
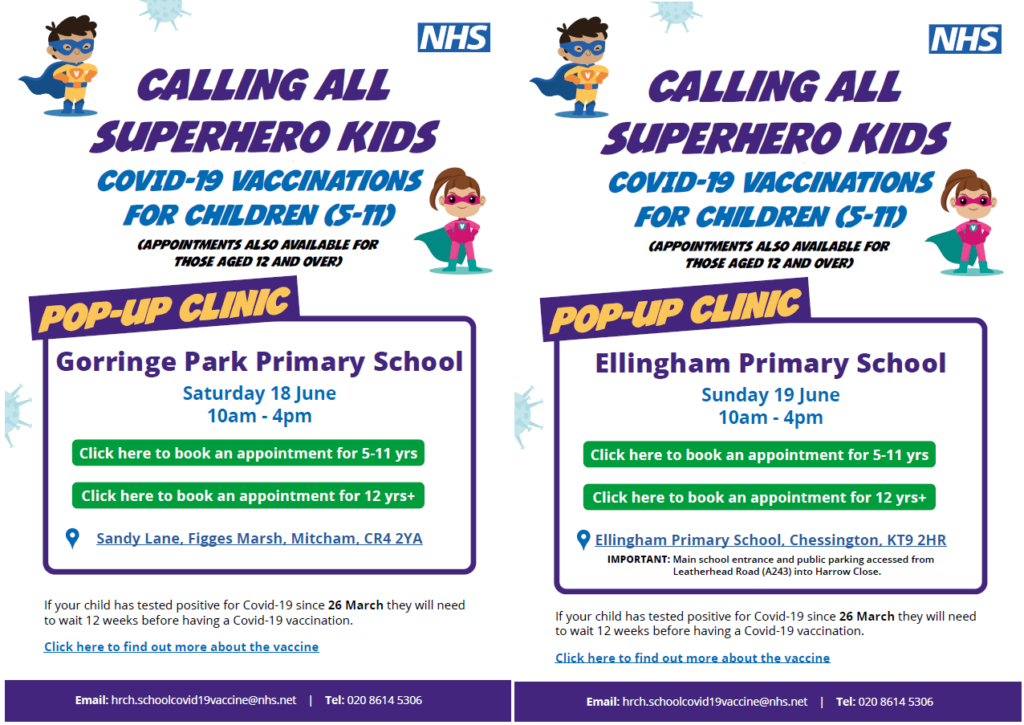
In June 2022 I was moved to write this article in response to a disturbing NHS COVID-19 vaccine advertising campaign, which appeared to be directly targeting children aged five to 11 years by using cartoon superhero characters and a party invitation style leaflet promoting COVID-19 vaccine pop-up clinics for primary school-age children. Although sent to their parents, the poster directly addressed children with the bold title ‘Calling All Superhero Kids’ and was designed in the style of a children’s party invitation, with cartoon superhero branding, large writing and bright, eye-catching colours. At the time I commented that:
For the NHS to be directly targeting young children under 12 to encourage them to take a novel medical treatment and in such a superficial and coercive way is completely unethical and abhorrent.
I was shocked to see a similarly unethical initiative advertised on a London GP practice’s social media a few days ago. Its tweet (now removed following our comments– photo below) was excitedly advertising its ‘Annual Peppa Pig’s Flu Clinic’ with promises of party food, soft play and other kids activities, as a fun and desirable setting to receive their flu vaccine.
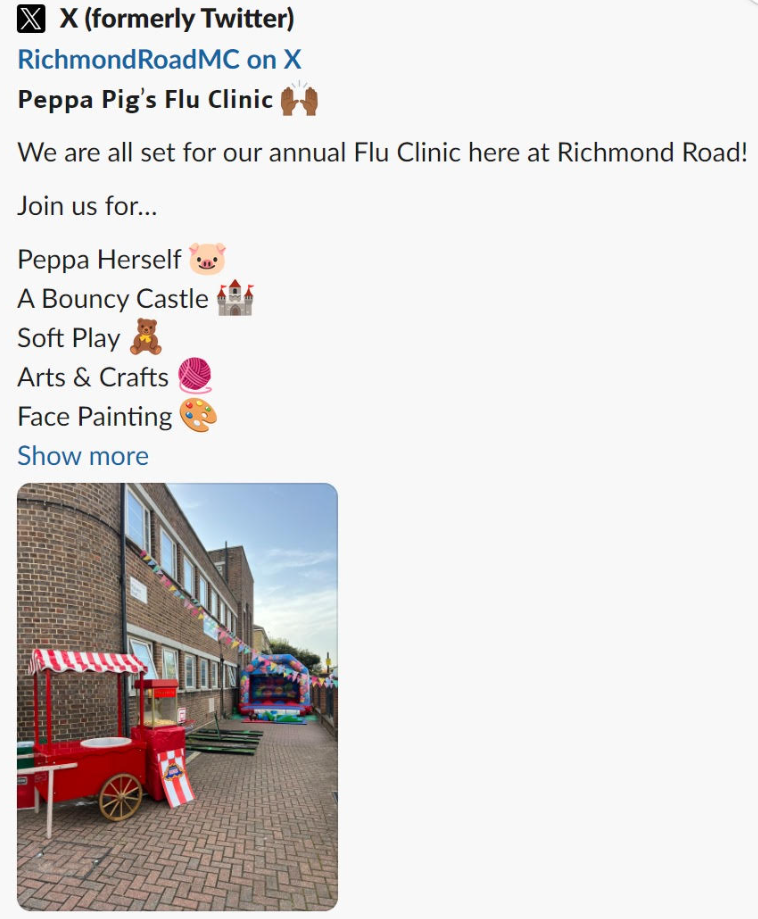
Further investigation revealed that the Richmond Road Medical Centre’s Peppa Pig Flu Clinic has been running since 2021, with a post promoting the 2021 clinic on the GP practice’s Facebook page and this 2022 clinic highlights video and event update below posted on their website:
Peppa Pig’s Flu Clinic – September 2022
We had a brilliant turnout at our second Peppa Pig themed flu clinic at the Surgery.
In response to the local Polio outbreak, we also offered polio boosters to eligible children. The event was action-packed with an array of fun activities for the children to enjoy which included face-painting, arts and crafts, a bouncy castle and of course the chance to meet and greet Peppa herself!
Dr. Jonathan Engler, Co-Chair of HART, also flagged up in this tweet another poster from Richmond Road Medical Centre, using the same Peppa Pig marketing but this time to plug its COVID-19 Vaccine Clinic for “vulnerable” children – which in reality includes perfectly healthy children who live with a so-called “vulnerable” adult.
At this stage, when multiple organisations and doctors around the world (including the World Council for Health in November 2021 and Dr. Peter McCullough in a speech in the EU Parliament in September 2023) have called for the complete withdrawal of COVID-19 genetic vaccines from the marketplace, citing data that the risks outweigh any benefits for all cohorts, particularly for younger people, it is indefensible that medical authorities in the U.K. are still giving these products to children.
As the CEO of the U.K. Medical Freedom Alliance, one of the U.K.’s leading voices on medical ethics, I have recorded and published a video statement calling out the complete violation of medical ethics in creating this event – full transcript below.
This statement is in response to shocking images of ‘Peppa Pig’s Flu Clinic’ on Richmond Road Medical Centre’s Twitter feed. It appears to be using the
popular children’s cartoon character Peppa Pig (along with party food, soft play and other kids’ activities) to advertise and promote flu vaccines to children.I would like to remind the NHS, medical organisations and healthcare professionals responsible, that laws and ethical and professional codes enshrine
the principle of properly obtaining informed consent for all medical interventions. As well as requiring a full explanation of risks as well as benefits, they specify
that coercion and bribery must not be used. In addition, the Human Medicines Regulations Act 2012 outlaws the advertising of medical products.The cynical use of cartoon characters, bouncy castles, face-painting and popcorn to promote vaccines to children, prompting ‘pester power’, is unacceptable.
This sinister behaviour and marketing should have no place in the sober and ethical provision of healthcare, especially to children who are particularly vulnerable
to this sort of exploitation.
At the U.K. Medical Freedom Alliance, we are deeply concerned about manipulative and unethical marketing of vaccines directly to children, and the use of inappropriate and coercive settings to deliver these injections, such as this party clinic, which makes informed consent impossible and makes children vulnerable to exploitation for material gain by the pharmaceutical industry. This culture of ‘medical grooming’ of children must stop now and as parents we must protect our children and demand that they are not targeted in this way
Dr. Elizabeth Evans is CEO of the U.K. Medical Freedom Alliance.












To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
It’s beyond unethical. It’s demonic.
Damn right, Stewart!
Fantastic article… but utterly unconscionable behaviour.
People are avoiding these ‘therapies’ on a large scale, so one can only assume this is only about money.
And if it’s not, let them have a full and frank debate, with all the up to date evidence and REAL informed consent.
So evil
This has reached a new level of twisted now. What I would like to know is whether this type of aggressive, false, and immature marketing stunt has any impact on vaccine uptake in children? Are people still so uninformed that they’ll take Peppa Pig’s word for it if she tells parents their children will benefit?
To any rational mind, surely such events would give pause for thought as to the real motivations behind “vaccine” campaigns?
If these jabs were provably beneficial, the sober evidence would be there, freely available with links to the relevant peer-reviewed studies that demonstrated unequivocally that the benefits outweigh the risks for all age groups. But it isn’t, so they need to bring in Peppa Pig to blag about it and brainwash young minds, and appeal to the “Superhero” aspirations of children so they can experimentally alter their genes.
It breaches laws, medical ethics, and the basic morals common to all humanity!
When they come for our children…. Its a hill I’m prepared to die on.
And the response from the GP practice is…….?
Ultimately Fishy and the rest of his government are responsible for this. They know damn well that a phone call to the appropriate earhole could stop this immediately but they have done nothing. Guilty.
A more aggressive response would be to list all the doctors and nurses working at this Practice along with their mugshots. Let’s see the cowardly response to that.
Name and shame.
huxley, re “…list all the doctors and nurses working at this Practice along with their mugshots…”
The question is – how are these doctors and nurses obtaining informed consent for administering this vaccine product?
What information are they giving to parents to justify their children being subjected to this medical intervention?
See my previous comments which indicate children don’t need this medical interference.
What on earth is going on in the medical ‘profession’ that these people are being recruited to foist upon the population unnecessary medical interventions?
This is a scandal of ginormous proportions which is coming to a head now with the Covid and flu vaccination scams.
How do we obtain accountability, particularly against rogue governments which are operating as handmaidens to the pharmaceutical industry, along with the medical profession?
A fine post. 👍
The notorious Anthony Fauci co-authored an article published in January this year, admitting: “As of 2022, after more than 60 years of experience with influenza vaccines, very little improvement in vaccine prevention of infection has been noted. As pointed out decades ago, and still true today, the rates of effectiveness of our best approved influenza vaccines would be inadequate for licensure for most other vaccine-preventable diseases.” (My emphasis.)
So how are these flu vaccine products still being approved today?!?!
It’s mind-boggling how people have been exploited for years with rubbish flu vaccine products – how much has this racket cost taxpayers I wonder? How much damage to health is being done with these repeated medical interventions that are of little or no benefit re flu?
It seems to me this is out and out fraud…
And consider how children are the target for this scam, apparently tying them into the flu vaccine market for life, with vaccine products they don’t need.
This was admitted during a Lords committee meeting in the UK in June 2020, by Peter Openshaw from Imperial College London (also home of the notorious ‘modeller’ Neil Ferguson).
Peter Openshaw was present at the meeting as one of the members of the UK’s Sage scientific advisory group Nervtag, advising on the Covid-19 response. According to a report in the Guardian, Openshaw was advising the Lords committee that “A vaccine against Covid-19 may not work well in older people who are most at risk of becoming seriously ill and dying from the disease…which may mean immunising others around them, such as children.” (My emphasis.)
Openshaw said: “Sometimes it is possible to protect a vulnerable group by targeting another group and this, for example, is being done with influenza. In the past few years the UK has been at the forefront of rolling out the live attenuated vaccine for children.” (My emphasis.)
According to the Guardian, Openshaw said “giving the nasal spray flu vaccine to children who do not often get severe flu protects their grandparents”. (My emphasis.) Openshaw was using this example to justify giving Covid-19 vaccine products to children and health and care workers, to “also help protect older people who have the most contact with them”.
What do you think about this? About children and others such as health and care workers being given flu and covid vaccines to protect the elderly? That is, adults and children who aren’t at serious risk of either flu or ‘Covid’ being pressed to sacrifice their own naturally effective immune response, and being vaccinated, repeatedly, to purportedly protect elderly people – is this ethical?
How do we effectively take this on, challenge unnecessary vaccinations being pressed upon people who do not need this medical interference?
How is informed consent being obtained for this racket?
Further to my comment above, I was so shocked after reading the report in the Guardian I referred to, I raised this matter in August 2020, in a BMJ (aka The British Medical Journal) rapid response, please see:
Is it ethical to vaccinate children to protect the elderly?
Again, what do people think about this?
Is it ethical to vaccinate people who aren’t at serious risk of disease to purportedly protect another group – e.g. vaccinating children to purportedly protect the elderly against flu or covid?
We have to demand accountability for this gross exploitation of people, including children, with unnecessary medical interventions such as vaccines.
Further to my comments please have a look at the email I sent to Peter Openshaw and Arne Akbar in September last year – Is it ethical to vaccinate the young to purportedly protect the old?
We have to address this now – they are brazenly jabbing children to purportedly protect old people – this is unethical!
It is in fact literally criminal.
Jabbing without informed consent is a criminal offence.
Terrific.
See also this article re flu vaccination of children in France – they’re coordinating a campaign to exploit children with these products, this must be challenged now.
Why Vaccinate Healthy 2- to 17-Year-Olds Against Influenza? Medscape, 17 October 2023
Ha! I bet the manufacturers aren’t ‘fazed’ at all! Rather rubbing their hands with glee at children being roped into this racket…
How is this happening, this gross exploitation? How can the medical profession be going along with this? Have they no idea at all of their legal and ethical obligation to obtain informed consent for vaccination?!
The medical profession carrying out this cannot be considered as professional.
Its not just children [NB. MPs are crap – they are the ones letting this go on day-after-day year-after-year and say and do nothing – total corruption at every turn – with honourable exceptions like Bridgen and Chope – and dishonourable ones IMHO like Penny Mordant].
This official misinformation [lies IMHO] specifically about ‘flu and covid injections is from an email sent recently to all 65s and over [see also post in these comments by Elizabeth Hart]:
“More information
Seasonal vaccinations have proven safety records. They give you better protection than any immunity gained from previous infections.
………
Kind regards,
Dr Nikita Kanani MBE
GP and Deputy Lead
NHS Seasonal Vaccination Programmes
NHS England
Have they no shame? GMC referral is indicated as a mater of urgency! The doctors involved should e struck off!
Crazy, evil world.
TPTB and their ‘followers’ are happy to manipulate children, by lying, to get highly questionable substances into their bodies…but children and younger persons must not be subjected to the perils of ‘betting / gambling’ involving well-known characters who may influence them.
https://www.manchestereveningnews.co.uk/news/greater-manchester-news/sky-bet-tweet-featuring-manchester-27925824
Gambling with their health and life with ‘health’ products is ok, then?
EVIL
Very very well said this diabolical practice has got to stop and those promoting it held to account.
Unbelievable the medical professionals have failed us – period.
Is there a Cos Play freedom fighter outfit, just for Mark Dolan.