
HART recently published concerns about the wisdom of COVID-19 vaccination in pregnancy and we now look further into recent reports from many countries about falling birth rates. The big question, to which we have no clear answer, is whether these two issues are linked. Birth rates have been declining in recent years but there does appear to have been a sharper decline in 2022.
Hagemann et al. in August 2022 published an analysis of birth rates in Europe. The paper includes a detailed methods section, outlining how they calculated the proportion of young adults being vaccinated in each month from January 2021 and then correlated vaccine uptake with birth rates nine months later.
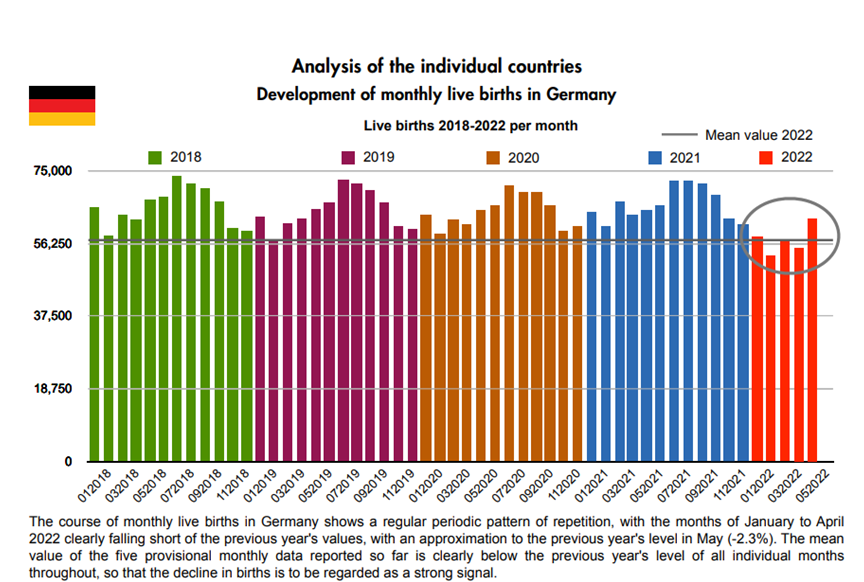
The birth rate from Germany shown in Figure 1 strongly resembles the pattern seen repeatedly across the countries of Europe.
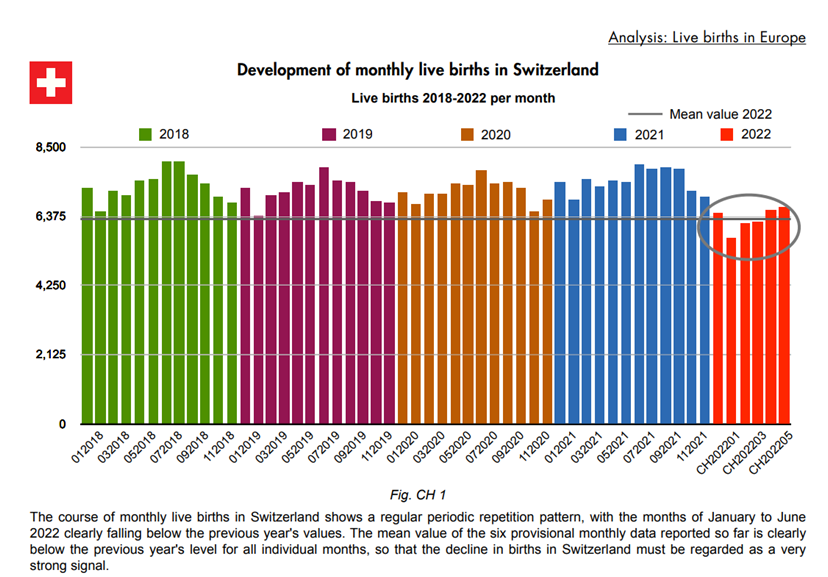
An almost identical pattern is seen in Switzerland.
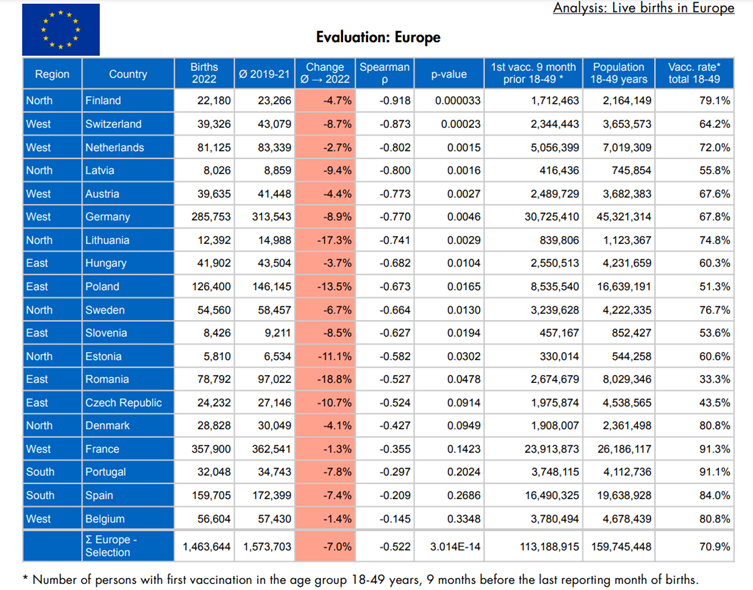
Reduced birth rates in 2022 spread right across Europe to a lesser or greater degree, as shown below.
So what could be causing the decline in live births? The explanations fall into two basic categories: either fewer women are becoming pregnant or there are more pregnancy losses (or both).
- Fewer pregnancies:
- a. Choice – are people less confident about the future, whether economic or climatic or other societal pressures, and has this affected the choice of pregnancy? Or, did they choose not to get pregnant around the time of vaccination?
- b. Lack of opportunity – did lockdowns prevent people meeting and making relationships?
- c. Are there more problems with fertility or conception (both male and female causes)?
- More pregnancy losses:
- a. Spontaneous miscarriages
- b. Terminations
- c. Stillbirths
The first group of ‘societal’ reasons (1a) are beyond the scope of this article but should not be disregarded. Lockdown effects (1b) seem unlikely to be a major factor, in that the birth rates in 2021 continued to follow the pattern of previous years. However, there remains a question of the time lag between a relationship starting and the arrival of the first baby.
This leaves ‘medical’ causes of infertility (1c) and pregnancy losses (2) from miscarriages (2a), terminations (2b) and stillbirths (2c).
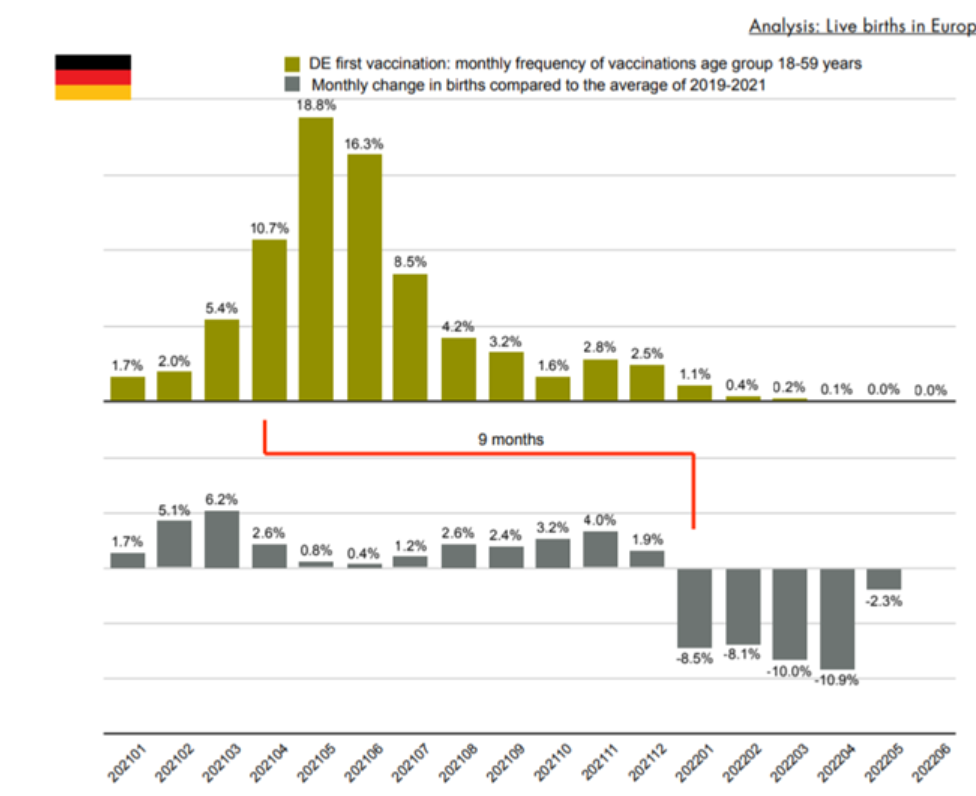
Returning to Hagemann’s European data, the authors illustrated a nine month time lag between vaccine rollout to young adults and the point at which birth rates drop below the 2019-2021 monthly average. The chart below shows monthly percentage vaccine uptake in younger adults in the top half of the graph and change in birth rates in the lower half (Figure 3). This is likely too simplistic for what is almost certainly multifactorial, but nevertheless when replicated in many countries raises some uncomfortable questions.
Fertility and conception
Fertility rates (pregnancies per 100,000 women) fluctuate in time and place for many reasons but there has been concern at a general downward trend. Whilst for those concerned at the ability of the Earth to sustain growing populations this may seem to be a ‘good’ thing, it has caused consternation for others.
But the urgent question is whether widespread COVID-19 population vaccination has had any effect. The minimal animal work carried out by Pfizer on the biodistribution of the lipid nanoparticles used in its vaccine showed concentration the testes, although at a much lower levels than the ovaries. More worrying was a fall in motile sperm count noted in sperm donors following vaccination, a decrease which was still present five months later. For women, menstrual disturbance has been widely reported, even to the point of finally being included in the MHRA Yellow Card reports. It is also known that the spike protein shares features with syncytin, hence there is a theoretical potential for antibodies to spike protein to attack the placenta. Indeed, studies have shown raised antibody levels to syncytin after Covid vaccination.
Pregnancy losses
Miscarriages
Miscarriages are not notifiable or registered, making risks much harder to ascertain, as discussed recently by HART, including differences in how the background rate for miscarriages has been estimated.
There have been many public statements around the safety of COVID-19 vaccines in pregnancy, which are still being pushed, despite the dropping of vaccines generally for healthy non-pregnant under-50s. Pregnant women were specifically excluded from all the vaccine trials, and participants had to agree they (or their partners) were not planning to become pregnant during the course of the trial. Thus, most of the ‘safety’ data has come from cohort studies after rollout. This is fraught with methodological problems and biases, as highlighted by Norman Fenton.
A paper from the U.S. looking at VAERS data using the proportional reporting ratio for COVID-19 vaccines to influenza vaccines, showed an increased ratio for menstrual abnormalities, miscarriages and a number of foetal abnormalities, but some have claimed (without supporting evidence) that there is the potential for bias, in that reporting may be higher with a new vaccine.
Terminations
The ONS published data this week showing that in 2021 the conception rate fell in every age group under 40 years of age and the abortion rate rose for every group aged over 18. Similarly the abortion rates in Scotland have shown a marked rise since mid-2021. The rise in terminations coincides with vaccinations in pregnancy. It would be particularly important to learn how many of these were later terminations due to congenital abnormalities.

Stillbirths
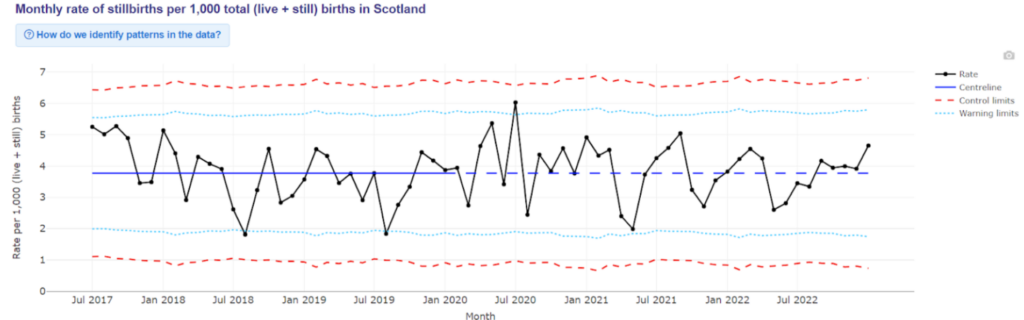
In theory, stillbirths should be easier to chart since they must be registered, but ONS data are published several months in arrears. Provisional figures for 2021 for England and Wales showed the first rise in stillbirth rate since 2014, but causes are not clear. There are no Government data on stillbirths by vaccination status in England. However, the stillbirth rate remained stable in Scotland as shown in Figure 5.
Neonatal deaths
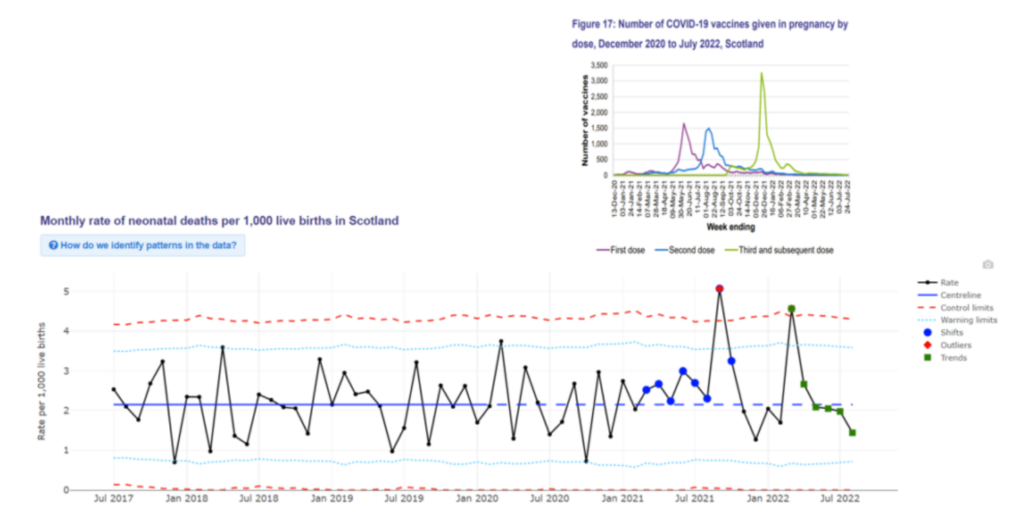
Whilst these are not reflected in the falling live births, they are nonetheless equally tragic for parents. Concern has been raised in Scotland that the neonatal death rate was 1.7 per 1,000 live births for women vaccinated at any point in pregnancy but double that at 3.4 per 1,000 for those delivering within 28 days of a COVID-19 vaccine. Two spikes in neonatal deaths have led to an inquiry, but depressingly there is still no plan to include vaccination status in its remit, as shown in the reply to a recent open letter to the inquiry chairman, consultant neonatologist Dr. Helen Mactier, in which it was – somewhat unbelievably – stated that there were no plans to examine vaccination status, as to do so might induce vaccine hesitancy. The figure below shows the timing of these peaks in neonatal deaths relative to peaks in vaccinations in pregnancy.
Meanwhile, the RCOG is still actively promoting vaccination in pregnancy and has failed to respond to requests for its evidence of safety, particularly given the now milder variants and the high levels of immunity in young adults.
The question is, when is the Government going to order a proper investigation to put an end to speculation over whether correlation does or does not reflect causation? Without access to the raw data, HART is unable to shed any more light on the subject.
Dr. Ros Jones is a retired Consultant Paediatrician with a special interest in neonatal intensive care and paediatric HIV. She has served on the Advisory Committee of the National Perinatal Epidemiology Unit and on the Education and Training Committee of the RCPCH. She is a member of the Health Advisory and Recovery Team (HART), on whose website this article first appeared.











To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
Climate Change did it, silly.
I vote for SNGBS (Sudden Not Getting Pregnant Syndrome). Most likely due to NHS failures and an increase in women taking the pill.
This article kind of reminds me of how serial killers like to revisit the scene of their crimes:
https://www.telegraph.co.uk/global-health/women-and-girls/infertility-one-six-who-world-health-organisation-figures/
See the smoking gun, anyone? If there is such complete certainty that vaccines are not a contributory factor in neonatal deaths, etc. that they do not even warrant investigation, how can the statement about investigating them engendering “hesitancy”, or “harming confidence”, make any sense?
It would only make sense if there was strong suspicion among those pulling the strings of this inquiry that there WAS a link between vaccination during pregnancy and the drop in birth rates. And furthermore it would only make any sense if they wanted to obfuscate the fact (by failing pursue a relevant line of inquiry).
I was utterly dismissive about conspiratorial musings on a “depopulation agenda”, but now the data, along with the bizarre ducking of the question by all the frontline investigators, is indecorously hand-waiving in that direction!
Interestingly non-lockdown, heavily vaccinated Sweden also shows a drop in birth rate.
In the ’80s/’90s, when I had my sons, women knew not to take any medications during pregnancy, including painkillers such as aspirin and paracetamol. They knew to lay off alcohol, cigarettes, too much caffeine and some cheeses.
I firmly believe that the jabs are responsible for the reduced birthrate and the increased miscarriages and stillbirths. I’m prepared to accept that there was no evidence of this when the jabs were rolled out (since Pfizer carried out no trials) but there is evidence now and it is disgusting that the MHRA and other authorising agencies are not prepared to investigate it.
I am astounded that so many young women ignored all the longstanding advice about the effect medications can have during pregnancy and participated in the mass medical experiment.
I think that if a pregnant woman sees nothing wrong with getting injected with these gene therapies ( demonstrating the fact she’s not done any independent research of her own ) but runs a mile from liver pate or avoids shellfish then she needs her bloody head read. These people are on a par with masktards who’ve had multiple clot shots. Complete imbeciles and beyond help.