
The following is a guest post from Lockdown Sceptics’ in-house doctor, formerly a senior medic in the NHS.
In early November, Patrick Vallance and Chris Whitty were summoned before the House of Commons Science and Technology Committee and questioned about their presentation of data to justify a second lockdown. Following their appearance, the government was obliged to ‘correct’ a number of misleading graphics which portrayed the situation as being far more serious than it actually was. The Government was officially criticised by the U.K. statistics watchdog for the misleading presentation.
After last night’s Downing Street press conference I expect Greg Clark, the Committee Chair, will be scheduling a repeat appointment.
Professor Whitty’s presentation was a blatant example of data selection. At the risk of image overload, I will run through a few points he made and quite a few more that he somehow overlooked. This is by no means a comprehensive critique – to be frank, I don’t have time and I doubt the readers have the patience to go through all the egregious errors and data manipulation that went on last night. We will have to leave that to the Science and Technology Committee.
Let’s start with hospital admissions. The official slides measure admissions per 100K population. Here it is, showing an alarming rise in admissions in the North West of England in Graph One.
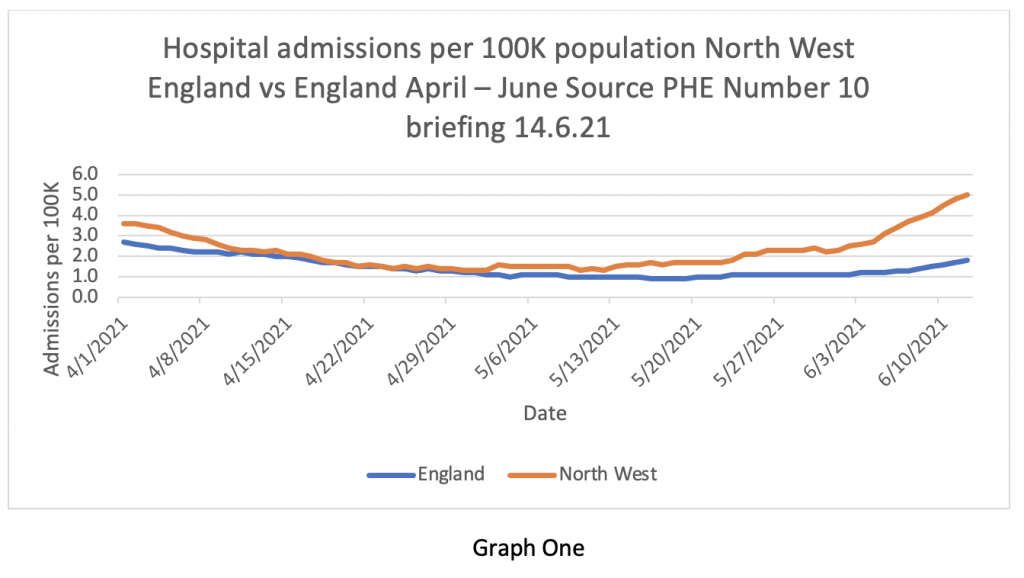
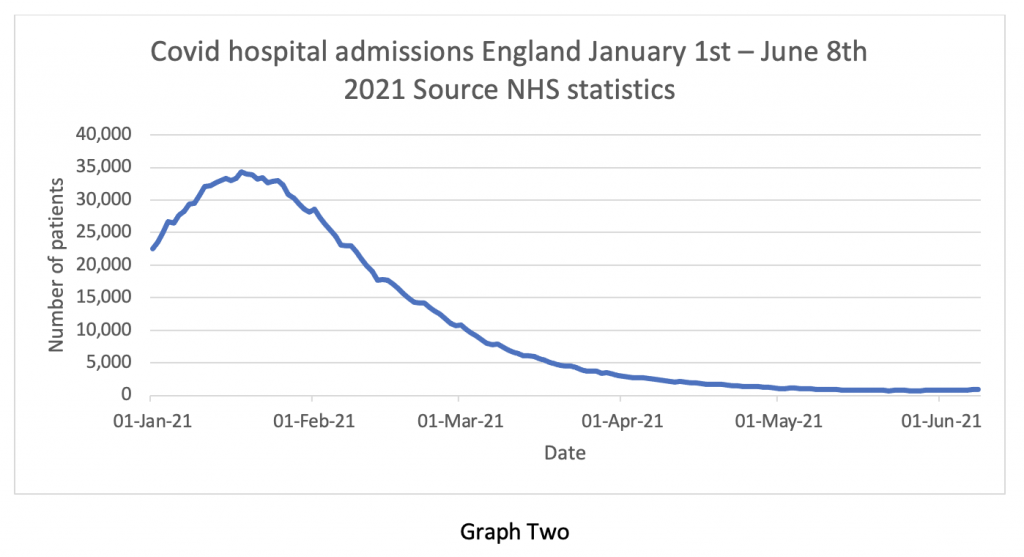
But Graph Two puts that ‘alarming rise in admissions’ into context – it’s so tiny one can’t actually see it. This is a classic statistical trick – altering the ‘y axis’ scale to imply a greater increase and altering the ‘x axis’ only to show the bit of data that supports the hypothesis and deliberately to exclude data points that refute it. For some reason, the following contextual graphic didn’t make it into the briefing pack.
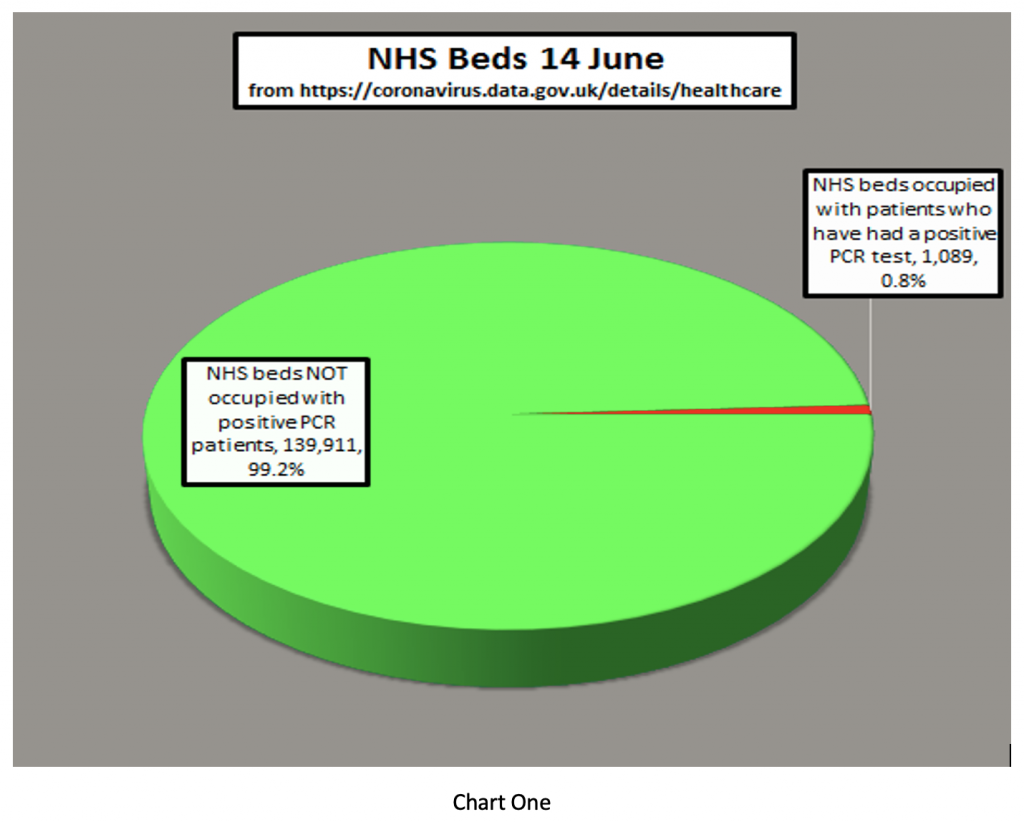
Next, the Prime Minister said that “the doubling of patients being hospitalised is very concerning for the Government”. It isn’t clear to me where he got the information that the number of patients being hospitalised has doubled – I can’t find it anywhere. I wonder whether number 10 might find Chart One useful. It shows the number of COVID patients in hospital vs the total NHS inpatient load. At present, less than 1% of inpatients in NHS beds are occupied by patients who’ve tested positive for COVID-19. In fact, there are 1079 patients and 1257 hospitals – we literally have more hospitals than patients.
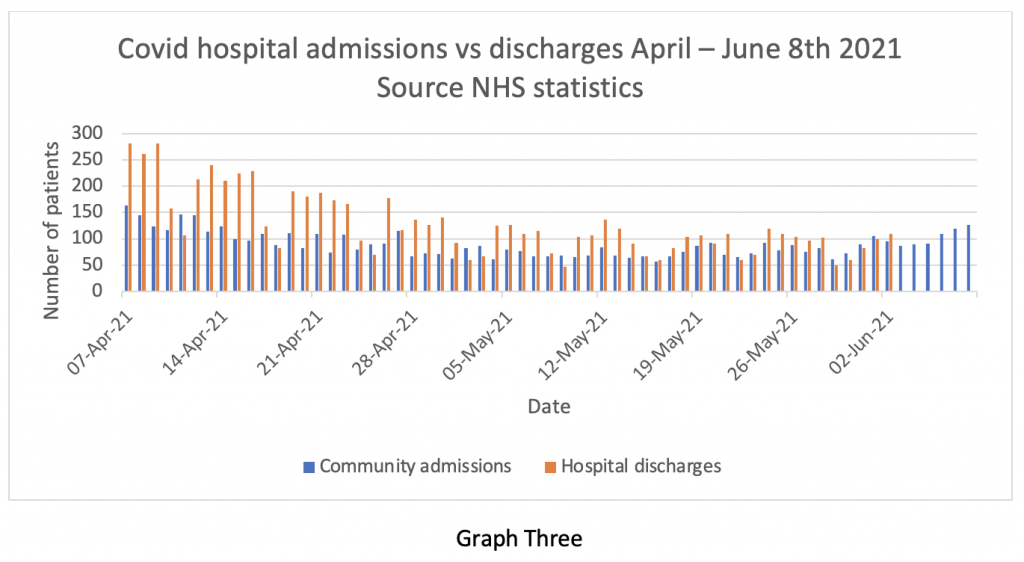
Of course, stating the number of admissions to hospital can also give the wrong impression if it isn’t balanced against the number of discharges. The NHS does not release discharge information very often, but we do have it up to the beginning of June – admissions and discharges are compared in Graph Three (blue for admissions, yellow for discharges). Clearly, admissions and discharges are pretty much in balance at the end of May and beginning of June. Earlier in the series, discharges exceeded admissions, despite the warnings of catastrophe from SAGE about the re-opening of pubs and schools.
What this graph means is that the total inpatient load on the NHS is virtually static at about 1% of capacity – patients are going out as fast as they are coming in. So, where’s the problem?
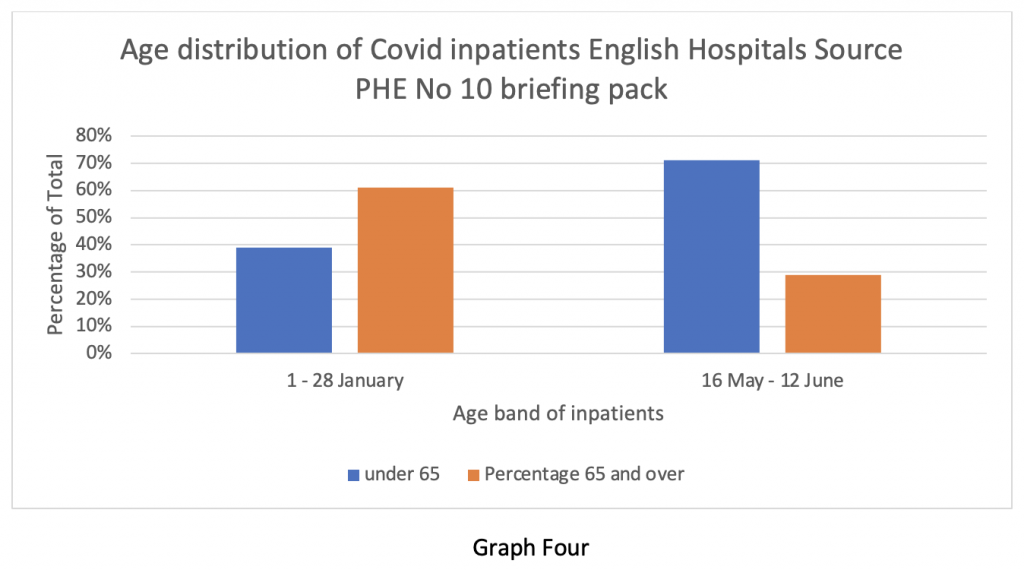
Professor Whitty did show a slide illustrating the percentage change in the age profile of patients admitted to hospital. Here it is in Graph Four. It shows the effectiveness of the vaccine in keeping older people out of hospital. But it implies that there are larger numbers of younger people being admitted instead.
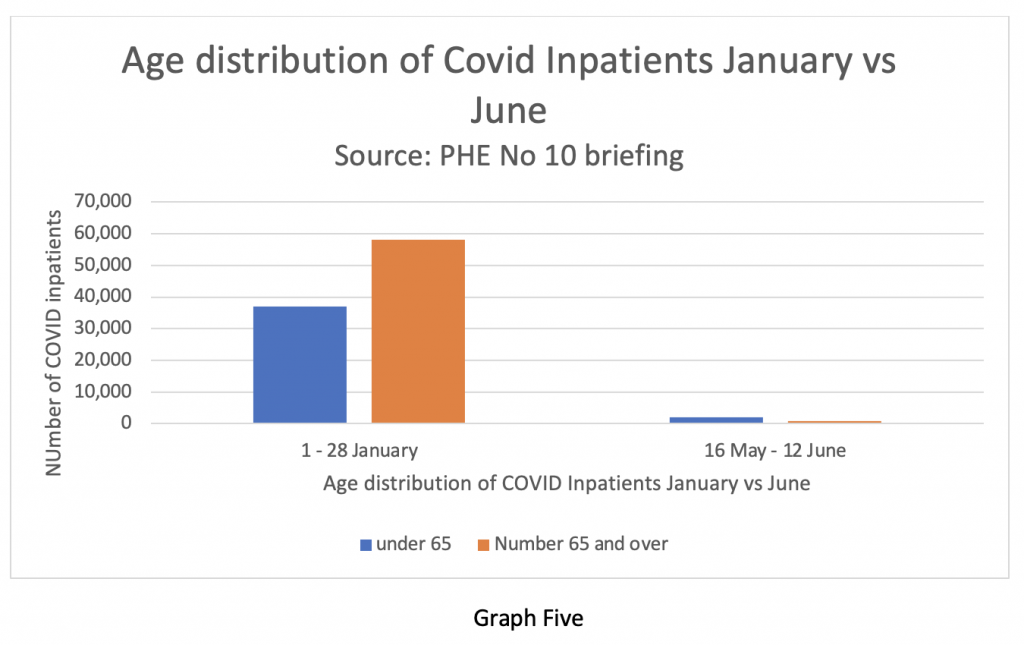
But when we look at the absolute numbers, we see the data presented in Graph Five. It shows the overall absolute numbers admitted now as a tiny fraction of those in January. Another classic statistical trick.
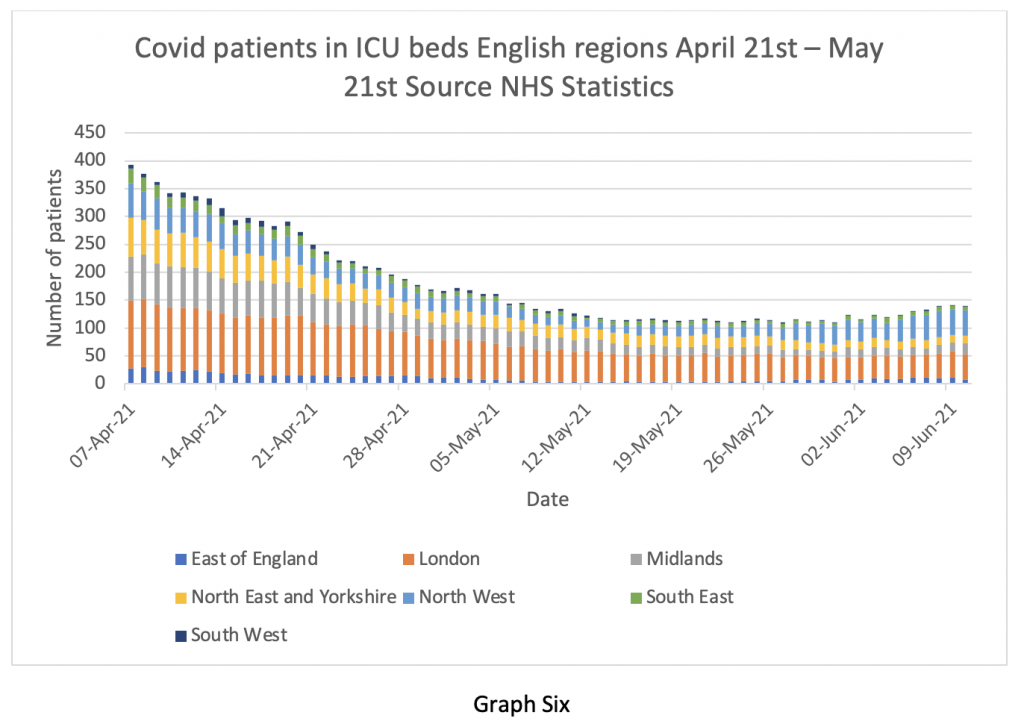
Of course, how seriously ill the patients are makes a big difference to outcome. Graph Six shows the number of COVID patients in ICU up to June 10th. There has been a tiny increase in the number of ICU cases in the last two weeks – arguably statistically insignificant, but we are well below the numbers from six weeks ago. I wonder why Professor Whitty forgot to mention this?
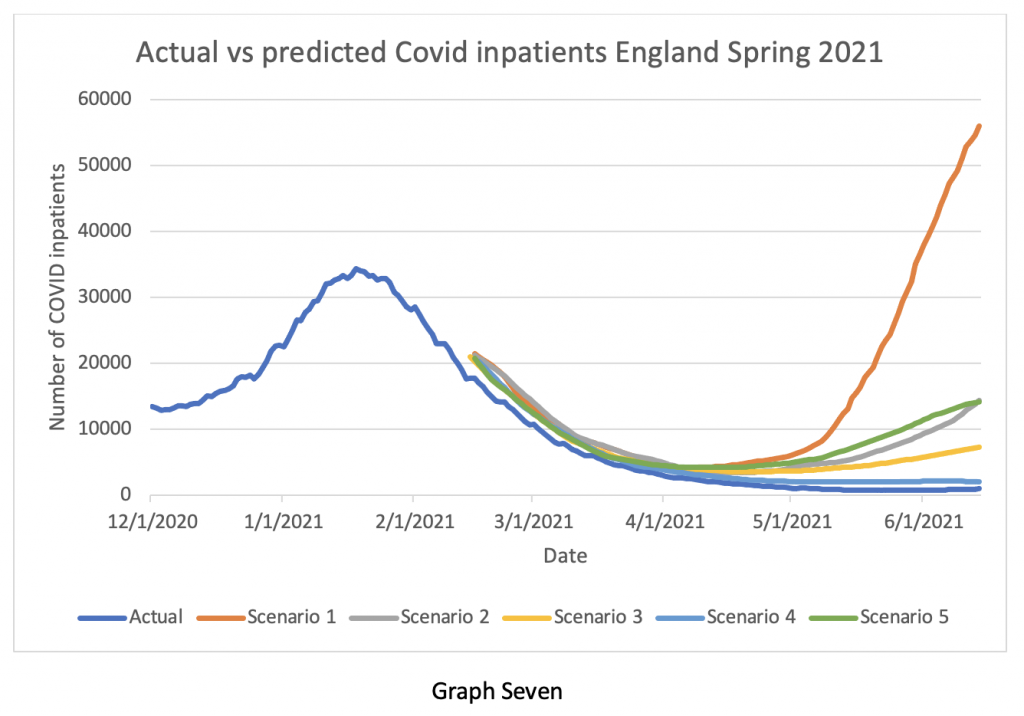
Much was made of the possibility of the situation with the Delta variant getting out of control and there being an ‘exponential rise’ in cases – I think I’ve heard that before somewhere. So, Graph Seven compares what actually happened (the lower blue line), with what the modellers from Imperial, Warwick and others predicted would happen in April and May. Look at the vertical axis – the predicted numbers of patients by the various modellers were out by factors ranging from Eight times to 50 times. The closest prediction still said we would have twice as many inpatients at the beginning of June than we actually have. Given this astonishingly inaccurate performance, why does Professor Whitty continue to have confidence in the modellers? And why does the Government continue to believe him?
And at the risk of boring the readers with official documentation, I came across a briefing note dated June 3rd 2020 from SPI-M-O, one of the acronym salad committees advising the Government.
Point 26 is interesting:
Analysis based on CO-CIN data indicated that as of 1st May, 30% of positive tests in hospital were linked to hospital acquired infection, including those in up to the fourth generation of transmission following discharge. Since then, as the number of cases in hospital have decreased, the proportion of infections that are hospital associated has increased, and was approximately 80% as of the 1st June. These estimates are preliminary and dependent on modelling assumptions used. SPI-M-O consensus statement June 3rd 2020.
To be frank, I’m still not quite sure if that can be true – do they really mean that 80% of the hospital inpatient load acquired Covid while in hospital for other reasons? Regular readers will recall I have frequently drawn attention to the (officially denied) high incidence of nosocomial infections, but I have never seen an estimate as high as 80% before. I think someone in authority needs to examine that statement and the raw data behind it very carefully and explain it to the public. It’s such a shocking number.
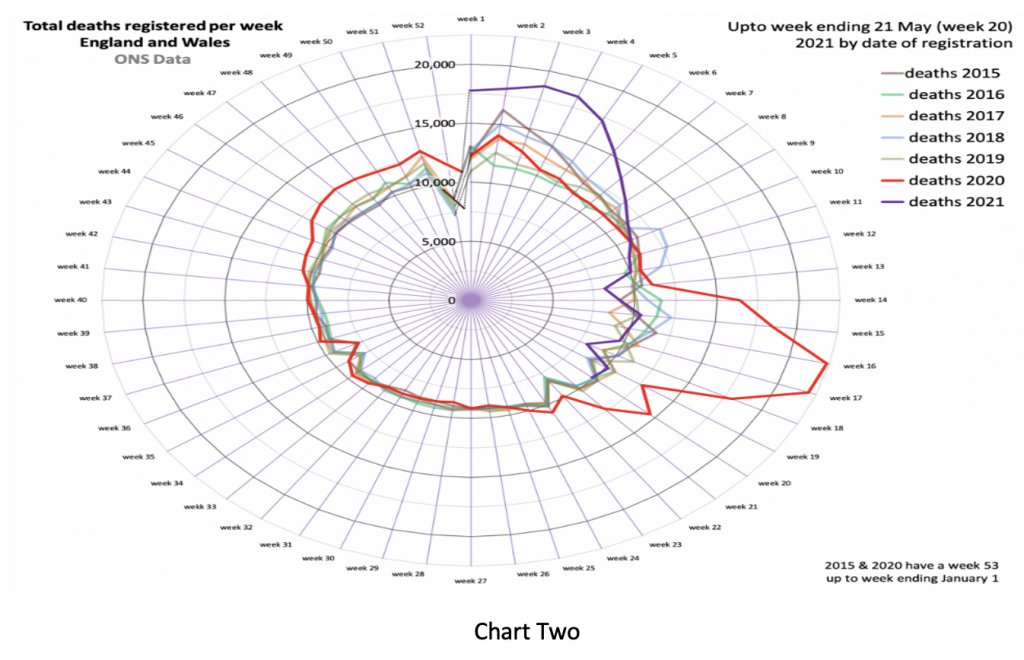
Next, we look at deaths. Here is my favourite Nightingale graphic, courtesy of Professor Carl Heneghan’s team at the Oxford Centre for Evidence-Based Medicine. The purple line shows overall deaths in England and Wales being below the five-year average up until the end of May.
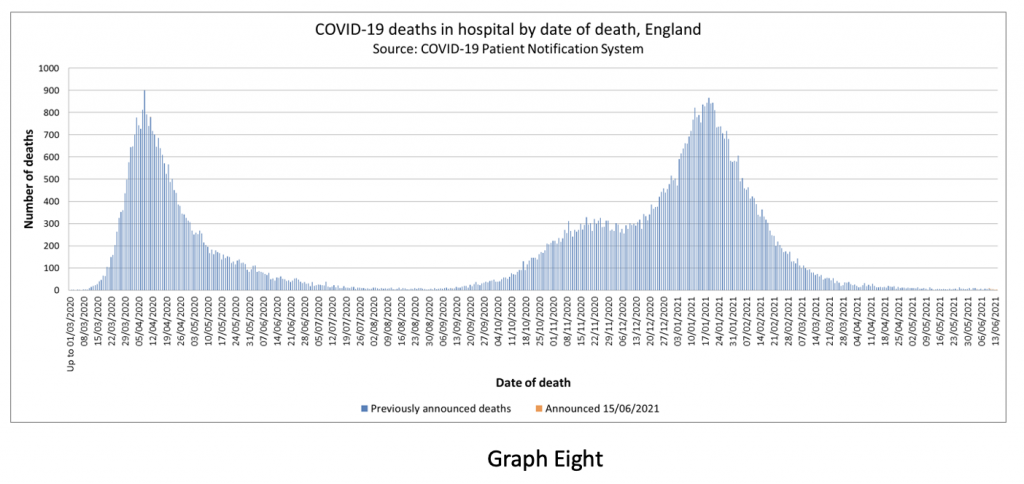
Of course, there is clearly a lag between infections, hospitalisations and deaths, so Graph Eight shows the overall Covid mortality. Can you see the worrying rise in Covid-related deaths in the last two weeks? No? Well, I can’t see it either – because it isn’t there.
The statistical tricks and data selection on display last night should be obvious to a junior medical student. They cannot be an accident or oversight. What really bothers me is just how blatant and amateurish this trickery is. It implies the Government is aware the deception will be seen through in an instant by anyone familiar with the whole picture – but doesn’t care.
The WHO still recommends that lockdowns or other societal restrictions are used as an intervention of last resort – when there is literally no other option left to prevent health services from being overwhelmed. There were occasions in the last 12 months where a reasonable case could be made to support short lockdowns. We are quite clearly not in that position at the moment.
My concern about the current situation is not just the manipulation of health data for political reasons (although that is certainly worrying), but that societal restrictions are now being viewed as a normal tool for the Government and ‘our NHS’ to use whenever they see fit – these are lockdowns of convenience, not of necessity. If the British public does not wake up and stop this behaviour, then it will continue ad infinitum.
I end with a fairly lengthy quote from Michael Gove talking in 2003 about identity cards in a Newsnight discussion:
It’s not the case that the state can demand of me certain things, those who exercise power, exercise power at my, your and David’s pleasure. Ultimately the important thing to recognise is that we as free citizens devolve power upwards – we don’t operate at the licence or leisure or pleasure of those who happen to govern us at any given point… I just have an a priori preference for limiting the powers of the state at any given time, because the general rule over the whole of human history is that once powers are yielded to the state at moments of crisis or emergency it is never the case… that the state hands them back.
I couldn’t put it any better than that.
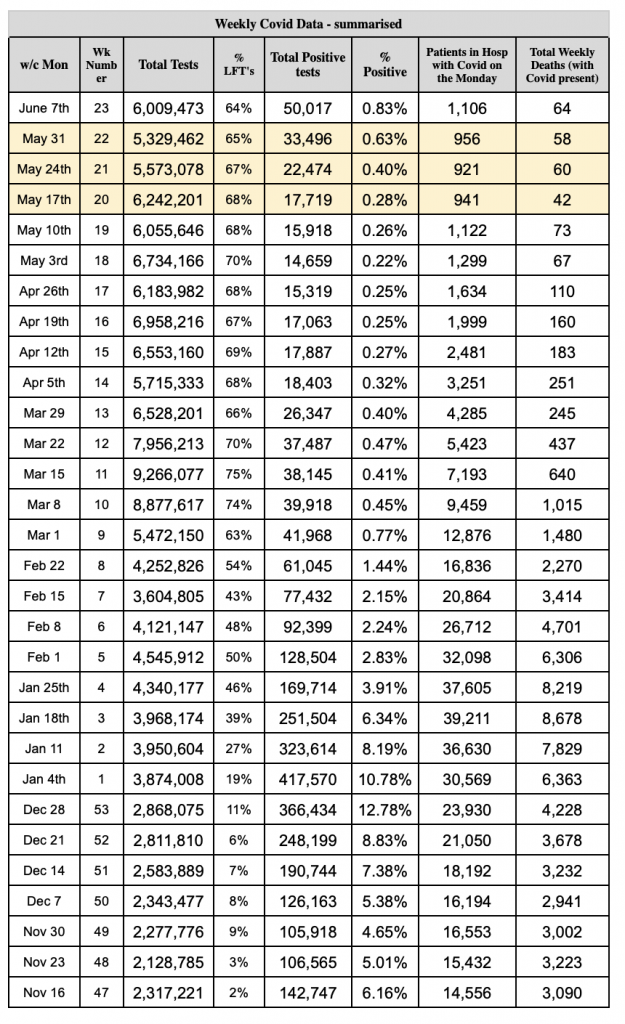
Stop Press: A reader has helpfully put together a data table showing the total number of tests, the number of positive test results, the percentage of positives, the number of patients in hospital who’ve tested positive and the total weekly deaths. As you can see, the latter two numbers are fairly flat.












To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
Referendum Fails? Or was it carried out and delivered the result the citizens wanted, rather than acting as a rubber stamp for the politicians? I guess there are all sorts of failure modes, which would result in the outcome being null and void, but return an unexpected result is not a failure.
This can only be good news if we can trust the democratic process to deliver the will of the people.
My principle concern is that although our elected representatives are ostensibly ‘populist’ those who enact government policy in the civil service, the uniformed services, the education and health systems and local government are all staffed by ‘graduates’ of the Gramscian Common Purpose organisation. They have won the ‘culture’ inside our public bodies which have become manifestly Culturally Marxist. Unless government can take a broom to the upper echelons of these organisations and get any Common Purpose graduate to reapply for their job, nothing will ever change at the ballot box.
I am sure every nation has its own equivalent to Common Purpose acting as the vanguard for the Long March through the Institutions.
Principal not principle. 😠
Good news.
Most people understand that the Eco Fascism is what it is – the end of our civilisation.
Notice the disconnect between the hoi polloi, the Wat Tylers, and the elite, the plutocrats, the pharma-ments, the useless Churches and the Richard II’s.
Surely if you mean rhyming slang, you mean Richard III’s of which Bill Gates is the biggest and smelliest
Just to be clear – a narrow majority of those who voted were in favour of bringing forward the target from 2045 to 2030. The referendum failed because the turnout was far too low.
Indeed it was 50.9% in favour https://de.wikipedia.org/wiki/Volksentscheid_Berlin_2030_klimaneutral and they weren’t so very far short of their quorum either, some fear propaganda might nudge the result over next time.
Absolutely. This result won’t stop the Davos climate train. They’ll look at it as a problem to fix before continuing full steam ahead.
Time is not on the elite’s side.
The more time passes, the more people realise what net zero actually means in practice.
100% of the FFF and det Luischen supporters in Berlin voted Yes. This meant 442,210 yes votes. Almost as much (423,418, just 4% less) voted No. In total, this means 18.2% of the population voted Yes, 17.4% of the population voted No and 64.4% didn’t bother (rounded to one decimal place). A sensible referendum law, ie, one designed such that it’s not susceptible to activist minority groups whose members are more motivated to vote than the general population, would either require a significant majority of the actual electorate, at least 65% – 75%, or count the non-voters as opposed to whatever change was proposed.
A sensible referendum law, ie, one designed such that it’s not susceptible to activist minority groups whose members are more motivated to vote than the general population, would either require a significant majority of the actual electorate, at least 65% – 75%, or count the non-voters as opposed to whatever change was proposed.
What a pity we didn’t have such a ruling for the Brexit referendum.
That’s something I thought at that time as well: Majority in the range of measurement error, probably partially caused by bad weather in London. Considering that this turned me into an illegal alien overnight, ie, someone whose legally gained so-called permanent right of residence was withdrawn and that I then had to re-apply for it which was a seriously unnerving process, I think I had (and have) a right to see things in this way.
I don’t think you can claim the same for you.
“I think I had (and have) a right to see things in this way.
I don’t think you can claim the same for you.
Are you saying because the referendum did not affect my status I have no right to see the problems with it?
I’m saying two things:
1) You’re barking up the wrong tree. I’m legally resident in the UK. This doesn’t mean I had any voice in this (while pretty much everyone else on this planet — every citizen of a commonwealth country who was legally in the UK at that time — had).
2) I have a right to be critical of this procedure because it negatively affected me despite I had no voice in the decision (also stripped away my right to vote in local elections). Unless you’re either British or legally resident in the UK, it’s really none of your business.
Plus an additional one: The Brexit discussion is over. Time to move on to more current affairs.
We didn’t have a vote before joining, therefore membership was undemocratic (and unconstitutional, as was pointed out to Heath), so leaving without any vote at all would have been democratically perfectly acceptable.
We would then need a massive “yes” vote in order to democratically rejoin. Except it would still be unconstitutional.
The shock on hearing the result exhibited by remainers like Johnson -he only pretended to be a leaver because he knew the majority of Tory party members were and he was thinking about his leadership hopes – tells us that the vote was rigged, but they screwed up by not rigging it enough. I don’t just mean rigged in the sense that millions of foreigners were allowed to vote, or that Jo Cox was murdered by the intelligence services in a not-quite-successful-enough attempt to swing the vote (they should have picked a far more sympathetic MP)
The ‘foreigners’ allowed to vote here were those who had nothing to lose and everything to gain from the referendum outcome being what it indeed became and whose immigration numbers have since skyrocketed. This was even not so covertly marketed as such: Stop white people from continental Europe coming here and throw the ones who already came, based on trusting that what they were told would be the law governing this was actually a law under a bus, so that more global majority people can come to the UK instead.
Or the devolution votes in Scotland and Wales. Devolution in Wales went ahead based on a Referendum vote which won on a majority of around 6,700 votes (less than 0.5% of the vote).
Yep!, and look where devolution has got us.
This loss, tactical or not, will be used to galvanise the Blue Hair anti life nutters.
On a parallel theme, with elections coming up in the UK, is there a place / website where you can buy T-shirts, badges etc with pithy sceptical slogans? (I wonder if even the manufacturers / distributors of these items have there own sort of D notices on them – I’m deeply suspicious that no campaign of a ribbon or lapel badge or personal adornment of some sort has emerged to signal general libertarian / sceptical / pro CO2 inclinations.
Perhaps it’s an area Bob Moran could get into. Simple t-shirt merch? I say this as an early doors customer for one of his fantastic hoodies with the demonic child injector on it – if anyone remembers that one!
So, anywhere to buy decent protest merch, anybody?!? I do think like the Lincoln Green of Robin Hood we should be able to identify each other (and I know there are many sub variants of resistance not unlike LGB etc.) on the streets. Surprised it hasn’t happened.
If you look on ebay you will find plenty of sellers who will print or embroider items of clothing such as caps, t-shirts, hoodies, sweatshirts with your own message.
I have a “Bollox to Lockdown” t-shirt which I ordered off eBay in April 2020 – family not amused.
I also have a couple of embroidered polo shirts:
No
SD
Covid 1984
The Covid 1984 is very attractive.
This is good news.
All government is by consent in the end, and when people withdraw their consent en mass, there’s nothing the government can do about it.
Even tyrants like Ceaușescu don’t last long once the people decide they aren’t having any more of it.
Governments ignore the populace and press on regardless with their agenda. Who voted for uncontrolled immigration or Netzero?
Look at what happen after the Brexit vote, even today we have not left properly and with not so subtle moves now to keep us aligned and eventually rejoin.
I do wish us British had some French passion.
An interesting referendum, in that it looks as if the percentage of the voting population required to go forward with the change was just 24%. Many aspiring politicians would love a voting system that gets them into power on that basis. Others might call it… well, loaded.
They might want “no part of it” but like the rest of the wealthy western world they are going to get it anyway. Tyranny does not ask you politely to accept it. But remember, most people who think they agree with NET ZERO because they think there is some kind of climate change crisis underway only think that because their mainstream News Channels are feeding them evidence free garbage in support of the political agenda of Sustainable Development. If there was a totally neutral assessment presented to the people of the politics, science, morality and social aspects of the climate issue those people would certainly have a much different point of view. ——–Propaganda works and that is why government and it’s bought and paid for media use it so extensively.
There has to be something to celebrate
First Friday Freedom Drinks
Please contact directly regarding food
Friday 7th April 7pm
Oakingham Belle
Oak Avenue (Junction A329 London Rd)
Wokingham
RG40 1LH
If you take the majority as the difference between those who agree and those who don’t it is 0.0425% almost the same as the proportion of CO2 in our atmosphere. Apart from the fact that the human contribution to this has a minimal impact on our climate, CO2 is essential for life and plant crops would grow better with more of it. Real scientists who are not tainted by financial support from those benefitting from the nett zero craziness know this and report it, but their reports are not broadcast by mainstream media and it is necessary for intelligent people to search for it to find the truth. Perhaps the Germans are better than our people at finding it.
I’m not sure it can be described as a resounding rejection when 82% didn’t bother to vote.
It looks more like a resounding result for apathy….. or possibly a resounding result for “it won’t make any difference if I vote NO since the Globalist Eco Nutters will ignore a vote they don’t like.”
The globalists will see a majority of 1 as approval.
Yep! and a loss to one vote, or any result they did not want as a wrong result and must be overturned. See various EU referendum results these last couple of decades and the subsequent reactions..