
There follows a guest post by an NHS Emergency Department doctor on what, from his frontline vantage point, is behind the current hospital blockages and ambulance delays. This article first appeared on the website of the Health Advisory and Recovery Team (HART), a group of experts offering a second opinion on COVID-19 policy. Sign up for updates here.
As Emergency Department doctors, we were always going to be on the frontline. In spring 2020, we were taken to one side and it was suggested we might have to say goodbye to our relatives for the foreseeable future. Few realise the fear generated in hospitals in 2020. As Emergency Department consultants we were put on 24/7 emergency shift rotas and provided with vacant hotel rooms to live away from our families for their protection. Many of our colleagues left us to it and, soon after, patients arrived showing us signs that had been put up on their GP’s door saying “closed due to the pandemic”.
Spring 2020 saw a combination of assessing and treating sick patients who had unusual and characteristic presentations of Covid in an otherwise quiet Emergency Department. The less-sick patients queued in their cars for assessment in the rapidly delivered ‘Covid-pod’. Huge hospital Covid signage was hastily erected. Doctors were redeployed to work in the Emergency Department from other specialties that were literally cancelled or scaled back hugely. I had one come to me at midnight asking why there were twice as many doctors in the place as patients; that he was bored and hadn’t seen a patient for three hours. Pre-lockdowns we were seeing over 300 patients each day. During the lockdown madness this dropped to less than 100 on some days. Many patients were petrified at the idea of coming to hospital. Others were instructed to stay away from the hospital unless extremely ill. This went on for months. Then the patients gradually came back, some with essentially no other access to healthcare. The department has not been quiet for some time now.
For many years now, my department (as with others throughout the U.K.) has been used as an overflow ward when beds cannot be found in the main hospital. Currently this is happening to an extent I have never previously experienced. A shortage of beds has been an issue for at least two of the three decades I have practised emergency medicine. It gets worse every year. The causes are multifactorial, but can be related to reduced numbers of beds or staff, decreasing access to community care, increasing waits for specialist referral and an elderly population whose primary (sometimes only) source of medical care is an emergency department. There is a major problem at the community discharge interface with patients waiting on packages of care, step-down wards, community beds and nursing homes. This exacerbates the bed cuts over the years and the centralisation of specialist services. I have heard of a hospital where one man will likely see his third Christmas as an inpatient. Patients are staying longer, and a lot are dying in hospital. These problems have just been exacerbated by ‘Covid Rules’, segregating the ‘Covid exposed’ from the ‘Covid recovered’ from the ‘Covid test positive’ from the ‘Covid test negative’ patients.
Emergency Department clinicians battle this with increasing frustration as the result is people essentially living in the department. Our department is back to seeing over 300 new patients per day and on one day last week we had over seventy patients living here awaiting hospital bed placement. Deaths in the department are increasing because sick people are remaining in the department for increasing lengths of time. The hardest bit is those needing end of life palliative care that get it delivered in the mayhem of an emergency department. It is very distressing for patients, staff and relatives.
Emergency departments operate as an outpatient interface between hospital and community. In the U.K., about the turn of the century (2000), most acute hospitals changed their admission arrangements from a GP referring to a specialty bed to a ‘single portal of entry’ arrangement. It was shrouded in the ‘safe and effective’ argument, but was a disaster on many levels. GPs no longer decided on admission; they decided on sending to the Emergency Department to decide on admission. The emergency departments were pulverised with a ‘four hour target’ for admission (under Blair’s Reforming Emergency Care). The media blamed emergency departments for ‘failing’ to meet the four hour target when, in effect, they were looking after the patients needing beds as well as serving emergencies.
The proper work of an emergency department is that of unscheduled care – people sourcing help in an emergency. The greater volume of work now is ‘processing’ admissions for inpatient specialties that don’t have beds for them. The Emergency Department is then expected to look after them, providing ward-level care (and sometimes intensive care) in corridors and rooms until a bed is available or they have been discharged (or left for heaven) from their Emergency Department trolley. (We have beds with hospital specialist mattresses for pressure sores in our corridors because of the long stays.)
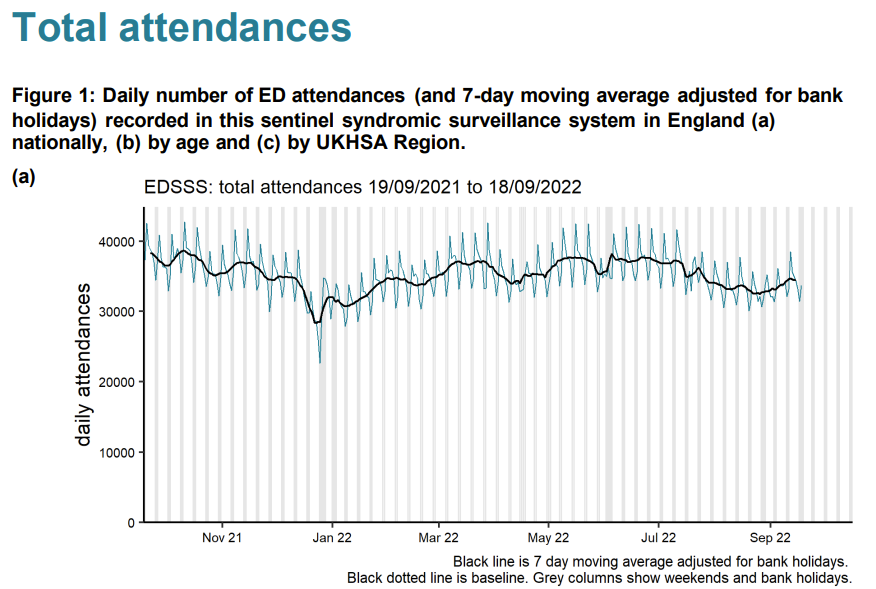
So, to say the numbers of admissions to emergency departments are lower than they were in the summer (as they currently are) gives no picture of the real congestion in emergency departments. You need to look at the number of patients waiting for beds. We are used to winter pressures with peaks and troughs. In 2021 we averaged 25 waiting in the department at a time (for at least a day) with no summer let-up. This year, for the same period, it is 45, with the worst summer ever. Emergency attendances are down – but admitted patients living in the department for days are more than doubled.
That aside, we have robust triage systems (stretched to the limit) where conditions that must be treated promptly are picked up within a target of 15 minutes of arrival (heart attacks, strokes, sepsis, haemorrhage etc.). The system is not perfect, but essentially these patients are identified as ‘time dependent conditions’ and brought to the Resuscitation Room for immediate assessment. Some are flagged by the Ambulance Service as ‘stand-by’ calls and sometimes paramedics take patients directly to where they can have, for example, urgent cardiology treatment to minimise damage from a heart attack. On the other hand, I am well aware of the recent problems with extensive delays in ambulance response times for some patients and occasions where the prioritisation has gone wrong.
Time-dependent conditions are being managed in the same way we always have and therefore perceived delays in managing them cannot be assumed to be contributing to the recent uptick in excess mortality. It is clear from experience that the incidences of heart attacks and strokes have increased significantly, although it will take time to demonstrate this with data.
I have thought about what could be causing the excess mortality we have been seeing. With regard to ambulances in particular, there are many factors involved and it is difficult to quantify which is the greatest as the data are simply not available.
1. Ambulance staffing
Ambulance staffing has been an issue over the last two years. Paramedics have taken massive ‘Covid’ leave over the last couple years. As with hospital staff, any persistent cough (pre-testing), any positive test or even a contact with someone who had tested positive and you were expected to take 10-14 days off too. Any paramedic deemed ‘vulnerable’ would stay off too. The net effect of this was fewer paramedic ambulances on the road. We had private ‘ambulances’ including St. John and Red Cross supplementing patient hospital transport. That was a major factor, but is becoming less so now as there are fewer infections, and ‘Covid’ leave becomes sick leave again.
2. Hospital Chaos
A fear of accusations that hospitals had been responsible for spread of disease meant there were over-zealous systems of separation put in place. Patients were cohorted in the Emergency Department awaiting classification: PCR-positive, PCR-negative, Covid-recovered, Covid-exposed, clinical-Covid without a test result etc. These patients could only be admitted to a ward bed if there was one available in their category. This problem was compounded with ward beds being closed for ‘social distancing.’ Covid rules meant if a patient needed resuscitation it was done in the only (tiny) negative pressure room in the department.
Patients were kept in ambulances until a separate room in the Emergency Department could be found because the whole department became organised around one disease. It was not uncommon in certain trusts to have your first 24 hours of hospital treatment in the back of an ambulance. Some hospitals would not count the time in the ambulance as part of the patient’s hours in the department, meaning there was a perverse incentive to keep patients in ambulances.
3. Community Chaos
For those that haven’t noticed, for many, general practice now consists of a telephone triage service and a ‘vaccination’ service. For a lot of people that means their only source of healthcare is the Emergency Department and their only way of getting there is an ambulance. Where previously a nursing home may have had GP visits, now problems are dealt with by calling 999.
Despite this, there have been fewer patients overall attending the Emergency Department in 2022 than the equivalent period in 2021 (which was massively up on the empty departments of the lockdowns). Unfortunately, the patients are much sicker, older or simply can’t endure having formal investigation of a complex problem postponed further. Each of these patients requires more time and stays longer. We have the same amount of staff to deal with the 300 new presentations whether the department is empty or has over 70 living there. Our Emergency Department had it as a ‘never event’ to keep a patient in an ambulance, but recently we have been overruled by the pervasive ‘Infection Control’ who now dictate who can come in. An ambulance being used as a holding bay is an ambulance that can’t be turned around for another emergency.
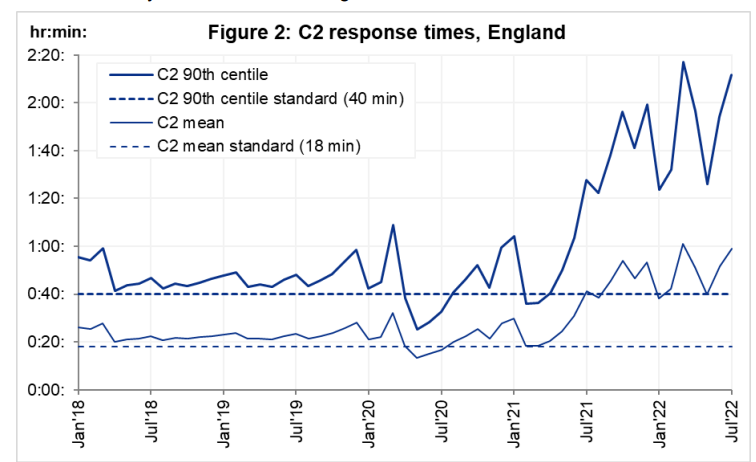
Ambulance wait times started rising from July 2021. This was when ‘Freedom Day’ from the winter Covid restrictions finally arrived and at that point patients had had enough. There was a massive upswing of hospital presentations (accompanied by perhaps a little guilt at how the elderly had been managed) and in came the patients. A proportion of these patients were victims of having not had healthcare in lockdown. For example, I recently saw a patient who had a dangerously swollen abdominal aorta – an aneurysm – which had reached a size where surgery was needed to prevent rupture and death. Surgery was cancelled twice resulting in a re-attendance at my department after it catastrophically and fatally burst.
However, it has been many years since I have seen this number of patients with heart attacks and strokes. The timing of the uptick has coincided with the vaccination programmes. Correlation is not causation (unless it fits the narrative of course). Yesterday, I saw a superbly fit young man with no cardiovascular risk factors who had had two previous vaccinations. Despite healthy kidneys he had a cardiac cell death test result through the roof (troponin of over 800) after having chest pain while exercising. I worry that the spike protein or other factors have caused damage to the blood vessel lining cells such that exercise is precipitating spasm or rupture of plaques in coronary arteries leading to heart attacks. There are too many professional and amateur athletes now getting acute myocardial damage post-inoculation for it to be a complete coincidence. And it seems to be an effect unfortunately that can persist for many months after the injection. We are allowed to talk openly about the consequences of lockdown on health but not about potential consequences of the vaccines.
The pressures on emergency departments are therefore multifactorial. They stem from changes in how patients are referred to specialty care, the role departments have taken on as an overflow ward, and the additional constraints brought in with Covid rules. However, on top of these issues, the sicker patients we have seen, even in summer, have caused catastrophic pressure on the system. The knock-on effect is ambulances unable to drop off their patients and not being available for calls such that ambulance waiting times have rocketed. There is only so much we can do as emergency physicians. What is really needed is a sustainable fix for these underlying problems.












To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
I wish I shared your optimism, Toby. The next indignity seems to be the imposition of face masks. It feels to me like a humiliating badge of compliance.
Even under lockdown and social distancing, no one can tell that you’re actually ‘going along with it’. Conceivably, at any time, no one really knows whether you’ve been out for more than an hour, or even twice that day; they don’t know you’re not going to buy something non-essential at the shop. They don’t know whether you clap at the appointed hour on a Thursday night. These are tiny slivers of freedom and dignity to cling onto.
But impose face masks, and your compliance – and shame – is unambiguously there for all to see. Not only do you have to wear the masks, but you’ll probably have to source them yourself – The Sun is even giving instructions on how to make them. Perhaps Lockdown Sceptics could have some made with an image of Neil Ferguson on them. Alternatively, perhaps, we should make them look like disgusting health hazards with apparent flakes of skin, blood and pus stains on them.
Or we could just refuse to wear them. I will do just that
Seems increasingly likely doesn’t it, just to ratchet up the fear levels another notch. Plod are going to thoroughly enjoy themselves enforcing that one.
Agreed, non compliance will be a badge of honour in my mind
And I’m not accepting their vaccine either no matter what, no matter, even if I’m excluded from society for the rest of my life, it’s just not happening. These people are not trustworthy and their exploits in India have me convinced of this. Not happening.
Amen!
On an attendant note – and no, I will not wear a face mask – what is all this bull about essential items? As far as I understand it if an item is on sale you can buy it. And that comes directly from a government that can’t really do joined up writing. It’s the Plod (not the brightest profession in the world) who have mostly mentioned non-essential items, conveniently forgetting that there isn’t a shortage of anything (well not much) and there is no rationing. And how the hell would they apply that ‘so-called regulation’ to shopping online?
Facemasks are no indignity, I will agree to wear one from the moment they decide to switch to facemasking instead of all the indignities caused by lockdowns, loss of our rights and loss of our jobs. I suggest we make a priority of removing irrational measures like lockdowns and dangerous police powers, replacing them with non-intrusive but effective measures like face masks, wash basins, open windows instead of air-con, copepr plated door handles and more regular public transport to reduce crowding is the right step to take.
Wearing a yellow star was considered non intrusive in 1939
Firstly, everyone would wear facemasks, they wouldn’t be of “yellow star” type use to mark out those a government wishes to oppress. Secondly a facemask is also a useful defence against facial recognition surveillance cameras, quite good for making state intrusion trickier for them. Unlike a yellow star beng used to track you a facemask makes tracking harder. We need to be willing to give ground on minor things like facemasks, things that actually hep make a difference but don’t restrain our important rights, in exchange for making the forces of government give ground on the intrusive measures, make a deal of it, we will take every reasonable precaution to stop the spread, as soon as they stop forcing unreasonable precuations upon us. We have to show that our way is effective and workable without needing their intrusion, that way mroe people will come to see the sense of our anti-lockdown, pro-liberty, pro-business cause.
When would the enforced face mask law be lifted? The one that says that a person when outside the home needs to cover their face, even when walking alone in the countryside – because if we make it optional or common sense, some people will take them off when sunbathing in parks and that wouldn’t be ‘fair’.
If it’s just a ‘minor thing’, why would that rule ever be lifted? At any time there could be a new virus with pre-symptomatic shedding, so it would pay dividends for people to have to wear face masks all the time – even in the home come to think of it.
With regards to facial recognition, there’s no problem because each citizen could eventually be issued with personalised bar-coded face masks.
If face masks are made mandatory for certain activities, and it proves impractical in some circumstances not to comply, a design of protest face mask would be useful. At least people could feel like they have stated a view and are not simply endorsing the rule.
Suspect facial hair might be in vogue, as we know it makes face masks virtually useless!
Will masks be required ‘in the bedroom’ (asking for a friend)
Dark glasses might me more appropriate in my case
Read Dr John Lee’s article on this subject in the Spectator.
He contends that even surgical grade face masks are designed to filter bacteria – not viruses, which are typically ten times smaller.
A cloth face mask has pores in the weave that are 1,000 to 5,000 times larger than a typical coronavirus – pretty much an open door to them.
Masks do almost nothing to protect you, but they do ensure that if you catch it then your breath, the spit while you talk and your sneezes coughs travel less distance. They let us mingle in society (with basic 2m social distancing) in a way which makes viral spread a lot trickier, as particles (the virus clings to saliva droplets far bigger than the viral particles themselves) travel a lot less distance if a mask slows their exhaled velocity first. Facemasks are a good alternative to lockdowns.
Being forced to wear a mask would be the final straw for me and I would refuse too. Besides if they can’t find enough for the NHS where on earth do they think we’re going to find them?!
Hi Paul,
I understand your frustration. I thought the same. But after, I read an article somewhere. A doctor said that my mask protects others and their masks protect me. So my mask is not for me. It is more for anybody else around me.
For me, it was a reasonable argument.
If I get the choice, masks or lockdowns I pick masks. We need to be clear that in resposne to lifting lockdowns we will take the sensible health pre-cuations necessary, this is a good offer to negotiate with. You end lockdowns, we wear masks. You re-open all the pubs for takeaway service, we wash our hands even more often. You re-open our jobs, we’ll use some spare time to deliver food to the old people who might actually be at some risk if they caught the disease. And so forth, for each intrusive measure the government removes, we accept a non-intrusive one.
Thank you Toby for your brilliant research and journalism. This website gives us all hope and shows that not everyone is paralysed by fear and led by an irrational response.
I still can’t understand why Neil “Haven’t Got A Clue” Ferguson carries such weight in government decision making. His track record is nothing short of abysmal! The man has no understanding of the importance of the economy nor the non-Covid healthcare crisis this totally unnecessary lockdown is creating.
Would happily mount a campaign or petition to get him sacked/removed from his position for his indeed abysmal track record.
I am constantly looking for a campaign/action group but this is the only page I am a member of right now. I am a lawyer/teacher and writer and would happily protest in the streets (but of course the Coronavirus Act makes this illegal (unlike the Civil Contingencies Act which we chose not to use). Are there any organised protests in the UK?
I have never in my life considered protesting but would strongly consider it now, unfortunately I have no idea about how to go about it and am not aware of any groups, Reddit might be a good place to look. Convenient that it should be made illegal, however I am almost at the point of not caring because it will generate attention.
I remember some time back there was a website trying to organise a protest in early April against the lockdown and it got taken down pretty quickly
If the Americans can do it, why can’t we?
P.S. If anyone wishes to make their thoughts on Professor Ferguson’s “model” known to him personally, he is on Twitter: @neil_ferguson
Toby, your updates are extremely helpful. In my view, the single most mendacious aspect of the globally adopted propaganda here is the use of deaths “with” as opposed to deaths “from”. The distinction is drawn parenthetically (occasionally), but my understanding is that the degree to which this is misleading is proportional to how widespread the disease is. If 50% of the population has it, one would expect at least 50% of deaths to be part of the rising “Covid-19 death toll”.
I believe the solution (for the UK, at least) lies in simply looking at the year-on-year comparison of deaths whose underlying cause is respiratory disease. These have been recorded for ten years, and, as I understand it, must include all deaths that were actually caused by Covid-19. ONS will release w/e 10th April tomorrow, which will be interesting because there definitely was a spike w/e 3rd April (week 14), and how that spike continues will give a good idea about true excess mortality. The numbers lag because they are by date of registration, so not only is the availability of data a week behind, but also the deaths that it describes may be up to two weeks old.
However, at at the end of week 14, the total number of deaths from respiratory failure (which we have to assume includes those actually caused by Covid-19) was 25,012. At the same point in 2018, the figure was 31,659.
It may be that we do see a significant spike in the coming weeks, and that 2020 starts to compare with, or even exceeds 2018. If we do see that, the conclusion would be that the effect on mortality was slightly worse than a very cold winter.
I have been producing the graphs each week (as have others, e.g. https://twitter.com/hector_drummond/status/1251177611100913664 and https://twitter.com/hector_drummond/status/1251176564051640320). I think it would be great to include this in your next update.
Thank you so much for your calmness and rationality. I am baffled at the country’s reaction to this. How can we get this data out to a wider audience and/or organise a protest on this?
A very big daily thank you Toby for your work.
If nothing else, it’s reassuring to know that there are others who question this crazy approach taken by our cowardly government.
I’m off for a longish walk than usual this afternoon. This is following the new interpretation of the guidelines, that as long as I walk for longer than the drive to it then I’m fully compliant.
I’m wondering how far I can stretch things? Its a 9 hour round trip drive to the Lakes for me, so as long as I walk for 9 hours and 1 minute then I’m good! A trip to Scotland maybe pushing it a little though …
On the subject of IFR, has anyone heard any results from the Porton Down antibody survey?
On 3rd April Matt Hancock said (note past tense “We have already”): “Yes, but I’m not assuming any come on stream – that’s pillar three, as we call it – in order to hit the 100,000 target. We have already 3,500 a week of antibody tests at Porton Down, and they are the top quality, the best test in the world. We’re using those for research purposes to understand how much of the population has had coronavirus. This is one of the great unknown questions. But that’s obviously a very small number, 500 or so a day.”
Anyone got any idea why the Porton Down laboratory has the Health Secretary listed as a 75% of more shareholder?
I walked to and along Poole & Bournemouth promenade yesterday, definitely a good deal more people, cyclists and cars about than a week previously, Easter Sunday. In the absence of much evidence of Covid in the local Dorset area, suspect many are beginning to suffer from Lockdown fatigue. Guido reporting increasing incidence of anti-lockdown demonstrations around the World. As ever (see Brexit and ‘Climate Emergency’ the noisy woke, the MSM, ‘celebrities’ and social media jockeys give the impression that the vast majority are ‘on board’, I suspect (hope) the level of cynicism is underreported.
Update, I just took a sunny, late afternoon drive around the Sandbanks peninsula, it wasn’t essential, I didn’t need to or have to, I just wanted to, for my own pleasure. Felt good.
Sounds to me like you didn’t actually encounter any other human beings, hence no risk of spreading in either direction. No civilised person could comdemn you for those actions. I wish this text field would let me underline the word “civilised”, today I define it to mean any person who can understand statistics and respects that a risk of death always exists hence quality of life is more important than quantity.
There is some racial data for the UK. According to the Guardian, nearly 25% of patients critically ill are Asian or black, versus 16% for black and Asians in the general population. For the at-risk age group, that 15% is much lower. I doubt if it is Vitamin D. It is far more likely to be obesity, diabetes and hypertension, all of which have significantly higher incidence in blacks and Asians than whites and all of which increase the risk of COVID. There may also be genetic disposition, particularly around ACE2 in the lungs. I have heard (but seen no data) that the Somali population in Sweden is disproportionately affected, and may be in London too. I note that the UK has the largest Somali community in Europe.
Doesn’t it just reflect the ethnic composition of London, where most of the cases are? London has a majority ethnic minority population. Plus poverty and high density living I imagine.
Hi Phoenix44
Re effects of covid on Sweden’s Somalis, Go to BMJ link in Young’s blogabove.
ATB
Here are 53 measures we can take right now to end the lockdown and reopen the economy and public life while continuing to limit the damage COVID-19 is doing: https://medium.com/@codecodekoen/covid-19-53-suggestions-for-reopening-the-economy-in-a-responsible-way-f8616bb2cf83
I have written to my MP to advise him that I will not accept the shutdown for my age group till 2022. I am a fit pensioner at the moment, and dread to think how I would survive or not if this length of time was imposed upon me. Among my friends the fear factor is running very high at the moment and I am worried some may not be able to last such a long period of time in lockdown. I am very positive regarding this virus, I will not let it beat me or worry me but unless the Government change this plan many elderly will worry themselves into an early grave.
Christine, I do hope your MP has the courage of conviction to accept and represent your point of view. The emotive rhetoric surrounding this “deadly virus” seems to have been engineered so as to discourage any form of critical thought or rational discourse.
There was a move at the start to adopt a measured and proportionate approach to tackling this “crisis” with the aim of building a “herd immunity”. Unfortunately, that gave way to an irrational knee-jerk response that has only reinforced the herd mentality.
You may wish to check Fumento’s points a bit more carefully yourself before citing them, as the points you’ve pulled out contain serious errors or mischaracterizations of what was written in the papers. To pull out a couple of examples:
The paper citing 1.4 million deaths for Ebola stated that it was for *four months* of uncontrolled or unmitigated behaviour and multiplying by 2.5 to estimate for unreported occurrences and used this as a justification for taking countermeasures and the importance of putting mitigations in place as early as possible. A few sentences after the 1.4 million figure, it goes on to say “The cumulative number of Ebola cases for Liberia and Sierra Leone could double to approximately 8,000 by the end of September 2014”, which is somewhat closer to the 8,000 you quote and something of a justification of the model.
The error with AIDS reporting is even greater; the 17,325 cases in 1993 is from https://www.researchgate.net/publication/8010413_Migration_and_AIDS_in_Mexico_An_overview_based_on_recent_evidence and is actually the number of cases in Mexico, not the United States which by mid 1993 had 315,390 cases. It’s difficult to understand how such a fundamental error was made in the first place and is not the kind of error made in a “particularly good” article; you may wish to raise your quality threshold somewhat.
The point made, though, is a good one and still stands:
‘Use and abuse of mathematical models: an illustration from the 2001 foot and mouth disease epidemic in the United Kingdom.’
‘‘The progress of an outbreak of FMD is extremely difficult to predict in the early stages of the disease. The course of an outbreak can be critically affected by minor and inherently unpredictable events, such as a single livestock movement. For this reason, predictive disease models, which depend on statistical probabilities of transmission, have not met with much success in predicting the spread of FMD from herd to herd, and still less the impact of
control measures……….’
‘The UK experience provides a salutary warning of how models can be abused in the interests of scientific opportunism.’
https://europepmc.org/article/med/16796055
The point (or at least Young’s point which appears to be that models don’t work very well) doesn’t stand if several of the papers cited actually do make good predictions and the author is either deliberately misrepresenting them or has made a mistake so inpet that they’ve confused the USA and Mexico and *still* doesn’t spot it after seeing the absurdly low resultant infection rate. Even if you don’t like Ferguson’s work, the vCJD deaths that occurred are inside the 95% confidence interval of the paper cited in the article of 50 – 50000, the very high CI is the reason that the second sentence of the abstract says “well grounded mathematical and statistical models are therefore essential to integrate the limited and disparate data” which Young & Fomento have missed, as well as the lower bound number completely and not taking into account that it was even before any bovine to human transmission had been detected at all.
There may be things to criticise in the COVID-19 modelling which can be done by criticising the actual models, starting parameters or the maths themselves, which Young doesn’t do. Picking out a policy failure aruond FMD, an animal disease, from nearly two decades ago says nearly next to nothing about the current situation. Yes, predictive modelling in the early stages is hard as they’re very sensitive to initial conditions and real world outcomes are affected by behaviour and policy changes. But the government has to have a policy response (even if that is a do-nothing, no-response) which if it isn’t guided by models is going to be guided by…what exactly?
“… the government has to have a policy response (even if that is a do-nothing, no-response) which if it isn’t guided by models is going to be guided by…what exactly?”
The 64 trillion dollar question. Maybe it has to be the result of rationalism, not empiricism. The ‘science’ doesn’t replace the need for judgement calls – it merely disguises or defers them. I don’t think it even ‘informs’ them when it is so obviously confused itself.
Sweden used cool, calm rationality in deciding that the disease would have to be a factor of ten worse than indications (possibly just anecdotes) were showing it to be, in order to justify destroying the economy and suspending civil liberties. One factor was, apparently, that they could see that a lockdown is a self-reinforcing strategy, making it almost impossible to come out of with any sort of coherent justification. Our government is now wrestling with this this problem, meaning we are probably going to have to trash the economy and society even further while the press and public are psychologically conditioned to accept a relaxation of the lockdown.
Government actions should, in a perfect world, always be evidence based. Evidence provides data, and data can be used for decision making. Models using accurate data can indeed provide useful decision support tools. The author’s point here is straightforward: models are inherently unreliable, dependent as they are on the quality of the data provided, as his referenced paper points out:
‘Then Fauci finally said it. “I’ve spent a lot of time on the models. They don’t tell you anything.” A few days later CDC Director Robert Redfield also turned on the computer crystal balls. “Models are only as good as their assumptions, obviously there are a lot of unknowns about the virus” he said. “A model should never be used to assume that we have a number.”
Which, of course, is exactly how both a number of public health officials and the media have used the them.’
The criticism of modellers is that they themselves are aware of the limitations of modelling but may not always be as diligent as they might be in making that clear:
‘The models essentially have three purposes: 1) To satisfy the public’s need for a number, any number; 2) To bring media attention for the modeler; and 3) To scare the crap out of people to get them to “do the right thing.”’
‘……all the modelers know that no matter what the low end, headlines will always reflect the high end.’
On a separate point, the fact that a paper may be 14 years old quite obviously in no way invalidates its conclusions, most particularly when it concludes:
‘The course of an outbreak can be critically affected by minor and inherently unpredictable events, such as a single livestock movement. For this reason, predictive disease models, which depend on statistical probabilities of transmission, have not met with much success in predicting the spread of FMD from herd to herd, and still less the impact of control measures……’
That point is particularly relevant to Covid 19. Covid 19 data is all over the shop. The virus could have crossed over to humans as early as 13 September 2019 or as late as 07 December. Testing has been sporadic and unreliable. Mortality rates are unreliable, since no international standard for recording cause of death exists.
Short of good data, as they are, to input into decision support tools, leaders have to exercise judgement; and democratically accountable leaders are extremely risk averse, with the honourable exception of Sweden, which has a health authority independent of political control. Hmmmm.
Democracy: the least worst system of government.
Good data is being gathered in the U.S. Hopefully we are doing the same. Then the able bodied can all get back to work, knowing that the risks we take with this virus are really no different to those we take every year with influenza:
https://www.youtube.com/watch?v=k7v2F3usNVA&list=PLq8BgDugd2oyqmYx6RdVlJfQeAdhJkhc3
I think we have been walked to this outcome for quite sometime. I am in no doubt the controlling powers are moving to complete population monitoring. We will no longer have freedom to buy and sell. Go outside or partake in any activity without the information being collected.
If you think back to the arrival of Alexa. In most people’s homes. The fact your phone listens to your conversations and targeted advertising appears amongst your social media. All this information is for sale.
This virus is without doubt nasty but the fear of it has been made much worse. The measures put in place to hasty and withdrawing them all I dont think will ever happen. You only have to listen to the WHO and the measures they want to take.
The rapid tell tale society that phones police re gatherings of people are doing the job for them.
I could go on. I will just say if you are not aware take a look at The Corbett report.com and the Last American Vagabond. Both put out great information on the USA and the rest of the world.
We cannot trust any death figures when they are being recorded incorrectly and the numbers will drop as the epidemic passes and the government change the recording rules to suit their message.