
Wokery and Government overreach are the great issues of the early 2020s. Lucy Letby isn’t of the same order. Nevertheless, this young woman, of previously blameless character, has been imprisoned for the rest of her life on circumstantial evidence. With rare exceptions, the media have relished turning her into a ghoul. They are ably assisted by the Cheshire Constabulary who, post-trial, drip-feed corroborative detail to add verisimilitude, as in Gilbert and Sullivan’s ‘The Criminal Cried’. They tell the media that Letby kept an “encrypted diary”, with “L.O.” having some sinister meaning. In fact, Letby has a cursive script and it’s L.D. not ‘L.O.’, being nurses’ common shorthand for ‘Long Day’, or a 12-hour shift. They’ve auctioned the film rights for their investigation, with ITV placing the winning bid. I’d advise ITV to check carefully for spin.
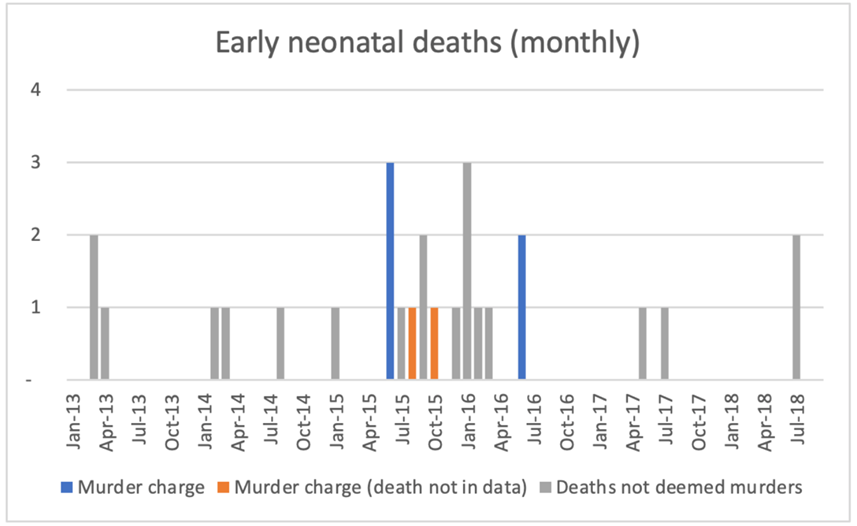
No one who cares about justice should be comfortable with this case. To briefly re-cap: Ms. Letby worked at the Countess of Chester neonatal unit from 2012. From at least 2014 this was a Level II unit, meaning that it took very premature babies. From mid-2015 to mid-2016, 15 infants died and a similar number had major collapses. This was far more than in the preceding and subsequent periods (figure 1). The consultants raised alarms, leading to internal investigations then a review by the Royal College of Paediatrics and Child Health (RCPCH), commissioned in mid-2016.
Concern about Ms. Letby arose early, and she was moved to a desk job in July 2016. In response she began a grievance procedure, claiming that doctors were persecuting her. At this stage their concern surely related to competence; no Royal College would touch an investigation that should properly be a police matter. Assertions that “Doctors suspected Letby from 2015” should be read in this light. Post-mortems, performed for six of the seven deaths for which Letby ultimately was convicted, recorded “natural causes”.
Initial findings were in Ms. Letby’s favour. Her grievance was upheld and the RCPCH report, released at the end of 2016, expressed concern about the unit’s staffing and safety, saying that it was unsuitable for Level II. By then it had been downgraded to Level I anyway, with the most premature and sickliest babies delivered or sent elsewhere. There’s no mention of Ms. Letby or any other staff member, but it is beyond credulity, given the consultants’ suspicions, that she wasn’t quietly discussed. Doubtless there were separate confidential communications. They can’t have been damning, for Countess of Chester management notoriously forced the consultants to apologise and indicated that Letby would resume clinical nursing. Unhappy with these outcomes, the consultants involved the police in the spring of 2017, igniting the powder trail.
A 10-year retired paediatrician and professional expert witness, Dr. Dewi (David) Evans was recruited by the police. By his account he reviewed 30-something deaths and collapses, distinguishing 15 (eight murders and seven attempted murders) for which Letby was charged. Unfortunately, we don’t have his workings, nor the exact reason why he excluded seven deaths, except that he told talkRADIO that “they died for the usual problems why small babies die: haemorrhage, infection, congenital problems”. Nor do we know why the judge threw out one murder charge.
Now, go to figure 1 and examine the critical mid-2015 to mid-2016 period. Even if one removes the seven deaths for which Letby was convicted (orange and blue), the remaining eight (grey) form an excess cluster compared with the previous period (the subsequent period is not comparable owing to the unit’s downgrade). That means that we are asked to believe that Letby’s murders coincided, quite by chance, with a spike of other excess deaths, all of them unsurprising. I’d accept this if Letby was a strychnine poisoner, if seven babies died from strychnine and seven died owing to a concurrent viral outbreak. It’d be shocking, but clear. But these were highly-vulnerable babies, mostly premature and with other health issues. Do the suspicious and non-suspicious excesses really divide so precisely? A lifetime in biology and medicine tells me it’d be remarkable if they did. Biology and medicine are full of grey zones.
Dr. Evans says that – very correctly – he was working blind to whether Letby was present at a death or collapse or not. But, given the complexity, why was he the sole reviewer? And how does that much-published list of nurses’ presence and events look if all events, suspicious or otherwise, are included? Was she also present at many non-suspicious events? Maybe she just worked a lot.
The causes of death Dr. Evans found variously included air embolism in the blood (infants A, D) or stomach (C, I and P) or interference with nasogastric tubes (infants E,O). They differed from the natural causes identified at post-mortem by coroners’ pathologists, from whom we heard nothing at the trial. Methods of attempted murders included insulin poisoning (infants F and L), excessive feeding (infant G) and traumatic assault (infant N).
Even if we reject the contemporaneous post-mortems and accept Dr. Evans’s later diagnoses, air embolism is not proof of deliberate injection. A PubMed search combining “air”, “embolism” and “neonates” yields 271 hits. If I then add “infection” I retain 37 hits and if I instead add “enterocolitis”, I have 17. Sato and colleagues describe an infant with bacterial peritonitis producing so much gas that ultrasound revealed “intravascular microbubbles moving into a pulmonary artery”. Smith and Els describe four fatal cases of infant cardiac embolism (i.e., air in the heart) and underscore the hazard of air being accidentally or negligently introduced in infants with difficult venous access. Beluffi and Peroti describe air embolism as a “rare complication of intensive care, noting links to enterocolitis (i.e., gut infection), surgical procedures and infant respiratory distress syndrome (which they call hyaline membrane disease)”.
The possible role of infection should be underscored. The Chester unit’s sewage system, or that of the ward above, was defective, providing an obvious source of infection. That is why the hospital plumber, called as a defence witness, visited repeatedly. Contaminated water systems notoriously cause clusters of neonatal unit deaths. What outbreak investigation was done at the time? Any? None? Were sewage leaks the reason why the Unit was later rebuilt?
Turning to the two insulin cases, which played a major role in the conviction: why was no alarm raised about extraordinarily high readings? A clinical biochemistry department signed them off and a paediatrician received them. Did either read them? The second case (Baby L) was in April 2016, when the unit staff were acutely aware of a string of adverse events. For baby F, in August 2015, there’s the question of how the insulin was delivered. The prosecution alleged it was via an intravenous feed bag rigged to run over 48 hours. But this bag had to be changed after Letby went off-shift owing to problems with the line. As her defence pointed out, it’s inconceivable that it’d be replaced with the one other bag that she’d also spiked or that, if she’d spiked multiple bags, there was no cluster of insulin-poisonings. What really happened is deeply uncertain, and the blood samples were discarded long ago.
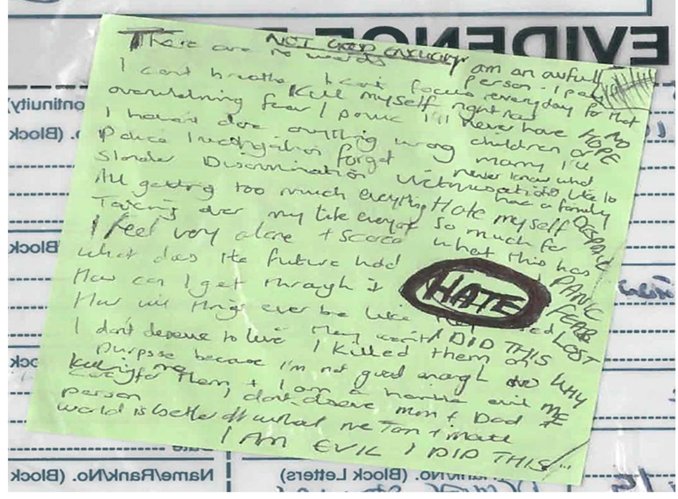
Dr. Evans’s analysis was one major factor in Letby’s conviction. The other was her own notes, most notoriously one on green paper (figure 2). This includes the much-quoted phrases: “I killed them on purpose because I’m not good enough to care for them”, “I’m a horrible evil person” and “I am evil, I did this”.
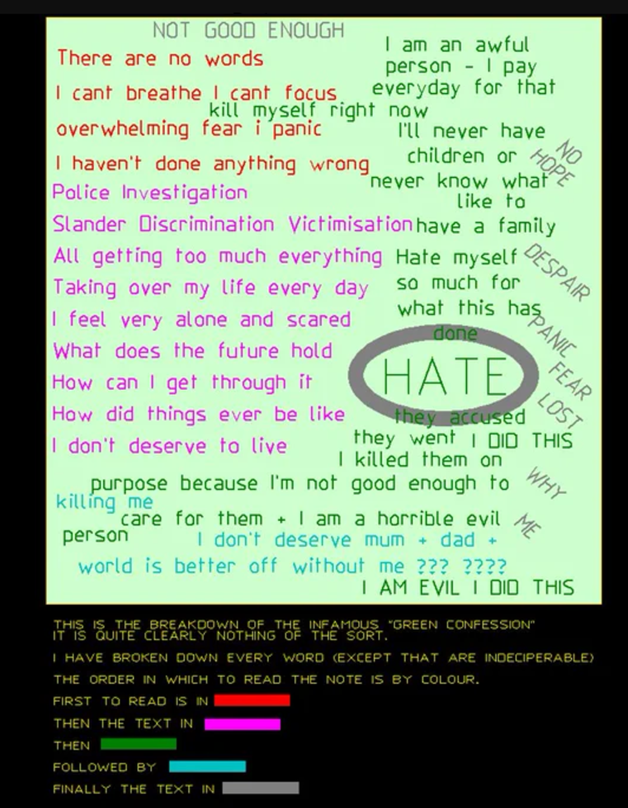
Reading the note is tricky. Words overlap and those on the same line do not always belong to the same sentence. The most convincing decrypt I’ve seen asserts that it was written in five parts shown, colour coded, in figure 3 (though I’d put everything in block capitals into the grey block).
Much is a stream of fear and self-loathing but what’s critical is in green, bottom right, below the heavily encircled “HATE”. This reads: “They accused; they went…”, followed by those claimed confessions. “Accused” isn’t certain to me, being obscured by the heavy circle around “HATE”, but the meaning is clear from “They went”, which is to say that “They [the police] asserted that…”. Read that way, it’s a shell-shocked woman describing a police interview, not a confession.
I do not know that Ms. Letby is innocent. I wouldn’t be surprised to learn she wasn’t the world’s best nurse, nor that the doctors had legitimate concerns about her competence. But I am far from convinced that she is a murderess on the evidence that has been presented.
She worked on a Level II unit that, based on the RCPCH report, wasn’t fit for purpose. Her ‘killing spree’ coincided with an excess of other deaths that the principal expert witness says were “due to the usual problems of small babies”. Air embolus – if it was the cause of death – was diagnosed long after the event and can arise for other reasons besides malicious injection. Her ‘confession note’ can be construed very differently. In a remarkably similar case, a Dutch nurse, Lucia de Berk, was convicted of neonatal murders based on circumstantial evidence and an ambiguous diary, then exonerated. Many think that Letby’s defence barrister failed to make the best of her case, with no expert bar the plumber called on her account. It is vital that she is allowed an appeal.
It is vital too that the pending Statutory Inquiry interprets its brief as widely as possible, and considers the possibility, however small, that it is built upon a false premise. The Countess of Chester Hospital was not a happy place to work. In December 2015, one unnamed paediatrician wrote to the management: “Over the past few weeks I have seen several medical and nursing colleagues in tears… they get upset as they know that the care they are providing falls below their high standards,” adding “chronically overworked” and “no one is listening”. Doctors and the hospital management clearly disliked and distrusted each other. Dr. Gilby, who became CEO after Letby’s arrest, is now suing for constructive dismissal, asserting she was bullied and undermined by the Trust Chairman.
Isn’t this the perfect setting for care to go horribly awry, without foul play? Or have we reached the point where it becomes expedient to blame miscreant nurses for the NHS’s failings, just as our 17th Century forebears attributed societal calamities to witches?
Dr. David Livermore is a retired Professor of Medical Microbiology at the University of East Anglia.












To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
The current leftwing lie that fascism/Nazism came from the Right is obviously designed to divert attention from the contemporary Left’s support for the despotic total-control state. However, the lie was created and first used by the Bolshevik-controlled Comintern of the 1920s. (“The Faces of Janus: Marxism and Fascism in the Twentieth Century” by A. James Gregor shows how the lie was invented and developed.) It is the Comintern that is the source of the madleft’s “anything I don’t like is fascist” infantile lunacy.
For more detail on the leftwing origins of fascism, I recommend L. K. Samuels “Killing History: The False Left-Right Political Spectrum”. In 500 pages of detailed quotes Samuels proves that fascism and Nazism came from the Left. Interestingly, Samuels had a run-in with Wikipedia (the pseudo-encyclopedia) when he published an article showing, by using a quote from Mussolini’s own writings, that Mussolini thought of himself as a leftwinger. Wikipedia deleted the page because Samuels refused to delete the word “left” from the Mussolini quote.
I’ve always taken politics to be a clock face with the centre at 12 and totalitarianism at 6. No mater which way from 12 you go, whether to the rights towards 1 or the left towards 11, if you keep going you end up at the same place. “Fascists” to the right, “Communists” to the left.
Except, there are no Nazi’s or Fascists to the right and there never has been as Jeff admirably points out above. They are simply handy terms corrupted by their owners who simply disavowed the terms.
Excellent points and facts there Jeff.
No Fascism in stolen elections….
Thank you for this.
“However, the lie was created and first used by the Bolshevik-controlled Comintern of the 1920s.”..
Why would they lie, to what gain?
And who were the Bolsheviks?
How has this lie gained traction for over a century?
This is extremely important, so much of history is a lie, so much has been turned on its head…
“To speak the truth is a petit-bourgeois habit, a luxury of worry-free and aimless people. To lie, on the contrary, is often justified by the lie’s aim”
Lenin
“A lie told often enough becomes the truth”
Lenin
“If you tell a big enough lie and tell it frequently enough, it will be believed”
A. H.
“It is not truth that matters, but victory”
A. H.
“Accuse the other side of that which you are guilty.”
Joseph Goebbels
“If you tell a lie big enough and keep repeating it, people will eventually come to believe it. The lie can be maintained only for such time as the State can shield the people from the political, economic and/or military consequences of the lie. It thus becomes vitally important for the State to use all of its powers to repress dissent, for the truth is the mortal enemy of the lie, and thus by extension, the truth is the greatest enemy of the State”
Joseph Goebbels
I came across a speech made by A. H. in 1937. Here is an excerpt and the wording and sentiment are firmly on the left.
“…For you must also understand this, my people’s comrades: No leader can use more strength than his followers give him! What am I without you? What you do not give me, I can never use for your own benefit! If you refuse me your unanimous unity, what should I do?! I am a single man, I can possess the best will. The will is not worth more to you than your will is worth to me! And that brings us to the problem of freedom! Freedom, yes! Insofar as the interest of the national community gives the individual freedom, it is given! Where the freedom affects or even impairs the interests of the national community, the freedom of the individual ceases! Then the freedom of the national community takes the place of the freedom of the individual!”
That’s the bit Dr Alexander left out of his article: People who like to pose as a right-wing – typically, they’re closet communist neoliberal anarchists – also want to call their opponents Nazis. Hence, Hitler and the NSDAP keep flipping from extreme-left to extreme-right, depending on who presently wants to abuse whom.
Fascism, like National Socialism, was a right wing political movement trying to restore the best bits of what was believed to be the traditional order and to get rid of the liberalist republic which was – by the facists/ Nazis – believed to be just a stepping-stone towards (Jewish) communism. That Stalin and Hitler both ruled dictatorially and both drew part of the theoretic legitimization from answering the so-called social question, ie, deal with the issue of the impoverished proletariat, doesn’t mean they have anything else in common.
Soviet communism/ bolshevism was based on the idea of a dictatorship of the proletariat as new ruling class while physically eliminating most members of the old ruling classes, ie, the aristocracy and the bourgeoise.
The social concept of national socialism was to bring the proletariat back into the fold of the traditional, patriotic/ nationalist order by improving its material lot and giving its members more power to solve workplace disputes in cooperation with their employers instead of by killing all in some bloody revolution.
These are two very much different ideas. Plus, there’s defining characteristic of the real political right (as opposed to closet communist neoliberal …), namely, the belief that leaders are leaders by birth/ grace of God/ you-name-it and that the state should be organized accordingly vs the left idea that political power should ultimatively come from the consent of the governed and the state be organized as some sort of republic abstractly designed on a suitable theory of republican government.
Fascism, like National Socialism, was a right wing political movement trying to restore the best bits of what was believed to be the traditional order
This is not true. To be a conservative in the 1920s and 1930s was to support the monarchy, or the restoration of the monarchy, to support the strengthening of the social position of the aristocracy, and to support the social position of the Church. Neither Hitler or Mussolini supported this conservative position. They were both socialist revolutionaries. They were both leftwing.
If the nazis were left wing, why did they support Franco’s monarchist (and as you say, therefore conservative) Falangists in the Spanish Civil War, and not one of the myriad of left wing organisations (social democrats, socialists, communists, trotskyists, anarchists, syndicalists etc.), all of whom were vying for power? And why did Germany’s own aristocracy support the nazis?
Soviet communism/ bolshevism was based on the idea of a dictatorship of the proletariat as new ruling class.
This is not true. Soviet communism/Bolshevism was based on the dictatorship of a bourgeois political party that in point of fact brought the working class under the rigid micro-managed control of the bourgeois party. Lenin in particular was opposed to the working class if it exhibited ideas and behaviours that the bourgeois Left opposed.
I saw an observation earlier this year “we are in a magical world right now where everything is fascism except worshipping state authority and merging state and corporate power” which sums up our non-progressive progressives.
On a historical note, in the early 1930`s Trotsky recognised the danger of the Nazi Party in Germany and called for a United Front of Social Democrats and Communists to oppose them. Stalin declared the Social Democrats to be “Social Fascists” and no different to the Nazis. There is even evidence of Communists and Fascists joining together in thuggery to break up Social Democrat Party rallies and meetings.
For further reading on the subject read “What is Fascism and How to Fight it” by Leon Trotsky, still available I think.
Undeniably Trump is a ”fascist”. The evidence of this can be seen here;
Trump: “One of the most urgent tasks… is to decisively defeat the climate hysteria hoax.”
“The radical left’s fearmongering about climate and our future is… destroying America’s economy, weakening our society, and eviscerating our middle class. It’s really hurting us.”
“We have to defeat the climate hoaxsters once and for all.”
https://x.com/wideawake_media/status/1854482837350555810
And here. This is big. He’s also said elsewhere that he wants the death penalty brought in for immigrants who murder citizens or police officers, so yes, extreme fascism on display;
”Day 1.
An end to gender affirming “care” in minors.
Cry harder, libs. You can’t mut!late kids anymore.”
https://x.com/HazelAppleyard_/status/1854308510907138092
Facisism is a form of government and society which puts its race and society over and above any individuals. Communism is a form of government which puts it’s form of government over and above the individual. Both subvert the individual in different ways but expect the individual to serve the greater society, for the greater good. A proper government is a society which actively promotes individual freedom and responsibility, and so ultimately serves each individual of that society. As Thatcher said there is no such ‘primary’ thing as society and thats because it’s made of individuals with their individual hopes and dreams. Society can’t have hopes and dreams.
Mussolini’s Fascist manifesto was silent on race. Hitler is incorrectly labelled as Fascist, but he was not – he never was a member of the Fascist Party.
He was, as he frequently pointed out, a National Socialist. He was a racist.
This conflation of racism and Fascism is by lazy minded poorly informed people who do not know the definition of either.
Yes Mussolini only went after the Jews at a later stage to please the Nazis, who were cleaning up the metaphorical mess they made in North Africa. Also Oswald Mosley and his Blackshirts were not antisemitic, only after various attacks by Jewish groups on their venues etc, did they become antisemitic.
“No government has the right to decide on the truth of scientific principles, nor to prescribe in any way the character of the questions investigated. Neither may a government determine the aesthetic value of artistic creations, nor limit the forms of literacy or artistic expression. Nor should it pronounce on the validity of economic, historic, religious, or philosophical doctrines. Instead it has a duty to its citizens to maintain the freedom, to let those citizens contribute to the further adventure and the development of the human race.”
Richard Feynman
Fascism is indeed the name that Mussolini gave to his movement, his totalitarian socialist movement.
‘No individuals or groups (political parties, cultural associations, economic unions, social classes) outside the State. Fascism is therefore opposed to Socialism to which unity within the State (which amalgamates classes into a single economic and ethical reality) is unknown……But when brought within the orbit of the State, Fascism recognizes the real needs which gave rise to socialism and trade unionism’
Mussolini 1932
Fascism is, quite simply, Big State authoritarian socialism and it is to be found within every government currently in power in Western Europe (and the Russian ‘Union State’) and the U.S.
It is to be hoped that Mr Trump’s stellar performance may halt its long march….
You can put a cig paper between ‘Fascism’ and Communism.
Different points of emphasis.
Same result.
Difference between Catholic & Anglican – both in essence Christian.
Pretty simple really. Mussolini and Hitler were both Socialists. It’s of particular note that in 1945, to commemorate 25 years since the naming of the party, Hitler delivered a speech. In said speech he spoke about a world Socialist movement based on Socialist nations. He said that he may not see it in his lifetime but it would happen.
A few years back, when Corbyn was standing for Election, John McDonell spoke of his Socialist dream of a world Socialist Government. The two were eerily similar and, as I recall, the only difference was that McDonell didn’t mention nation states.
It is also interesting that no Socialist I ever met will accept that Hitler was a Socialist. They claim he was Far Right. Funnily enough, the term Far RIght was coined by British Socialists in the 1930’s to distance themselves from their German brethren.
Today, Far Right handily seems to encapsulate everyone the Socialist do not much like like Grannies who vote for Reform and non-white people who hold the most powerful positions in the nation.
Fascism is a branch from the same root as Socialism.
The latter exerts power and control over society and the economy by seizing direct ownership of private property “the means of production” and by all labour being employed by the State. This is centralised control.
Fascism (mostly) leaves property in private hands and employment by private enterprise, but all must operate as directed by the State in the interests of the State. This is dispersed control.
Both in practice amount to the same thing.
The Fascist model currently forms the basis of European economies – unsurprising given the popularity of Socialism and Fascism in Europe before and after the war, and the bureaucratic class running governments after the war were the same ones running governments before and during the war.
The outlier was the UK until it embroiled itself with the EEC/EU, and so far despite FDR, this fascistic model has made slow progress in the USA but a Democratic win would have established it firmly there.
Trump is the antithesis of Fascism – upper or lower case “f”.
We in the UK now have a fascistic government that Mussolini would envy… all we need is for it to be anti-Semitic and the chap with the little moustache would be pleased too… Oh!
It would be a mistake to take these lefties seriously. The problem is that if we do and try to analyze the fault in their thinking then to some extent we already accept their ideological framework.
I think back in the 1940’s George Orwell pointed out that fascism was even by then a completely meaningless word. It simply meant “any idea that deviates from our groupthink”.
You think biological sex is real – you are a fascist.
You think men and women should have separate toilets – you are a fascist.
You don’t think children should be chemically or surgically castrated – you are a fascist.
And so on, and so forth.
This is just it. The left cannot or will not acknowledge that their own model is fascistic. It bears striking similarities to Naziism in that it demands a cult-like obedience and adherence to the doctrines of state, with dissenters labelled, corralled and harrassed (for now). We are locking up dissenters on trumped-up (no pun intended) charges.
All political systems can benefit from introspection, but this is something the current power structure refuses to engage in. I have seen the many, many leftist reaction videos now doing the rounds on YouTube, and the overwhelming opinion amongst them seems to be that Kamala was rejected because she is a woman of colour, because society is of course, racist and misogynistic.
I feel quite safe in saying that the readers of this site (as a representative sample of the dissenters), could not care less about sex or race as markers of quality, but reject Kamala because she is a continuation of the status quo; which has arguably damaged society and personal freedom immensely.
She was rejected because people have simply had enough – not because of any of her innate human attributes.
”I feel quite safe in saying that the readers of this site….could not care less about sex or race as markers of quality..”
Need to take issue with this. Had you inserted ”majority” in there I’d have agreed with you but anyone who is a regular to this site will know that there’s certain men whose entire schtick is making disparaging, insulting posts about both the opposite sex and people of a different ethnicity, such is their obvious hardwired hostility towards females and non-whites. I could quite easily name names. People of colour cannot do right for doing wrong and will be forever judged first and foremost on their skin colour before they’ve even had a chance to prove themselves in any role, according to certain posters on here, and the exact same thing can be said for women. If a woman makes a pig’s ear of something it’s *because* of her sex that she’s deemed inept, therefore women should never be allowed to be in that job in the first place. But if a man is proven equally crap at his job, well, he’s just crap. Nothing to do with his sex at all. It doesn’t even get a mention. So there absolutely are bigots and misogynists on this site, and it’s remiss of you to not acknowledge this fact. However, I totally agree that the dreadful Kamala Harris was not out-voted due to her sex or ethnicity, she truly was inept irrespective of these two physical characteristics.
Which was the salient point I made.
But I do acknowledge your comment – thankfully such prejudice is very much the exception rather than the rule here.
This forum takes enough flack from the usual quarters without any of its users painting further targets on it.
Thank you for that, it needed saying.
👍 Well I can’t be the only one who’s noticed a certain pattern of unhealthy, abnormal behaviour whenever ‘the usual suspects’ get predictably triggered, either by an article or other posters’ comments.
The “real” left disowned The Guardian years ago.
Many people, including on here, mistake “liberals” with the left.
The only good leftist I can think of in your comment is people like Tony Benn.
The Brexit debate showed who on the left were “good leftists”.
Tony Benn, Bob Crow, Michael Foot, Peter Shore, Barbara Castle would have all voted for Brexit as did Dennis Skinner, George Galloway, Larry Elliot, Tariq Ali, UK communists and many of us on the left.
Those using the term that irk me the most are not those who do it cynically for gain – politicians, “academics” and “journalists”. It’s the bien-pensant useful idiot pseudo intelligentsia who piss me off most. It demonstrates a remarkable airheadedness and laziness of thinking, and an insult to anyone who has suffered under actual fascism.
Their desire is to remove the human will from the discourse altogether hence their fondness for the technocracy. It’s when you become so tormented with feelings of worthlessness and lassitude that any expression of the stronger aspects of the human life force become odious and threatening. So there is no point trying to educate such people because their ignorance has a spiritual rather than an intellectual basis,
If you want an understanding of twentieth century fascism then it is good to look at the Italian Futurist movement and its manifesto because it is a crystalization of this force that his hated and it was the most vital force in German fascism You can even find a breakdown on Wikipedia. You can’t understand the rejection of our current culture without being aware of this. It is an exposition of the failure of technology and a description of where its worship leads.
Trump is a very experienced alpha male businessman. He can cut up rough and quickly change to being polite and civil in a moment. He ‘would’ demand respect as his experience of life and business has given him a automatic grasp of outcomes others could spend years learning and more often never do, I think of Shakespeares Coriolanus, a much respected brave soldier who’s name alone would win a battle. Trump doesn’t need to consult his peers. Coriolanus, however was unfit, by personality, for civil office much preferring the excitement of battle. Trump’s battles were in a civilised society which he is accustomed to. Coriolanus was Shakespeare’s first play of his Roman trilogy that included Caesar and Anthony and Cleopatra. The late Professor Paul Cantor of Harvard and also Virgina wrote books and produced YouTube video lectures on the plays. The plays were about the fall of Empires,
Make no mistake, God sent President Trump and Harris is Satan’s acolyte.
“The gates of hell shall not prevail against it” is a Bible verse from Matthew 16:18, where Jesus promises that his church will never be destroyed and will survive until his return:
Brilliant. Can you write an essay on ‘transphobia’ too? It seems the trans cultists are calling everyone a transphobe.