
Last week, amid fanfare from both advocates and opponents of centralisation of future pandemic management, the world continued its unfortunate stumble back to old-fashioned public health fascism. The World Health Assembly (WHA) adopted the package of amendments to the 2005 International Health Regulations (IHR), apparently just hours after a final text had been agreed by its IHR working group. The amendments were watered down from previous proposals under which countries would undertake to place areas of their citizen’s health and human rights under the direction of a single individual in Geneva. Nonetheless, they lay vital groundwork for the further subversion of public health towards a recurrent and lucrative cycle of fearmongering, suppression and coercion.
A day previous, the draft Pandemic Agreement (treaty) had been put back for further negotiation for up to 12 months, undoubtedly a set-back for the World Health Organisation (WHO) Director General and his major private and national donors. Chief among the reasons seems to be a continuing reluctance of African countries (and some others) to roll back healthcare to a pre-WHO colonialist model. This is understandable, but African countries are heavily indebted, especially since the economy-shattering response to COVID-19 that WHO and others convinced, or coerced, them to follow.
It seems likely that a reformed Intergovernmental Negotiation Body (INB) will be more circumspect in the way it manages debate over coming months, and external pressure on countries will be ramped up. There is much at stake, hundreds of billions in profit per pandemic if COVID-19 is a guide. Countries with major Pharma interests take this seriously. So do the World Bank and International Monetary Fund, who have previously signalled strong support.
The key IHR amendments were adopted
The IHR amendments passed by the WHA appear mostly innocuous and have been widely reported as such. They add catch phrases like equity in a context of intent to push commodity-based responses and restrictions of freedom that clearly increase inequity, and emphasise the needs of low-income countries whilst commoditising pandemic responses to the benefit of Western institutions. However, the important gain for the WHO and its backers (almost 80% of the WHO’s work is specified directly by its funders) is the wording that further strengthens surveillance (Annex 1) – the key element on which the rest of the business case around future pandemics hinges. This is adopted, and there is a willing workforce to make it happen.
Surveillance ─ identifying threats early and responding ─ seems an obvious thing to support. Doubtless most country delegations were supporting them on that basis. It is particularly aimed at detecting passage of potential pathogens from animals to humans, as in the current publicity around avian (bird) flu. This seeming obvious public good is why this whole agenda has got so far, and why it is so easy to sell to anyone who has not stopped to think.
The justification for increased surveillance put forward by the WHO is hollow. COVID-19 now looks almost certain to have resulted from gain of function research and a subsequent lab leak. The U.S. congressional hearing currently underway is demonstrating that prominent scientists who wrote letters denigrating the rather obvious lab-origin hypothesis agreed in early 2020 that this was indeed likely. You don’t stop the next Covid-like event, therefore, by spending tens of billions per year on surveillance of wet markets, farms and forest dwellers. You just watch a few labs, improve lab security or, if you are serious, stop gain of function research. The other justification behind the WHO’s agenda, that outbreak risk is increasing, is demonstrated to have been grossly misrepresented by WHO, the World Bank and the G20 High Level Panel. The last major acute natural pandemic, as the WHO generally defines them, was the Spanish Flu over a century ago.
‘Spillover’ of potential pathogens from animals underlay the pre-antibiotic Spanish Flu, and also the probable origin of HIV from a simian (primate) immunodeficiency virus. The main spillover event of HIV is considered likely to have occurred before WHO was inaugurated over 75 years ago. Apart from relatively minor influenza outbreaks (that we already have a surveillance operation to deal with), other zoonotic-spillover outbreaks have had relatively tiny mortality since.
The West African Ebola outbreak, while bad locally, killed fewer people than four days of tuberculosis. The first SARS outbreak in 2003 resulted in just eight hours of tuberculosis deaths. However, funding from tuberculosis management, which deteriorated since the onset of Covid, will be further diverted to this surveillance operation for hypothetical natural threats that have not eventuated in over a century.
Basic nutrition funding also declined during COVID-19, despite the number of children with malnutrition rising. The WHO’s agenda, tightly controlled by its funding, is inevitably shifting from population health to the health of Pharma and laboratory research. The Western research community has simply proven more powerful than the communities that WHO was supposed to serve. Money has a way of salving pricks of conscience, and people need a job.
Building the industry’s foundations
So, to understand what is going on here, the original programme within the proposed Pandemic Agreement and IHR amendments must be understood. A massive surveillance operation will be monitored and directed by the WHO, or a committee under WHO oversight. Its main focus will be the identification of viral variants that spillover from animals to humans (‘zoonotic spillover’) or have potential to do so. Many will be found, because this is nature. Sixty years ago, such outbreaks were hidden in the background of disease noise, but now we have clever technology to distinguish them. The IHR will ramp up the use of these technologies and publicise ‘threats’ ─ and a ‘threat’ is all that is needed to trigger a ‘Pandemic Emergency’ response.
Once a threat is identified, the Director General can recommend a series of measures including border closures, quarantine and mandated medical examinations. These were once considered extreme, but became mainstream in 2020 for a virus that kills mostly chronically-sick people at an average age of about 80. The media, heavily sponsored by Pharma, supports this approach, while social media companies have signalled that proclamations from the WHO shall be considered the dominant, and perhaps only, allowable narrative. An IHR amendment noting the importance of suppressing contrary opinion was among those accepted in Geneva.
The WHO will share samples of newly identified viral variants with its preferred pharmaceutical companies. It will then manage the regulatory passage of their 100-day mRNA vaccines (with taxpayer support) and arrange both the market (freedom through vaccination) and liability protection (through publicly-funded insurance schemes). At least this is the intent ─ as described elsewhere. The delay in the proposed Pandemic Agreement has slowed down parts of the whole, but the 100-day vaccine programme is well underway.
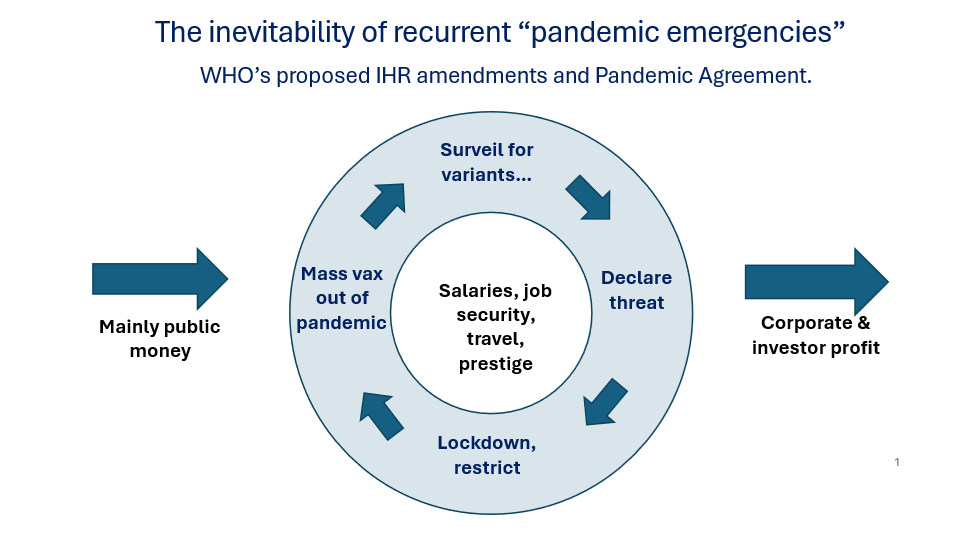
So, the groundwork is laid for the ‘surveillance-declare threat-lockdown-coerced mass vaccination’ approach that has been in brewing as an idea among Pharma-related circles for over a decade, and forms such an unbeatable way of extracting money from others, whilst appearing on a superficial level to be altruistic. There are solid reasons why penalties for fraud are seen by Pharma as just another business expense. There are also reasons why coercion and conflict of interest were once considered incompatible with public health. However, the growing army of public health bureaucrats and researchers now dependent on this model have a strong interest in making it happen and are vocal in their support.
Returning public health to its unedifying roots
COVID-19 proved this paradigm can concentrate wealth and power at an unprecedented rate. The WHO, transformed over recent decades from an international organisation answerable to all Member States to a public-private partnership directly responsive to its major funders, is the obvious tool to bring this together. But the World Bank has its own pandemic fund, the World Economic Forum of private rich people has cemented its influence over national leaders, and the United Nations Secretariat has its coming Summit for the Future in September 2024. The noise in Geneva over the past two weeks constitutes just a part of this behemoth of centralised control and, of course, centralisation of wealth.
Colonialism in the 19th century was built on ‘equity and inclusion’. The colonies needed to be conquered and suppressed so that the benefits of another’s superior civilisation could be foisted on them for their own good. Slavery was sometimes justified in a similar manner. European fascism and the eugenics and technocracy movements of early 20th century North America were based on similar principles. What we are seeing from the international public health establishment is no different, and will be no less nasty in its outcomes. The IHR amendments we have just seen adopted, like the early policies of Mussolini, will be important in building the machine required to run it.
We have just taken a further step down the road to a world built on false claims and the rule of self-declared experts. This is not something that can be ‘won’ but an unending battle against human greed and self-interest that will always be with us. The hard part is to recognise the intent through the mix of fear (keep watching bird flu) and flowery verbiage. When those who advocate a change are the ones who stand to gain at others’ expense, and when they misrepresent the risks of failing to follow their lead, we should start to understand. Greed is not a new problem.
The recent months of negotiations have shown that many involved in the process are recognising potential harms, and a few countries are raising reservations. However, self-interest, coercion and propaganda are a powerful combination. Those pushing medical fascism, and those enchanted by it, are very much in control. A further step down this fascist road is no victory. But if we keep exposing false narratives and refuse to comply with stupidity, there are signs that the worst of the current agenda may yet be derailed. Truth remains the chief enemy of all that is currently being forced on the world by a self-entitled few.
Dr. David Bell is a clinical and public health physician with a PhD in population health and background in internal medicine, modelling and epidemiology of infectious disease. Previously, he was Director of the Global Health Technologies at Intellectual Ventures Global Good Fund in the USA, Programme Head for Malaria and Acute Febrile Disease at FIND in Geneva, and coordinating malaria diagnostics strategy with the World Health Organisation. He is a Senior Scholar at the Brownstone Institute.










To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
Brilliant article! Thank you. Very well said.
The Conservative Party’s two main problems are, as you have identified, ‘Blair’s Britain’ and the ‘extended civil service’ of rather dim, self satisfied, self gratifiers, neither of which the Conservatives have ever had the backbone to confront.
Consequently they have frittered away the goodwill of those who gave them a decent majority precisely to take on that egregious, nest feathering, pompous and self serving, fat and sweaty blob of bureaucratic functionaries.
The Reform Party is now the beckoning refuge for that, by now, incandescent vote.
It remains to be seen how big the Reform vote will be, and how diminutive that for the utterly hopeless bunch of incompetent buffoons who make up today’s ‘Blunt & Pincher’ party.
But The Netherlands has shown us the way……
My opinion is that the old chestnut about the Irish farmer being asked for directions, holds good: “If I were you, I wouldn’t be starting from here.” 650 MPs mean 450 gravy-trainers not fit for purpose. Civil Serice, NHS and MOD Procurement: bad jokes that no-one ever found funny. A root and branch clearout of the Augean stables is required, but I don’t see any Hercules figure on the horizon. (Notwithstanding N. Farage’s sterling efforts). Glad to be in the ‘departure lounge of life.’ What a pretty pass!
I very much share your dismay.
‘When he stopped there was a considerable silence.
I then asked: “Where is the strategic reserve?” and, breaking into French, which I used indifferently (in every sense): “Ou est la masse de manoeuvre?”
General Gamelin turned to me and, with a shake of the head and a shrug, said: “Aucune.”
There was another long pause.
Outside in the garden of the Quai d’Orsay clouds of smoke arose from long bonfires, and I saw from the window venerable officials pushing wheel-barrows of archives on to them.
Already therefore the evacuation of Paris was being prepared.’
Churchill
Alanbrooke, Monty and Alexander got the BEF out of the merde and, ultimately, Alanbrooke, backed by Churchill, got the entire country, and (Western) Europe, back to calm waters.
But it got worse after Dunkirk before it got better.
A Stygian darkness is now on the horizon.
It is to be hoped, in the next few years, that the darkest of the night to come presages some kind of new dawn, the warmth of its illuminating rays a long way off yet……
Beggar!
I reciprocate your sentiments Monro, The ‘Stygian darkness’ to which you refer, I sum up prosaically (in the words of Derek and Clive). “—and I turned to the manager, and with all the dignity I could muster, said; “Is this any way to run a fucking ballroom?””
Top
Deep State.
Unified across the G20.
They meet in various confabs including the crap called COP.
Rona messaging was the same across the G20 as were the policies and timings.
Just a cockup…..
“We are Governed by Process…” A major part of it being the first past the post system; the modern “Conservative” Party will be glad that it is.
We are governed by ppl bribed not to represent their constituents. Plus any possibility that someone can’t be paid off there are supra national treaties/bodies that prevent any real change in nation states.
“Shortly before the referendum of 2016, David Cameron and George Osborne drew up plans to purge the entire Right of the party, reconstituting it as a purely centrist force.”
——
And that, I think, is why Cameron’s been brought back now. I think Sunak was ordered by the Party Grandees to make him Foreign Sec, because there’s nothing whatsoever in it for Sunak himself …. with the useless little pipsqueak being continually upstaged by Call Me Dave.
The Party Grandees are anticipating the post-election split and want Cameron in place to lead what remains of the LibCON faction into unity with the LibDEMS. He did it once in 2009, to keep “the Right” under control and now they want to make it permanent.
That will leave any right-wing Conservatives who are left in Parliament with the choice of uniting with Reform or being completely ostracised.
Something else that is rarely mentioned is the control that has been wrested from local constituency selection committees. More and more I hear that some unknown bod (to the local members) has been imposed from on high by the Conservative & Unionist (just to remind ourselves of its history) Central Office (sorry, CCHQ as it pompously calls itself now).
Blair began the destruction of the power of Parliament. The Supreme Court and the Bill of Human Rights, were un-necessary. Parliament has always been the absolute court of hearing, and our Human Rights were enshrined in the common law. Then devolutions, then more power to Brussels, and the gradual shift from parliament to Quango’s which has continued apace ever since.
What does parliament decide? To rubber stamp legislation written by well funded activists, promoted by MP’s who, although there is no memo or meeting, they know what’s good for them, and their kind. No-one will upset the apple-cart while they’re filling their pockets.
Finally, the legislation is passed and passed on to another quango where it can take on a life of its own, driven by political activism, without adequate scrutiny, by unelected officials. The people who take our votes, fail utterly to act in the interests of the citizens. In fact they act against our interests, and they don’t care. They are our superiors, intellectually and morally and they don’t need our permission, or so it seems.
I agree with you, except to make explicit the implied ‘They think they are our superiors’
I have yet to meet, or even see on TV, an ordinary MP who is anywhere near being “intellectually superior”. Nigel Farage is, and that is why they hate him so much. Parliament nowadays reminds me of the entertainment committee of a working mens club, “are the jokes rude enough, and is the beer cheap enough?”, ok booked, next! The unfortunate part is that none of either front bench is anywhere near this low standard either, or at least isn’t prepared to let it show in actions. If they do they are immediately sacked! Oh, wait a moment, that is what happened to Boris, Liz, and hopefully Rishi soon, although I doubt he meets my first sentence either. I predict Cameron will be PM by the end of February, or possibly someone else. Cameron is trying to give away Gibralter at the moment, with no mandate or democratic vote by the BRITISH inhabitants either.
Has the Author ever heard of the World Economic Forum? Does he not have any awareness of their activities and influence on Global politics and politicians?
Aparently not, The plot: says it is all alive and well in Westminster, part of the Gove group, without actually mentioning it (probably for legal reasons)!