
Suicide is a bit of a hit and miss affair. I can think of six cases of people I’ve known who’ve taken their own lives. One, a very successful business executive, threw himself out an office window; he survived the fall, only to hang himself a couple of years later. The girlfriend of a lodger survived throwing herself in front of an underground train: she left it too late and got blown back onto the platform, breaking a hip. She too, some while later completed the job by jumping off Beachy Head. A business acquaintance, having been diagnosed with Parkinson’s blew his brains out with a shot gun, literally, leaving his wife to clear up the mess. The girlfriend of another acquaintance killed herself when her boyfriend went off to university, only for the boyfriend, my acquaintance, to follow suit on the anniversary of her death. Finally, a university fresher I knew, depressed and alone in his halls of residence, killed himself during the first lockdown. Apparently a grim and drawn-out death. I blame Ferguson, Whitty, Boris and the other nutters for that one.
Of the six, two failed the first time. Two had access to shotguns and made a good job of it. Two others used a drug cocktail, which while fatal, was neither quick nor, so I’m told, painless. While jumping off Beachy Head shows a level of determination beyond my imagining. Half were in their late teens or early 20s. Each one a tragedy in its own way, leaving behind misery, heartache and untold complications.
To my mind only one of these deaths made any sense. I suspect a psychiatrist would concur. However, as we’re seeing in Canada, and who knows perhaps all too soon in the U.K., it won’t be doctors making the decision, it will be ‘human rights lawyers’ should proponents succeed in following Canada’s lead and making state assisted suicide a human right, opening the floodgates to those who, with help, could get their lives back on track.
Given that two of the suicide attempts I detailed resulted in failure but significant injury, I can see that there is an argument for getting the state and a doctor involved – the argument based on ‘utility’. Surely, if a doctor were to be involved, while the suicide may still be, in the eyes of the rest of us, a mistake, then, to quote Macbeth:
If it were done when ’tis done, then ’twere well it were done quickly.
Surely, the involvement of a doctor would at least make it all cleaner, more efficient.
However, it isn’t only my acquaintances who have a tendency to botch their suicide attempts; most efforts are unsuccessful. I doubt any data on the efficacy of suicide attempts are particularly accurate, but the chart in Figure 1 reflects the estimates I’ve seen. 17.5% of attempts using a firearm fail. 40% of hangings fail. Heavens, even 70% of jumpers survive! One can only imagine the injuries this all results in.
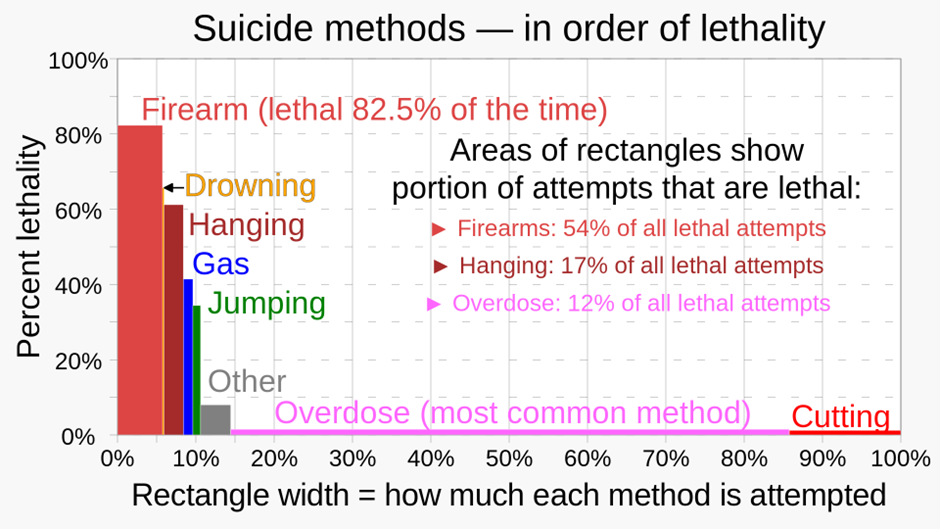
Apparently, only about 5% of people who survive a suicide attempt go on to kill themselves within the next five years. Clearly, most people who attempt suicide and fail get over it. I’m not sure that getting professional help to improve their first-time success rate is necessarily a good idea.
However, are doctors likely to improve on your own ham-fisted efforts at ending it all? Having looked at the evidence, I was surprised to find it appears you’d be better off consulting a slaughterman than a doctor. Slaughtermen kill hundreds of large mammals every year with barely a misstep.
It might not immediately occur to you, but doctors, certainly in countries where they already have assisted dying or the death penalty, do a fair bit of killing already, though I’m not sure they can hold a candle to slaughtermen.
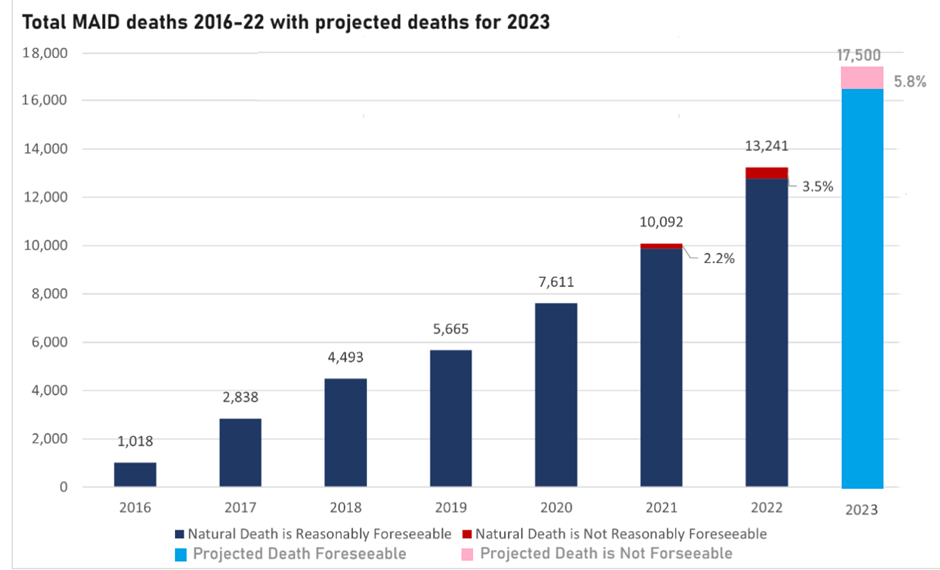
There were 24 executions in the USA in 2023. Back in 1999, enthusiasm peaked when 98 prisoners were put to death. By way of contrast, in nearby Canada something like 17,500 people will have been ‘euthanised’ in 2023. That’s almost 50 deaths per day! Quite something. Canada, with a population one eighth the size of the USA, is killing twice as many people each day as the U.S. executes in a year.

You might think that with this level of killing both Canadian and U.S. doctors would have it down to a fine art. Apparently not!
Executions of death row inmates takes various forms: lethal injection, gas, the electric chair, hanging and firing squad. All are fraught with problems. There are newspaper articles galore detailing no end of horrors: how long it takes for the prisoner to die, difficulties getting the needle in the vein, failures of electric chairs, firing squads missing. Having killed a few chickens and, grimly, once a very sick old ewe on an Australian sheep farm, I have every sympathy for those called to do the killing and the real-life difficulties that present themselves as you make a hash of what, on paper, would seem to be the most straightforward of tasks.
John Wyatt, Emeritus Professor of Neonatal Paediatrics, has written a very moving piece in the Spectator concerning the likely impact on practicing doctors if a bill recently drafted by the Scottish Liberal Democrats legalising ‘assisted dying’ gets passed by the Holyrood Parliament. Doctors would then find themselves being expected to kill patients. How to square this with a doctor’s primary objective ‘do no harm’? In the article he notes that the Hippocratic code prohibits physicians from participating in judicial executions. Clearly, the ethics around extending a doctor’s duty to killing their patients presents huge ethical dilemmas.
To me, one of the most intriguing points raised by Wyatt is that “once the physician has certified the death, he will be legally instructed to produce a false and patently misleading death certificate – saying that the certified cause of death was the underlying disease, rather than the lethal poison that had just been administered”. Given the controversary during the ‘pandemic’ in the recording of deaths ‘with’ or ‘of’ Covid, and the corruption of ‘all-cause’ mortality data, a sceptic, such as me, is highly suspicious of this particular sleight of hand.
It will be argued by many that there’s a vast difference between executing a murderer and ending the life of someone, either terminally ill or who, for whatever reason, wants some help ending his or her life. Many will argue that there’s a difference morally. But one question I’d never previously considered was the ‘how’. How do you go about killing people?
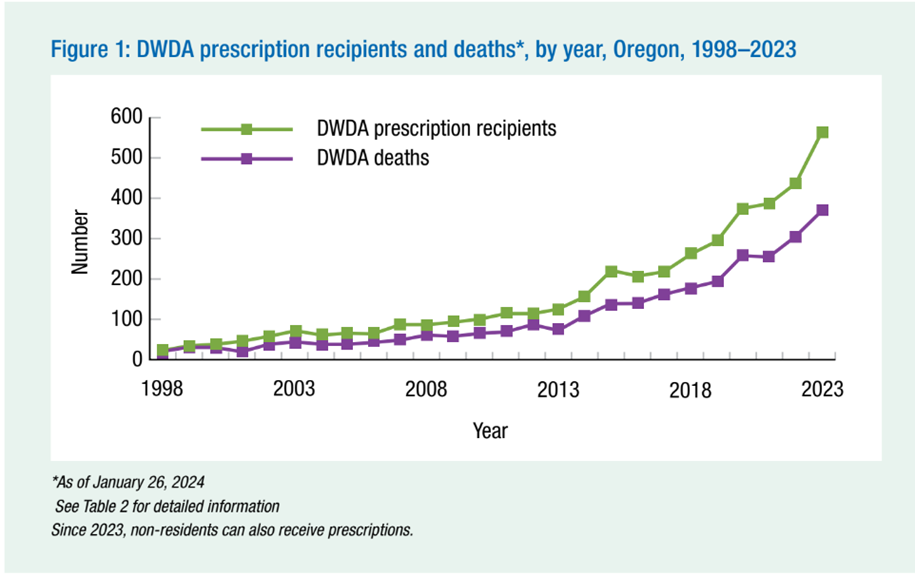
In addressing this problem, I’m indebted to one of the Daily Sceptic‘s regular below-the-line commentators who, beneath one of my recent articles, linked to a blog post by Sir Desmond Swayne MP which included a report by the Oregon Health Department, entitled ‘Death with Dignity’. The report details the annual results of Oregon’s Assisted Dying Act.
It’s in the area of ‘efficacy’ that the Oregon report is so illuminating. Let’s start with a bit of context. In Oregon they aren’t killing people on the industrial scale of Canada but they still manage to kill more than 20 times the number executed across the entirety of the USA.
Five hundred and sixty people were prescribed the lethal drugs in 2023. Of those, 367 – just 65% – died from the cocktail. The other 193 people didn’t survive the drugs – they either didn’t take them, died of something else before ingesting the drugs or the medics lost track of them.
The report includes a handy summary of what happened to the those prescribed with the drugs in 2023, which I’ve reproduced in Figure 5.
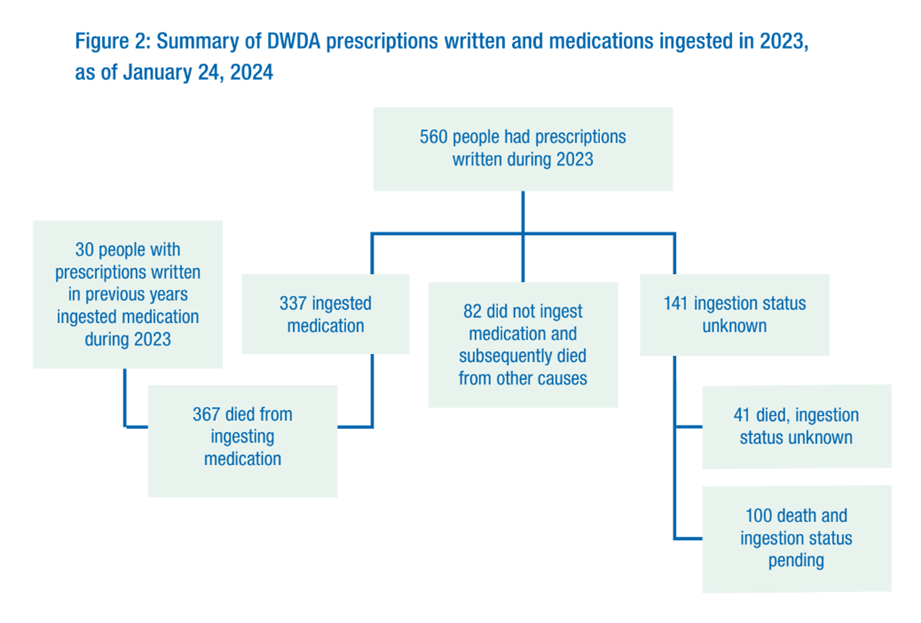
As an aside, it’s worth noting that 17 patients, presumably from the group who didn’t ‘ingest’ the drugs, outlived the six months residual span of life, the maximum time that, according to the doctor, a patient can be expected to live and still qualify for assisted suicide. Be that as it may, you can see that nothing is straightforward, nor – if you are someone considering suicide – is it terribly reassuring.
The following tables are lifted from the report.
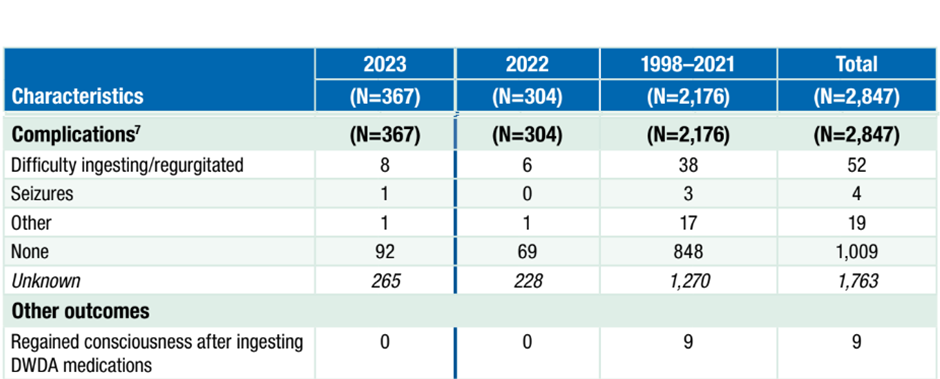
Firstly, let’s look at ‘complications’. Well, the first thing that strikes you about the findings is how incomplete they are. Of the 367 who took the poison there are no data for 265 (72%) of them. Of the 102 (28%) for whom we have data, 8% had difficulty swallowing or regurgitated the poison. One patient had a seizure.
It seems odd that for most patients no data are available. However, the next table gives you some clues as to why this might be. Figure 7 shows who was with the patient when he or she either took the drugs or died from the drugs. For only 58 (16%) of the 367 patients was the prescribing doctors present when the ‘medicine’ was ingested. And in only 44 (12%) of cases was the doctor present when the patient died.
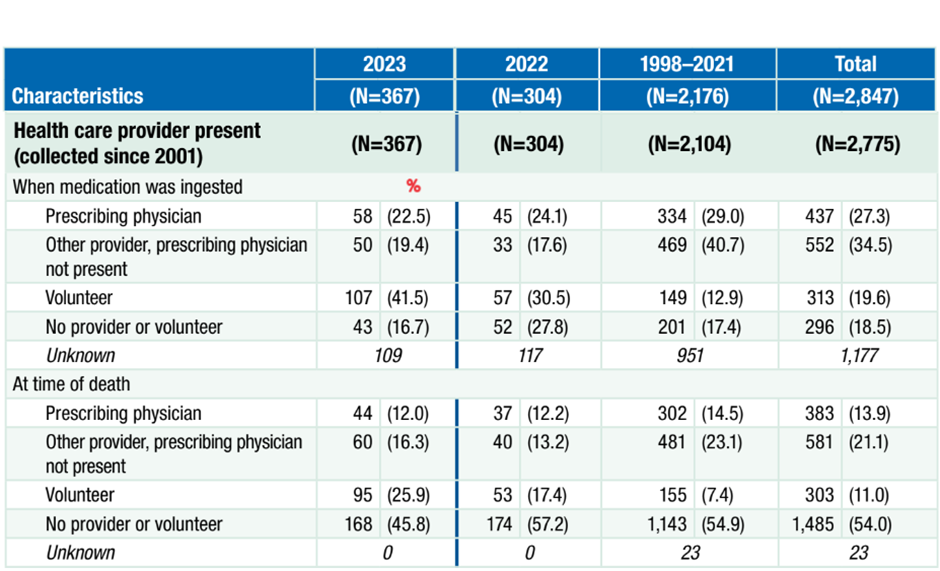
In 14 cases the doctor appears to have left the patient between ‘ingestion’ and death. Similarly, while of the 258 cases for which there are data, 43 were seemingly alone when they ingested the ‘medicine’, by the time of death 168 were seemingly alone. This all suggests the ‘medicine’ isn’t all that fast acting.
Figure 8 tells us just how fast the ‘medicine’ takes to do its job. For 34% of the patients we have no data. Of the 64% for whom there are data it took from one minute to over eight hours (488 mins) for the patient to lose consciousness, with a median time of five minutes. Death took rather longer. The median time to death was 53 minutes, while at least one poor soul took 137 hours, not far off six days to die! Can you imagine if this happened in an execution chamber, or an abattoir come to that.
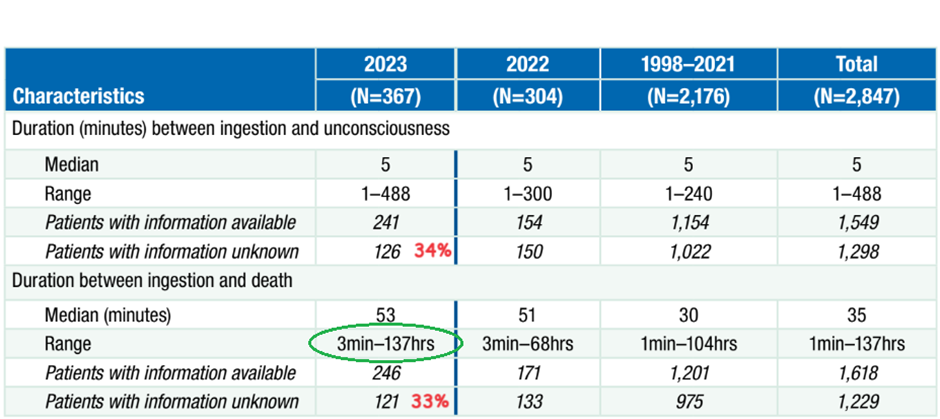
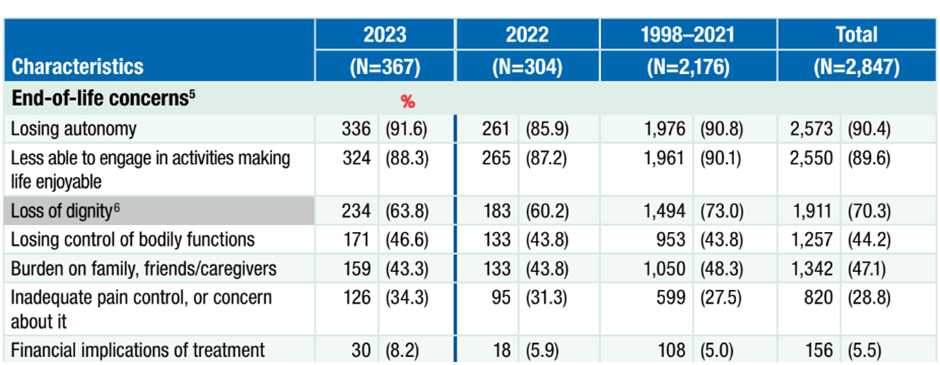
Figure 9 has data on the ‘why’. Why did these 367 people want to die? Only 34% mentioned inadequate pain control. For most it was losing autonomy, being a burden on their family, or just not being able to enjoy life.
The message I take from the Oregon report is that the mechanics of all this look very messy. Admittedly, these data are limited to Oregon. Maybe they do things better in Canada or the Netherlands or Belgium. Maybe they’ll do it better in Scotland or eventually England and Wales when it’s inevitably introduced – but I doubt it.
I suspect killing a person can be every bit as messy and distressing as I found killing that old ewe in Australia 40 years ago. Certainly, having been fairly equivocal about assisted dying, having read this report I can’t think it’s something I’d be happy recommending for my loved ones.
I’ve always been a bit of a doodler. One thing I frequently drew while in boring meetings was a guillotine I could build in my garage. I’d decided that it would probably be the quickest, most pain-free way to go. The design was ingenious if I say so myself. However, in recent years I’d rather assumed I’d be happy to let the professionals take over when the time came. Well, not any more. I must go and dig out those old notebooks, I suspect my home-made guillotine or the local slaughterman will prove the better bet.












To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
Those people in the Titan submarine diving to see the wreck probably had the best idea.
As a veterinary surgeon we are allowed to euthanise animals to stop unnecessary suffering, so over the years I have euthanised animals. It is a peaceful process if done well. No need for suffering.
I don’t understand what they actually did here.
This is not a post to advocate assisted suïcide for people, just saying that the actual process should not be part of the argument.
That’s something I’ve wondered in the debate over the US death penalty. I wondered if the vets were covering up what happens when the dog owner leaves the scene, but you reassure me on that.
Still, it does seem that it is particularly hard to kill people.
Interesting to ask if it’s just the time delay that causes doctors to leave the scene so often – or whether the same troublesome conscience intervenes as it did when I discussed abortion with the gynae staff in my hospital days: 3 out of the four junior docs who did TOPS hated it, and the fourth claimed not to care… but he was, in fact, a Catholic and very obviously in denial.
Most doctors will do euthanasia against conscience, telling themselves it’s the law or just following their training, and cause untold damage to their ethical compass (even without the Hippocratic Oath), and hence to the trustworthiness of the whole profession..
Most doctors will do euthanasia against conscience, telling themselves it’s the law or just following their training, and cause untold damage to their ethical compass (even without the Hippocratic Oath), and hence to the trustworthiness of the whole profession..
It is a matter of degree. I am sure countless doctors have upped the morphine to help someone avoid pain in their final days and have known it was the right thing to do (I hope they will do as much for me).
MTF –
Proper terminal care (since Dame Cicely Saunders) has always involved titrating regular analgesia against the pain, so that if possible there is never pain, or minimal.
Doing it that way minimises sedation and confusion, so that patients get to live until they die, and it was established a couple of decades ago that such dosing does not significantly shorten life.
It is the ill-trained doctor (or in my experience ill-trained and arrogant) who takes it upon himself to decide to overdose a patient deliberately.
We’ve had many dogs as part of my family over the years and each time one is euthanised my wife, or I are present during the process. It’s very quick and painless.
Most of the time the owners elect to stay with their pet during euthanasia. I explain what will happen first, as it really is quite quick, so they are prepared.
When a large animal like a horse can be put down by injection, I do wonder why it is so difficult to, essentially, put down a human.
I was wondering that. I’ve had pets euthanised and the vet will take them away and return with the body in a matter of minutes. Surely the drugs that work with animals will work with humans if the dose is increased.
Vets will generally anaesthetise an animal with an injection or gas then give a lethal injection. This means it’s the same for an animal, and therefore could be the same for a human, as having an anaesthetic before surgery.
Presumably the problems occour because in most countries doctors can’t inject drugs they can only prescribe tablets for a patient to take themself. Obviously the law could be changed to allow, but not force doctors to do so against their beliefs, doctors to give a general anaesthetic followed by lethal procedure so death is quick and painless. It would be interesting to see data from Dignitas in Switzerland regarding who euthanasia is carried out and average time to death.
We should go where the data takes us. No subject is taboo. This article is an excellent demonstration.
Thanks, Nick. A tough subject to research!
And leave that doodle a doodle please. We need you 😃
See you at the next DS Christmas bash.
Hancock’s midazolam and morphine cocktail worked well for hundreds if not thousands of elderly people, perhaps he should be called upon to oversee this latest iteration of democide….
I think it should be tried on him, to ensure it’s effectiveness first.
My mother committed suicide about 20 years ago. She was 69, had suffered what used to be called a nervous breakdown and was extremely depressed. The NHS had been giving her a cocktail of sleeping pills and anti-depressants for about 3 years and on at least one occasion they got the dosage they were giving her massively wrong which had exacerbated her problems.
Only a very few years later (maybe only 3, it’s hard to remember) there were reports in the papers that the anti-depressants she had been taking were linked to an increase in suicides.
She desperately wanted, in her words, to “go home to Jesus” and succeeded at her third attempt, which was a combination of a large number of over-the-counter painkillers and sleeping pills. The latter was presumably to ensure she didn’t wake up as the painkillers took effect. I have no proof but for various reasons strongly suspect that my late father “assisted the process.” If he did, it was his last act of (genuinely) caring for her and if I’m right, I applaud him for it. After the second attempt the medical authorities had said they would Section her if she tried again (and therefore out of his care) so the third attempt had to be done properly.
Suffice it to say I have learned from her experience.
Harrowing story, thanks for sharing nevertheless. The medical profession is, I feel, to be avoided at all costs. Especially the state sponsored bit.
I remember once visiting a walk in surgery to take them up on a flu jab (a previous life, over 15 years ago, when I had a modicum of trust in the “health” system!) and the GP told me he didn’t think I needed it and refused to administer it. Hats off to that professional. A rare breed. He made me think. At the time I felt rather indignant!
Hmmm, interesting. I’m becoming increasingly torn on this whole topic; there’s obviously a perfectly good moral argument for assisted suicide under certain circumstances. There’s also the very real issue of how to police our malevolent overlords abuse of power – pretty sure that can’t be policed. But there’s also the problem of people being in states of depression that are temporary – something I hadn’t given enough consideration to before, but really should have, as I have first hand experience of this. Twelve years ago, after finding myself in a huge amount of debt, and convincing myself people were better off without Mr Lemming, I tried to hang myself using the upstairs bannister as the anchor. Kicking away the chair I found myself dangling for a handful of panicked seconds before the upstairs wooden bannister pole snapped and I unceremoniously crashed to the floor. I can remember sitting there, with a sore neck, thinking “Can’t even f*ckin do that right. Fat bastard!”, and at that point I actually started laughing. That moment was pivotal in my life. I managed my sort my debt out shortly after and have never again considered anything similar. I’m now happy (or as happy as a naturally miserable sod can ever be). My wife is the only person that’s ever known about what I did, so I suppose this confession is some sort of late therapy. God knows. Anyway, the point is that, if I’d been successful, I’d have been one of millions of people who would have made an irreversible mistake, and assisted suicide will make this a whole lot easier.
I can’t know how low you must have felt to attempt that, but I’m glad you not only failed but also that the attempt didn’t cause you permanent issues
Thanks for sharing.
Bless you for educating us! Healing starts at the moment of Oblivion 👏
Thanks for the confessional, Free Lemming. It would scarcely be sensible to allow a medic to make a judgement on your real state of mind when you were not up to understanding yourself.
And presumably under these laws, for a doctor to say, “In my experience people who survive suicide attempts are usually glad to be alive – why not wait a bit?” would be considered illegitimate conversion therapy.
Wow— you are very courageous to make such a confession. I read somewhere that people who fail to kill themselves do often change their minds, and are glad to be still alive, so they never try it again.
Just to let you know you’re in good company, there was a news story years ago about a man in despair who decided to commit suicide by closing all the doors and windows in his small house and turning on the gas oven. But he got so bored with waiting that after a while he decided to smoke a last cigarette. The explosion blew him out of the house and into the next field. Completely unharmed, he was suddenly so glad to be alive that he never tried again, and lived a happy life thereafter.
Well done for turning your life around.
As someone who has also made an unsuccessful suicide attempt you’re story resonates with me. I would find it very hard to support assisted dying for people with mental health problems as, by definition, when in crisis they aren’t “thinking rationally”. However for people with very painful terminal conditions who have been judged by a professional to be “of sound mind” I definitely think they should have the right to pass away peacefully at a time of their choosing and would like this option to be available to me rather than have months, or longer, or a grim meaningless life in a care home. The biggest problem with assisted suicide would be avoiding a slippery slope which is something Canada has clearly been unable to do.
I guess the effectiveness of any “assisted suicide” scheme will depend on how the Uniparty frames the legislation.
If it is just another duty to add to doctors’ “busy schedule”, I guess it will be another request where you’ll be promised phone call in about six weeks time. If the doctor is busy, perhaps a call from the “practice nurse” (who turns out to be a medical student of some kind.)
But if the NHS adds this little task to their “Quality and Outcomes Framework” (whereby, like prescribing Statins, the higher the percentage reached, the more dosh the General Practice gets to share out between themselves), then I’m sure the UK will seen show those Canucks a thing or two.
Do Not Resuscitate? Not a problem!
Knowing Nick Rendell sounds like a hell of a risky business. My wife and I, and I’m in my 70’s, have never known anyone to commit suicide. But, my wife heard of two cases of friends of friends.
“Or that the Everlasting had not fix’d
His canon ’gainst self-slaughter! O God! O God!” Even Hamlet had a problem with suicide.
I don’t know anyone that has committed suicide, and I’m very old! Could it be association with the author that’s making these poor souls top themselves?
The Pierrepoint family apparently made ending someones life very quick and efficient. I’m not suggesting hanging as a method of assisted suicide but if their methods were so effective then it does seem that ending life can be easy and quick if done correctly.
I hate to suggest another level of bureaucracy but if assisted dying is officially sanctioned in this country then it stands to reason that there should be training and specialisation in the subject for those administering the method, rather than relying on our already overworked (and Hippocratic oath bound) doctors.