On August 25th, the ONS published on ‘Deaths involving COVID-19 by vaccination status, England: deaths occurring between April 1st 2021 and May 31st 2023‘ and an Excel datasheet.
Then, on October 20th, an Adjournment Debate on the Trends in Excess Deaths occurred. It was attended by Andrew Bridgen MP, a handful of other parliamentarians and the Westminster cat called Mog. Ostensibly, the debate was about the role (if any) of Covid vaccines and excess deaths.
On October 24th, in response to the debate, the U.K.’s Department of Health and Social Care (DHSC) released a document called ‘Trends in Excess Deaths and Covid-19 Vaccines‘.
We will spare you the safe and effective routine that seems to be the lot of any minister or public official and look at the data on which statements such as “There is no evidence linking excess deaths to the COVID-19 vaccine” are based. As a preliminary note, we should point out that vaccines should be plural as several varieties were being used, but it looks as if the Government cannot distinguish one from the other.
The DHSC document contains the following statement:

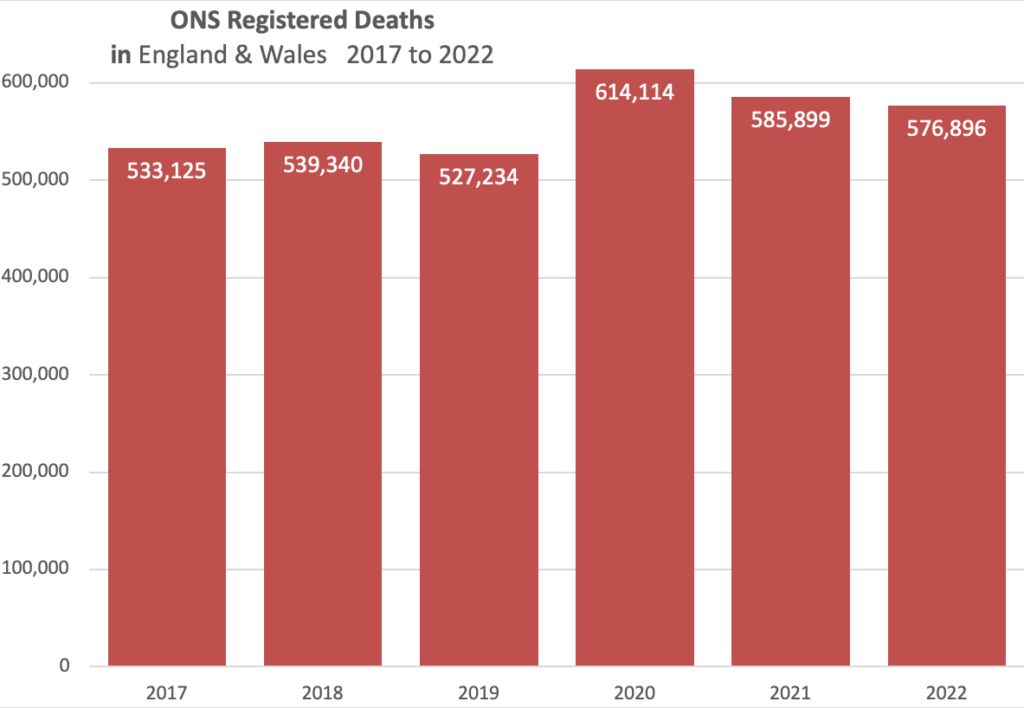
First, is the mortality rate in 2022 lower than in 2020?
The mortality rate is the estimated total number of deaths in a population divided by the total number of this population, expressed per 100,000 population, for a given year.
There were fewer deaths in 2022 than in 2020, so the mortality rate would be lower. However, this is an erroneous comparison as even the Office for National Statistics (ONS) removes 2020 data from its averages due to the high number of deaths in the first year of the pandemic. The ONS reports a five-year average (2016 to 2019 and 2021).
The number of deaths registered in 2022 in England and Wales was 6.2% above the five-year average.
However, let’s press on. The DHSC referenced data from the ONS, which have featured prominently in Trust the Evidence as an expert picker of cherries. It is helpfully hyperlinked with the lamentation that comparing vaccinated with those who remained unvaccinated is fraught with difficulties as non-coverage reached 4.6% of the population, so the confidence intervals around any estimates will be wide.
We would be slightly more cautious as coverage has varied over time, and boosters have reached an all-time low. Anecdotally, they are thought to be below 10% take-up.
Digging further on non-coverage (i.e., those who were not exposed to one of the Covid vaccines), we came up with estimates varying from less than 1% to up to 20%, but we are not even sure which age group or groups this applies to.
For example, we found statements such as “Over nine in 10 people aged 12 years and over in the U.K. had received one dose of a COVID-19 vaccine”. Fenton in 2021 estimated that up to 20% may have never received a vaccine. This stimulated a reply from the ONS to an FOI request. We also found this estimate of never vaccinated at 1,571,260 (estimate as of July 2021 for adults over 16 years). Confusing, is it not? Especially when the Minister’s statement is so black and white.
However, let’s again press on. We are not reassured that each candidate vaccine has been assessed and its potential harms monitored by the MHRA, whom we know does not investigate deaths thoroughly, is 75% funded by industry and has transitioned from “the watchdog to the enabler” according to Dame June Raine, the Chief Executive of the MHRA.
The core of the Government reassurance is based on the dataset called ‘Deaths between April 1st 2021 and May 31st 2023‘, released in August this year. As usual, it is helpful to read the definitions before looking at the data. So, what definition did ONS use:
Following guidance from WHO, the ICD-10 codes U07.1 (COVID-19, virus identified) and U07.2 (COVID-19, virus not identified) have been used to record deaths from COVID-19 since 2020.
We hear you ask: if the virus has not been identified, how do they know it’s Covid rather than, say, influenza or streptococcus pneumoniae or something else? Ah, stop splitting hairs; let’s carry on, please!
Table 1 of the ONS ‘Monthly age-standardised mortality rates by vaccination status for all-cause deaths, deaths involving COVID-19 and deaths not involving COVID-19, per 100,000 person-years, England, deaths occurring between April 1st 2021 and May 31st 2023’ shows that 1,038,215 people died of all causes, 986,395 who were ever vaccinated and 51,730 who were unvaccinated.
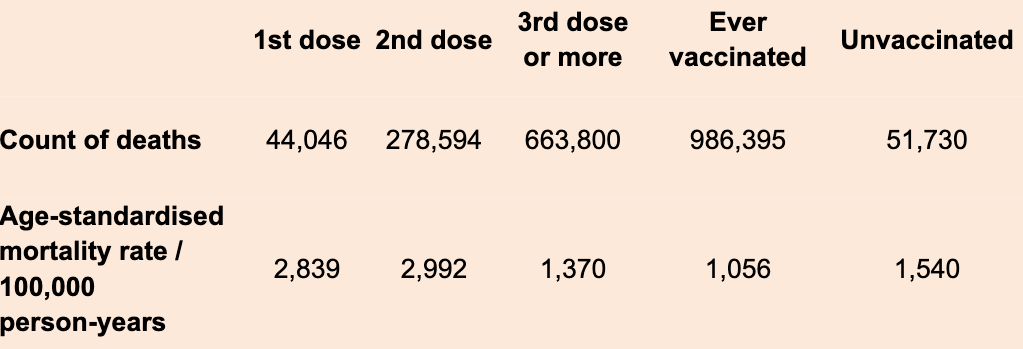
There’s something odd about these data: the age-standardised mortality rate per 100,000 person-years is higher for the first and second dose, but then the third dose or more drags it down – particularly the fourth dose looks like it does.
To make sense of these data and make statements that there is no evidence linking Covid vaccines to excess deaths – as the DHSC does – we need to be sure that the ever-vaccinated number is accurate and that the groups are comparable.
As an example, for comparability, we don’t know the number of people who were exempted from the vaccination, for instance, because they had a terminal condition and were going to die imminently. The fourth dose may include low-risk people such as healthcare workers, armed forces, security people and so on. We need clarity to make sense of any comparisons. At the very least, the ONS should try and propensity match sets of treated and untreated subjects.
For accuracy, we don’t know how many were not exposed in the unvaccinated group – we don’t know the denominator. The ONS counts only the people both registered in the 2011 census and registered with a GP in 2019.
Professor Fenton considers it more than double the ONS estimate, increasing the age-standardised rate to over 3,000. It could be even higher as the number of people who have never been vaccinated is currently unclear. ONS methods can only produce a rough estimate, and its current methods underestimate the denominator for the unvaccinated – the size of this underestimation needs to be clarified.
Further problems accrue when we look for reliable denominators. We found some denominator data from the ONS ‘Number of vaccines given by report date‘ referring to the period October 1st 2021 to May 31st 2023, so not quite the same as the numerator data. In addition, the ONS page is unclear whether the third dose data include those who received further doses (the over-three categories). Piling the problems on, the numerators refer to people aged 18-plus, but the denominator data have no age breakdown.
We carried on, noting the lack of transparency and clarity in the Government’s stats.
ONS does provide breakdowns by age group for numerators. Still, we could not find the same for denominators, meaning we know how many people died in, say, the 40-49 group by exposure but not how many people were exposed in that age group. ONS provides a standardised person-years rate with a link to its methods, but the raw data on which the person-years are calculated are not available.
In addition, text such as “To calculate the ASMRs [age standardised mortality rates] by vaccination status, those aged under 10 years were not used, as the associated dataset includes only those aged nine years and over because it is linked to the 2011 census” makes describing, understanding and analysing these data impossible.
Given the age structure, the only conclusion we can draw is that the Government should explain to all of us, step by step, the methods used to reach the sweeping conclusions in the statement, accompanied by all data, warts and all.
Poor quality data and analyses and lack of clarity have beset the Covid pandemic. We also cannot assess the integrity of the ONS data: some of the data entry points are concerning. For example, there is a death counted in April 2021 for a third dose or booster given at least 21 days before (so March 2021). The vaccines were first rolled out on December 8th 2020 (by October 2021, deaths started to be counted against the fourth dose or booster).
To add to our confusion, the ONS report in the vaccine tables the deaths for April 2021.
Ever-vaccinated had 28,175 deaths, and the unvaccinated 3,577 deaths. However, from ONS weekly deaths for weeks 14-17 (April) in 2021, there were 39,169 deaths. The difference is 7,417 deaths. We checked between April 1st 2021 and May 31st 2023, where 1,038,215 people were counted as having died of all causes. Yet, in the ONS data from week 14 of 2021 to week 21 of 2023 (26 months of data, from the beginning of April to the end of May), there were 1,239,287 deaths. So, the vaccine counts are missing just over 200,000 deaths – where have they gone?
What are we to make of this discrepancy?
Answering questions about excess deaths cannot be done in days as the DHSC did – using inaccurate statistics further undermines confidence in patient safety. The only way to assess excess deaths is to undertake a thorough investigation, as we first pointed out in August 2022 and on several other occasions.
Simply throwing out numbers – as the ONS does – undermines confidence, which is already at an all-time low. No one checks the data; it’s about time someone did.
Dr. Carl Heneghan is the Oxford Professor of Evidence Based Medicine and Dr. Tom Jefferson is an epidemiologist based in Rome who works with Professor Heneghan on the Cochrane Collaboration. This article was first published on their Substack, Trust The Evidence, which you can subscribe to here.













To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
“Grant Shapps faces Tory mutiny over hydrogen levy plans”
Not put off by the billions wasted on badly thought out plans to counter the thing that isn’t happening, we’re going to double down, again..?
“Insolent, unproductive and dominated by HR, the Civil Service thinks it rules Britain”
‘Release them back to the private sector’.? They wouldn’t last a morning in the private sector.
“They wouldn’t last a morning in the private sector.”
Absolutely correct. The senior civil servants I came across when I worked amongst them were thick, arrogant beyond belief, clueless job-wise and masters at ducking and diving. Of the scores I cam across only two would have stood a chance working in the private sector.
It and the people are not much different in the large corporation part of the private sector anymore.
Igor has made an interesting discovery using UK data regarding a significant increase in hospitalizations 6 months post Covid booster;
”The most important fact we see is that for people over 50, the most dangerous period after vaccination is between 6 and 9 months after their last dose. Their risk of hospitalization is several times higher than before six months or after nine months. The increase in risk far outweighs a small reduction in the first six months.
So, people who take a Covid booster first go through a somewhat reduced hospitalization risk for the first six months, then go through a dramatically heightened risk of hospitalization, then hospitalization rates “return to normal,” with the normal being very high. Does that look like the vaccine provides any benefit? Not to me!”
https://igorchudov.substack.com/p/ukhsa-boosters-greatly-increase-covid
Neil Oliver
Well said, that man. Much sense spoken.
Just a thought on ULEZ:
Are these prisons being built in preparation for Billy’s next release?
“Catastrophic Contagion” is apparently going to be the big one. How much more effective and targeted would it be if people were closely confined in 15 minute cities?
Excellent point Hux, ref the LTNs especially, something I’ve been ruminating on too.
I also wondered about the power supply required by all that additional surveillance: the local town is just finishing off it’s 2nd ‘smart junction’ and about to start a 3rd, the multiple cameras of which are all cabled. As are the many additional street cameras installed during the lockdowns – all while we’re being told to freeze to death in the dark at home. How’s that supposed to meet Net Zero then?
“I also wondered about the power supply required by all that additional surveillance”
This is where the £37 billion on Track and Trace went, something I have mentioned numerous times – smart junctions, smart cameras. T and T was never just about a bloody app.
Hey don’t forget about ‘Outbreak 24’, the SARS-5 plandemic scheduled for next year. They’re keeping us guessing obviously. Wow these pandemics really are like buses…
They’re keeping us guessing obviously. Wow these pandemics really are like buses…
I’ve not heard of ‘Outbreak 24’ Mogs. Can you post a link?
https://rumble.com/v28nqro-outbreak-24-simulazione-della-pandemia-2024-dove-il-virus-sars-cov-5-creer-.html
This simulation was in Italy in 2021. There’s probably plenty more that we’re not even aware of. Obsessive b’stards!
Many thanks Mogs.
“Fake trans applicants ‘could trick universities’”
But but but aren’t straight A pupils – whatever their race, creed or colour – simply a result of white privilege? It’s only your pronouns that count these days…..
…and this just in from down under:
https://rumble.com/v297guk-february-11-2023.html
I was appalled to learn that the Guardian loons had accused Neil Oliver of antisemitism. To accuse someone of antisematism because they talk about global elites and their out in the open conspiracies is disgusting.
Made me feel quite sick
The Groan is a sickening travesty of a publication even by the sickening standards of the MSM.
Interesting take by Craig Murray on the Sy Hersh story. https://www.craigmurray.org.uk/archives/2023/02/sy-hersh-and-the-way-we-live-now/
“… But what most worries me about the entire story is the unanimous complicity of the mainstream media in ignoring the completely obvious.
The media line, parroted here relentlessly by the BBC and corporate media, was that the Russians had probably themselves blown up the pipeline on which they had expended such great resources and three decades of intense diplomatic activity, and which was to be the key to Russia’s single most valuable source of income for the next 40 years.
This was always quite literally incredible. You would have to be deranged to believe it.
It actually taught me not just that we truly are in the realm of totalitarianism and the Big Lie, but I learnt something very important about how the Big Lie works.
The secret is not that people genuinely believe an outrageous claim. The secret is that people do genuinely believe that they are in a battle of good against evil, and it is necessary to accept the narrative being promoted, in the interests of fighting evil.
Don’t question, just follow. If you do question, you are promoting evil.
I am sure that is how it works.
State and corporate stenographer journalists are actually intelligent individuals. If they thought about it, they would realise that the narrative that Russia blew up its own pipeline is obvious nonsense.
But they are convinced it is morally wrong to think about it…. ”
There is also the not to be overlooked issue of the No2Nato event on 25.2.in London having to go underground.
That development aloneis actually a confirmation of Peter Hitchens fear already having become reality.
He suggests attending it even if you disagree but are pro free speech.
https://www.theparliamentmagazine.eu/news/article/edible-insects-european-union#:~:text=In%20May%202021%2C%20the%20European,the%20house%20cricket%20in%20March
A load of crap about…crap.