
Net migration hit a record high of nearly one million in 2023, 170,000 more than previously thought, in an extraordinary indictment of the Tories’ post-Brexit record on ‘cutting immigration’. The Telegraph has more.
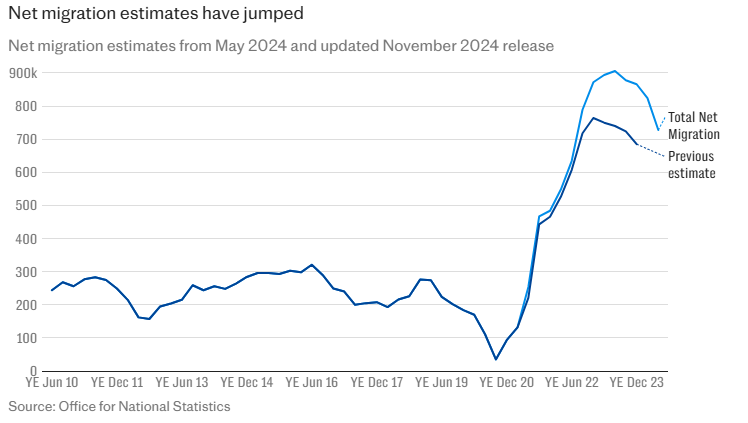
The number of people entering the U.K. minus those leaving reached 906,000 in the year ending June 2023, according to updated estimates from the Office for National Statistics (ONS). This has been revised upwards from a previous estimate of 740,000.
The net migration record was formerly thought to be 764,000 for the year ending December 2022. This estimate has also been revised and now stands at 872,000.
However, the most recent figures show that net migration is falling and is down by 20% to 728,000 for the year ending June 2024. This is the fourth highest net migration total on record.
The revised estimates come as separate Home Office figures showed government spending on asylum in the UK stood at a record £5.38 billion in 2023-24, up 36% from £3.95 billion in 2022-23.
The recent decline covers the year before the election when the Tories cracked down on migration, with measures including bans on foreign workers and students bringing dependants, increases in the skilled worker salary threshold from £26,200 to £38,700 and curbing shortage occupation visa schemes.
The ONS said the total for the year to June 2023 had been revised upwards by 166,000 from the initial estimate of 740,000 because of more data becoming available.
It reported that better analysis of the number of refugees from Ukraine and improved information on the migration behaviour of people arriving from outside the EU had also impacted estimates. …
The ONS said that while remaining high by “historic standards”, net migration is now “beginning to fall” in the wake of the measures introduced at the beginning of this year.
Non-EU nationals accounted for 86% – just over one million – of the 1.2 million people who entered the country in the year to June 2024. EU nationals made up 10% or 116,000, and returning Britons accounted for 5%.
Of the 479,000 people who left the U.K. in the year ending June 2024, around 44% – 211,000 – were EU nationals and 39% or 189,000 were from non-EU countries. Some 16%, or 79,000 were Britons.
More than a million people entering the country each year – no wonder there are queues for everything and the NHS is overrun.
Worth reading in full.











To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
There’s no risk to me from Covid at all. So why would I take any of them?
The MHRA keep saying the benefits outweigh the risks, but that is completely different for different age groups. Where is their age based risk analysis?
there’s is a massive risk to me from all sorts of things I do. so what? I have no intention of living forever. But I’m not a lunatic. I’m not taking an emergency licensed drug with very early (and will only get worse) safety data. If other people do, that’s fine with me. It won’t be the last time that people inject drugs to make themselves feel better in the short term
“I have no intention of living forever. “
… and I bet they won’t devote every f.ing TV and radio channel to your demise like they’ve done for Phil the Greek
you never know!
Nah, Steve – Even you aren’t going to get the absurdity that has descended in broadcasting for Phil the Greek. I just put on the box (‘Now’, I assumed ‘the Royal arse-licking will be over’) But, f. me – it’s continuous celebration (?) wall-to-wall crapology – as if this guy had some suprnatural significance.
I mean … I thought that the Covid propaganda was absurd – but, even if of a shorter duration – this tops anything so far.
Which brings us to the realization that it’s part of the same propaganda mind-set in its necrophiliac drooling.
“ I just put on the box” – I just found the problem
Essentially, you’re putting your finger on a key issue (see my post) : the deceptiveness of looking at relative rather than absolute risk.
Oldest scam in the pharma book.
It is impossible to do an age based risk analysis or indeed any risk analysis because we do not have any long-term data. The risk of VIPIT clots is the minimum risk that we currently know of, it will only increase as more of the apparent vaccine deaths get assigned (like the strokes and heart attacks that are being hidden), whereas the risks of batflu will only decrease (like with all viruses).
Yes that’s what will happen. The medium to long term effects of these vaccines will likely prove catastrophic for those who have been foolish enough to have bared their arms for Bill Gates’s toxic special brews. As such, they won’t be able to risk a large contingent of unbelievers getting on with their business, while the vaccinated are dropping like flies. So we must be ready for yet more ludicrous lies, to back up their campaign to take out those, who don’t fancy an early trip to the grave.
While it doesn’t help to be very old and ill, the main risk of dying from Covid is having a history of flu vaccination. Hence we see the age profile of those who suffer worst.
I absolutely agree. Why anyone who is outside of any sort of ‘risk’ category would voluntarily take the vaccine I have no idea.
But then again as i am in a ‘risk’ category i STILL would be reluctant to have any of the vaccines.
Who the hell determines ‘risk’ anyway? Should that not be up to the individual anyway?
‘potential harms’ should read ‘potential harms as known currently’
Exactly. It’s not even ‘known’ a few months down the line how these treatments are going to pan out, never mind in years to come! Although I have my suspicions…The trials don’t even finish until next year or the year after. And worryingly many serious ADRs are are being reported via the Yellow Card scheme but this reporting is being ignored by the MSM.
I would suspect most vaccine candidates never make it – certainly no mRNA ones have. So its a statistical likelihood that these vaccines will be withdrawn at some point in the future. The idea that ‘short term risks’ = ‘risks’ makes me want to take up smoking
Correct. For a vaccine entering Ph3 studies (so has passed earlier stages where a neutralising antibody response and also possibly a T cell response are see, and there are no giant safety red flags) Probability of Success is about 50-60pct.
Passing the earlier stage (proof of concept) is I think, from memory, about 20pct POS.
The interesting data is in the benefits column – not the ‘harms’.
These risk charts only include the rare blot clots and a few outliers SOFAR.
They do not incorporate what’s still possibly gonna happen in that area and with regard to ADE, infertility, brain diseases through nanoparticles, cancer through mRNA etc..
And the benefit charts are blown up by the from/with Covid manipulation.
In short: for anyone healthy under the age of 80, it’s objectively a negative risk/benefit ratio and on top of that in essence like playing Russian roulette for many, many years to come.
If you still fancy it or see it differently, by all means get the shot.
But shut up if you get sick and only blame yourself then.
And finally start to respect the decision of the people who come to a different conclusion and stop coercing, threatening or calling for discrimination against them!
The severe adverse reactions to all the vaccines, are way higher than the blood clotting. It’s clear to anybody who bothers to read the data as it emerges around the world, that the risk/benefit window is only reached for the old and vulnerable.
Problem then becomes if they’re too vulnerable, they can’t cope with even small side effects.
I think this is quite clear, and if a normal development timeline with lots of animal testing had been followed, I’m not sure any of these vaccine candidates would have entered the clinic (ie been put into people)
“He made his comments as Matt Hancock, the Health Secretary, stressed that the benefits “spectacularly outweigh the risks” for those in their 40s. …”
I’m in my 60s and to all intents and purposes, I have no chance of being admitted to ITU ‘with Covid ((whatever that is) right now. That is a downright lie or in polito-speak ‘economical with the truth. This is well people,stringed with symptomatic respiratory disease stringed to admissions stringed to ITU admissions. Then compared with an injection from which you gain no benefit but quantifiable harm. Stats have already shown the disconnect between these groups which I note they are gradually admitting through gritted teeth. I don’t understand how he can get away with this. It Is A Lie. Shameful. Blatant.
This is the Trolley/Train Track Dilemma. If you jab a thousand people under 40, you know that say 1 will die. If you don’t jab a thousand people under 40 you may fail to extend an 80 year old’s life by 6 months or you may. How can doctors stand by their professional oath and do this, setting aside the Nuremberg principle and all the unknowns. It beggars belief.
“I have no chance of being admitted to ITU ‘with Covid ((whatever that is) right now.”
… and the Telegraph reported data projects that 127.7/100,000 of the worst affected category between 60 and 69 would gain the benefit of not getting admitted to an ICU from a stab in the dark!
Is the AZ/JJ risk because they are vector vaccines?
Nobody knows yet. May be toxicity related to the precise nature of the spike protein they produce.
As I’ve said in another response re. the data reported in the Telegraph – work out the maximum reported absolute risk reduction.
… and weep : it’s actually below 1% by my calculation. Such are the deceptiveness of big numbers to the unwary.
Can’t say I am convinced by these graphs in The Telegraph. The paper has had a strange fanaticism about promoting these experimental ‘vaccines’ and ridiculing any who raised concerns. Now they can’t avoid admitting that there is some risk, they have resorted to down-playing it But do we really believe the coincidence theorists who say there is no link between the January / February surge in excess deaths and the vaccine roll-out? The more they deny it, the less convinced I become.
Those graphs are actually a confirmation of the practical irrelevance of the ‘vaccines’ if you do the numbers.
The Telegraph charts are a typically flawed risk assessment. They are comparing apples with oranges. They are not looking at the severity of outcome associated with the risk (probability) of the hazard. The maximum (credible) severity for Covid in an otherwise fairly healthy person under 65 is short term hospitalisation. The maximum (again credible) severity from taking the “vaccine” is death !
Yes agree.
The telegraph graphs are incomprehensible and dangerous nonsense. Irresponsible journalism in my opinion.
As you say they are not even comparing deaths with deaths.
The Telegraph can’t know the potential harms. The long term affects can’t be known without travelling into the future. These are after all experimental vaccines with emergency approval only, that co-opt the body’s cells to produce the spike protein. They are not traditional attenuated or inactivated vaccines that present weakened or ‘dead’ virus to the body’s immune system in a not dissimilar way to natural infection.
And the short term harms are only those that have been admitted to so far. No data has been published showing mortality of those vaccinated vs those not vaccinated. So short term affects are only being assessed through the totally inadequate yellow card system. Remember it wasn’t long ago we were told the AZ vaccine was completely safe.
Thanks for posting the harms vs benefit charts. I’ve been looking for that sort of thing to help make my own decision..
Chart showing chance of dying or not dying from or with covid (SARS-C0V-2) by age band since first recorded SARS-C0V-2 death
I’ve posted this before but have now updated to 8th April 2021 following the ONS publication ‘Deaths registered weekly in England and Wales, provisional: week ending 26 March 2021‘
Here is a chart showing the chances that an average person in each age group would have died with or from covid in England and Wales versus not died with or from covid. This is based on the full period from the first covid recorded deaths in early 2020 up to 26th March 2021 (most recent data point).
The proportion of the population in each age group dying with or from covid is the red bar element. Apologies but this red bar is hard to see for most age groups, that’s just the way it is.
I think it may be useful for anyone weighing up the small risk of dying from covid in the context of a decision on whether to have an experimental vaccine or not. That is in weighing up (any) reduction of this risk provided by experimental vaccination against the significant potential harms of experimental vaccines.
a) Note that even a theoretically 100% effective experimental vaccine can’t stop a death with covid, it can only prevent a death from covid. So even a theoretically 100% effective vaccine isn’t helping you with most of that red bar; you still die but without the covid label
b) The red bar represents the proportion of the population in each age band who have subsequently died with or from covid since the first recorded covid deaths occurred around March 2020. The chance of someone dying in the future from covid (which is more relevant in terms of vaccine decision making) is likely considerably less than this past risk.
c) If you are in good health and have no comorbidities, and you make sure your vitamin D levels are reasonable then your risk of dying from covid is just a very small element of that already small red bar. If you have comorbidities then your chances of dying may be considerably more than the average person in that age category, but then a) and b) may still bring your odds down to somewhere close to that red bar.
(I’ve based population on the mid-2019 ONS population figures without adjustment for the population change into 2020. For the purpose of the chart this seems reasonable to me)
I’ve written to my MP in the United Kingdom – Dame Angela Eagle – twice, to inform her that cancer-causing ethylene oxide is being used to sterilize the swabs used in imported Chinese Covid19 Rapid Antigen Lateral Flow test kits. Our Prime Minister Boris Johnson has recently announced plans to roll out these tests to the entire UK population, but he is neither notifying us of any potential danger, nor are the UK Government screening these imports to verify their safety. I believe the International Standard ISO 10993-7 does not cater for constant, repeated, invasive use of these swabs, millions of citizens’ are being kept in the dark and their health could be foreseeably and avoidably placed at risk: https://wirralinittogether.blog/2021/04/08/update-cancer-causing-ethylene-oxide-in-rapid-antigen-lateral-flow-test-kits-to-be-rolled-out-across-england-weve-sent-a-second-email-to-our-mp-dame-angela-eagle/
I wonder if we can rule out the high exposure risk – and possibly the medium too – given that we’re apparently close to herd immunity.
Seasonality could also be a factor so even the low exposure risk could be a bit pessimistic – for a few months at least.
I won’t be shooting up with a vaccine to escape the ills of the 21st century just to make myself feel better. In fact, the only form of escapism I’d recommend right now involves listening to Philip K Dick audio books on YouTube. Try it. Each one is a guaranteed, 8-our-long, mind expanding experience, with no drugs involved … and get this – forewarned is forearmed – because all sorts of harbingers appear about not just impending globalism, but it goes one step further and into the workings of crazed, deeply-threatening, psychopathic interplanetary corporations and governments, which proliferate throughout, spreading their malign influence. The only requirement to get deeply immersed in this stuff is a capable, insightful, enquiring mind. The prescience and foresight of this author is staggering. Forget everything you witnessed in the Hollywoodised PKD movies and listen to these novels. They amount to a science fiction narrative that oh so gradually has been assuming reality as each day goes by.
Interesting comments from the SAGE modelling group (March 31st)
Paragraph 56 begins
https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/975909/S1182_SPI-M-O_Summary_of_modelling_of_easing_roadmap_step_2_restrictions.pdf
h/t to @AhraniLogan
https://twitter.com/AhraniLogan/status/1380249545456619522
One of whom, we must assume is Prince Philip.
Just to be clear, is this report saying that wave 3 will have more cases of Covid in hospital in the vaccinated group than in the unvaccinated group\/
I wonder what information they use to make that projection? Saying that it is the ‘at risk group’ simply doesnt cut it as an explanation.
FFS include the risk to those who have already had Covid-19, PLEASE, Daily Telegraph.
All this is based on so many flawed assumptions that it’s preposterous.
Quite so – and it is based only on the known clotting risk (and indeed only on reported problems, which are inevitably under-estimates), ignoring various other known risks plus unknown future problems!
You have to wander how many of these present as strokes or “sudden adult death”, or “found collapsed”. I bet the rate of death from this new “vaccine” syndrome is higher in the elderly/older age bracket. It’s just not recorded, because, you know, “old people die”. And if they were serendipitously to die with covid particles up their noses, all the better, as their death will be recorded as a Covid death.
And thus we’re all blimmin trapped in an unending lockdown.
Strange goings on, so our wise health secretary decided not to follow the manufactures guidance to inoculate the second jab after 3 weeks, but rather to wait 12 weeks. I suspect to make the numbers look good and persuade the hesitant to follow suit. Someone, who works in a governmental department, has been forced to take it on the basis that they couldn’t come into work otherwise, turned up to work this week and the second dose was being administered. It was 8 weeks after first one, others are being given it after 6 weeks. I am assuming that they have run out of candidates for the first one. How can it be right to even alter the recommended dose in the first place. They were extremely ill after the first one, stomach cramps, violent headaches and constant tiredness. The later 2 symptoms have persisted. They are not faring any better after the second one and says they will not be taking any more. No information after the first one and given a leaflet after the second. I am lucky to be able to work for myself and make an informed choice, which is NO! NO! NO!
How would you calculate the cost/benefit of vaccinating teenagers? I ask having just seen the news that Pfizer wants emergency authorization for use of its vaccine on 12-15 year olds. Cost would include the price paid for the vaccines, staff costs, organization of it all. Benefits? Asking as a non-expert.
Hmmm, interesting how the goalposts move all of the time. First of all they said that the AZ vaccine was safe. Now they are saying that it is a risk, but that the risk is worth it for the majority of people. We now know that they were lying when they originally said it was safe, but the truth has started to leak out and they had to change their position.
So does anyone really believe this latest attempt to try and persuade us that this vaccine is a good idea given the previous set of lies? Once they have lost your trust, you would be a bit of a loonie to trust them again.
I think some people have been driven so mad by fear of the virus and were clinging onto the vaccine as their salvation….they’re going to grasp any positive commentary about any of the vaccine now in desperation of maintaining their hopes ….and block out any bad news on the dangers
The one that makes me laugh (ruefully) are all the people who a year ago were washing their groceries with bleach and not listening to anyone who said “you’re more at risk in a car” are now saying “you’re more likely to die in a car crash than from the vaccine”. Mumsnet is full of these idiots.
At least the car gets you places in comfort. What benefit does the vaccine give you? Protection (maybe….or maybe not) from something you don’t need protecting from anyway.
The only benefit I’m aware of is psychological, in that certain elderly people I know who have had the jabs, seem to be less anxious than they were. Of course, a lot of it was artificially ramped up in the first place.
These numbers don’t seem to make sense/add up at all.
Look at the top chart, which assumes (I think) that 2 in 10,000 people, i.e. 20 in 100,000 people, catch covid19 (during the month in question?).
So are they saying that 5.7 out of every 20 healthy 40-49 year olds who catch covid will end up in ICU? Or 2.7 out of every 20 30-39 year olds? That cannot be correct – we know that the risks are vastly smaller than this.
Additionally, the numbers are ambiguous because absolute “risk” itself is not definable except over a particular time period – so are the data on the left referring to risk during a one month period? Or during a lifetime? Or what? It is certainly apples and oranges to equate risk of disease, in a one month period, against a one-off risk of vaccination.
However, if the vaccines must be repeated every year (like with flu), then it might be reasonable to equate the risk per jab against the risk of covid per year.
I may well have misunderstood something – grateful if others can look at this.