Dr. Richard Ennos, a retired Professor of Evolutionary Biology at Edinburgh University, has undertaken a thorough analysis of the U.K.’s COVID-19 ‘Yellow Card’ vaccine adverse event data and found it indicates “unequivocal safety signals” for adverse reactions caused by the Pfizer and Moderna vaccines affecting the blood, the heart and female reproduction. He concludes that: “There can be no question that the mRNA vaccines should be withdrawn with immediate effect.”
In the U.K., three COVID-19 vaccines – AstraZeneca (AZ), Pfizer (PF) and Moderna (MO) – have been used in a nationwide inoculation programme aimed at preventing harm from the SARS-CoV-2 virus. All three vaccines provide the genetic code that enables vaccinees to produce within their bodies the spike protein of the SARS-CoV-2 virus, the molecule associated with the pathology of COVID-19. In the AZ vaccine the genetic code for the spike protein takes the form of DNA, and is introduced into recipient’s cells by a genetically modified chimpanzee virus (DNA, adenovirus vector). For the PF and MO vaccines, the introduced genetic code takes the form of heavily modified RNA, and is carried to recipient’s cells within lipid nanoparticles (mRNA, lipid nanoparticle). There is no control over either the tissues to which the vaccines are transported or the length of time for which spike proteins are produced by those tissues.
All three vaccines rely on novel technology that has never before been used in humans. At the time of their introduction, they lacked any long-term safety data, and therefore required Conditional Marketing Authorisation from the Medicines and Healthcare products Regulatory Agency (MHRA). To monitor the safety of the three vaccines the MHRA established the COVID-19 vaccine Yellow Card reporting scheme (C-19VYC). This collates standardised reports of suspected adverse reactions to the COVID-19 vaccines that can be analysed to detect safety signals and potentially trigger withdrawal of the vaccines. Here we show that a thorough analysis of the C-19YC data indicates unequivocal safety signals for adverse reactions caused by the mRNA vaccines PF and MO affecting the lymph system, the heart and female reproduction.
The strength of the C-19VYC reporting scheme is that it is capable of generating an enormous amount of valuable information about adverse reactions to the experimental COVID-19 vaccines. Reports of suspected adverse reactions can be submitted not only by physicians but also by the recipients of the vaccines themselves, providing valuable feedback to the MHRA based on first-hand experience. This inclusive aspect of the C-19VYC reporting scheme has proved very successful, with nearly half a million adverse event reports submitted, roughly one for every hundred recipients of the COVID-19 vaccines in the U.K.
Despite this strength in terms of quantity of data, the C-19VYC reporting scheme has a number of serious weaknesses related to the nature of the data collected. These weaknesses place limits on the scheme’s ability both to detect and to measure safety signals. The first problem is that the scheme does not identify or include a control group of individuals, who have not taken the vaccine, against which to compare those who have. Other major weaknesses are that reporting is passive rather than planned and takes place at a single point in time. Thus, reporting relies on the sufferer of the adverse reactions or his or her physician making the connection between the vaccine treatment and the adverse reaction. As a consequence, many adverse events will go unrecorded, and this becomes more likely the longer the delay between treatment and the associated adverse reaction. Reporting rates of adverse reactions are also likely to represent only a fraction of actual cases because physicians or recipients may have too little time to fill out the onerous paperwork, may not have knowledge of the Yellow Card scheme, or may be unwilling to countenance the idea of harms resulting from a medication in which they have placed trust.
As well as being low, reporting rates are expected to vary substantially between different sectors of the population. Experience shows that females post roughly three times more adverse event reports than males, and the reporting rate for adverse reactions varies with age, dropping off in the elderly population where adverse reactions may be obscured by multiple forms of pre-existing chronic illnesses. In addition, reporting rates are likely to vary with the severity of the adverse reaction. Individuals are far more likely to have the motivation and tenacity to file a report if their adverse reaction is severe than if it is mild. On the other hand, if the adverse event results in death, grieving friends or relatives may be too preoccupied to file a C-19VYC report.
Recognising the limitations in the C-19VYC programme is a very necessary first step in exploiting the enormous volumes of data that it has produced. In its published summaries the MHRA is at pains to emphasise that the Yellow Card data cannot be used to calculate true rates of adverse effects or to compare the safety of the different vaccines, both because of the nature of the data and the existence of many confounding factors. I view the MHRA’s statements as a challenge. In the remainder of this article, I will endeavour to show that the MHRA’s view is overly pessimistic and that the enormous efforts of those who have submitted Yellow Card reports of COVID-19 vaccine adverse effects have not been in vain.
In order to independently analyse the C-19VYC reports, it is essential to have access to the raw data. The first FOI request for access to the full anonymised C-19VYC data was made in June 2021. This, and subsequent FOI requests have been refused on the grounds that it would be too onerous to pass on the raw data, and that anyway the data would be published at a future date. However, it should be noted that the MHRA sends the C-19VYC data without delay to the companies that market the COVID-19 vaccines. Some 18 months after the first FOI request, the MHRA has at last released information gathered by the C-19YC scheme that is sufficiently detailed to allow independent analysis and calculation of safety signals.
A cursory look at the C-19VYC data indicates that the rate of reporting of serious and fatal adverse events is nearly three times higher for the adenovirus AZ vaccine (3.912 serious or fatal reaction reports per 1,000 doses) than for either of the mRNA vaccines PF or MO (1.341 and 1.344 serious or fatal reaction reports per 1,000 doses respectively). Although there has been no formal withdrawal of the AZ vaccine by the MHRA, the use of the AZ vaccine has effectively been discontinued, perhaps because of this worrying safety signal. With the discontinuation of the AZ vaccine, the most important question becomes whether serious safety signals can be detected for the remaining mRNA COVID-19 vaccines, PF and MO, that are still being employed.
As I have emphasised earlier, the data available from the Yellow Card scheme are the result of passive reporting. This means that any detailed analyses based on absolute numbers of reports of adverse reactions are problematic. However, a well-established protocol, known as proportional reporting rate analysis (PRR) has been devised for detecting safety signals using passive reporting data such as those collected by the C-19VYC scheme. The principles underlying the PRR protocol are explained below.
Suppose that we wish to see whether a novel vaccine substantially increases the frequency of a particular adverse reaction, say severe headache. If there is no connection between administration of the vaccine and the frequency of severe headaches, then the proportion of all adverse reaction reports that are severe headache should be the same for the novel vaccine as for the established and thoroughly tested vaccines. However, if administration of the novel vaccine does cause severe headaches, there will be a higher proportion of all adverse reaction reports that mention severe headaches for the novel vaccine than for the established vaccines. By dividing the proportion of adverse events which mention severe headache in the novel vaccine by this same proportion calculated for the established vaccines, we obtain a measure of the strength of the safety signal for severe headaches caused by the novel vaccine, the proportional reporting rate or PRR.
A safety signal is formally detected if three conditions are met. First, there must be a substantial number of reports of the chosen adverse reaction in the novel vaccine database. Second, the proportion of all reports that mention the chosen adverse reaction must be statistically significantly greater for the novel vaccine than for the established vaccines. This can be established using a simple ‘chi squared’ test. Thirdly, the proportion of adverse reactions calculated for the novel vaccine must be at least twice that calculated for the established vaccines (PRR>2).
To apply this PRR methodology to detect safety signals for the novel mRNA COVID-19 vaccines PF and MO, we make the very conservative assumption that the AZ vaccine does not increase the frequency of the particular adverse reactions that we are investigating. The AZ vaccine thus takes on the role of the safe, established vaccine in the PRR analysis. Therefore, we use data from the AZ vaccine to calculate the proportion of the chosen adverse events that we would expect in an established, safe vaccine. We then calculate the proportions of the chosen adverse event reports that occur in the PF and MO data, and compare these with the figure that we have calculated for AZ to obtain the PRR. If there is a significantly higher proportion of the chosen adverse event reports in the mRNA vaccines than in the AZ vaccine, and the PRR for the mRNA vaccine is two or more, this constitutes a strong safety signal requiring investigation and appropriate action.
In December 2022, MHRA released two data files from the C-19VYC scheme for each of the three COVID-19 vaccines. The first file contains an identifier for each Yellow Card report, the sex and age of the individual involved, and a classification of the severity of his or her adverse reaction – non-serious, serious or fatal. The second dataset includes the report identifier and various medical classifications of the adverse events suffered (there may be more than one adverse event per report). Perhaps the most accessible classification for the layman is based on the tissue type affected by the adverse reaction e.g. muscle, nerve, blood. By marrying up the two datasets, it is possible to create a single file for each of the COVID-19 vaccines that includes the report identifier, the sex and age of the patient, the tissue type affected by the first adverse event listed in the report (to avoid pseudo-replication of the reports), and the severity of the adverse reaction.
Data in the file described above are used here for PRR analysis to detect and measure the strength of safety signals associated with the adverse effects of the mRNA vaccines PF and MO on blood (harm to the blood and lymph system), the cardiac system (harm to the heart), and reproduction in females (harm to the menstrual cycle). The analysis has been confined to severe adverse reactions (serious plus fatal) to avoid the possible charge that the adverse reactions we are analysing are of little consequence to those they affect. To acknowledge the fact that reporting rates vary with both age and sex, the reported PRR values have been calculated in samples that are matched for both age and sex. This allows vulnerability to particular adverse reactions to be compared between age groups, and between females and males. It should be noted that when the analysis is conducted in the manner described, it yields minimum estimates of the strength of the safety signals because it assumes that the AZ vaccine does not increase the rate of the adverse reaction being studied. If this is not the case, the estimated strength of the safety signal associated with the mRNA vaccine concerned will be greater than we report.
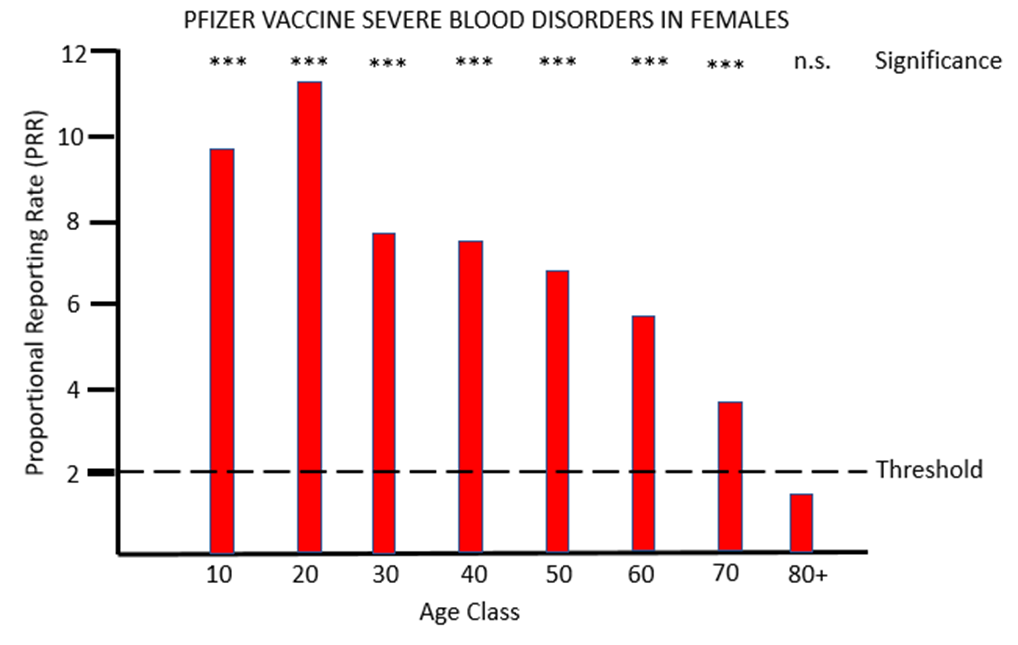
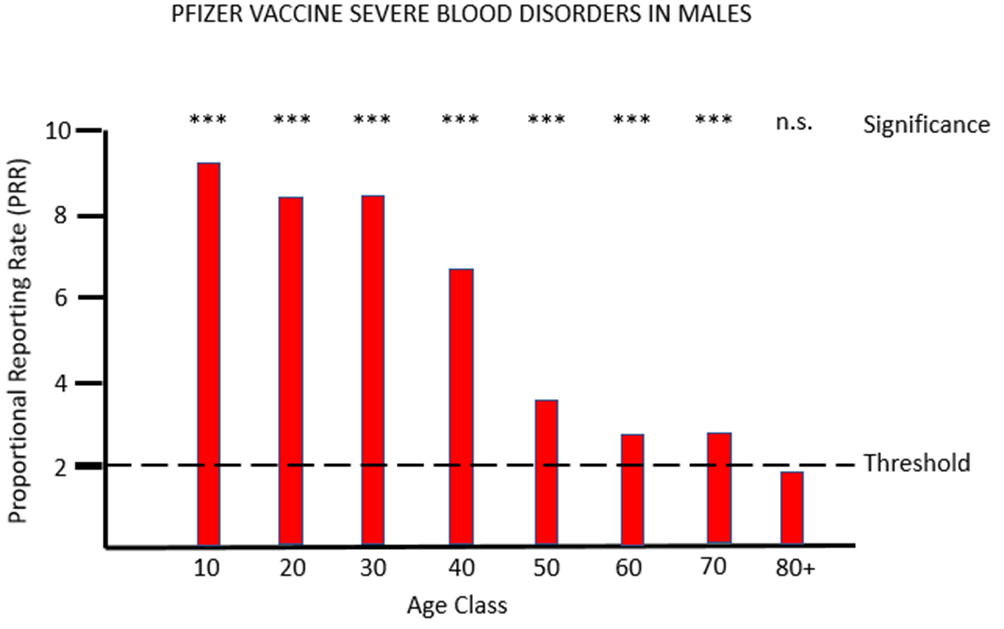
Figure 1a and 1b show the results for females and males respectively of PRR analysis of adverse reactions associated with the PF vaccine that affects tissues grouped under the MHRA classification blood (blood and lymph systems). For both sexes, and across all except the very oldest age class, there are very striking safety signals, with proportions of severe adverse event often more than eight times higher after PF vaccination than after AZ vaccination.
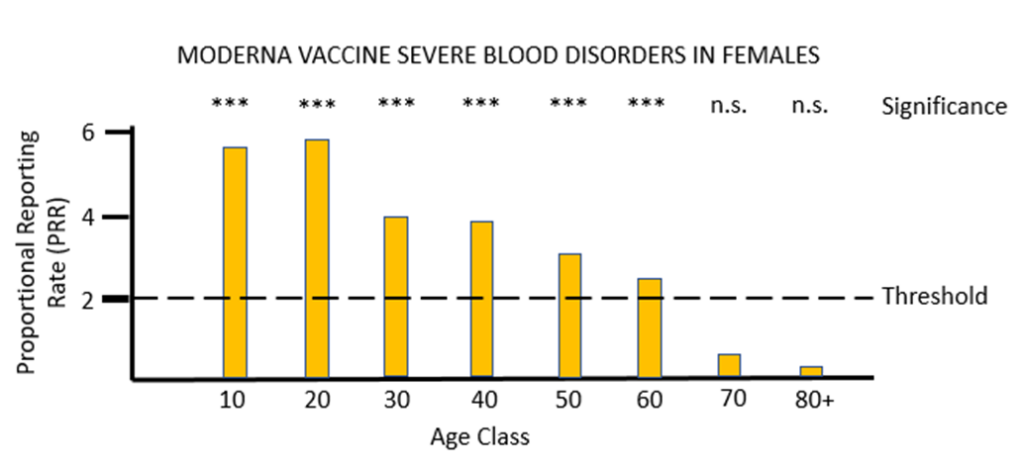
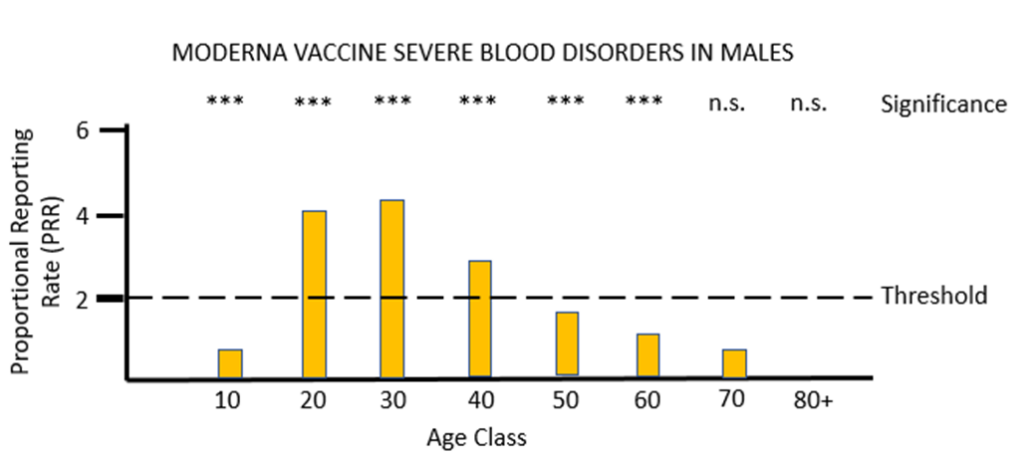
For the other mRNA vaccine MO, the proportional reporting rate is again very significant and well over the threshold level for safety signals in most of the female age classes and in males aged between 20 and 49. The vast majority of these severe adverse reactions affect the lymph system rather than the blood, and the diagnosis given is lymphadenopathy. It is very worrying that in its “Coronavirus vaccine – summary of Yellow Card reporting” in January 2023 the MHRA fail to mention any possible adverse effects of the mRNA vaccines on the lymph system, despite such a strong safety signal being present when the Yellow Card data are appropriately analysed.
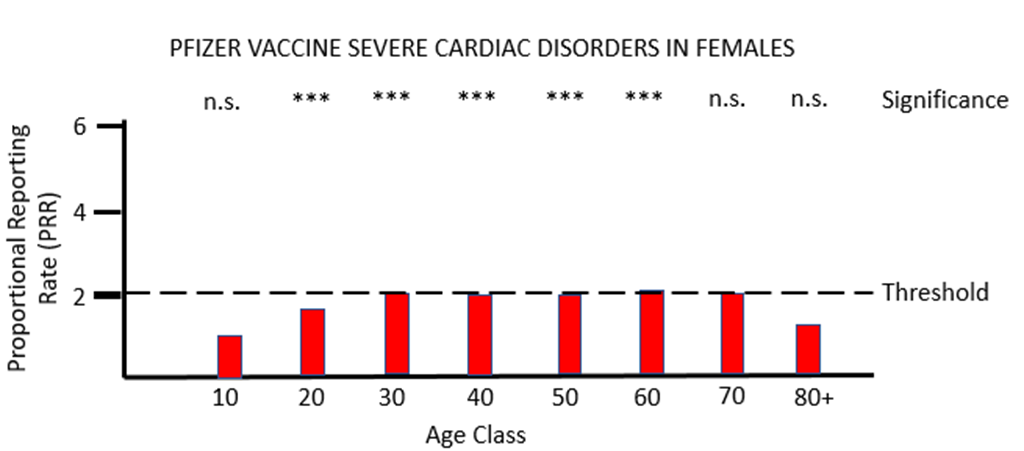
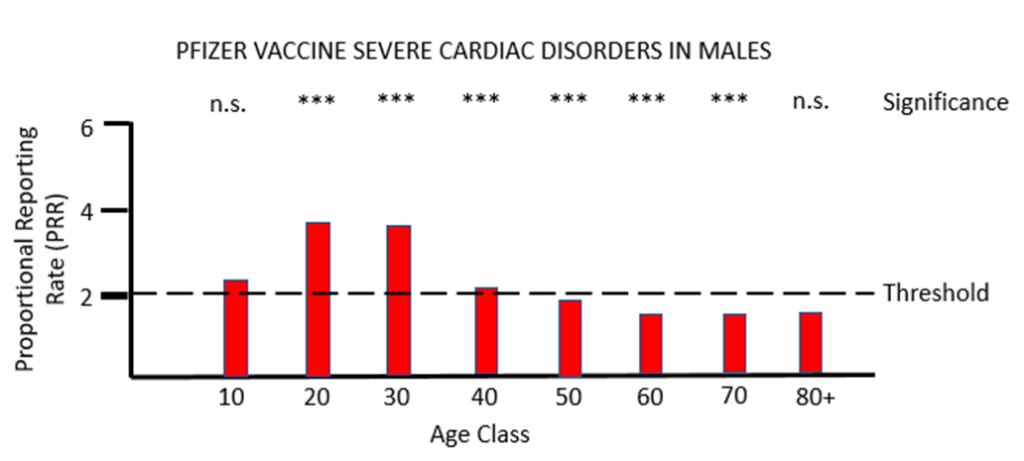
When PRR analysis is applied to investigate possible adverse effects of PF vaccination on the heart (cardiac, Figures 3a and 3b), there is a clear and significant safety signal for males between the ages of 10 and 50. For females values of PRR very close to the threshold value of 2 are present for ages 30 to 80.
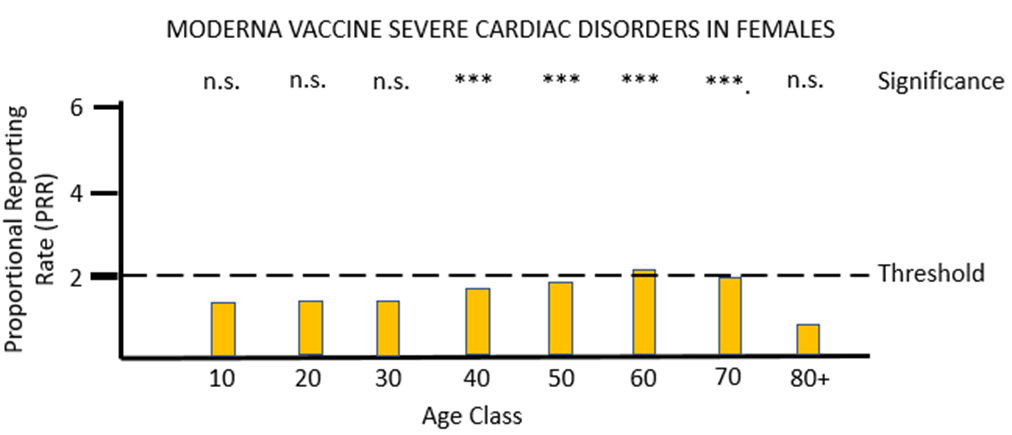
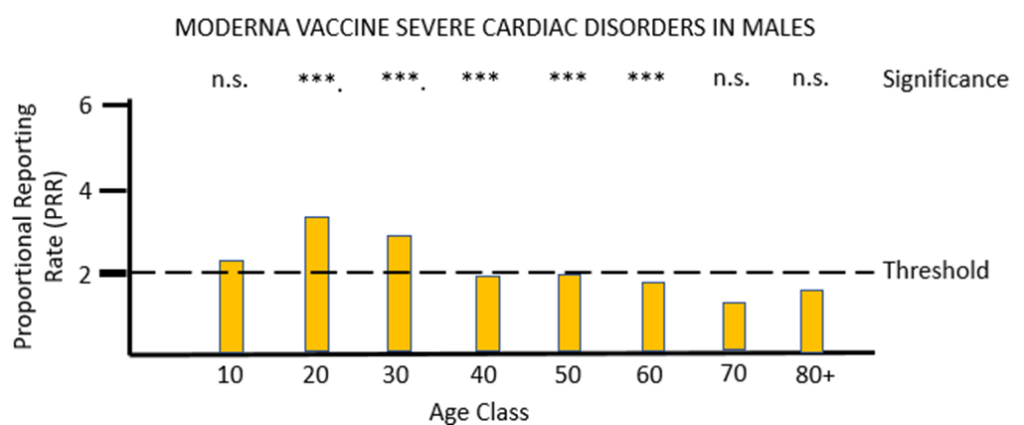
For vaccine MO (Figures 4a and 4b) the same pattern of safety signals for severe cardiac disorders are found as for PF: high and significant proportional reporting ratios in young males from 10 through 40 years of age, and reporting ratios close to or just exceeding 2 in females 50 to 80 years of age.
The MHRA has conceded in its Yellow Card summary that: “There has been a consistent pattern of higher reporting of these suspected events (myocarditis and pericarditis) with both the monovalent COVID-19 Vaccine Pfizer/BioNTech and COVID-19 Vaccine Moderna, and of these occurring more frequently in males.” However, it has not apparently made any attempt to use the Yellow Card data to demonstrate a formal safety signal in the manner described above. It is also apparently unaware of the safety signal in females. Its response to the high number of reports of myocarditis and pericarditis generated by the mRNA vaccines has not been to withdraw the offending products, but instead to alter the safety information associated with these products and alert health professionals to look out for these very serious adverse events after the relevant vaccines have been administered: “[T]he product information for both monovalent COVID-19 Vaccine Moderna and COVID-19 Vaccine Pfizer/BioNTech was updated to inform healthcare professionals and patients of these reports and provide advice to be aware of important symptoms for myocarditis and pericarditis.”
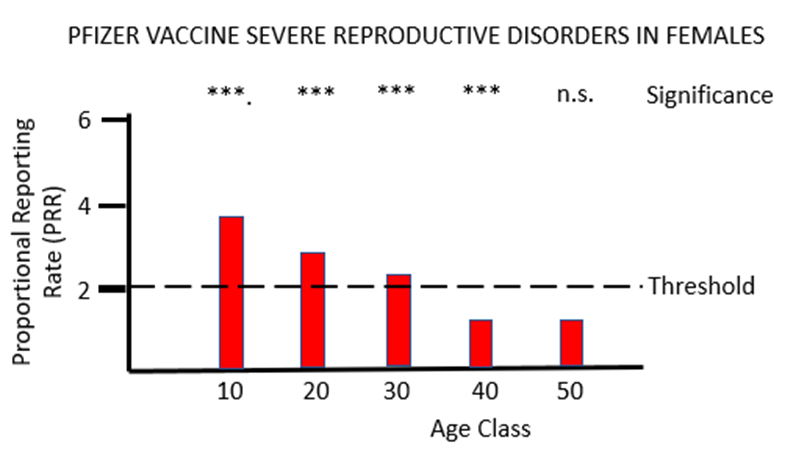
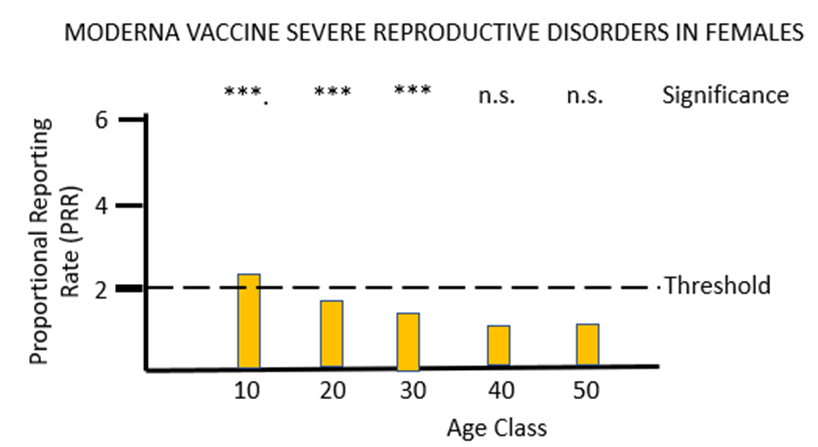
The final piece of analysis reported here investigates whether the Yellow Card data yield a safety signal associated with female reproduction following inoculation with the mRNA COVID-19 vaccines. Figures 5a and 5b illustrate the results of PRR analysis for the PF and MO vaccines respectively. For PF there are significant safety signals in age groups 10 through to 40, while for MO a formal safety signal is only found in the youngest (10 to 20 year) age groups. The vast majority of the adverse event reports for female reproduction involve disruption to the menstrual cycle and excessive menstrual bleeding. Again, these have been recognised by the MHRA as side-effects of the mRNA vaccines but their severity has been downplayed, and no attempt has been made to formally identify safety signals despite the relevant data being available. As before, the MHRA has done nothing to protect the public from the severe adverse reactions to the mRNA vaccines that the Yellow Card data have revealed: “Evidence from the most recent review suggested a possible association between the Pfizer and Moderna COVID-19 vaccines and heavy menstrual bleeding. … The product information for the Pfizer and Moderna COVID-19 vaccines is therefore being updated to add heavy menstrual bleeding as a possible side effect.”
A number of conclusions can be drawn from the analyses reported above. The first is that by applying PRR methodology it is possible to use the passively reported Yellow Card data to detect and quantify safety signals for novel vaccines, to gain insights into particular sex and age classes that may be affected by particular adverse reactions, and to compare the safety profile of different vaccines. The second conclusion is that the mRNA COVID-19 vaccines do not appear to be safe. Glaring safety signals are apparent indicating harm to the lymph system, the heart and to female reproduction. There can be no question that the mRNA vaccines should be withdrawn with immediate effect. The final conclusion is that the MHRA has provided no protection to the U.K. public from the adverse effects of the novel COVID-19 vaccines. Its regular publication “Coronavirus vaccine — summary of Yellow Card reporting” has been an exercise in defending the COVID-19 vaccines from criticism rather than defending the U.K. public from the COVID-19 vaccines. Its reports lack any scientific rigour, include not a single piece of statistical analysis to support the conclusions drawn, and are an affront to the huge number of individuals who have been injured or killed doing what they believed to be ‘the right thing’.
Dr. Richard Ennos is a retired Professor of Evolutionary Biology at Edinburgh University. He writes: “This article is dedicated to two groups within the U.K. First, the many who have been killed or injured by the rollout of the experimental and untested COVID-19 vaccines to an innocent and trusting U.K. public. Secondly to the dedicated physicians who have filed Yellow Card reports cataloguing the COVID-19 vaccine injuries and deaths. I would like you to know that your suffering and endeavours have not been in vain.”












To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
This ignores what I suspect is the more likely reason. Like any nation, the help they are willing to extend is limited. When budgets are set you have to be careful and often, will be too careful. That is why we have so many potholes in the roads each winter. We could spend a bit more and get the job done properly (and actually save on future potholes, because a stitch in time saves nine) but we don’t. Ukraine is not the West. Our finances are stretched. The US will have its own equivalents of English potholes to deal with where the electorate want more to be spent. So given Ukraine are a foreign nation and it is not the first duty of the US to defend Ukrainian citizens and it is in the nature of any bureaucracy to provide “just enough” finance for most projects, that is why they are providing just enough for them to survive and too little to prevail. It is precisely the kind of project likely to fall into the “not quite enough finance for solving the potholes” pattern.
This is not to say you are wrong, but speculating about motive involves imponderables, at least until years have passed and memoirs written. The reasoning I have laid out above is a universal so though not necessarily the whole of the reason, will be sure to be part of the reason if not most of it.
Why am I thinking about Mr Logic from Viz?
Your choice read to stay abreast of politics?
How long did it take the world’s pre-eminent military powers, with formations already fully trained, equipped, disengaged from conflict, with air supremacy, to prepare an offensive against a third rate tin pot dictator in Iraq?
Errr……that would be six months.
This article, in my view, fails to comprehend the complexity of offensive operations employing mechanised combined arms formations, particularly the logistical organisation, preparation, required.
Add to that a lack of air superiority, constant threat from various surface and air launched munitions, massed field artillery, and the achievements of the Ukrainian Armed Forces so far, in defence and attack, seem admirable.
The Americans then whopped Iraq in a week, if you remember.
The air campaign took four weeks, in fact, which made the rest of the coalition effort straightforward.
But you miss the point.
To put together everything required for a major (Army Corps) mechanised offensive, out of contact, takes six months.
To get the required wherewithal into Ukraine whose forces are in contact under constant air and artillery threat is a great deal more difficult.
Added to that, Britain doesn’t have enough defence equipment or defence production capability to supply Ukraine with much of what it needs.
The U.S. has more but also many more overseas defence commitments.
This is not that complicated. Putin judged his moment well and caught the West napping.
We have form in that regard.
Was the West napping, or was it prancing and preening and thinking a behavioural nudge here, an accounting adjustment there, could remake reality in n it’s favour? I’m fairly sure that it thinks this mindset will bring about the desired outcome in Ukraine.
at the same time, cold calculating minds organise the same deficient response, by well calibrated design.
The West was napping. Britain could barely put a Brigade in the field. Germany’s Army appeared to be largely equipped with broomsticks.
The only militaries properly equipped were in Finland and Sweden, closest to the aggression. And they were neutral. They are not neutral any longer.
That is the best guide of all as to what is going on
Maybe but as usual they just bomb cities “back to the stone age” as I remember. This tends to help. No doubt this lessens collateral damage. Lol.
It seems the Russians have control of the air, and as such could easily destroy Ukrainian cities or to lessen casualties could destroy power stations and other essential infrastructures.
Apparently they have chosen not to do so .Yet.
Thoughts as to why not…
They manifestly don’t have control of the air, not even air superiority let alone supremacy. That is why all of their deep strikes, all of them, are with ballistic & cruise missiles rather than aircraft, and even those are increasingly being shot down.
The notion Russia is showing “restraint” is not supported by the evidence. They are throwing everything they have at Ukraine short of nuclear weapons; having lost so much of their best equipment, they are bringing obsolescent T-62 tanks out of storage.
Re:
“For those who might be sceptical of this, here’s what Professor Hal Brands had to say in an article defending Western involvement:
If only there were a way for Russia to escape from the US and NATO’s ruthless and cunning plan to weaken it by, I don’t know, withdrawing its invasion forces from Ukraine…
This is the voice of someone that thinks the nation state, with its traditions, its physical and economic integrity, is unreal. Crudely, for Russia the war is a necessity. For Europe, a choice. An incredibly bad choice based on green delusion, vanity, hubris, but a choice all the same.
“This is the voice of someone that thinks the nation state, with its traditions, its physical and economic integrity, is unreal.”
Well I’m not quite sure how you deduced that from my very brief response, but I do indeed think that the nation-state is both an entirely artificial political construction, and the greatest source of both internal oppression (the extent of which obviously depends on the nature of the regime with non-democratic systems such as China and Russia itself being the worst offenders) and worldwide hatred, conflict and violence.
The sooner we advance away from this completely unnecessary and destructive type of human organisation the better; and lest this be misunderstood it is quite the opposite of a call for worldwide government, but rather for peaceful and non-sectarian types of administration.
“Crudely, for Russia the war is a necessity.”
In what way was it necessary for the largest country in the world with over 6000 nuclear weapons and a massive conventional armed force to invade its relatively tiny neighbour?
Also, and to return to your first point, in the case of Ukraine the Russian regime has clearly shown that it certainly does (selectively) believe that the “nation state, with its traditions, its physical and economic integrity, is unreal”;
But for precisely the opposite reasons to my own.
“For Europe, a choice. An incredibly bad choice based on green delusion, vanity, hubris, but a choice all the same.”
I don’t support the use of armed violence but certainly do think that it is quite right for people throughout the world, including in Europe, to oppose Russia’s unilateral and brutal assault on Ukraine and not bow down before its blood-curdling nuclear threats, threats to invade other neighbouring countries etc.
On the Green thing you mentioned, one of the very few good things that might come out of this appalling situation is the dawning realisation that the Climate Change / Net Zero delusion has led to catastrophic energy supply problems and costs which in turn will hopefully lead to ditching the whole misguided project.
No, only for Russian imperialism.
Probably a silly question but why does the west want to weaken Russia? I have never understood why from the moment the old Soviet Empire collapsed, we did not do all we could to make Russia an ally, forge alliances with Russia and include that country in all that we do. Russia has a tradition of art, culture, literature and music much aligned with the rest of Europe, there was and in my view still is, the chance to get Russia inside the tent with us, not outside the tent throwing bricks at us.
Why have we made Russia an enemy when we could and possibly still can, make it a friend?
I fell in love with Russian art, literature, music, architecture etc at an early age, so much so that I visited the country at the turn of the century – the trip of a lifetime! Incidentally Tolstoy was and is one of my greatest literary heroes and as a staunch advocate of non-violence will be spinning like a propeller in his Yasnya Polyana grave at the current situation in Ukraine.
In any case I don’t believe that any significant forces in the West wish to weaken Russia per se but rather to undermine both its current military aggression in Ukraine and ward off any possible future imperial expansionism.
There is also a sympathy for the much oppressed population of that country and quite correct desire for its currently brutally tyrannical regime to be replaced by a multi-party liberal democratic system; of exactly the type that was being established in Ukraine and causing the Putin government so much worry that it might inspire its own population to call for similar constitutional change.
LOL! Russians can sort their own Government out without the ‘help’ of the USA or the UK…or any numpties from the ‘West’..what on earth gives you or anyone outside of that country the right to think about any form of regime change?
Ukraine was being nicely established as an American/CIA proxy state….it will be lucky if it doesn’t end up as a mini-Syria, or Afghanistan, the way any country that America gets involved with ends up.
What a load of twaddle to excuse American Imperialism….
LOL! Russians can sort their own Government out
Anyone in Russia who attempts to challenge the government, promote liberal democratic reforms, campaign for an alternative to President Putin etc faces harassment, beating (see eg Pussy Riot and the Cossack militia), arrest, imprisonment (eg the hugely courageous Alexei Navalny), or murder.
So the word ‘can’ seems somewhat misleading here.
without the ‘help’ of the USA or the UK…
All human beings on this planet have both a right and duty to offer sympathy and moral support, where appropriate asylum etc to those suffering under the jackboot of oppression (eg currently in Russia, China, Iran, Saudi Arabia etc).
what on earth gives you or anyone outside of that country the right to think about any form of regime change?
Please see the above. If I was alive during the 1930s I would also wish to see the similarly brutal and tyrannical Nazi regime replaced with a multi-party liberal democratic one (ditto the USSR, Italy etc).
Incidentally the use of the term ‘regime change’ here can be misleading, I am certainly not encouraging or supporting any sort of violent intervention but rather moral and practical support for peaceful pro-democracy campaigning.
Ukraine was being nicely established as an American/CIA proxy state…
The Ukrainians themselves have made it crystal clear via the ballot box that they wish to move forward to a western-style liberal democratic setup, and were far advanced down that route when President Putin decided to try and put a stop to it.
.it will be lucky if it doesn’t end up as a mini-Syria, or Afghanistan, the way any country that America gets involved with ends up.
There are nearly 200,000 Russian, not US, troops in Ukraine (though I understand the Russian forces have taken heavy casualties, something which I completely regret. My opposition to armed conflict is based on sympathy for all those caught up in it)
What a load of twaddle to excuse American Imperialism….
Again the naked expansionist imperialism being displayed in Europe right now takes a Russian, not American, form.
Imagine all the people, living for today…you hoo.. could say I’m a dreamer, but I’m not the only one……..I hope someday you’ll join us, and the world will live as one!!!
ah, my favourite bit of the banter….the faux-shaming part ..”if you don’t think the same as me you don’t care about these poor people….” Well I also care about the poor starving Syrians, who still have the USA illegally occupying part of their country and stealing their oil and food…I’m sure we are all learning the ‘good democracy’ lesson from that…?…and maybe America’s goading of China is just because they just want to spread that darn democracy so hard!!?
In the latest poll I saw the Ukrainians very clearly blamed their own Government, the USA and NATO in massive percentages for where they find themselves now…I mean we could ask them, but unfortunately all the opposition parties and media who might have told us what they really want (rather than the Elenskyy propaganda) have been banned, so we will never know…I mean no one is allowed to voice the slightest bit of opposition are they?
In fact that doesn’t seem very democratic does it?
I don’t recognise the Russia or China you describe…which isn’t odd because it’s the West’s cartoon version…you’ll be telling us they still have foot binding next…..you are welcome to pretend to believe it…..
ie resistance to its threatened imperialism.
Sucked from your thumb.
You present a load of twaddle to excuse Russian imperialism. Oh yes the Russians are really sorting out their government, eh, with all their democracy, free press, right?.
Ukraine has willingly befriended the West and US, and can sever the link at any time. That that is not imperialism by any stretch of the imagination. Unlike, say, military invasion.
Putin has authorized the use of chemical weapons and murdered British citizens in Britain, demonstrating complete contempt for international treaties, agreements that he has signed.
We know from his own agencies that his expansionist adventurism planned to move on to Moldova after Ukraine.
How far should we let him go?
On that note, so has the British establishment through its ongoing support for clearly damaging vaccines. None are innocent. Putin serves a purpose as the west’s current focus of evil. The Salisbury poisoners were totally inept, bumbling idiots, leaving behind an easily followed trail a mile wide, when it came to doing a relatively simple but horrific job…”All you had to do was one thing…” Actually, it was so inept that I sometimes find myself thinking that it was all a set-up. Who knows what to believe these days…
The British government has destroyed so many British lives over the last two years.
But they have not breached the Chemical Weapons Convention to which they and Russia are both signatories.
The British government are, however, in breach of the Budapest Memorandum guaranteeing Ukraine’s territorial integrity to which they and Russia are also both signatories.
That is why we are helping Ukraine to restore their territorial integrity.
A trail just round the corner from the local chemical weapons place as well. No shortage of relevant specialists on that occasion. That said, much of my interpretation of it all at the time was via BBC News and the G.
It was the same stuff, Novichok, that they used on Navalny’s underwear, which they inadvertently admitted to in a recorded conversation.
Alles klar.
One word: money. I too thought along similar lines of thought to yours and for a brief moment I felt it was happening but then of course the invisible hand of not-god intervenes because you can’t make any serious money out of peace and stability. You need endless crises and conflict because that’s what makes money.
Unadulterated drivel. Making armaments that get blown up only helps the few that make them, everyone else is poorer for it.
It depends what you mean by “the west”. There are quite a few western organisations that do actually co-operate with Russia for some things, such as the GLONASS product as an alternative to the American GPS for satellite navigation. Some products can use either of them. And don’t forget about the International Space Station – at present, Russian rockets are the only mode of transport there and back.
Wholeheartedly agree. After all that the Russian people went through in the Second World War and considering we were on the same side why have we allowed this war to even start?
I detest and utterly despise the deep state yanks for igniting the conflagration and my contempt for the evil that is Bozo is off the scale.
I greatly admire Russia and its people. This ridiculous war saddens me greatly.
There’s a slight misunderstanding here: You were fighting on Stalin’s side in WWII, enabling him to export communist revolutions to all of eastern Europe after large-scale ethnic cleansing and devastation (lasting to this day) of formerly flourishing landscapes in order to fullfill the old Russian political goal of erecting a Russia-dominated empire of all slavic people in this area. He never fought on yours.
Yes, why did Russia start this ridiculous war ?
Purely because of its rampant imperialism.
We could have when the Soviet Union was dismantled by Gorbachev. I doubt if we could now.
To not try to get Russia on board with the west was one of the most inexplicable foreign policy blunders in my lifetime. We were giving money to everyone at that time (didn’t we bail out a bunch of Asian banks?), and could have helped Russia have a softer landing after their collapse, but we didn’t. The Russians witnessed how we (and by we, I mean the USA) rebuilt Europe after WWII and how Germany was rebuilt and welcomed back into the fold. We did nothing like that for Russia. That enabled despots like Putin to gain power.
I suggest wearing of high-priced Chinese imitations of US medical masks produced with no quality control whatsoever but copying the general shape to counter this horrible threat. And schools must immediately be closed to Protect the Children[tm] until a gene-engineered proxy war vaccine has been developed and widely applied. Nobody’s safe until everyone has been punctured!
Russia has an extremely simple way to stop being battered by this proxy ram which is so ruthlessly efficient that it couldn’t stop Russia from occupying large swathes of Ukrainian territory and that is Cease hostilities and withdraw. This will cause the devious NATO strategy of getting proxy-invaded by means of Russian surprise attack on Ukraine to unravel very quickly.
It’s pretty clear what the goal of the Ukrainian people is:
‘ there are enough sabotage groups in the city and every week they blow up the cars of Russians. We had to remove reg plates from our car and check underneath it every hour, walking in the city alone is strictly not recommended. An open pro-Russian stance in Kherson today requires either real courage or desperate recklessness’
Rusich 05 Sept 22
Britain and the U.S. are both signatories of the Budapest Memorandum guaranteeing Ukraine’s territorial integrity.
It would seem that those goals are in perfect alignment.
What is it with you and the bloody Budapest Memorandum? You cling to it like crap to a blanket!
Unlike article 5 of the NATO charter it does not require a specific response from any of the signatories…..
It is an agreement, not an official treaty..it’s neither legally binding nor does it carry any enforcement mechanism…
So what’s the big deal?
Interestingly though one of the points in the Memorandum that the signatories re-affirmed was the fact that they would refrain from ‘economic coercion’…..??
Since 2014, when America usurped the legally elected President, they have given Ukraine in excess of $12 billion..for various reasons but also…’to improve its interoperability with NATO’ (but it’s no threat to Russia..LOL)
Since 2014 the EU have given over 5 billion pounds to Ukraine….?
Between them Cargill, DuPont and Monsanto own agricultural land in Ukraine the ‘size of Italy’…17 million hectares….(Shareholders include..Blackrock, vanguard and Blackstone!)…..
It might just be me but all that seem pretty much like economic coercion!!?
You advocate Britain joining Putin in reneging on international agreements?
The Chemical Weapons Convention has no ‘enforcement mechanism’ either.
There is a great deal of Putin’s largesse swilling around Europe funding oddballs and their dotty little organisations.
I wonder if any of it funds so many of the crude, hopelessly batty comments on here?
What’s the big deal about agreeing to respect borders?? Nothing wrong with some recreational imperialism eh? You just can’t imagine the similar fuss in 1939 I suppose.
Like military action, refraining from economic coercion was ruled out. So if one side breaks the agreement, the other side must just lie back and welcome the rape? Is that what the Memorandum says?
Neither America nor anyone else ‘usurped’ the Ukrainian president. He fled after widespread popular disgust with him expressed by peaceful demonstrators, many of whose assassinations he and his Russian pals organised.
And Yes it is just you – buying land is not ‘economic coercion’.
It’s a war against Russian imperialism, not Russia. There have been no attacks on Russian soil.
And from the outset the big fear was always a nuclear response by Russia to any decisive fightback.
Russia entirely brought this on itself, and can end the crisis immediately by returning its troops to Russia.
Adam Schiff is a Congressman, not a Senator.
As a congressman Schiff earned a reputation for flat out lying about the Russian collusion hoax by repeatedly promising to have damning evidence against Trump that never actually appeared.
If you can’t get the basics right, there’s not much of a foundation for the remainder of Noah’s arguments.