
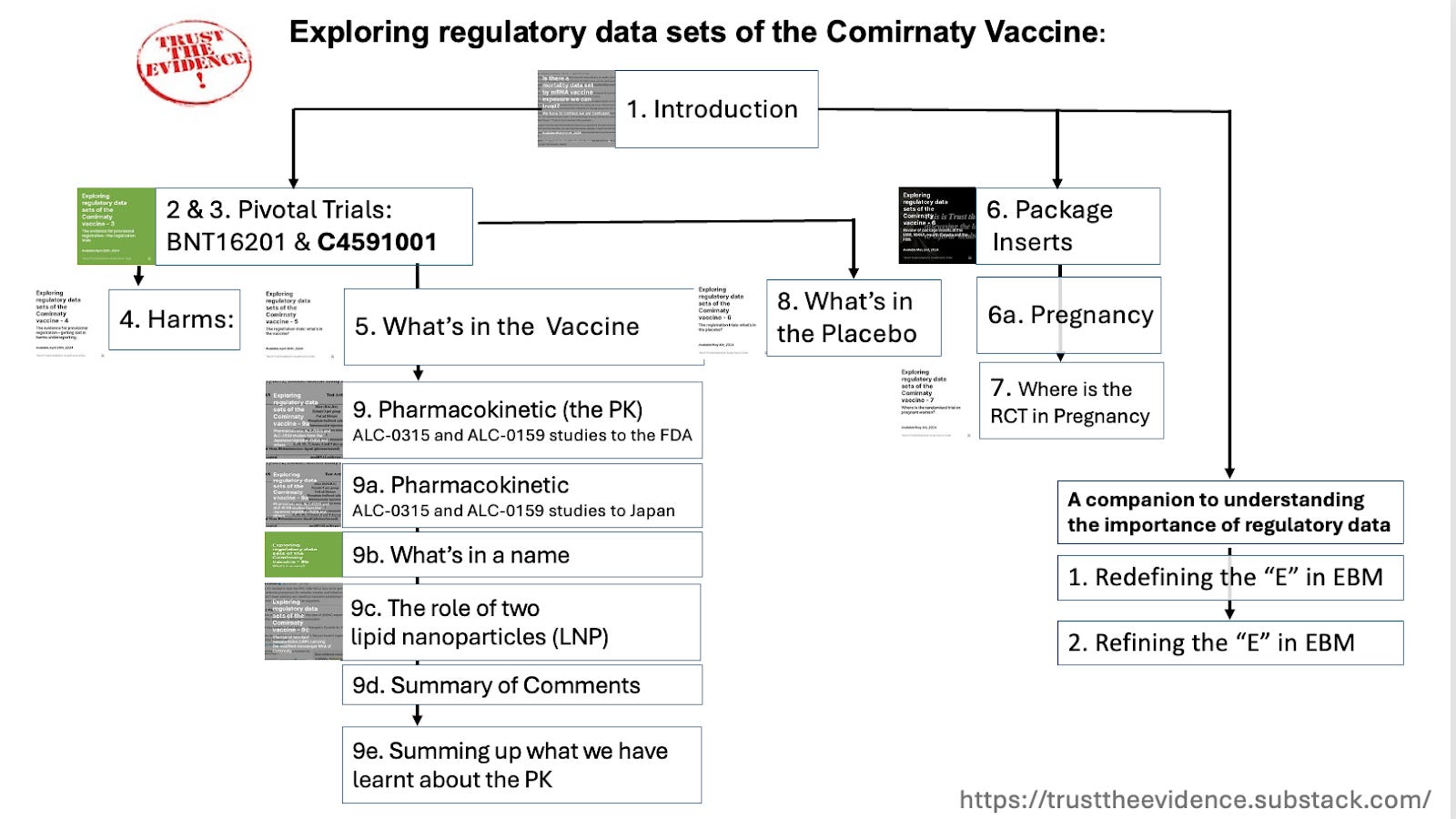
Well, what do you know? It feels like yesterday, and we have already written loads about Comirnaty, the Pfizer/BioNTech Covid vaccine, and the properties of its two lipid nanoparticles (LNP) and modified messenger RNA. So, have our readers, who have commented in their droves, Just look at this diagram drawn by Picasso Heneghan:
This is a list of firm points and 15 questions we have established so far on the pharmacokinetics (how the body interacts with a drug) of Cominarty:
The lipid ‘excipients’ ALC-0315 and ALC-0159 were new. Regulators note the limited experience with these compounds.
1. Whose job is it to close the gap in evidence and ensure patient safety when new experimental compounds are included in vaccines?
Experience of their use in humans was limited. They act as the carriers; the RNA is a different story. The metabolites were found everywhere in the rats’ organs (liver, spleen, ovaries and so on).
The significance of their widespread distribution is unclear for humans, but the concentrations were very high in the liver and ovaries and almost certainly toxic.
2. Does this hold true for humans, too?
3. What is the possible toxicity of LNPs in humans, especially after repeated exposures?
Vaccine particles (antigens, adjuvants and excipients) in other vaccines are not usually found in many internal organs; they are usually concentrated around the injection site. We are unclear about the half-life, although the EMA seems to think it is long.
4. Is there a dose-response?
5. What is the half-life of mmRNA in the elimination phase in different organs?
6. What happens to the mmRNA in humans in different organs?
One or more of their ingredients are considered carcinogenic.
7. Why were no carcinogenic studies carried out in animal models prior to provisional licensing?
8. Why were no genotoxicity studies carried out in animal models prior to provisional licensing?
Nanoparticles are vastly different, and some are toxic, which is concerning. Our understanding of their behaviour in complex biological systems is extremely limited.
9. Where are the post-marketing studies following up on the cancer risk?
The Japanese regulator considers Cominarty as a “powerful drug”. Cominarty is a formulation consisting of tozinameran encapsulated in LNP.
10. Should mmRNA vaccines be classified as a drug?
11. Why is a modified messenger RNA abbreviated to mRNA, which we are taught stands for messenger?
The Japanese regulator reports Pfizer’s explanation that the pharmacokinetics of mmRNA formulation encapsulated in LNP is dependent not on the encapsulated mmRNA but on the LNP.
12. Is the LNP inert as Pfizer claims it is?
The MHRA enabler (formerly a regulator) does not know anything about the metabolism of the nanoparticles or the mmRNA, nor does it hold vigilance data for the Covid vaccine harms, and it knows nothing about the rate of underreporting of harms.
13. Whose job is it to ensure patient safety if the regulator/enabler is wilfully ignorant of the evidence of harm at the approval stage of novel vaccines?
There are no published studies of Cominarty in pregnant women. All the regulators report in the package insert that: “No data are available yet regarding use during pregnancy” (EMA and MHRA) and “The available data on COMIRNATY administered to pregnant women are insufficient to inform vaccine-associated risks in pregnancy” (US FDA).
14. Why has the only randomised controlled trial on pregnant women not been published?
15. Why does the messaging to the public differ from what is reported in the package inserts for pregnancy?
For now, we are leaving the pharmacokinetics behind (we’ll likely return) and moving on to the heavy lifting of determining the effects of Cominarty.
This post was not written by impersonators and is not commercial in confidence. It is not carcinogenic and will not self-disrupt or autodelete. We are not on the payroll of any pharmaceutical company, and given the content of our posts, we have been notified that HMG will award us the order of the boot.
Dr. Carl Heneghan is the Oxford Professor of Evidence Based Medicine and Dr. Tom Jefferson is an epidemiologist based in Rome who works with Professor Heneghan on the Cochrane Collaboration. This article was first published on their Substack, Trust The Evidence, which you can subscribe to here.











To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.