
This is the sixth of the weekly round-ups of Covid vaccine safety reports and news compiled by a group of medical doctors who are monitoring developments but prefer to remain anonymous in the current climate (find the fifth one here). By no means is this part of an effort to generate alarm about the vaccines or dissuade anyone from getting inoculated. It should be read in conjunction with Lockdown Sceptics‘ other posts on vaccines, which include both encouraging and not so encouraging developments. At Lockdown Sceptics we report all news about the vaccines whether positive or negative and give no one advice about whether they should or should not take them. Unlike with lockdowns, we are neither pro-vaccine nor anti-vaccine; we see our job as to report the facts, not advocate for or against a particular policy. The vaccine technology is novel and the vaccines have not yet fully completed their trials, which is why they’re in use under temporary and not full market authorisation. This has been done on account of the emergency situation and the trial data was largely encouraging on both efficacy and safety. For a summary of that data, see this preamble to the Government’s page on the Yellow Card reporting system. (Dr Tess Lawrie recently wrote an open letter to Dr June Raine, head of the MHRA, arguing that: “The MHRA now has more than enough evidence on the Yellow Card system to declare the COVID-19 vaccines unsafe for use in humans“, a claim that has been “fact checked” here.) We publish information and opinion to inform public debate and help readers reach their own conclusions about what is best for them, based on the available data.
- Dr Robert Malone, the inventor of mRNA and DNA vaccine technology, has expressed concern about the safety profile of the current Covid vaccines and the censorship of discussing the issues, and called for them to be properly investigated as a matter of urgency. See also his appearance on Bret Weinstein’s podcast (deleted from YouTube) along with Steve Kirsch, who has written of his concerns about the vaccines here.
- The UKMFA has written an open letter objecting to a report on BBC Newsround (a children’s television news programme) by Professor Devi Sridhar, Chair of Global Public Health at the University of Edinburgh, about vaccine efficacy and safety.
- Researchers at RCSI have published a study in the Journal of Thrombosis and Haemostasis in which they show that COVID-19 patients had higher levels of pro-clotting VWF molecules and lower levels of the anti-clotting ADAMTS13. This has yet to be applied to clots in vaccinated patients but may have implications.
- A study in the British Journal of Ophthalmology noted the occurrence of corneal transplant rejection after vaccination with COVID-19 mRNA vaccines.
- In Public Health England’s latest Variants of Concern Technical Briefing, the fully vaccinated have a 0.64% chance of death after testing positive for the Delta Variant whereas unvaccinated individuals have a 0.096% chance of death – a seventh of the risk. However, this is likely to be primarily a result of the much younger age profile of the unvaccinated.
- Dr. Diego Rubinowicz, a Urologist in Palm Beach County Hospital, has observed increased PSA levels in vaccinated men, leading to possible misdiagnosis of prostate cancers.
- EudraVigilance – the equivalent of the Yellow Card reporting system in the EU – has logged reports claiming 15,472 people have died and 1,654,407 have suffered injuries following receipt of the Covid vaccines in the EU.
- VAERS – the American version of the Yellow Card reporting system – released new data on June 11th bringing the total to 358,379 reports of adverse events following Covid vaccines, including 5,993 deaths and 29,871 serious injuries between December 14th 2020 and June 11th 2021.
- Suspected adverse events in the U.K. as reported in the media: Vanessa Newton (45); Lucy Taberer (47); Sophia Gomes (43).
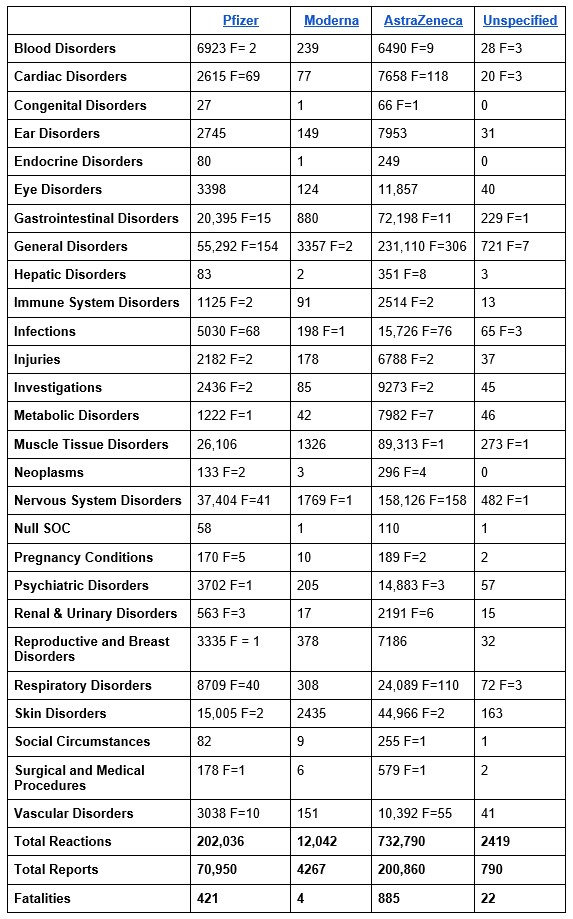
Summary of Adverse Events UK
According to an updated report published on June 17th (covering the period up to June 9th), the MHRA Yellow Card reporting system has recorded a total of 949,287 events, based on 276,867 reports. The total number of fatalities reported is 1,332.
- Pfizer (15.6 million first doses, 10.8 million second doses) now has one Yellow Card in 372 doses, 2.9 adverse reactions (i.e., symptoms) per card.
- AstraZeneca (24.6 million first doses, 17.7 million second doses) has one Yellow Card in 211 doses, 3.6 adverse reactions per card.
- Moderna (0.56 million first doses) has one Yellow Card in 130 doses, 2.8 adverse reactions per card.
Key events analysis:
- Acute Cardiac Events = 10,370
- Anaphylaxis = 1,130
- Herpes = 3,276
- Headaches = 95,316
- Migraine = 8,803
- Blindness – 46 (Pfizer) + 229 (AZ) + 1 (Moderna) + 3 (Unknown) = 279
- Spontaneous Abortions = 201 + 10 (still birth)
- Vomiting = 13,102
- Facial Paralysis incl. Bell’s Palsy = 1,157
- Face Swelling = 1,439
- Disturbances in Consciousness = 12,726
- Strokes and CNS haemorrhages = 2,006
- Guillain Barre Syndrome = 336
- Dizziness = 28,349
- Tremor = 10,180
- Thrombosis & Embolism (All types) = 5,146
- Pulmonary Embolism – 246 (Pfizer), 1236 (AZ), 3 (Moderna), 5 (Unknown)
- Deep Vein Thrombosis – 156 (Pfizer), 928 (AZ), 1 (Moderna), 6 (Unknown)
- Nosebleeds = 2,455
- Seizures = 2,214
- Paralysis = 804
- Haemorrhage (All types) = 4,229
- Reproductive/Breast = 10,931












To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
“The MHRA analyzed the data and confirmed that the benefit of the COVID-19 vaccines “far outweigh any currently known side effects”.”
In other words: “Trust Us”.
Funny, I’m finding trust in the authorities is in remarkably short supply, after over a year of outright dishonest fearmongering, exaggeration of covid risks, suppression of dissent, and covert psychological manipulation.
They have only themselves to blame.
Absolutely – my sentiments exactly.
I mean, while politicians and governments have always bent the truth in the past this is now very different – this has become a pathological form of lying where the lies are now stretching and even exceeding the limits of believability.
The MHRA that receives funding from the Gates Foundation.
Just wait til they start giving mix and match booster jabs in autumn. Based on the adverse events data we already have, how can anyone think this is a good idea?!
These articles would be much better if you took that fence post out of your arse…
You are spot on – the entire rationale of this site is highly informed evidence based information which has shown the entire so-called pandemic to be spurious – ie PCR test based cases and doubtful cause of deaths – at the very least it turns out not to have been an emergency’… therefore why do we need to approve experimental and obviously dangerous vaccines to healthy people? (Oh and why not use readily available now proven effective products on the sick?)
Sorry for being dense but what does that mean?
Ever heard of sitting on a fence?
Ah right -I would sit astride the fence not on top of a protruding fence post.
First case of postmortem study in a vaccinated patient. SARS-CoV-2 found in lungs, heart, kidney and cerebrum and more. Patient did not have typical covID symptoms, tested negative at first, but positive shortly before death. It has been suggested that if you simply have covID it should not be found in multiple organs. https://www.sciencedirect.com/science/article/pii/S1201971221003647
Worth a read. The last couple of paragraphs in it before “conflicts of interest” are quite dry, but in effect, they don’t fully understand the risks to the recipient. Logically, the ‘vaccine’ itself actually caused the death – although it doesn’t actually say so.
Incidentally, it does demonstrate that those ‘vaccines’ that use polyethylene glycol (PEG) are not confined to the muscle injected to; it spreads everywhere.
Yes confirms that PEG ‘protects’ the spike from the immune system long enough for it to get everywhere, including the blood/brain tissue barrier. then the immune system spots it and goes into overdrive, blood clots and haemorrhages occur as the spike ‘factories’ are in operation.
This can create immediate problems, including death. But any future contact with a ‘wild’ virus , possibly any coronavirus not only SARS2, can send the immune system into self-destruct mode.
Quite insane. We are as children meddling (generally and routinely) with fundamentally massive potentials for harm/good. We may have fairly decent brains, but lacking in wisdom, we are a danger to ourselves – and everything we touch.
It is incredible really, how we have escaped utterly annihilating ourselves thus far.
Isn’t this the “pulmonary immunopathy” referred to in this article?
https://pubmed.ncbi.nlm.nih.gov/22536382/
As I understand it, it refers to a dangerous induced over-activity of the immune system, where the cure mechanism becomes toxic.
Is that a new introduction?
Whatever prompted that…..?
It was inevitable as the adverse events and deaths pile up.
Maybe it’s time to discuss the biology of what happens when you inject these spike protein generating Nonsterilising inoculations into people….
It’s all just a ‘coincidence’…
https://www.google.co.uk/amp/s/news.sky.com/story/amp/changes-to-periods-after-covid-vaccine-could-be-coincidental-gynaecologists-say-12338043
Are you suffering from “propaganda disorder?”.
Classic!
“…trial data largely encouraging…” Not true!
The vaccine trial data is incomplete.
Proper trials have been abandoned. We have mass vaccination without control group or follow up. Adverse reactions are swept under the rug.
No true emergency ever existed. Patients were denied effective treatment.
People have been mislead and coerced into getting the shots.
The shots are harming and killing people in the short term. No one knows what the long term effects will be.
About time LS took a stand.
“Proper trials have been abandoned”
Precisely. Of course, there can never be absolute certainty over safety, but the accepted norms of safety trialing were there for a purpose.
There has been no proper debate over whether these norms should be adjusted. No analysis of the overall picture relating to medicine testing. This current abandonment of the framework has been done on the hoof – an a whim – driven by a highly suspicious set of motivations.
Coercing people into an insufficiently tested concoction is against all international norms and ethical rules.
Arguably we are the trial group – personally looking forward to the thinning of the herd, I might be able to finally afford to buy a house in London.
I imagine the reason LS is looking at both sides is so that it is seen to act in an impartial way. This way, those who are not yet seeing the reality are more likely to read it rather than thinking that it is all ‘ conspiracy’.
I heard Dr Tess Lawrie being interviewed on Omar Khan’s Uncommon Wisdom last week ( please listen if you haven’t already) and her comment was that however horrendous the truth is, you have to be as bland and unemotional as possible to get your commentary across, otherwise you are dismissed as being over-reactionary.
A side effect well known from flu vaccination, exactly this, below, has happened to a 92 year old family member after the second pfizer dose:
‘We report a severe “flare” of PMR in a 70-year-old patient after receiving the adjuvanted trivalent influenza vaccine.’
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7002008/
Copious literature bleats that the risks from covid are greater than the vaccine risks.
In fact, the risks from covid are the same as the risks from the common cold. Overall all cause mortality is plumb normal (see attached chart) for the year.
There are over 160 other identified common cold viruses for which there is no vaccine.
The protection given by covid vaccination for the elderly and infirm is consequently extremely limited, far outweighed by the health risks incurred from the vaccination.
The penalty of not having the vaccination?…..to be ‘stuck’ in arguably the finest country in the world….you know…..the one everyone is trying to get into……
Tricky decision……or not really……..
(With thanks once again to the author of the chart – brilliant!)
Well described, but who did they start dishing it out to? Oh, the ‘elderly and infirm’, and observe what went onto their death certificates earlier this year…..
What I don’t understand about this chart is how the author derived it from the ONS Monthly Mortality Analysis. The required data isn’t in the data set. I am not saying the chart is wrong but I would like to understand how he/she created it.
(I made this comment when Tim used this chart before, but too late to get a response)
It’s easy enough to calculate it if you have the raw data by age. If you’re starting from scratch, you’d need the age profile of the UK population by year and then apply the EU standardised age profile (2013) to calculate the age appropriate adjustment.
Many ‘data geeks’ already have the previous data and just update each month or so.
Yes – but to reconstruct it for May to May you need to have the deaths by age for each month. That data is not in ONS Monthly Mortality Analysis and I am not sure where it is available.
Go to
https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/datasets/monthlymortalityanalysisenglandandwales
Download the spreadsheet
(choose the latest May 2021 download)
Go to the ‘table 1’ tab
Go to the people column
The rate per 100,000 column are the monthly figures since 2001
Combine the June 2020 to May 2021 (inc of both) data to get the year to May 2021 figure
Combine similarly for other years
Create a chart from the answers
Thanks but I am familiar with that spreadsheet. The trouble is the monthly rates are not broken down by age. So you can’t get May to May broken down by age. So you can’t do age standardisation.
The monthly figures above are the age standardised figures. The age standardisation has already been done by the ONS.
Table 1: Age-standardised mortality rates by sex, deaths registered in January 2001 to May 2021, England
It’s not May to May as that would be 13 months, it’s June to May!
But you can’t just take the age standardised rate for each month and average them to get the age standardised rate for the year. That’s a fallacy. You have to get the actual deaths for age group for the period you are talking about and then do the standardisation operation for the period.
Of course you can average them. Any error is trivial.
Thanks. This is a really good update.
The thing that winds me up about the vaccine enthusiasts is not their belief that it will get us out of lockdown – though I feel this is misguided- nor their desire to do it for others.
No it’s the way they arrogantly assert the vaccine is safe.
If they just said they were taking a chance, I wouldn’t mind.
As an aside, Devi Sridhar’s comment about vaccines being safe for children really winds me up.
This woman is so smug I honestly cannot stand her.
Anyone who is now advocating that vaccines are safe for anyone but most of all children, should have to face the law at some point soon.
Is it just me or does that ‘Factcheck’ from Health Feedback read like bullshit? Where is the proof that MHRA are investigating ANYTHING. I seem tp remember 2 sisters interviewed on UK Column whose father passed away suddenly stating that MHRA took weeks to acknowledge their concern and when they finally did said that they would have to review autopsy results (of course there was no autopsy) before reaching a conclusion. I wouldn’t trust the MHRA or June Raine as far as I could throw them.
“…the fully vaccinated have a 0.64% chance of death after testing positive for the Delta Variant whereas unvaccinated individuals have a 0.096% chance of death – a seventh of the risk. However, this is likely to be primarily a result of the much younger age profile of the unvaccinated.”
Note the eagerness (see the last sentence) to find benevolent alternative explanation here.
How often does the reverse occur when some unscientific conclusion about the marvellous efficacy of the ‘vaccines’ is stated?
Tells me the young don’t need their “help” then…..
If you look at the Steve Kirsch video “Are Covid-19 Vaccines Safe and Effective“, one of the things he looks at are unexplained deaths. It’s beyond me to dice the ONS mortality figures in the same way he did for the US ones, but I think it’s still instructive to take a look at this year’s figures and compare them to last year’s. If you look at these, two age groups have significantly more deaths this year than last for the first 21 weeks of the year. The 45-64 age group had an increase of 848 in 33,012 lost in 2021, The 15-44 age group had an increase of 679 in 7034. This latter is much more anomalous as its over two and a half times the standard deviation of mortality in this age group for the same week range in the years between 2010 and 2019 inclusive. Something odd is going on here. Now, of course this may be missed cancer and heart treatments causing this, or indeed the ‘Indian variant’, The ONS does report higher deaths for Covid in this age group in the first 21 weeks of this year, namely 773 as opposed to 485. However that still leaves 391 excess losses that cannot be down to the new variant, even if all the Covid deaths are due to Covid. What has caused this increase in mortality? Now I’ll repeat the important mantra, “Correlation does not imply causation”. However, given that the main article tells us that 1332 deaths have been reported through the Yellow Card data for the entire population these excess deaths this year compared to last mean that at the very least, the vaccination programme has a case to answer.
“Now, of course this may be missed cancer and heart treatments causing this, or indeed the ‘Indian variant’, The ONS does report higher deaths for Covid in this age group in the first 21 weeks of this year, namely 773 as opposed to 485.”
Is it not a little early for missed cancer treatment deaths to be showing up? I mean, those with such very aggressive cancers probably would mostly have died anyway, I’d guess.
Some extra deaths from other untreated conditions would be reasonable in this age bracket, I suppose. But of course as Kendrick points out, a lot of common clotting-related harms (strokes, heart attacks, deep vein thrombosis, pulmonary emboli) will be indistinguishable, except in long term statistical hindsight, from vaccine caused deaths:
COVID19 – the spike protein and blood clotting
As for supposed higher deaths from covid, it seems likely these could as easily be vaccine deaths as covid. And is there really any justification for believing any of the variants have higher death rates in younger groups? Is there any way to untangle those from vaccine deaths, and is anybody trying to do so?
Just a random observation about medicine safety.
Today I picked up my (substantial) monthly prescription. It also included one new medication :
Compare and contrast with the process of experimentally pumping foreign genetic material into the population at large.
‘Nuff said, I think.