear is the key.
Fear of the unclean, – so ostracise and quarantine them, plague islands etc.
Fear of the wrath of God, so ostracise and kill unbelievers and develop a system where absolution can be be the only route to salvation.
Fear of Russians with snow on their boots ( a favourite of mine from childhood).
Fear of the Jewish people, to help launch an attempt at world domination.
Frightened people are so easily manipulated as those in power know full well.
Fortunately for the world the above examples were hampered by the lack of a modern MSM.
Unfortunately for us now TRPTB are able to control fear levels by the manipulation of the MSM.
We have to be able to prove, by science that the jabs are harmful in many ways. The likes of GVB are doing this, but sadly to a limited audience.
We have to continue to try and unpick the data to show the jabs are harmful.
I don’t envy the likes of you in being tasked with this but I thank you and others for keeping going.
The truth will out one day. Hopefully before it’s too late.
https://www.reuters.com/business/healthcare-pharmaceuticals/moderna-recalls-thousands-covid-vaccine-doses-2022-04-08/
Of course one reason for the death rate amongst single vaccinated might be that the first shot killed them.
I don’t think this is the case — there’ll be post-jab deaths for each of the doses and so you shouldn’t see a differential effect.
Why does the fat jabber have ‘telly propaganda’ written on the inside of her arm, as she pretends to jab with the cap still on the needle?
You could write war and peace on those bingo wings.
Let’s be frank, that face covering does us all a favour, just not in the way this tinpot tyrant thinks/pretends.
I vote she keeps it on in public at all times, until she ceases to be in public office.
Why is there a great big bung stopping the needle actually going into her arm?
Good question. Perhaps the ‘nurse’s’ arm was supposed to cover that part. But look, you’re focusing on the wrong thing, Tea. Look at the brave leader’s face. She’s smiling. She’s doing this for the greater good. She’s a hero, and she’s being filmed proving she’s a hero. Classic hero stuff. Stop muddying the waters with your pertinent questions. It’s unhelpful, what.
There certainly was plenty of arm flap to cover up the needle stopper. That nurse needs to be held to account.
I hate the photos showing the ‘celebrity’ vaccine recipients smiling.
It is propaganda, designed to make the vaccine hesitant look like they’re scared of the process — ie, the ‘celebrity’ is superior because they’re adult and not scared of such things.
I think it makes them look like morons, because they’re mistakenly thinking that the risk lies in the procedure (there’s zero risk in the procedure itself, the needle, the syringe) rather than the stuff being injected. But I’m in a minority — the majority will still have this sense of superiority because they weren’t scared of the needle.
Good points.
Maybe they should listen to Neil Young’s excellent “The Needle and the Damage Done” – in fact, old Neil could do with having a good listen to what he wrote as well.
On a more serious note, I don’t think they believe for one second that the “vaccine hesitant” are scared of the needle itself, that is merely used as a bullying tactic, trying to shame people into doing something they simply do not want to do by implying they are cowards otherwise. A most childish ploy.
Indeed. Also, since the muddled masses are so malleable, they automatically adopted the same line. Did you notice that? The criminals in power and dumb ‘celebrities’ suggested that the ‘hesitant’ were afraid of needles, and the hypnotised masses once again automatically adopted the same line/tactic and became the regime’s boot boys.
It’s photoshopped, so that people who are sensitive can’t get triggered by the sight of a needle… or something?
Because she’s not actually having it, she knows damn well its a tool of genocide.
At least she was wearing a mask. Meant it hid the teeth.
Well, I hope the long-suffering New Zealanders learn a couple of lessons that these figures seem to indicate:
Firstly, having the jabs does not create an invisible shield of armour around you that the virus cannot penetrate.
Secondly, you appear to be better off having either no jabs at all, or the booster. Having two jabs produces the worst outcomes of all, and by a long way.
Now, for all those still wedded to the idea that they simply must be jabbed at all costs because the alternative (99.9% likelihood of survival) is too dire to contemplate, all they have to do is work out how they get to the booster stage without going through the dangerous two-jab lottery first. Sounds like one of those insoluble conundrums to me. How do you get three jabs without having two jabs first? Answers on a postcard to Saint Jacinda, c/o NZ government. Actually, don’t bother. She knows everything already and won’t be listening.
The main message in the data is that it doesn’t really matter what you do, because for the majority (non vulnerable) the risks of infection are small compared with the other risks we happily live with every day.
More evidence that will be ignored,that those vaccinated are the ones at risk, they are the carriers and spreaders of Covid, so perhaps its the vaccinated that if I were as evil as the heads of Government in the western world, are the ones who should be shut out of society, stopped from having transplants, stopped from travelling, stopped from entering Restaurants, Bars etc, stopped from working. Because its very clear these vaccines are the generators of the disease and the breeding bed for new variants,
My interpretation of the reduction in deaths after jab 3 is that 0ne and two has already finished a number of people off, jab 3 is just polishing the outliers off, 4 will no doubt continue with the cull
I remember reading that the Italian elderly (where covid first struck) had been subject to a new flu vaccine campaign shortly before the pandemic began in Europe.
I wonder if those elderly got a little something special in those vaccines to help get things started?
Maybe they were giver Kinder Surprise eggs in hospitals and their care homes, for a surprise bout of salmonella and death?
https://www.bbc.com/news/business-61041760
I wonder why they would opt to mix the unvaccinated and the single dose vaccinated data for their presentation of hospitalisations?
Ahh, I know, it is because the hospitalisation data for the unvaccinated is truly awful and shows that the vaxxers were right ll along, and because they are worried that the unvaxxed will feel bad they are manipulating the data to make them feel better.
I wonder if the hospitalisations for the unvaccinated would be lower than for the boosted if they were presented as a separate category.
Quite. Unlike the rest of us, the NZ authorities actually have the underlying data, and can choose to summarise the data in a the ways that best suits their needs.
The jabs only work on horses so Jacinda’s safe, unfortunately.
Its because the vaxxines are infecting them.
Has omicron ever caused a case of Covid? I thought it was supposed only to affect the upper respiratory tract if it causes any symptoms at all. So if a person who is infected with omicron gets pneumonia (which means they are likely to be over 70 and already chronically ill), then if SARSCoV2 played a role that will have been some previous variant to omicron, not omicron. No pneumonia, no Covid.
Another thing is the rulers put resources into standardising language for their own purposes, so they can control what kind of questions can get asked. (E.g. “how can we cause less climate change?”) One example is “natural immunity”. This does NOT mean only the ability to produce specialised antibodies against a certain virus or bacterium after having recovered from an infection. It also covers the immune system’s first line of (non-specialised) defence. You have this defence against infections regardless of whether you were ever infected before. Few things about health are more important to know than this. Exercise, iron, vitamin C, etc. – they strengthen this immunity. This is an absolutely crucial part of having “good health”. “Good health” doesn’t mean you buy expensive skiwear or sports clothing. It means many things, but one of the most important is that you have strong immunity against infections. If you’re in good health, you don’t get colds all the time. That there have been no academic papers whatsoever, as far as I’m aware, comparing the relative efficiency against SARSCoV2 of lifestyle and “vaccination” is a strong illustration of the extent to which the government and its bum-sniffing “experts” are taking the p*ss. Far from trying to spread this basic knowledge about public and individual health, they are ignoring it – and if anyone asks the question and derives the obvious conclusion they are in danger of being denounced as a public enemy.
Edit: taking a bird’s eye view, it seems that several years of government and corporate promotion of “flu jabs” has played an important role in “de-skilling” the population where looking after their health properly is concerned.
My understanding is that even with the first variants most people would knock it out before it spread from upper/mid to lower with sufficient virulence. Only those who didnt have a good enough first line defence would allow the virus to spread lower and start with severe problems. I imagine it can still cause lrt problems in the weakest. Early treatment is key as ever, something thats been purposely suppressed from day 1.
Where’s the fun in that, though? More accurately, where’s the money in that line of attack?
I remember reading about the Indians treating people with large doses of vitamin D and zinc. They didn’t have the money for fancy drugs so treated patients based on symptoms. Not a peep in the mainstream. I take occasional joy in recounting these things to the drones around me. Not one of them can believe cheap treatments can tackle the greatest threat since the Black Death
Ive just read the hydroxychloroquine section in RFKs book. Truly disgraceful actions from Fauci and his cabal. Good honest doctors trying to help and save people get demonised while the establishment did nothing except sit waiting for people to get so sick they needed hospital and ventilators, $39000 a pop.
Yep. I do maintain the medical profession has done itself no favours. They revealed a shocking lack of willingness to challenge bad ideas.
Perhaps we can expect a backlash.
It is really weird.
Before 2020 domain experts pretty much all agreed that protection from coronavirus (cold) infections was mediated by the innate (probably NK-cells) and cellular (probably KT-cells), and that antibodies had a relatively minor role to play.
Then along comes covid (and the vaccines) and all of a sudden all that’s spoken of is antibodies.
I think we have to be careful extrapolating from NZ. Is it not likely that the vaccinated are mostly in the cities, exactly the places where you get the young professionals who are so keen to both virtue signalling and have higher anxiety (thanks to MSM and social media) than the more sensible remote populations that are much more used to being self-sufficient and less interested in acquiring a badge for their twitter profile?
with prevalence of Covid higher in the more densely populated areas (I presume) this could explain most of the difference in cases due to the higher concentration of vaccinated in those same areas where rates of infection are highest.
That’s a fair point — but we don’t have data to do analysis by location.
Well done in pulling out these stats from the opaque data the NZ government publishes. But the problem is that they have simply no idea what their case rates are since they totally gave up on their testing regime. Before they ridiculously belatedly introduced voluntary rat testing their case rates were pretty accurate but almost immediately after their case numbers dropped like a stone and are now worse than even semi-educated guesswork relying on self reporting through flakey apps and websites by people who are for many reasons exceeding reluctant and unlikely to do so.
The wonderful Nick Hudson (PANDA) stated that during the pandemic New Zealand banned the import of antibody tests. Can it possibly be true that they denied their population the opportunity to discover existing or acquired immunity?
Yes, it is true.
https://www.health.govt.nz/news-media/media-releases/covid-19-point-care-test-kits
https://www.youtube.com/watch?v=TBInd2v-inE
“Why is Omicron becoming more infectious in highly vaccinated regions?”
‘While those given a booster dose of vaccine seem to have lower levels of hospitalisations than found in the group containing the unvaccinated and those given only one dose of vaccine – as might be expected – the double dosed have significantly higher hospitalisation rates.’
Perhaps they used the same ‘trick’ as was used by the UK data manipulators, only counting booster 14+ days as triple vaccinated, and putting any hospitalisation/deaths of people less than 14 days in the double vaccinated group.
Thus double vaccinated figures are inflated, triple vaccinated reduced.
Boris Johnson the leader of the “Conservative” Party and our Prime Minister is totally oblivious of any statistics like these and those telling us of a 50% increase in cardiac issues in the ‘vaccinated’.
Everything he says is vetted and endorsed by Klaus Schwab, Bill Gates, Zuckerberg ‘Fact Checkers’ and 77 Brigade and his prepared script is as tight as his “drums of perpetual war” over Ukraine! ( Nice little UK/ Ukraine friendship flag badge he is wearing)
I see he has gone to see Zelensky – how appropriate – the two hammy actor/clowns reading from prepared scripts can compare notes! I don’t suppose he will ask him about the False Flag atrocity claims and the little matter of Biowarfare labs
I think the country may have a very large ( and growing) problem of “alienation”.
It seems to me that all this is just a bit of a ‘jolly jape’ for Johnson on his road to seek “riches and fun”.
The normal rules of politics, open debate, serious questioning and even half truth seems totally suspended by his personal “Permanent Emergency”.
Greetings from NZ.
Last year Craig Pardekooper analysed the US VAERS database and found patterns in the data suggesting 1 in every 200 batches of Moderna and Pfizer vaccines are toxic.
https://www.bitchute.com/video/rUZrdrfkJxYF/
https://www.bitchute.com/video/dMeX2F7KpD42/
Recently a friend told me that since January 2022, 3 of his friends had died, and a 4th was in intensive care shortly after receiving Pfizer jabs. The deaths were recorded as “COVID”.
Has one of the toxic batches been distributed in NZ?
I suspect excess death figures for first quarter will be interesting.
You’re reading the data wrong. The statement that “there was a much lower infection rate in the unvaccinated” is false.
The rates shown are per 100,000 population.
The infection rate is not per population. For vaxxed, it is the number of cases amongst vaxxed per total number of people vaxxed. Similarly, for unvaxxed, it is the number of cases amongst unvaxxed per total number of people unvaxxed.
What the graphs show are the the number of cases amongst vaxxed per total number of people. Similarly, for unvaxxed, it is the number of cases amongst unvaxxed per total number of people.
But there are far more people vaxxed than unvaxxed.
So you would expect the graph for the unvaxxed to be lower, because many more people are vaxxed than unvaxxed.
“So you would expect the graph for the unvaxxed to be lower, because many more people are vaxxed than unvaxxed.”
You would only expect this, if the vaccines were have little or no effect on COVID cases, no?
No. You would expect the vaccinated lines in the graph to be above the unvaccinated no matter what the effect of the vaccines. All that shows is that there are more vaccinated people than unvaccinated.
The difference in slope of the lines shows that the vaccine does have a positive effect.
The other thing shown here is that there are a lot of math illiterates on this web site. I’m not a fan of the vaccine, mostly because covid is not a danger to most people, so for most people the vaccine is useless. However, I can see that these graphs are useless and do not show what the author claims they show.
I wonder then whether the author is as mathematically illiterate as you allege the commenters are? I put my hand up to the fact that maths and stats are not something I’m on top of as I might like, notwithstanding a good ‘O’ level from the distant past. But I can read a chart, and have seen multiple reports that point to the same thing, written by supposedly competent statistical analysts. Why is it then, that they all miss the point you make? And it seems that whenever the point being made refers to declining efficacy and or increased hospitalisation, that’s when someone remarks that the author is looking at the data wrong. Are ‘official’ analyses, like we get in New Zealand from the ‘single source of truth’, the ones to be relied upon?
Is it not 100,000 vaccinated people, 100,000 unvaccinated people, total 200,000?
Infections higher in the vaccinated.
How else to explain rising infections in highly vaccinated countries.
Unless of course you think the high infection numbers are solely or mostly down to the unvaccinated?
Apparently pine needle tea helps too. I have some but haven’t been using much as I haven’t been much affected by these symptoms.
Hugh – did you make your own or did you buy it, and if so can you say where? I’m interested.
There’s something missing from this analysis: the definition of ‘unvaccinated’. Is NZ also, as with so many other countries, defining the unvaccinated/vaccinated switch point as 14 days after the second injection? If so, this means that all vaccine injuries arising before 14 days after the second dose are defined as arising in ‘unvaccinated’. Most vaccine injuries arise in the 14 days post injection. Are we looking at yet another covid data fraud? If NZ is defining the vaccinated/unvaccinated switch point as 14 days after the second jab, then this fraudulent definition renders all NZ data as gobbledegook. Calculations relating to NZ covid data are probably about as useful as data calculations relating to the number of Angels who might dance on the head of a pin. This would imply the actual vaccine injury rate is higher than the official data suggest. Lord Denning’s’ 1956 judgement that fraud vitiates everything it touches has particular relevance to New Zealand’s covid data and policy.
There are plenty of people claiming that these differing rates are due to Base Rate Fallacy.
It’s almost like they can’t accept reality.
But what if they are due to base rate fallacy? Can someone who knows what they are talking about please explain, if they aren’t due to base rate fallacy, exactly why? Amanuensis- perhaps you can?
My understanding is:
Take 100,000 vaccinated people
Take 100,000 unvaccinated people
That’s a total of 200,000 people.
Infections are higher in the vaccinated *per 100,000*
Base rate fallacy would be if it’s 100,000 total, a mix of vax and unvax
People are saying “ah, infections in the vaxxed are higher because there are so many more of them”
As we know, the vaccine’s effectiveness wanes over time.
Hence the constant “boosters”
Yes. That makes perfect sense. But the graph at the head of this article does appear to show base rate fallacy, based on the labelling of the Y axis and the title. Am I right?
I don’t know.
Just been having this exact discussion with my wife.
To us the figures only make sense if there are 4 sets of 100000 people and for the “unvaccinated” only 100 are “cases” but for the 2 doses there are approx.400 “cases” at the right side of the graph in the appropriate set.
Is the title on the graph a bit misleading?
Yes. Unless the title and label are wrong, the conclusion from that chart at least, is a base rate fallacy.
The MSM won’tbe able to hide these stats forever. They’re probably working desperately to find a way to blame the unvaccinated.
A mini sampling my two grandsons. The 16 year old took three experimental biologicals and sees no problem with that. When I told him immunity is short lived, he didn’t seem to care. He is applying to Oxford for university education. My 18 year old grandson said, when I asked him if he was aware of what was happening in Shanghai right now “I try not to listen to any negative news that is depressing. How do we know it isn’t propaganda”? He also mentioned the Chinese kids at his uni (Durham) who were born in the Uk mix with the other kiddies, the Chinese from China do not.
Well it is their future, but if it this easy to convince “intelligent” kiddies that these jabs are perfectly safe and effective and that the communist dictatorship is also benign, it won’t be that difficult for the WEF to take over the world once we middle age and oldies are gone. Grateful I won’t be here. The experimental biologicals are working their magic in all western countries.
It is interesting that there is no information on the effects of the different vaccines.
It would perhaps be instructive to know whether there was any significant difference between Pfizer and AZ results.
Can anyone suggest a reason for this?
NZ has used only the Pfizer product for its first and second doses. Other products are now available (AZ, Novavax) but the third shot (for those mandated) needs to be Pfizer as far as I am aware.
A couple of things to maybe also consider in any analysis re the NZ figures: From December 4th (or so, I can’t quite remember the exact date) those who had chosen not to partake in the Pfizer pharmaceutical were excluded from all walks of life other than the supermarket, retail shops which didn’t voluntarily exclude them, and medical/dental care. Council premises, funerals and weddings with over 25 people attending, cafes, restaurants, hairdressers, beauty & massage therapy, libraries, swimming pools, zoos, places of employment – the list goes on and on. We have only just been given permission to once again be considered something other than walking bundles of contagion, although many places still do. So much for the utterly illogical & “2 + 2 = 5” clarion call from our Dear Leader “We have to protect the vaccinated from the unvaccinated”. Even Michael Baker, our thorn-in-the side “expert” claimed that this exclusion was nothing more than a “nudge” to get people jabbed and would do nothing to prevent transmission. It will be interesting to examine the stats now that we have been “allowed out”. Another statistic which requires further analysis – as I think it does in many countries – is the “hospitalisation” figure. Here in NZ the definition of “hospitalisation” is 3 or more hours on hospital premises following first being seen by a doctor/nurse practitioner. It does not necessarily mean an overnight stay. Someone could be “admitted” and “discharged” in the same day and still be considered a “hospitalisation”.
In all these studies it seems odd not to specify out the vaccines used. I was given Astra Zenica twice and then boosted with Pfizer. The above charts could indicate that the effectiveness of the ‘booster’ dose could be related to the vaccine given. The vaccines are so significantly different to each other, it would not be surprising if they had different patterns of effects, so surely they should be analysed separately?
Maybe you should have kept checking. The sources you linked show that 96% of over-12s were at least partially vaccinated in New Zealand as of February 2022, which has since increased to 96.4%. That leaves about 151,000 people over-12 who are unvaccinated.
Since August 2021 there have been 35,152 infections in unvaccinated over-12s, which is an infection rate of around 23%.
Something is very wrong with the way you have interpreted the data.
The New South Wales Health Dept publish Covid stats daily, breaking it down into 0-4 jabs and age groups !!
Can’t for the life of me ork out why !!
Twits !!
Check it out for yourself at https://www.health.nsw.gov.au/news/Pages/2022-nsw-health.aspx