
The prevailing narrative tells us that vaccinating the frail and elderly against Covid saved millions of lives and had a dramatic effect on mortality. How strong is the presumed effect of a Covid vaccine in that vulnerable population? Is it as strong as many believe, or perhaps much closer to zero than to the other end of the scale?
First, there is bad news to share, even before estimating any possible benefit.
Data from Denmark, Israel, and Sweden show increased risk of infection within one week or so after the first dose.
Possible mechanisms include transient immunosuppression (decreased lymphocyte count), conversion of asymptomatic infection to symptomatic infection and infection at vaccination stations. News outlets in Israel reported outbreaks of Covid infections in nursing homes shortly after the initiation of the vaccination campaign, and again after initiating the booster campaign (use Google Translate). Needless to say, when the risk of infection increases, the risk of death increases too.
Skipping the hazard period, studies of vaccine effectiveness (VE) reported a remarkable result that should have surprised knowledgeable readers. Estimates for the elderly have been extremely high, sometimes similar to those for younger age groups. For instance, a study in Israel of elderly residents of long-term care facilities reported VE of 85% against Covid death.
That is not only contrary to basic knowledge from immunology but is also incompatible with the following observation:
After the second vaccination [by the Pfizer vaccine] 31.3% of the elderly [over the age of 80] had no detectable neutralising antibodies in contrast to the younger group, in which only 2.2% had no detectable neutralising antibodies.
Consider three facts:
- Almost one-third of the elderly (over the age of 80) do not develop antibodies after vaccination against Covid
- Vaccine-induced immune response is known to attenuate with ageing
- Flu vaccines do not offer high protection in the elderly
How could Covid vaccines have been highly effective in the frail and elderly?
They were not. VE values that are much higher than 50% are a priori implausible. Anecdotally, that’s an estimate from a simple comparison of vaccinated and unvaccinated residents of nursing homes in Sweden. Likewise, the aforementioned study in Israel (overall VE of 85%) indeed noted that effectiveness decreased as age increased. VE by age group was not reported.
But even 50% might be overly optimistic.
Several sources of bias have affected observational studies of Covid vaccines. I will focus on one which I think ranks high on the list. Most important, it can be roughly accounted for.
A naïve comparison of vaccinated people with unvaccinated people is grossly misleading because of the ‘healthy vaccinee’ bias, demonstrated repeatedly and better explained in the reverse direction. People who are not vaccinated are, on average, less healthy than their vaccinated counterparts, and therefore have higher mortality in general. The mechanisms behind this phenomenon deserve a separate discussion, but it is well documented nonetheless. Previous research on flu vaccines has also shown that the bias is not easily removed by conventional statistical methods.
Which means that even if nursing home residents in Sweden, in Israel or elsewhere were unknowingly injected with placebo instead of a vaccine, Covid mortality would have been higher in non-injected residents. We would have computed biased (false) VE, attributed to placebo.
How strong is the bias? What is the typical ‘general mortality’ ratio, comparing unvaccinated to vaccinated in the population? If we know the ratio — the bias factor — we can replace biased estimates of VE with at least roughly corrected estimates. That’s better than no correction at all.
Fortunately, we have estimates of that ratio from studies that compared non-Covid mortality in the two groups. Since Covid vaccines are not expected to reduce non-Covid mortality, any ratio higher than 1 is an estimate of the bias factor. (To simplify, I ignore the influence of vaccine-related death on that ratio.)
Based on data from the U.S. and the U.K., the lower bound of the bias factor is about 1.5, and the likely value is somewhere between 2 and 3. In general, the mortality rate of unvaccinated is two to three times the mortality rate of vaccinated. Some variation by age and other factors is expected.
I show here one example from a large cohort study in the U.S. (where the unvaccinated group was ‘diluted’ by those who were vaccinated later).
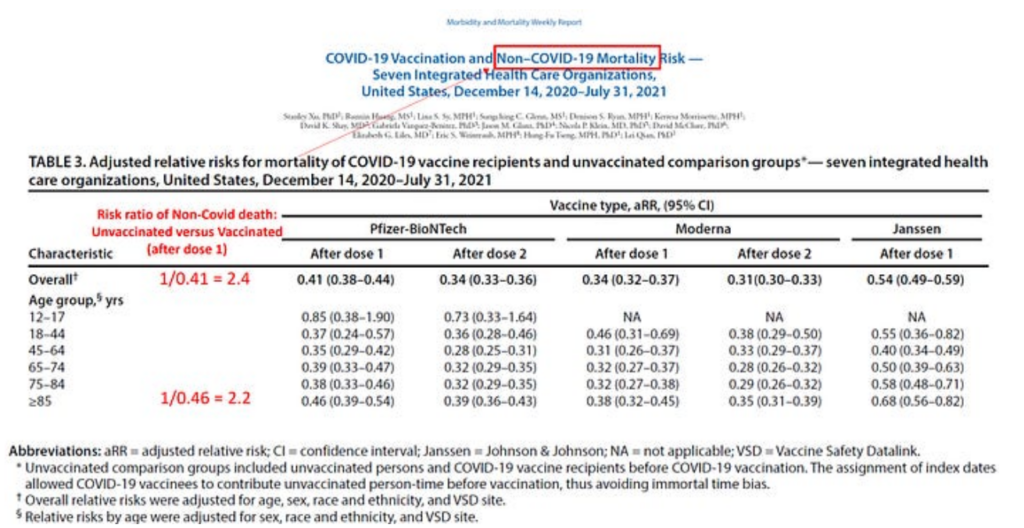
The relative risks (or risk ratios) of non-Covid death demonstrate the healthy vaccinee bias. They are all below 1, indicating that those who were vaccinated against Covid were less likely to die — from non-Covid causes! — than their unvaccinated counterparts. The inverse of these numbers is the bias factor, which ranges between 2 and 3, overall and in most age groups including the oldest (2.2).
Once the bias factor is estimated, say 2, correction of biased VE is simple.
Consider, for example, the aforementioned biased VE of about 50% from Sweden, which was based on a comparison of vaccinated and unvaccinated residents of nursing homes. VE of 50% is derived from a (biased) risk ratio of 0.5: vaccinated appear to be at half the risk of Covid death, or vice versa; unvaccinated appear to have twice the risk of Covid death (supposedly because they were not vaccinated). Since the latter have twice the risk of death to begin with, vaccination has made no difference. Multiplying the biased risk ratio (0.5) by the bias factor (2) restores the null effect (risk ratio = 1) and the correct VE (0%).
If the bias factor was only 1.5, that biased VE of 50% from Sweden will be corrected to 25%, much closer to futile than to a highly effective vaccine.
The correction method is approximate, and the healthy vaccinee bias is not the only culprit. What VE would we have observed had we been able to remove other biases as well?
We have to struggle with complicated biases in observational studies because we don’t have randomised trials with a mortality endpoint. And that is nothing short of scandalous. Let me end by explaining why it is scandalous and why there are no data.
When randomised trials were initiated, the pandemic might have been called ‘the nursing home pandemic’ because 30-60% of Covid deaths occurred among nursing home residents. Sweden was a prime example.
With that in mind, any first-year student in epidemiology will tell you that the first placebo-controlled randomised trial of a Covid vaccine should have been conducted in nursing homes, relying on ‘hard endpoints’ — hospitalisation and death. Not only should we establish benefits in the most afflicted population, but such a trial would have been statistically efficient, given the expected mortality rate. It would also have been highly feasible in terms of recruitment and follow-up. Having no meaningful mortality data from a randomised trial of a Covid vaccine is scandalous indeed. Who should be held accountable?
No such clinical trial was initiated because the big money was going to follow mass vaccination. Therefore, the pharmaceutical industry, with silent agreement of public health officials, focused on symptomatic infection as an endpoint — rather than death — in younger and healthier populations. Moreover, knowing the attenuated immune response in the elderly, they likely feared that studies of the mortality endpoint in nursing home residents would not deliver stellar results. And even if favourable, the results might not have sufficed for authorising mass vaccination.
To the list of public health misfeasance during the pandemic, we should add at least one nonfeasance: failure to demand randomised trials of vaccine effectiveness in nursing home residents. I suspect that if such trials were conducted early on, public demand for the vaccines would have been very different.
Dr. Eyal Shahar is Professor Emeritus of Public Health at the University of Arizona. This article first appeared on Medium.
Stop Press: Alex Berenson has highlighted the problem of healthy vaccinee bias in his latest post, focusing on a Hungarian study that once again found the unvaccinated population dying at about twice the background rate of the vaccinated population.












To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
Don’t know if I can get my head around this ”healthy vaccine effect” thingy. From the Berensen article;
”Considering how hard physicians and health bureaucracies have for decades pressed voluntary flu vaccinations for adults, it is no surprise that choosing to be vaccinated is strongly associated with more interest in healthcare and better overall health.”
Also taking into account what the author of the above article states; ”People who are not vaccinated are, on average, less healthy than their vaccinated counterparts, and therefore have higher mortality in general.” So are we really supposed to believe that, for instance, everyone that comments on this site who didn’t get the jab, we are of a lower socioeconomic status, have less access to good health care and are less health conscious than everyone who decided to get jabbed, in general? In my experience it is the people who eat crap, don’t exercise and smoke/drink who choose to be vaxxed because they think a magic jab will negate their poor lifestyle and diet choices. The same people who pop a multivitamin and pretend they’re healthy. So what the two authors are saying sounds illogical and back to front to me.
Am I misunderstanding something or are we all just anomalies on this site? lol
I must admit I did have a OFFS moment when reading this.
As an aside, I have just returned from taking the wife to the Doctors for a test that should have been done at the beginning of the panpanic but was cancelled. Only to find that the Doctors can no longer do the test because the test machine has been returned to the health board from lack of use. Not surprisingly, not only did the surgery actually contact my wife to make the appointment with the non existing machine, it was with a nurse who wasn’t trained to use it if it was available.
Post “pandemic” nothing has got better. Friend of ours was diagnosed with Prostate cancer last September.
Three weeks ago he had his FIRST treatment.
EIGHT months.
yes the highest % of people i found who knew better than to get the clot shot were the ones buying organic raw milk cheese and meat from the local organic farmer ,
while the ones who eat GMOS with out a care were the ones who wanted people like us excluded from schools restaurants and probably wanted us locked up
Yup. My wife and I. Both carnivores, our main foodstuff grass fed beef, from a local butcher and a farm shop (raw milk – I make it into Kefir) where we know the farmer.
Food waste? Tiny
Food miles? Tiny. Only food we buy from a shop is tea and coffee.
What is the definition here of healthy and unhealthy? We might look at someone and decide, based on their appearance and eating habits, that he is unhealthy, but is that what the “healthy vaccinee bias” in this article referring to? What percentage of a country’s population is considered unhealthy?
Stabs had negative efficacy. Post every stabbination death rates went up. We have record excess deaths in 2022-23. Millions were/are injured. The overall death rate in 2020-21 was the historical average, ergo no pandemic but a scamdemic.
Why does anyone thinnk putting chemicals into the deltoid and your bloodstream fights a ‘virus’ and a respiratory ailment in your chest area. FFS. People really are stupid and will write stupid analysis proposing some quack-effectiveness. The sun shining and vitamin D had a more positive effect than the quackcines.
I think it’s that, pre-COVID-19, people who had their shots were health conscious. I’ve had my polio, TB, tetanus vaxes down the years and I had actual illnesses mumps, measles and rubella (rubella in my mid teens really knocked me for six!) I had a flu shot twice when I lived in London in the mid-2010s, but became ill after the second one and was tired all the time for a couple of years. I’ve never had a jab since. No regrets at not taking the COVID-19 jabs. I was sceptical about them in the first place and I’m glad I held off. My poor Mum, who was vaccine injured, is having a pacemaker-defibrillator fitted: her vaccine-damaged heart function is now down to 52 per cent. The damage was only picked up because she was under observation for sarcoidosis on the lung.
Mogs, I got as far as you in reading this article and unless it can be explained in a better manner I would conclude it is total Boll Ox
 .
.
For all the differences on DS I do not accept that we are a bunch of perpetual Maccie D scoffers, in fact just the contrary. I gave up on this because it is simply arse about tit.
Hard to say for me personally as I know vanishingly few unvaxxed people so my sample size is tiny, but as a group they are probably MORE health conscious and healthy than the average. But there may be lots of unvaxxed people out there who are indeed less healthy – I think there are stats showing that unvaxxed have a higher % of “deprived” groups e.g. the poor, various ethnic minorities, and these people may well be less healthy on average – but I simply don’t personally know anyone in any of those groups.
I suspect there are two groups who declined the jabs.
Those, like me, who look after their own health and who are also sufficiently interested/intelligent to do their own research rather than believe the Government or just “trust an expert.”
Those who ARE less healthy and who either don’t speak English so were unaware of the propaganda, or who pay no attention whatsoever to “events” so were completely oblivious to the propaganda.
The only real question now is how were people so foolish, so easily lied to, so eager to go along with patent nonsense from the start? Why did no many ‘experts’ refuse to go with what must have been their own prior, contrary knowledge?
The fact that the vaxx increased infections was clear from the very start – graphs for the UK and Israel, two countries that started poking full guns blazing, showed a steep increase in infections that coincided with the start of the stabbing; one’s own eyes and common sense showed there had to be a link. Comment sections in newspapers were rife with people saying how unfortunate that they happened to catch the lurgy just in that two week interval – after evading it for a year. Viruses rise and fall, that a steep rise should be followed by a sharp decline is logical – so, probably zero to do with the vaxx, just smoke and mirrors. I remember feeling at the time that I was living in some parallel universe where to me it looked as if the vaxx was actually causing people to catch corona, while everyone else was saying that catching corona after being vaxxed didn’t mean it was not effective, it was just bad luck – just as they were saying ending up in hospital after the vaxx meant it was safe, as it had saved them from corona (but not from the ICU).
I remember reading reports in spring 2021 about an added dose of poison being given to the elderly (in Israel I believe) and that this increased the antibodies – the headline looked great, but upon further reading it only increased antibodies from a very low level to a somewhat less low level, but still nothing spectacular. So it was known early on that the people who needed the vaxx the most, were unlikely to get any real benefit from it.My mum got the BCG vaxx in spring 2021, and was told it wasn’t offered to people over 80 as their immune systems didn’t produce sufficient response. I can only assume that applies to all people over 80 for all vaxxes. So again, those in the know must have suspected if not outright known that all the claims were overblown puff and could not possibly be true, unless pfisser’s poison managed to redesign the human immune system (well, it may well have done, but I suspect that will manifest itself over the longer term, not in a matter of weeks).
The failure of the vaxx was there to see from the start, but people chose to listen to a disingenous message repeated over and over rather than believe what they could see and feel for themselves. The bigger the lie…
Fairly soon after the jabs were being rolled out globally, someone posted a series of graphs on YouTube showing that in EVERY country where the programme had started, there was an immediate and very steep rise in deaths. From memory, I recall that Gibraltar was particularly interesting since they had recorded no (or possibly one) Covid deaths before the jabs started but there was an immediate and steep rise immediately afterwards.
Unfortunately I no longer have the graphs since I stored them on my old computer, which gave up the ghost a year ago.
However, the data on the jabs leading to increased deaths everywhere they were rolled out must have been known by the global authorities.
There was a strong degree of opportunism in the trade, which undermined the more established protocols for developing anything novel. That said, I’m not sure that it was only the unwell who decided not to use the product on offer. Some of us who are actually quite fit and healthy might have taken the opposite view, having taken wise advice from various sources, and decided not to take a risk of using anything like that. Especially so on the grounds that it was being sold aggressively by the usual suspects.
The problem with the ‘healthy vaccinee effect’ is that there is no agreement about which direction it works in.
When Professor Fenton wrote to the Office for Statistics Regulation pointing out that ONS data showed bizarre spikes in unvaccinated non-Covid mortality at each successive peak of vaccination for each successive age group – when there should be no connection whatsoever – the regulator replied:
“In your paper you also state that the number of deaths reported within the first 21 days of receiving the first dose of the Covid-19 vaccination is below that which could be expected in the general population, and that this difference is evidence of systematic undercounting of deaths by ONS. Our view of this question starts with the consideration that the population included is not representative of the general population, and it is therefore likely that any pattern you observe is attributable to the ‘healthy vaccinee’ effect. This happens when people who are ill (either due to COVID-19 or another relevant illness) are likely to delay vaccination. The result of this effect is a lower-than-average mortality rate within the first 21 days of receiving a vaccination. This effect is described by ONS in their Deaths by Vaccination Status publication.”
https://osr.statisticsauthority.gov.uk/correspondence/ed-humpherson-to-norman-fenton-martin-neil-clare-craig-and-scott-mclachlan-ons-deaths-by-vaccination-status-statistics/
But if that’s the view of the ONS, as well as the Office for Statistics Regulation, the ONS simultaneously has a contradictory view:
“the vaccination roll-out was also prioritised by health status of individuals, with the extremely clinically vulnerable and those with underlying health conditions being vaccinated earlier than other people in their age group”
Section 2: Methods:
https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/bulletins/deathsinvolvingcovid19byvaccinationstatusengland/deathsoccurringbetween1januaryand31october2021#:~:text=However%2C%20the%20vaccination%20roll%2Dout,people%20in%20their%20age%20group.
So which is it? Can they make up their minds?
I keep coming back to this thought: if there was a deadly once in a century pandemic that warranted unprecedented measures, followed by a miracle safe and effective vaccine that it was imperative to take in order to save us from carnage or endless lockdowns, it ought to be easy to see all the millions of lives “saved”. But it isn’t. Mortality continues to be higher than before in many rich world countries. Occam’s razor suggests that either the vaccines are killing people or they are useless and Covid is killing them.
Covid jab made death more likely
Stand in the Park Make friends & keep sane
Sundays 10.30am to 11.30am
Elms Field
near play area
Very interesting article.
I believe there was collusion between the Pharmaceutical Companies, the American Security Services who were funding the Gain of Function experiments, and the so-called Regulators (which are largely funded by Big Pharma) to ensure that the experimental mRNA jabs were tested on as close to the entire population as they could get.
Big Pharma would make £billions.
The American Security Services would get the data they wanted – and the mRNA technology as a platform technology for future use.
The Senior Regulators would get to keep their jobs and transfer smoothly into Big Pharma providing they complied with the programme and authorised the experimental product for the entire population, including children.
They have killed tens, if not hundreds of thousands, and injured millions.
In a just world, they would all be hauled in front of a Nuremberg-style court.
These injections were not “vaccines”.