
I’ve written before about the World Mortality Database, compiled by researchers Ariel Karlinsky and Dmitry Kobak. It provides estimates of excess mortality for all the countries around the world in which reliable figures are available.
These estimates aren’t as good as the age-adjusted excess mortality estimates that the ONS has computed for European countries, but they’re the best we’ve got for making international comparisons. (The reason they aren’t as good is that they’re based on all-cause deaths, rather than age-standardised mortality rates.)
At the present time, estimates are available for 117 countries, comprising a large share of the world’s population. What do they reveal about which countries have done well and which haven’t, during the pandemic?
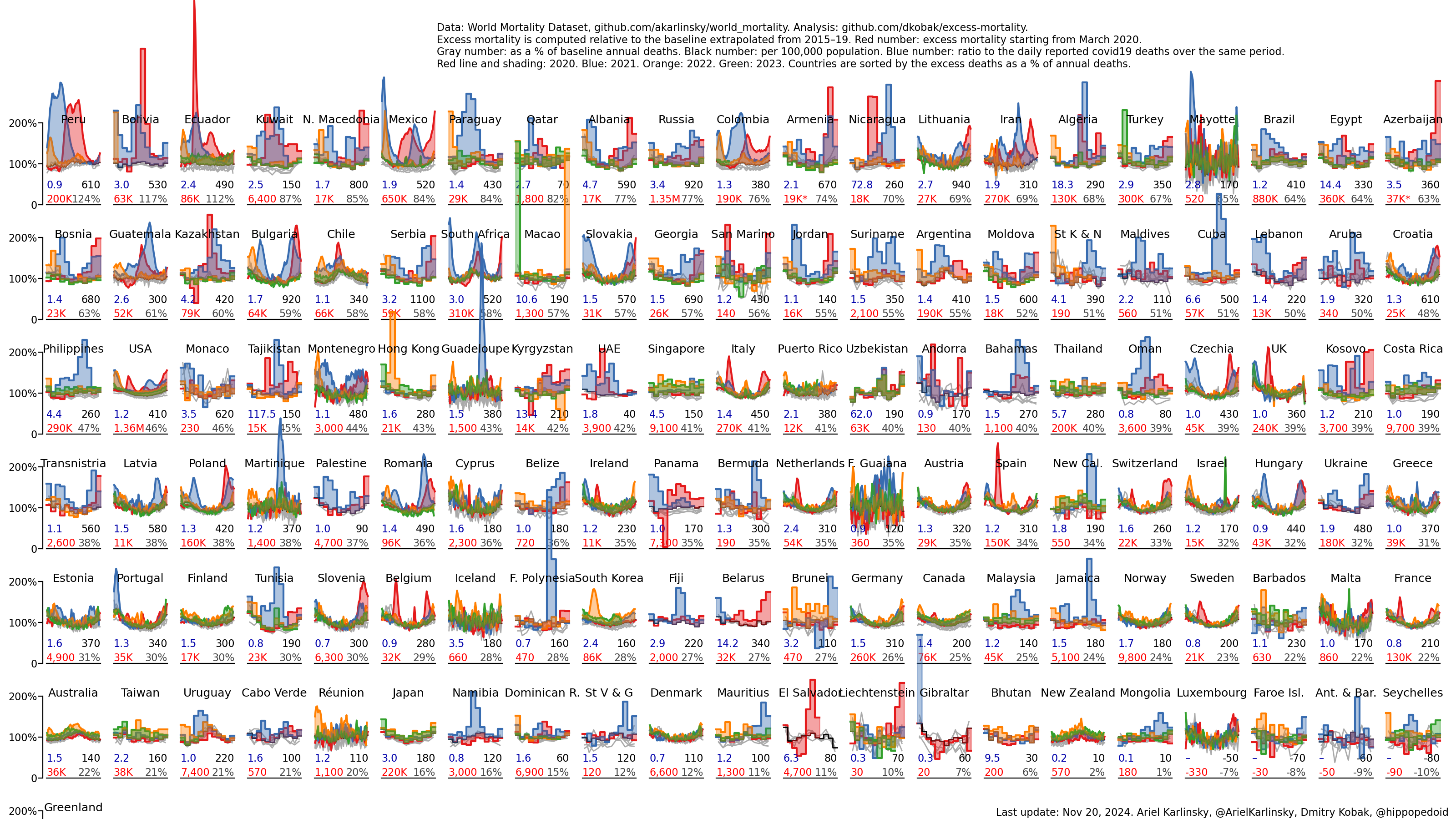
All the countries with high levels of excess mortality are in Latin America and Central Asia. And the top three – with exceptionally high levels of excess mortality – are all Latin American countries with large indigenous populations, suggesting that such populations might be particularly susceptible to Covid.
More illustrative, though, is the bottom of the chart. And here one thing really stands out: of the 15 countries with zero or negative excess mortality, no less than 14 are islands (the other being Brunei).
And of the 18 countries with 1% excess mortality or less, fully 17 have either one or zero land borders. The Dominican Republic only borders Haiti; and Brunei only borders Malaysia. (The exception is Malaysia, which borders Thailand, Brunei and Indonesia.)
After two years of lockdowns, mask mandates, and vaccine passports, it seems the best strategy for dealing with Covid is… be a small country with few land borders.
Much has been made of Australia and New Zealand’s success in containing the virus – up until December of 2021. But clearly this owes much more to their geography than to the specific policies they imposed. After all, almost all the countries at the top of the chart imposed stringent lockdowns as well.
A fair summary of the evidence in the chart above would be: Lockdowns can work to contain the virus, at least for a time, if you combine them with strict border controls. But once the virus gets a foothold in your country, they make very little difference.
Another thing to notice is that the East Asian countries are still concentrated at the bottom of the chart, strongly suggesting that some cultural or biological factor – perhaps greater prior immunity – explains the success of that region.
What lessons are there for the next coronavirus or influenza pandemic? Containment may be viable strategy for small islands and peripheral states with few land borders. But for the vast majority of countries, it isn’t worth pursuing. Instead, those countries should plan for focused protection.











To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
I think the lessons to be learned are to stick to the original plan.
Most UK deaths will end up being care home patients murdered by the NHS and the 100,000 excess cancer deaths (estimated by 2024). Then there’s the recession induced 15 million years of life lost plus the 120 million quality life years lost (maybe have to reduce a bit because Guardian readers loved lockdown).
Governments kill more effectively than viruses. If they’d have ignored it we wouldn’t have noticed it.
The government itself produced a report saying lockdowns would cost 200,000 UK lives – which is at least ten times the true number of deaths from respiratory disease over this period.
they say a recession takes 3 months off everyone’s life on average.
they may well know what they have done – but it would be hard to admit
over time the unintended consequences will come out.
Well recessions are generally caused by the people. (land speculation, 27 million home owners)
I hope they do, but fear it depends somewhat on who’s writing the history.
Unfortunately the nature of global media made it very hard for them to ignore.
There was no ‘murder’. There was an incompetent policy (see even Sweden). There was, as result, an overall higher death rate for those unusually surviving because of a period of low lethal infection and improving health care in general.
The ‘pandemic’ was otherwise – as any true sceptic would recognize – a period of limited impact in terms of lethality. You can’t have it both ways – a pandemic myth and unusually high mortality.
The supposed ‘first wave’ never occured.
The excess deaths in March 2020 arose from care homes being deliberately seeded with very ill hospital patients; care home staff fleeing their positions and residents dying from neglect, dehydration and in some cases starvation; patients being wrongly but on ventilators that blew their lungs out; given Midazolam which induced respiratory disease symptoms; wholesale community DNRs; cancelled medical treatments for people in critical condition and others vulnerable people being too frightened to seek treatment.
Under the newly impleneted WHO death registration guidance, most of these deaths were falsely attributed to ‘covid’.
This genocide has been falsely labelled “the first wave”.
Moreover, the governments own report said 200,000 people will die from the first Lockdown. So they have intentionally killed 200,000 people to allegedly save an undisclosed number of people from possibly getting a respiratory disease that may or may not have harmed them.
I’d say that crosses the Scotch standard of “wicked recklessness” that qualifies it for a murder conviction.
More importantly now than chewing the Covid bone is surely to see how the ‘long term plan'( 2030) is developing?
Isn’t the hysterically hyped Ukraine – Russian nonsense being used to distract from the Coup against democracy, take-over in Canada and to justify coming hikes in fuel prices as the result of the ‘sanctions’ against Russia (which will not harm Russia but will cut off Russian oils supplies and raise prices in Europe)?
The pressure on the British population is about to increase with deliberately engineered higher petrol prices and heating bills.
How can we not suspect that what Trudeau and the WEF ( both he and his deputy are pupils of the WEF) have got away with in Canada will be part of the longer term plan in the UK?
What is currently happening to the French and Italian people? Our media keep us in the dark about all oppressive measures in other countries.We do know that the French have received text messages telling them to get yet another jab to remain ‘vaccinated’!
Bank accounts frozen in Canada for opposing Trudeau, Canadian Banks taking orders from the Government – ought we not to be very worried about the precedent set?
Not one UK MP seems at all interested! Why not?
The most extensive analysis of all cause mortality I’ve seen is from Denis G. Rancourt, PhD Scientist. Social theorist. Researcher at Ontario Civil Liberties Association
His research can be found here: https://denisrancourt.ca/categories.php?id=1&name=covid
He was also interviewed by James Corbett here: https://www.corbettreport.com/mortality/
Further links in the show notes for the slides used in the interview etc.
TLDR: There was no pandemic
Hope-Simpson suggested an association between latitude and influenza.
I note that Guadeloupe is included as a separate entity, but as it is an overseas departement of France, along with Martinique, theoretically it should be included in the French data.
Having conducted a thorough scientific analysis of this data in the last 30 seconds ( about the same time as Drosten spent before producing his peer reviewed paper on the covid Rt-PCR test in jan 2020), I call this B.S.
Agreed.
Was it peer reviewed?
Original Epidemiological Sin: ignoring/excluding all confounding factors so a single favoured factor ‘proves’ whatever point you wish to make. Post hoc ergo propter hoc. (As with ‘climate change’ of all the confounding factors involved in influencing the Earth’s climate system, only one CO2, and only that from fossil fuels, can change the Universe.)
Confounding factors with respect to CoVid: age – younger populations will be less affected; general health and nutrition – poorly nourished people have lower resistance to disease; hygiene and living conditions – people living in dense households with poor standards of hygiene will spread and incubate pathogens more; prior exposure to similar viruses – where respiratory virus (among which coronavirus) are endemic, resistance in the population to new ones is higher; mobility – in less mobile populations infection spread more slowly.
But no, no it’s all about land borders and islands. Of course it is true if a pathogen dies not get onto an island or if all newcomers are quarantined for a time then the pathogen cannot get into the population. This is why Britain was rabies free, and how it was kept rabies free.
Although extraordinarily complex, this analysis does have greater potential than climate study, with each country to some extent its own “earth”. You’ve got to do your best to control for the myriad of variables, not give up before you’ve started.
‘… control for the myriad of variables…’
Impossible. Clue in word ‘variables’. Variables are unpredictable, and some unknown, their multiple possible outcomes are unpredictable, the interaction of these outcomes with other variable and their outcomes is impossible to predict.
This is where computer modelling comes in. The computer is programmed to predict all possible outcomes – a task the computer could never finish – so filters are applied so the computer produces outcomes within the range the filters allow. Those filters are designed to produce outcomes that will best fit round your hypothesis. Then the filtering is tightened to eliminate the outcomes at the margins, so the computer produces only the ones that ‘prove’ your hypothesis… therefore this proves your hypothesis which now becomes The Science™️.
Not really. Life is also a very complex situation with countless variables but we still make a model of the world in our mind and use it to draw conclusions and make decisions. So complexity does not by itself make a problem impossible, or there’s no point waking up tomorrow.
In comparison, I’m sure we can just about manage to draw some meaningful conclusions from a little bit of data. Which also doesn’t mean we should sell our souls to the modelling.
The difference here, surely, was that the variables included the clowns making the decisions and even the ‘data’ on which they based those decisions.
Too many silly ‘mistakes’ (or worse) were made early on with Wu-flu.
First, the consensus that it wasn’t a lab leak.
Second, that the existing pandemic plan wouldn’t (suddenly) work for this pandemic.
Third, that while waiting for vaxxes, existing treatments and palliatives should not be tried. Indeed would not be tried, since they were proscribed.
Fourth, that they convinced everyone that the vaxxes would prevent infection and transmission.
There are many more ‘variables’, but those got us off to a start that could hardly have been worse.
This article looks at the affinity of the spike protein to ACE2 receptors amongst different populations. This “virus” is a bio-weapon with the spike protein being the deadly toxin.
World depopulation determined by a racist & sexist toxin…
The jabs still contain the original toxic spike protein, this is why they need to get it into every arm on the planet.
Noah, this is what needs investigating further.
ACE2 coding variants in different populations and their potential impact on SARS-CoV-2 binding affinity (nih.gov)
They use different ACE2 inhibitors in the Far East to Europe/N America. We have known this will have an effect since Feb 2020. No need for more computer simulations of computer simulations.
The only pandemic we witnessed was a pandemic of misinformation, lies, statistical fraud and state-sponsored censorship of truth and facts.
Getting sick and tired know of this supposed sceptic site pushing the ‘pandemic’ myth.
It’s just a word. Some calamity took place, that we can surely agree on.
Some? You mean Government.
Its not ‘just a word’. Either a pandemic took place, or it didnt. If it didnt, why did the authorities the world over kill and harm millions of people by pretending it did?
At the very least, it was a pandemic of rotten (or evil) decision-making.
I’m still going with Edgar Hope-Simpson’s study of transmission identifying the seasons and lack of vitamin d.
Exactly. Most people have only 1/2 to 1/10th of the 50 ng/mL 125 nmol/L 25-hydroxyvitamin D their immune system needs to function properly. 0.125 mg 5000 IU vitamin D3 per day for 70 kg bodyweight will usually acheive this. This is a gram every 22 years, and pharma grade vitamin D3 costs ~UKP2 a gram.
See https://nutritionmatters.substack.com/p/covid-19-seasonality-is-primarily and https://vitamindstopscovid.info/05-mds/ .
Although I have always been against lockdowns and supported the GBD and their focussed protection it was plain to see in the early days of the virus that allowing plane loads of travellers descend into the UK who would then use public transport to disappear around the country was a recipe for increasing the spread of the virus.
Closing our borders earlier to foreign travel but allowing international freight movements may have removed the excuse politicians needed to lockdown the UK.
Spreading the virus. So what? It was harmless to 99%+ of the population.
It was deadly to the very old, frail and vulnerable just like flu is which doesn’t mean we should not protect them.
The Drosten protocol used a virtual reality ‘genome’ that doesnt exist in the real world. So how is it possible to identify this virus?
Not true.
I have had to counter so much misunderstanding of the PCR test that I have produced this essay to set the record straight.
https://classicrecords1.wixsite.com/the-sceptic/post/pcr-tests-and-kary-mullis
But, we didn’t protect them. We (or ‘they’) killed them in their tens of thousands (and that’s just the UK).
Can I try to add some reality to this please.
In the Far East they tend to revere the elderly, in the main they don’t pack them off to big care homes. They certainly do not have a policy of taking sick elderly people out of hospital beds and putting them with vulnerable elderly in care homes.
Japan for instance has never had a vaccination mandate imposed on its elderly, indeed it posts health warnings on the vaccines.
If you take away the April/May 2020 care home fiasco and the Jan/Feb vaccination drive for the elderly out of the UK/Europe/US numbers its not that different to the Far East.
The difference is societal, not medical, prior immunity etc.
The West has killed old people in the thousands, maybe millions, and given its widespread ocurence its hard to believe it was accidental.
NB small island populations are just too small to be statistically significant on a global basis to make any impact on the overall picture. Africa has a young population so was/is unaffected, S America is an anomaly which makes you wonder if they actually coincidentally had a bad flu year that has been recorded as ‘covid’.
The analysis is largely compromised by the noddy ‘baseline’ used for defining ‘excess’.
And why is it noddy? Surely they just compared to the average for the previous five years or similar, adjusted for population.
Selecting a small number of atypically low mortality years gives no coherent historical perspective.
Unfortunately, it may still be too early to call the winners in this, especially Down Under.
‘Lockdowns can work if combined with strong border controls’ – but if you have strong border controls, why would you need the lockdown?
The lockdown policies were a great success.
All the right people have made lots and lots of extra cash and the globalist digitalisation agenda has taken a great leap forward.
On top of that the over population problem isn’t going to be a problem for much longer courtesy of those warp speed products.
Peru Bolivia Ecuador Mexico. Maybe it’s an altitude thing.
Wild animals crossing land borders. It’s the animals wot did it.
La Quinta Columna – birds affected by EMF worldwide.
Any Ornithologists on here with a possible alternative explanation for this disturbing behaviour?
I heard the Australian PM (Scott Morrison, I think) on the radio this morning, talking about the Ukraine situation. He described the Russians, more than once, as “thugs and bullies”. Without a hint of irony.
“(Scott Morrison, I think)”
If he sounded like an absolute khunt, then it was indeed Scott Morrison.
Bingo. Scotty from Marketing. In fact, khunts find the comparison offensive.
Fewer. Door’s over there, chap.
The overwhelming importance of early use of ivermectin, hydroxychloroquine and other off-patent drugs may also be a visual worth putting up….
‘Chamie-Quintero et al (2021 preprint): ‘Ivermectin for COVID in Peru: 14-fold reduction in excess deaths nationally, then 13-fold increase after ivermectin use restricted’……
A few reports like that are fairly devastating indictments of active suppression of drugs with known safety profiles shown observationally to have phenomenal anti-viral effects…..
And for a recent example how well border controls work, we have Kiribati. Unless a country can transport itself to the moon or something like this, Don’t bother, it’s going to come seems a much better strategy.
Not surprising. If you have land borders you can stop people passing through them, but you can’t stop air blowing over them.
In practice, of course, land borders mean close cooperation, so there are always going to be SOME critical service persons coming through. You can only stop the virus getting a hold if you seal yourself off completely. Which can work for a week or so…
No one can possibly make sense of all this data.
Complete and utter unscientific nonsense.
Dr. Shankra Chetty of South Africa has determined Coronavirus as being of two distinct parts.
1) The initial virus (elevated temperature, sore throat etc.) which conforms to a regular influenza, which can kill, but can be treated with HCQ.
2) The second phase which doesn’t affect everyone but can be equally deadly if misdiagnosed and mistreated.
The second phase is an allergy, crudely put, to the crap generated by the initial phase. It can be treated with common antihistamine products.
Dr. Chetty has treated 10,000 patients personally with 100% success. The only people to have died were four patients sent to hospital against his express wishes by their families. All four died.
What’s chilling is that during the first wave of infections Dr. Chetty noted the only people affected were black patients. He put that down their social conditions.
The second wave was exclusively ‘brown’ people (paraphrasing).
The third wave was exclusively white and Muslim people.
“Lockdowns can work to contain the virus, at least for a time, if you combine them with strict border controls.” But is that the desirable response. Given that there are known and effective early stage treatments that equip the (treated and) recovered with far superior immunity than the (so-called) vaccines, lockdowns can cause a far greater level of suffering in society.