
I feel nothing but pity for British and non-British HIV carriers alike, but I rather think medical care for the non-British is the responsibility of their own country, not ours.
That said, if we’re going to spend £15 billion a year on foreign aid, then allocating £497 million of it to testing for, preventing and developing cures for HIV/AIDS seems to me to be money well spent.
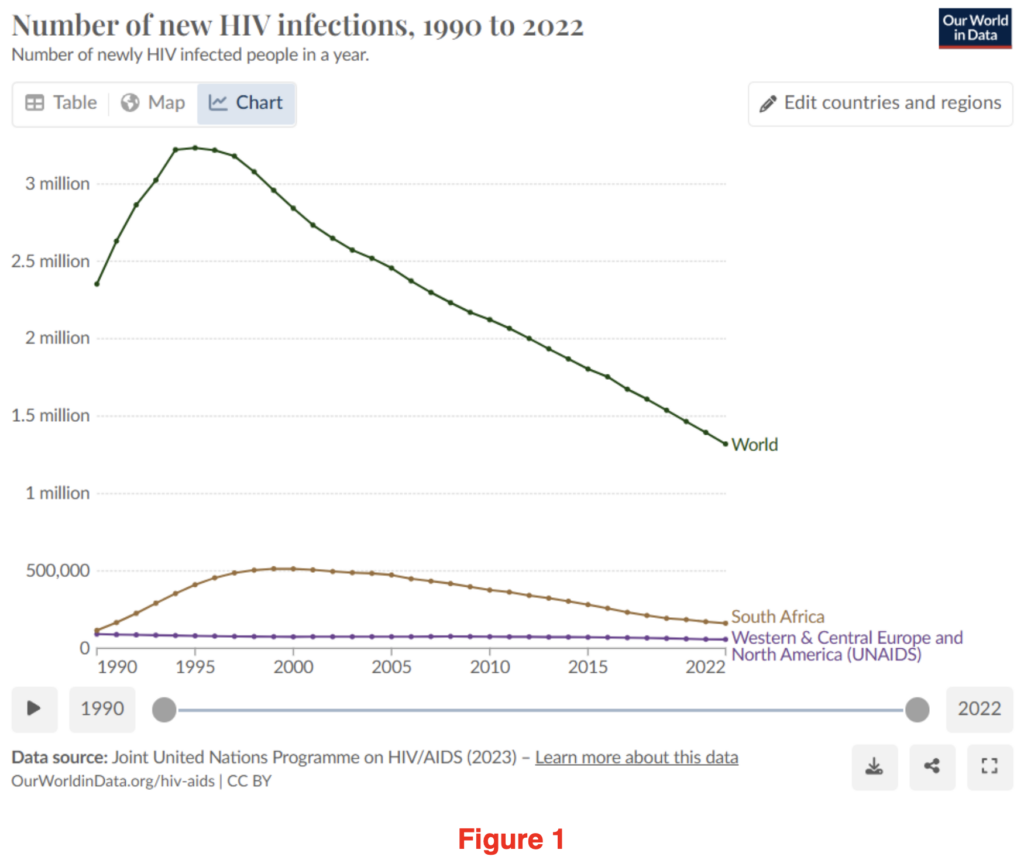
What’s more, it seems to be helping. HIV infections have been falling consistently across the world since the mid-1990s. The war on HIV/AIDS is one the world seems to slowly be winning.
It may have escaped your notice, but December 1st was World AIDS Awareness Day. Sir Keir Starmer made reference to it at PMQs on Wednesday 4th December and also issued a statement to mark the event, the main ‘takeaway’ of which was, “I am determined this generation will be the one that ends new cases of HIV within England by 2030.” Who could disagree? A laudable aim!
However, since the ‘pandemic’, I’ve become hyper-aware of nuanced language in government statements. Why equivocate by limiting it to “new cases of HIV within England”? Why not simply aim to eradicate HIV/AIDS cases from the country altogether?
I vaguely remembered reading recently that HIV cases in the U.K. were, contrary to the worldwide trend, on the increase. Could this be true and if so, was Sir Keir setting himself up to fail, or did his choice of words hide a different reality? I thought I’d just check out the data to see if Sir Keir was, as I suspected, being economical with the actualité?
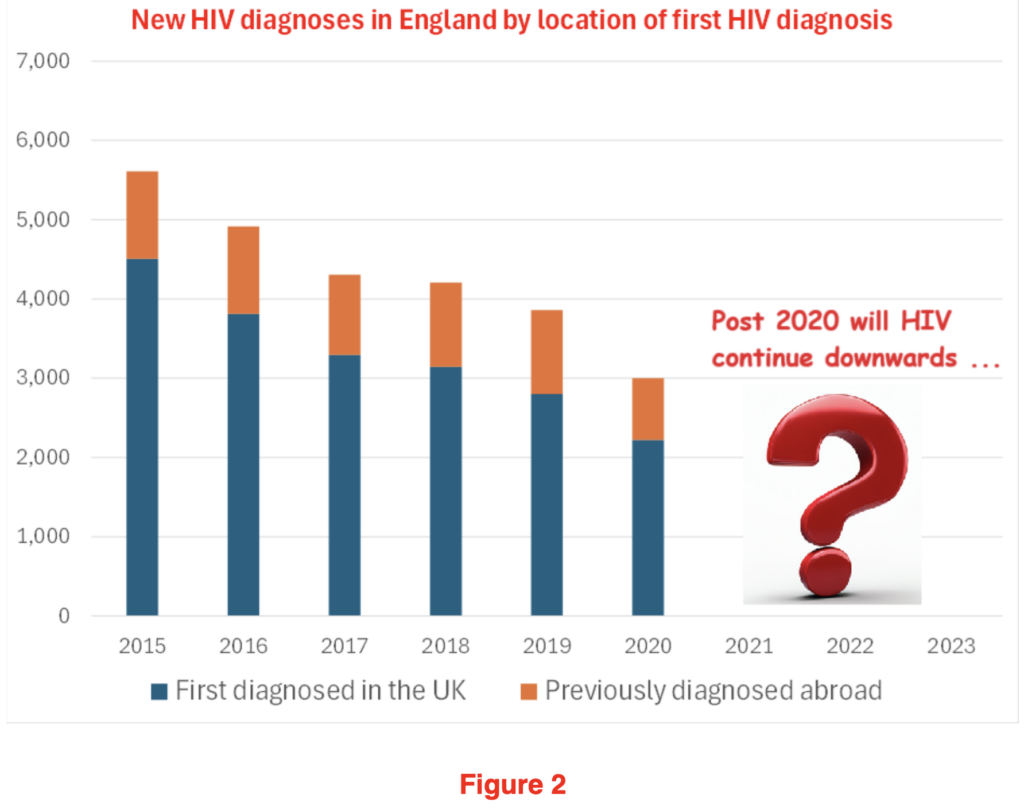
Fortunately, the UKHSA publish exhaustive data on new and existing HIV cases. If you’d looked at the figures for 2015 to 2020 (see Figure 2) you would think that this is all under control. New cases had almost halved over the prior six years. That this was, self-evidently, a good news story. Even better, that this was, that most rare of things, a good news health story. Surely Sir Keir must be well on his way to achieving his aim and eradicating new HIV cases within England by 2030?
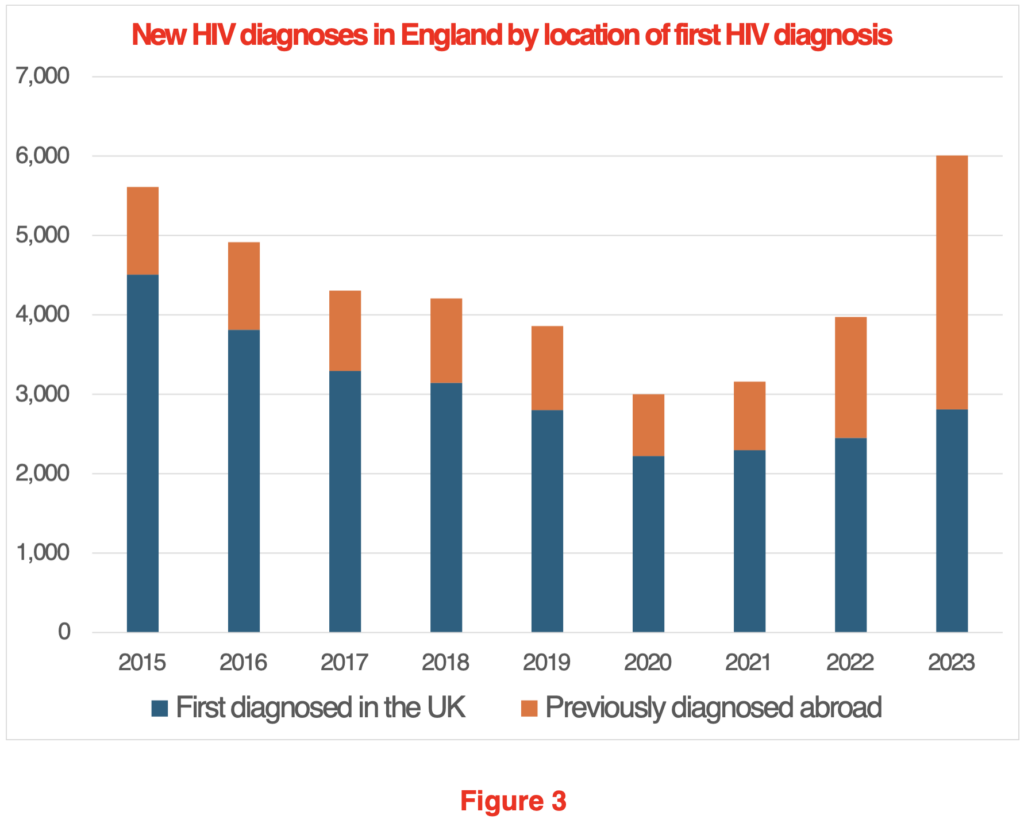
Alas, things have a habit of not working out quite how you expected. In Figure 3, I’ve added in the missing years from 2020 to 2023.
A rather different picture emerges. While diagnoses first made in the U.K. have drifted slightly upwards, new diagnoses, where the diagnosis was first made abroad, have gone up from a low of 778 in 2019 to 3,198 in 2023, an increase of over 300%.
I suppose the questions this throws up are; does it matter? Who are all these new HIV carriers? What, if anything, should be done?
Does it matter?
Each new HIV patient will land the NHS with a lifetime liability of about £520,000 at today’s prices. So, the 3,198 new patients from abroad who arrived in 2023 will land us, the taxpayer, with a future liability of about £1.6 billion. Of course, if it transpires that another 3,198 turned up in 2024, then that’s another £1.6 billion. You know the old adage, £1 billion here, a £1 billion there, pretty soon you’re talking serious money. So yes, if we want NHS funding to go to U.K. citizens, then we shouldn’t be taking on the lifetime treatment of non-U.K. HIV patients.
Recently the OBR published an interesting analysis demonstrating the relative cost to the taxpayer of varying types of migrants over their lifetime. Their data was converted into a handy chart by the Oxford University Migration Observatory that I’ve reproduced in Figure 4:
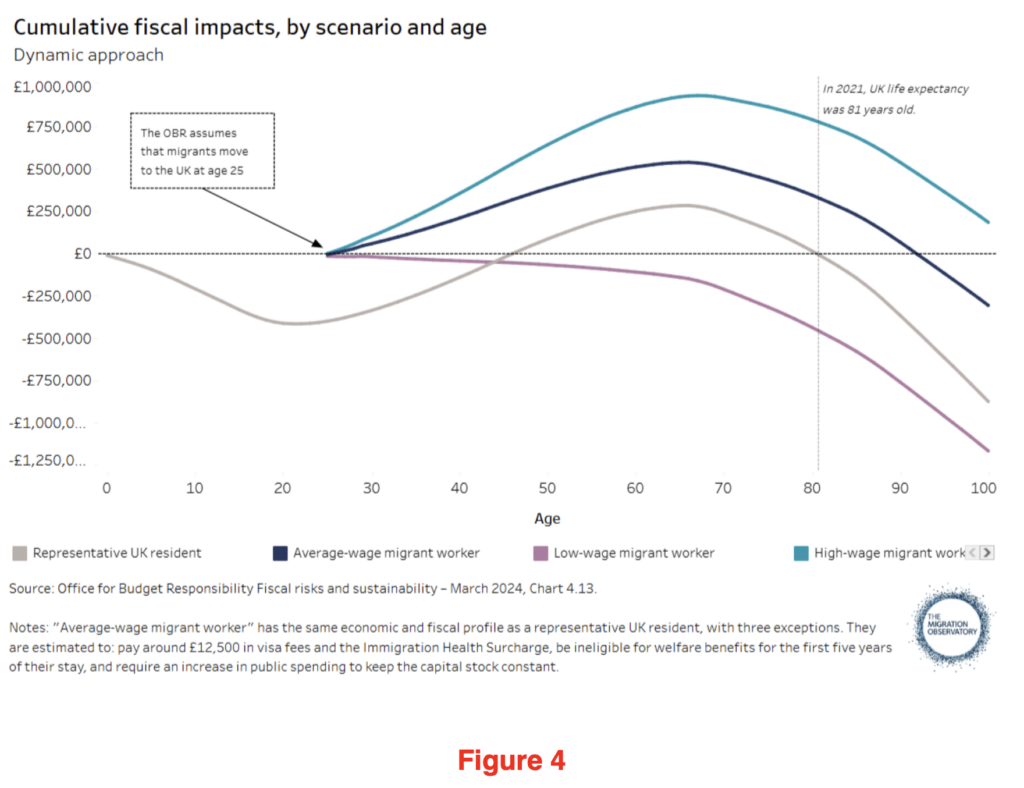
It shows that a “low-wage migrant worker”, should they live until they’re 81, would have cost the U.K. taxpayer £465,000. Call me a cynic, but my betting would be that the 3,198 HIV carriers who arrived in 2023 would tend to cluster in the ‘low-wage’ group, suggesting that each one represents something like a £1 million future liability to the taxpayer, once you add in their future HIV medical costs.
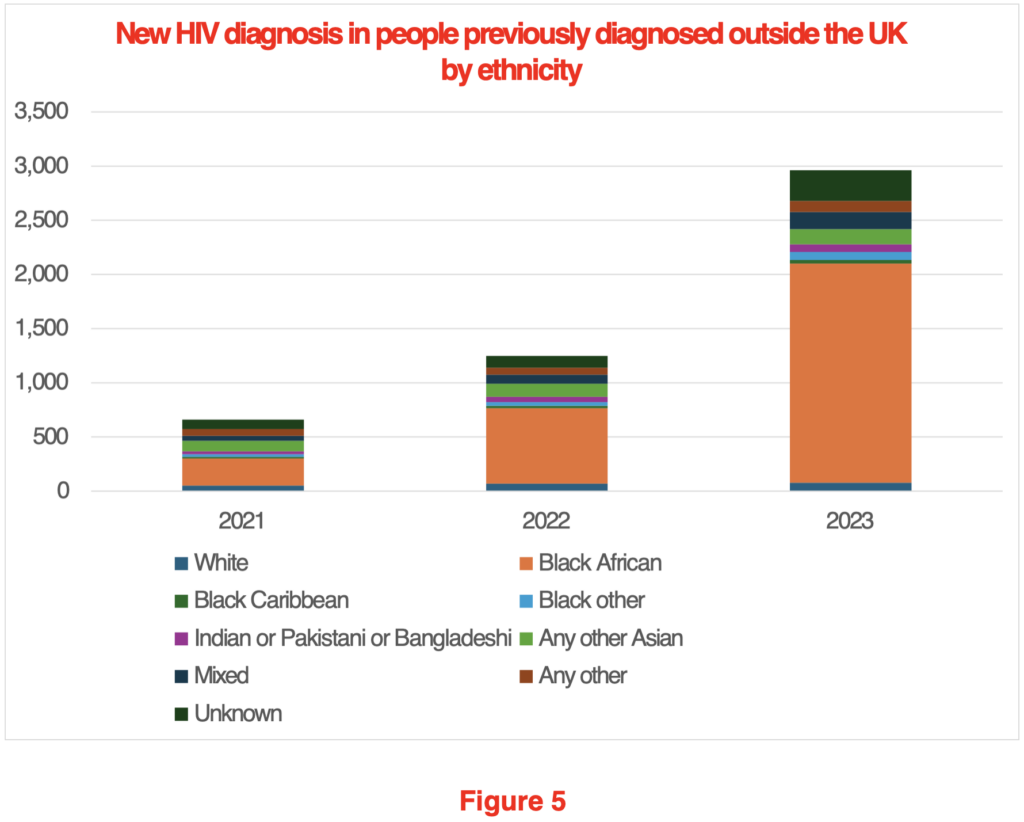
Who are these people who arrived with a pre-existing HIV diagnosis?
Figure 5 shows that by far the largest group, at 68% of the total (10% were of unknown ethnicity), were Black Africans. What’s more, almost 70% of these Black African HIV carriers are women. In all likelihood, many of them will have been granted visas as the dependents of other recent migrants.
What should be done?
This really isn’t that difficult a question to answer. We should make a negative HIV test a condition of being granted a visa. Presently this isn’t a requirement.
The Government’s press release marking AIDS awareness day makes great play of £27 million being made available annually to test people in A&E departments to find those already in the U.K. who are HIV positive. This implies that HIV prevalence is essentially a U.K. health issue. But the reality is, that if we want to reduce the incidence of HIV in the U.K., we need to acknowledge it is primarily an immigration issue. Rather than testing in A&E departments, the testing should be carried out prior to arrival in the country.
Testing in a migrant’s home country requires that we can trust the validity of the tests. It also glosses over the ethical issues raised by asylum seekers testing positive for HIV: should they be denied entry due to a positive test? There is also the risk that, if we deny treatment to recent arrivals or send them back to their home country, we may find that they go ‘underground’, with the risk of increased spread of HIV in the U.K. However, it should be possible to address all these concerns and still significantly reduce the number of new entrants arriving who carry the HIV virus.
Of course, it may be that the Government sees it as part of our ‘good world citizen’ role to take in HIV patients. If that’s the case, we should be clear about this to our taxpayers. But surely, the £500 million or so we spend annually from our Overseas Aid budget on HIV/AIDS initiatives should be the limit of our support for non-U.K. HIV patients. We shouldn’t be allowing people to come to the U.K. who inevitably create an ever greater burden on the public purse. The granting of a visa is conditional on multiple factors. Surely, it’s not unreasonable that a negative HIV test be added to the list?
It is this kind of disingenuousness from the Government that truly rankles. There’s an obvious problem, a relatively straightforward solution, but out of a misplaced sense of charity, or perhaps an overdeveloped desire to be kind, we find that our Government is misleading the public by focusing on a hunt for HIV carriers by the NHS, when we know the real problem should be addressed by our Border Force.












To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
Fake HIV. Fake PCR Tests. Same charade as Rona.
67 symptoms or more for ‘HIV’. Anyone can be told they have ‘HIV’ – symptoms include a cold.
The 2 ‘co-discoverers’, the Fauci poodle Gallo and the corrupt Frenchman Montagnier who won a Nobel prize, both made millions from the swindle and both have admitted that no HIV ‘virus’ exists.
But keep believing sheeple. And keep stabbing.
It was just a stabcidence that in the 80s the entire AIDS scam saved Fauci’s NIAID empire and the CDC. Just a coincidence. And a very useful template for Rona 2020.
I agree, as I read the article I was thinking that HIV is not a problem and does not “cause” AIDS but that Big Pharma is the problem. Hopefully RFK will sort that!
Nick, have you read “The Real Anthony Fauci” by RFK Jr?
And in the ridiculous US system it seems that Dementia Joe will pardon Dr Mengele – oops, I mean Fauci – against prosecution as well as extending it to those on the January 6 Committee on the FBI organised Capitol ‘riot’.
Riot?
No, not just a piffling riot.
An “Insurrection”, of course!
“What should be done?”
The obvious answer is to Shut the Bloody Gates.
Secondly, farm this out to a committee of MP’s with a warning that an initial report must be returned within ten years.
Sorted.
“out of a misplaced sense of charity, or perhaps an overdeveloped desire to be kind”
Since mass immigration from non-white countries started in earnest post WW2, successive governments have striven to hide or deny all the problems it has caused, and made it effectively illegal to question it. Why?
And it also highlighted the supposed power the Speaker has over MPs regarding Reform and the riots. So anything the state does that, if known about and might cause a stir in the public, can be silenced by the Speaker it seems.
It’s an evil trick
“testing for, preventing and developing cures”
Does that include teaching people to avoid practices so as to eliminate all risks.
No money in that.
I suppose circumcision is big business, US including; then again, so is the sale of condoms!
Odd how many diseases in the UK are increasing.
The greatest defence against disease, is good personal and general hygiene, good nutrition. Has there been a decline in that for some reason, I wonder.
It would be sensible, before making such generalisations, to 1) prove the existence of the HIV virus, 2) prove it’s the sole cause of AIDS and 3) prove the reliability of the PCR test in its ability to detect of HIV.
Everything else is meaningless noise no doubt meant to confuse and obfuscate the truth. That truth being AIDS is caused by recreational drug abuse, over exposure to environmental toxins and poor lifestyle choices…oh, and the fraudulent use of the PCR test!
The above is also the reason that why they’ll never be a successful vaccine to combat what is clearly a non-viral illness.
Please enter a discussion rather than down vote the post.
The ‘Real Anthony Fauci’ book discusses this over a few chapters. It shows that HIV doesn’t automatically lead to AIDS and also that some AIDS sufferers don’t ever have HIV. Nevertheless, this article still demonstrates the appalling state of UK borders.
Zero-covid, Zero emissions, zero HIV.
Zero brain.
Zero brain – thy name is Ed.
Peter Duesberg called the so called AIDS CRISIS for what it was way back in the 80’s.
Formerly a world, if not the world’s leading expert virologist – until he had the temerity of exposing Fauci/the MSM for what he/it was – a money making scam.
And if you’re dumb enough to even begin to think AIDS was caused by HIV, just pause a little to think why this deadly condition never really spread amongst the heterosexual population.
Putting it bluntly, the sad fact is that the anus is not designed to deal with multiple acts of anal sex. Not enough immune cells to deal with semen where it’s not really supposed to be you see….
Wonderful things condoms!
Even more wonderful, if you are a “Beloved Leader” who naughtily fancies a little hanky parky on the side; are you more at risk getting “friendly” with a random “asylum seeker” from Sub-Saharan Aftica, or perhaps a very young English schoolgirl?
What a conundrum. I can’t imagine the answer.
Good interview with Russell Brand about the connection between vaccines, autism and the medical establishment.
https://rumble.com/v5wo69t-aaron-siri-reveals-the-shocking-truth-behind-vaccine-trials-sf509.html?e9s=src_v1_ucp
I remember seeing an interview with a man from sub-Saharan Africa who had HIV. He was very fatalistic and accepted his potentially shortened life. He said that we are born from pussy and we will die from pussy. Although it is difficult to pick it up from the vag it has to be said. Can people not see that the true disingenuousness lies in the nature of such a pathogen itself. Especially in the light of exposees about Fauci etc.
I wonder why such a high prevalence of HIV in women though. I’m obviously aware of the ways in which people can contract HIV but unless these women were IV drug users sharing needles or having regular unprotected sex with multiple partners then I don’t get why there’s so many.
Good grief, this is extreme. Imagine living in a community where this might actually be necessary? I’d say women are better off learning self-defense or carrying some pepper spray, even a blade. Perhaps Muslim women might have more use for such a device;
https://x.com/jomickane/status/1866127705063960693
Wow. But then again, if circumstances dictate the necessity for such a device, then so be it.
Personally I have zero trust in any of their metrics. I don’t think I need to explain why given the billion dollar grift and death toll that followed the use of the PCR test, in ways which its inventor advised against. For me their measurement tools are part of their execution method. This nonsense is essentially an ajunct of a deeply sinister agenda. I bet I could get a group of infected African men and women and within a month I could get them clean and looking like piccaninies with watermelon smiles. as Bois Johnson was wont to say. Beautiful physical specimens and disease-free.
If you meet a proper African not only can you get them healthy but they can get you very healthy. When they have just arrived in this country their etheric body is very strong. You can feed off this. It is like if you live in the countryside and you spend time around a farmer or farm lads. There is a delight in being in the presence of their etheric body. Being out in the elements all day long isn’t very pleasant but it feeds your etheric body.
Yes there was a big black dude who used the local Gym (now closed) we got on well but didn’t like it when I mentioned how backward circumcision is. Rite of passage and all that, some things in some cultures are deeply embedded.
He was from Kenya.
We have no housing and no land. Zero immigration is the only policy which is positive for everyone.