The symptoms attributed to tarantism, a traditional syndrome allegedly caused by tarantula bites, include ‘anxieties’, ‘anguish’, ‘extreme restlessness’, ‘inner unease’ or ‘melancholy’, as described by the 18th century physician Francisco Xavier Cid, but also hanging upside down from trees in imitation of spiders, lying in tombs, throwing yourself into wells, wearing red dresses, handling swords and obsessively looking at themselves in the mirror. Other common symptoms, such as loss of consciousness, convulsions, lack of control, aggression and delusions, make atarantados behave similarly to those possessed by demons or the victims of evil spells, according to witchcraft historian Maria Tausiet.
The syndrome takes its name from southern Italy, probably from the city of Taranto, where the Mediterranean Tarantola (Ischcolus) is still found today, but it appears in other parts of Europe, as evidenced by the ‘Dancing Epidemic of 1518’ in Strasbourg, which affected hundreds of people, or the Spanish Tarantism itself, with its own characteristics – whose casuistry extended into Alto Aragon, as well as in southern Italy, until the twentieth century.
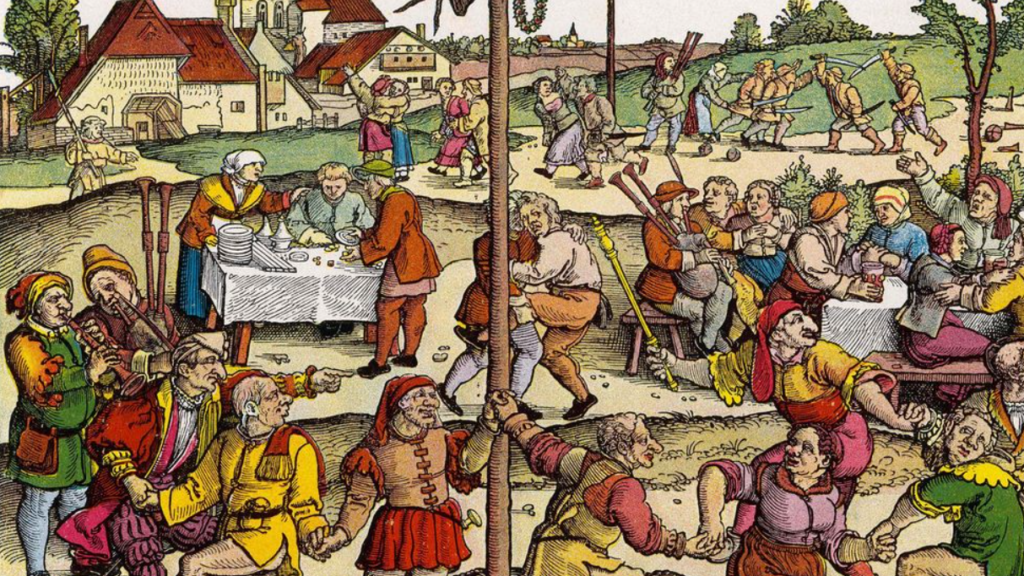
The exuberance of the symptoms, together with the surprising effectiveness of the symbolic ‘cure’ – that is, the fact that the performance of the Italian tarantella, or the Alto Aragonese jota, often in the midst of joyful community rituals, served as musical therapy for the distress of the ‘stung’ – aroused the scepticism of doctors and theologians, with the Church’s attitude oscillating between different degrees of integration and tolerance.
But were there really enough tarantulas to cause so many ‘cases’? Even if some of the cases were due to real bites and the probable effects of latrodectism – caused by the black widow spider (Latrodectus mactans) and not by the tarantula (Lycosa tarantulae), whose bite is rarely serious – toxicology cannot explain the syndrome. It does not follow that the syndrome was a mere invention. Tausiet herself points to the essentially social and cultural nature of the phenomenon, closer to ‘culture-bound syndromes’ and sociogenic syndromes than to the enlightened biomedical paradigm:
The spider bite, with all the ceremonies aimed at combating it, would therefore be a system for reconfiguring certain personal difficulties in such a way that the conflictive psychic contents, instead of manifesting themselves as individual neuroses without a horizon, could be modelled on a symbolic plane, within the mythical-ritual framework of community life.
Hystories: the social spider’s web
It would be a great mistake to assume that the modern extinction of tarantism, or of the picturesque – to us moderns – medieval epidemics of dancers, is simply the end of sociogenic illness and the disorders formerly known as neurasthenic or hysterical. Post-traditional society, with its new avenues for digital information and (dis)information, the empowerment of ‘civil society’ and the fragmentation of medical authority, seems to multiply the opportunities for the flourishing of ‘medically unexplained diseases’ in recent decades. According to Abigail A. Dumes from the University of Michigan:
What was understood as neurasthenia from the mid-19th to early 20th century came to be understood as hypoglycaemia in the 1960s, Briquet’s syndrome in the 1970s, chronic fatigue syndrome in the 1980s, and, by the late 1980s and early 1990s, multiple chemical sensitivity, Gulf War syndrome and chronic Lyme disease, among others.
For Elaine Showalter, the feminist scholar and medical historian, these are ‘hystories’, epidemics of post-Freudian hysteria. Modern syndromes would be characterised by the expression of individual and social stress, powerlessness and physical or sensory symptoms without clinical explanation, but often attributed – by patients and activist doctors – to an unidentified external cause. The new ‘tarantula bites’ range from physical candidates such as viruses, environmental toxins, products of Big Pharma, electromagnetic waves or chemical warfare, to such fantastic agents as satanic conspiracies, in the case of the false memory syndrome, or extra-terrestrial infiltration, in the case of ‘abduction syndrome’. The ‘hystories’ – for Showalter – have three basic ingredients: “a doctor, or other authority to define, name and publicise a disorder; unhappy patients with vague symptoms; and a supportive cultural environment”, starting with the USA itself, the “hot zone of psychogenic illnesses” and the true genesis of the new biomedical labels.
Initially, patients are people with a bewildering set of troubling symptoms and a wide range of possible explanations. Once they see their problems reflected in a prototype, they come to believe that the laws of a disorder describe their lives, and seek the aid of a therapist, some patients rewrite their personal narratives. They may become addicted to their symptoms, and embark on the career of being a particular kind of patient, one with chronic fatigue syndrome, gulf war syndrome or multiple personality. For some, the patient career may be a permanent way of life, with a self-supporting network of friends, activities, doctors and treatments.
Not surprisingly, Showalter’s work is met with hostility and, in some cases, efforts to get her cancelled by some patients, associations and doctors who interpret it as an attempt to delegitimise the suffering of those affected. This scepticism is symptomatic of our materialistic zeitgeist, which privileges ‘physical’ explanations of ill health and is progressively averse to psychological and cultural ones. However, Showalter’s contribution is relevant, as it underlines the importance of historical, social and cultural determinants of health, and adequately describes the danger of a biomedical misdiagnosis, overdiagnosis or even iatrogenic diagnosis, capable of creating itself and/or perpetuating the alleged symptoms.
A sociogenic virus
Maleness is a known risk factor when it comes to the severity of COVID-19 disease, a finding consistent with the idea of the male as the ‘sicker sex’, although this ‘sex disparity’ may also be due to social determinants, such as the fact that men are more likely to work in occupations associated with a higher risk of COVID-19 mortality. Although no major sex differences are observed in the proportion of infected women and men, male patients are three times more likely to be admitted to intensive care units, and are also more likely to die from SARS-CoV-2 coronavirus. In light of these data, it seems a sexual paradox that Long Covid, defined by the WHO as “an illness occurring in individuals with a history of probable or confirmed SARS-CoV-2 infection, usually three months after onset, with symptoms lasting at least two months that cannot be explained by an alternative diagnosis”, affects more women by a ratio of four to one.
One explanation for this paradox could be that the disease is either biogenic, psychogenic/sociogenic or a combination of the two.
The biogenic theory is that Long Covid is similar to other post-infectious syndromes caused by viruses, such as Chikungunya, Malaria or Epstein-Barr, which researchers link to immune activation and cognitive impairment apparently found in clinical syndromes such as myalgic encephalomyelitis (or fibromyalgia) or chronic fatigue. The sex difference in Long Covid, from this perspective, could be due to a presumed greater natural female vulnerability to autoimmune and central nervous system syndromes. According to López León and colleagues, “it is tempting to speculate that SARS-CoV-2 may be added to the viral agent’s list causing ME/CFS” (Myalgic encephalomyelitis and chronic fatigue syndrome).
A second theory points to the psychogenic and sociogenic origin of Long Covid. From this perspective, the sex difference in Long Covid could be due to women’s higher risk for disorders such as depression or post-traumatic stress, probably mediated by the sex difference in neuroticism and also between countries, and other factors.
A recent study based on a sample of 27,000 French patients shows that the explanation for the 18 persistent symptoms (with the exception of anosmia) is not the tarantula bite, i.e., serology (testing positive), but the belief of the patients that they’ve contracted the infection, which points to the need for medical evaluation of patients with suspected Long Covid “to prevent symptoms of other diseases from being wrongly attributed”. This peculiarity of Long Covid is consistent with an earlier study in young patients.
In fact, the studies that support a biogenic explanation yeild results that are compatible with the alternative hypothesis when controlling for symptoms common to psycho-sociogenic disorders. The five most common symptoms of Long Covid, for example, according to the study by Lopez Leon and colleagues cited above, are fatigue, headache, attention disorder, hair loss and dyspnoea. These are compatible with disorders such as depression, trauma, anxiety and somatic disorders. Comparing symptoms associated with “mass psychogenic illness” and Long Covid, there is an almost perfect overlap. Both include: fatigue, breathing difficulties, headache, abdominal pain, sore throat, cough, memory and concentration problems (‘brain fog’), anxiety and depression, diarrhoea or rash (HT). Similarly, it is now known that Long Covid is associated with a higher risk of post-traumatic stress disorder, which is an additional risk factor for developing so-called somatic symptom disorders.
Contrary to initial estimates, the percentage of patients reporting symptoms 12 weeks after contracting COVID-19 disease is estimated to be between 2.3% and 2.5%, according to respective analyses by Nature Medicine and the British ONS (which may even be an overestimate, as the studies assume that patients accurately report their symptoms) and most sufferers, even if they receive intensive care, make a good recovery according to an Italian study. More to the point, in children Long Covid turns out to be “rare and mainly of short duration”, according to a study of 37,000 children.
The overestimations could be partly due, as Noah Carl points out, to the alarm generated by the media and by some medical authorities about the consequences of Covid. “People may have been inclined to exaggerate their symptoms, and to report things they would not normally have reported,” says Carl. In other words, even if Long covid is in part a biogenic disease, which is an entirely reasonable assumption, the socio psychological and even cultural determinants of this important health issue cannot be ruled out.
Eduardo Zugasti is a philosopher and political adviser. English translation courtesy of Dr. Robert E. Whitley.












