“Many Covid deaths were ‘with Covid’, Covid mortality attenuated, and there was no substantial excess mortality, anyway, in the winter of 2021-2022.”
That’s the message of an article published by a research group from Denmark. Some of the authors are affiliated with Statens Serum Institut in Copenhagen, which is under the auspices of the Danish Ministry of Health.
I have reached the opposite conclusion: regardless of misattributed deaths, there was a major, prolonged Covid mortality wave and shocking excess mortality in a highly vaccinated country.
One of the two views must be wrong.
Let’s take a close look at that paper from Denmark. (Excerpts are formatted as quotations throughout; anything in red is my addition.)
During the last quarter of 2021, excess all-cause mortality in Denmark was at a stable low-to-moderate level, however with a brief peak of some substantial excess mortality in December 2021, before restrictions against COVID-19 were lifted (Figure 4).
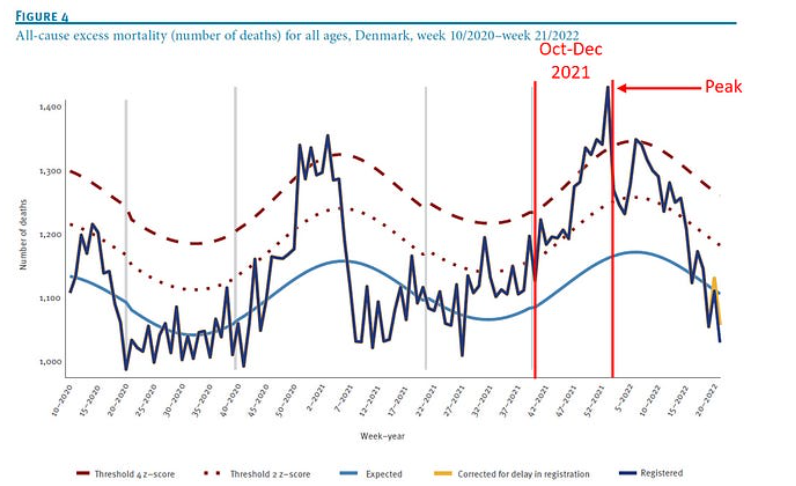
Indeed, there was one week (“a brief peak”) of substantial excess mortality, but that’s not the key point. In all other weeks of the last quarter of 2021, excess mortality ranged between 2 to 4 Z-scores above the expected level (blue line) — far from a minor deviation.
Later in the article, that “low-to-moderate level” during the last quarter of 2021 has changed to “the low excess mortality seen since late 2021”. What corresponded to low in the authors’ minds is unclear. Surprisingly, they did not quantify excess mortality in percentages, a common practice for the pandemic.
Avoiding any modelling, I simply compared the number of deaths in each month of the last quarter of 2021 with the corresponding month of every year between 2007 and 2019 and computed the excess (%).

We observe at least 10% excess mortality, and around 15% or higher in many comparisons. For a typical month in Denmark, with 4,000-5,000 expected deaths, that’s hundreds of deaths above ‘normal’. Was that considered low by the authors?
They continue:
In the beginning of 2022, excess mortality fluctuated within the range of moderate excess mortality with an overall downward trend, reaching a normal level from week 13 of 2022.
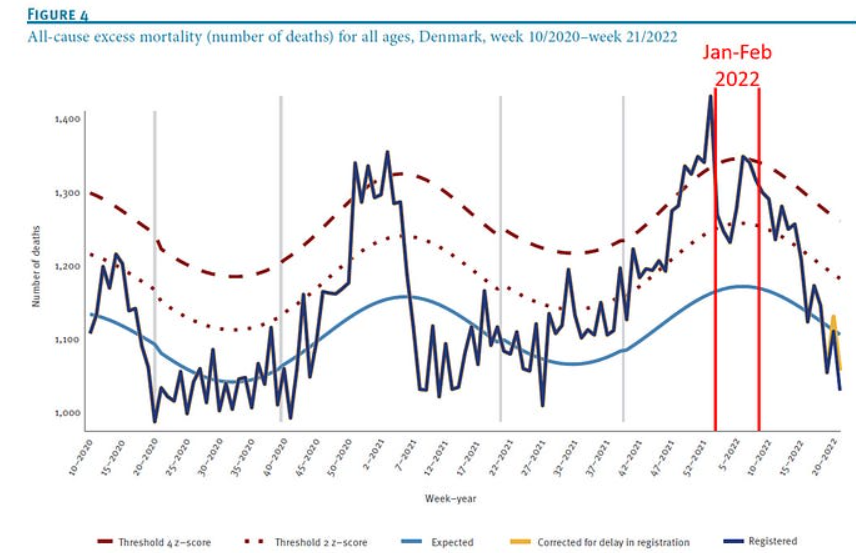
Excess mortality was lower at the beginning of 2022, but it was at least 5% in most comparisons with previous years, as shown below. (The comparisons with February and March 2018 are compromised due to a severe flu wave back then. See figure here.)

There is some element of subjectivity when quantities are described qualitatively. Consistent writing is expected, however. If the excess mortality at the beginning of 2022 is called moderate by the authors, how come higher excess mortality, in the last quarter of 2021, is called low-to-moderate or low?
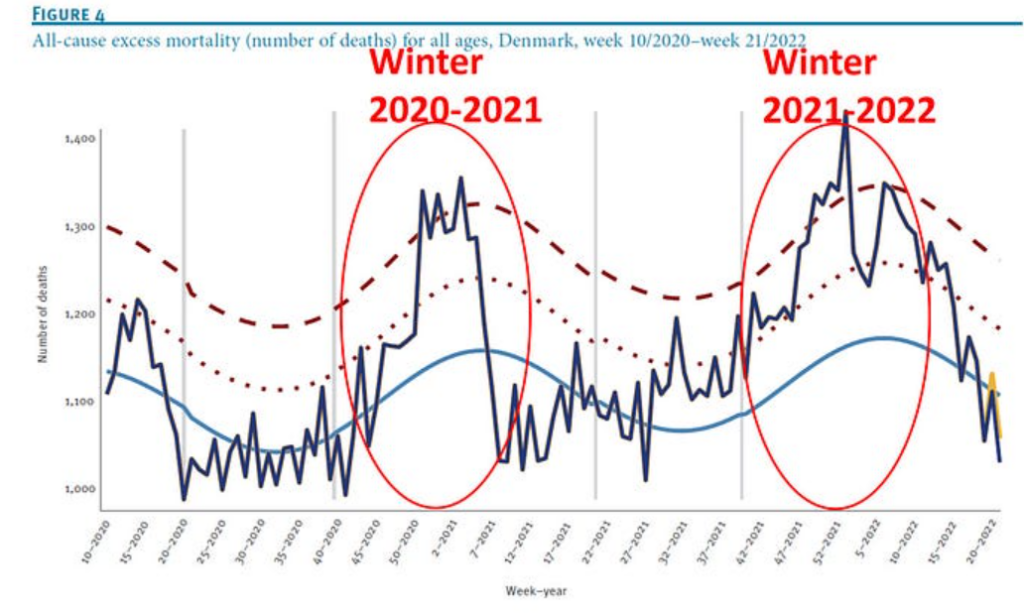
Compare, next, the distance between actual mortality (irregular line) and expected mortality (smooth blue line) within the equal-size, red ellipses. You don’t need to be a statistician to conclude that excess mortality in the winter of 2021-22 was substantially higher than in the previous winter, despite a high rate of vaccination against Covid (over 70% of the population was fully vaccinated by September 2021).
Assuming the Danish researchers accept, say, 5-10% excess mortality (a highly conservative range) in that six-month period, they need to suggest the presumed cause(s). Here is what they write:
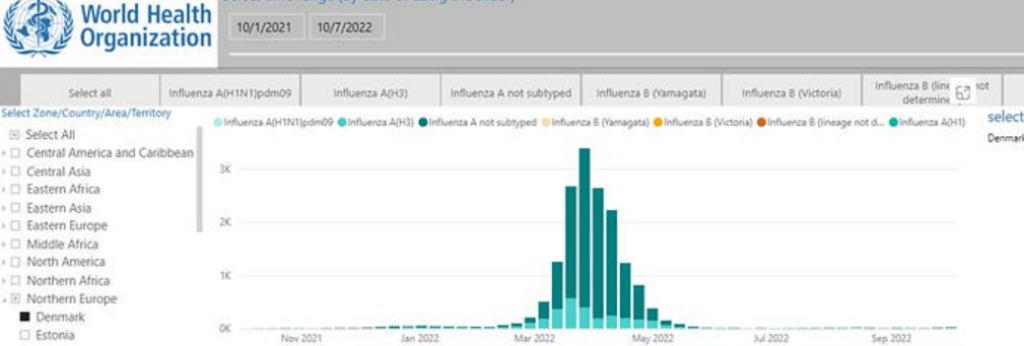
However, it is challenging to infer the cause of any excess mortality in the presence of more than one major public health event, such as in the case of COVID-19 illness and deaths coinciding with seasonal influenza epidemics, which we saw in Denmark in March 2022, with both infections especially affecting the elderly population.
Indeed, flu returned only in March 2022 (figure below), so it is irrelevant to most of the period in question. It cannot account for excess mortality any time earlier. Which other major public health event was there in Denmark during the winter of 2021–2022 besides a major Covid wave? The authors offer no explicit answer.
Much of the article is concerned with misclassification of deaths, specifically death with Covid as opposed to death from Covid.
That deaths have been misattributed to Covid throughout the pandemic is unquestionable. We can show a lower bound of the frequency whenever the number of reported Covid deaths substantially exceeds the estimate of excess deaths. But even then, and certainly at other times, the frequency of misattributed deaths remains uncertain.
When the prevalence of an infection increases, the probability of incidental infection — death with Covid — also increases. That’s the key point of the article.
They write: “We have presented a method for adjusting COVID-19 deaths for coincidental deaths…”
Then they qualify: “However, it is important to note that even coincidental infections may have contributed to hastening the death in some cases.”
The distinction is not always simple, indeed.
But they missed another key point. The rate of misclassification is determined not only by the changing prevalence of an infection but also by the changing mindset of a physician during the pandemic. For instance, if physicians think that a Covid vaccine is highly effective, they would be inclined to attribute a possible Covid death of a vaccinated patient to something else. That speculation may be supported by U.S. data, where the share of excess deaths above the tally of Covid deaths surprisingly increased during the Delta wave. Perhaps at that time, deaths from Covid of vaccinated patients have been attributed to other causes (because the vaccines were promised to be 95% effective).
Reality might even be more complicated. During a rising wave, as physicians confront more Covid deaths — in a highly vaccinated population — that kind of misclassification bias might gradually diminish, distorting the shape and location of the Covid mortality wave.
In short, inference on misclassification of Covid deaths from trends in the prevalence alone is insufficient, and trends in the mindset of physicians during a pandemic are insufficiently understood.
It is interesting to note that Covid vaccines are mentioned only once in the article, and rather casually. The authors are convinced that the vaccines, developed against the original strain, are effective against Omicron.
With the higher incidence of infection and a generally more benign illness caused by the Omicron variant in a national context of high booster vaccination uptake, as is the case in Denmark, a larger fraction of deaths will wrongly be classified as COVID-19 deaths, leading to an overestimation of the COVID-19 mortality burden.
Omicron accounted for three major mortality waves in Japan, a highly vaccinated country, resulting in substantial excess mortality before the return of the flu.
So let me repeat my previous conclusion: “Whatever the exact share of Covid deaths was, it is impossible to reconcile a highly effective vaccine with the excess mortality in Denmark in the past flu-year.”
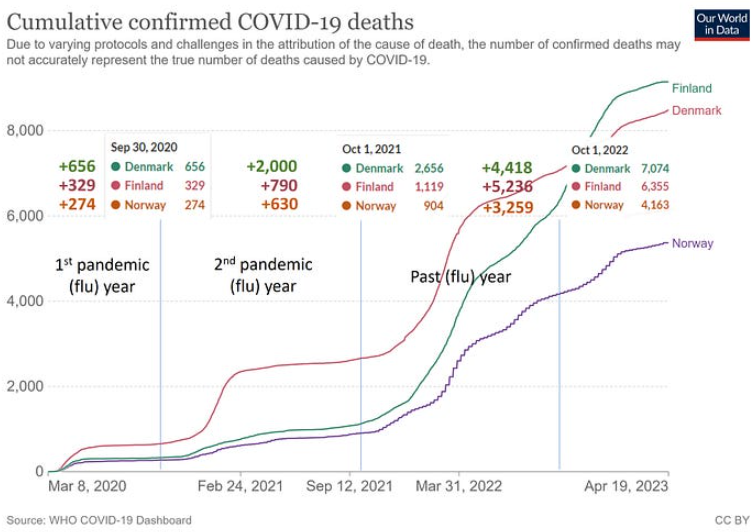
Between October 2021 and September 2022, the past flu-year, all-cause mortality in Denmark exceeded the expectation by about 10%. Even if Covid deaths accounted for only 7% excess mortality, that’s about twice the excess in the previous 12-month period.
There is no alternative view of the facts. Despite mass vaccination, Covid mortality markedly increased during widespread Omicron transmission in Denmark and in two of its Nordic neighbours.
Dr. Eyal Shahar is Professor Emeritus of Public Health at the University of Arizona. This article first appeared on Medium.












To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.
Yep. He thinks the grown ups are back in charge and we are all children who need to be told what to do by the grown ups who are the ones that know best. That pretty much nails it.
And my hunch is that most of the population agrees.
86% of those who voted supported parties who either explicitly or implicitly stood for enlarging the role of the state or at least keeping it the same.
Even people on the political right are happy enough with people being told what to do as long as it’s stuff they agree with
It’s a stupid idea and is based on the ideology of hate that pervades Labour. It doesn’t make any sense and it will cost more to the State than it ever brings in. How are schools supposed to cope with tens of thousands of new children in the middle of the academic year? The Brain Dead voted in The Seriously Brain Dead.
It’s not about sense – it’s about punishing people for their ideology
Their hate goes back a long way.
I remember the hate of non-state run schools from Labour, around the mid-1960s. I remember it well because I couldn’t understand how passing a school entrance exam was such good news, yet the school I was in was beyond evil, according to nearly half the country, and nearly all of the Media.
My Dad said that, as well as the Secondary Modern and Grammar Schools there should have been technical schools, but it hadn’t happened, which did imply that Politics wasn’t full of grownups, even then! See Tripartite System heading, here:
https://en.m.wikipedia.org/wiki/Secondary_modern_school
I expect one group didn’t want to damage the exclusivity of the academics, and the other wanted to destroy any streaming by ability.
And, after 60 years, we have the very same problem at polytechnic/university level, if we can admit there is a problem.
The state should get out of education completely.
The state should also get out of the business of nudging behaviour through taxation, whether that is a sugar tax or tax on alcohol or tobacco.
Notice the government want to teach children how to spot “Fake News” and “Misinformation” while at the same time trying to force the end of private education. That will allow them to have all the children in State Schools where they can be freely indoctrinated.
This policy of the government isn’t just about envy of independent schools. It’s designed above all to strike at independent-of-the-state parents. This is because the marxo-fascist madleft, the advocates of the total-control state, believe that the state should own and control children, not parents. They intend to turn parents into the agents of the state inside the family. Thus, this policy is the beginning of the marxo-fascist war on independent parents, and everyone in our society still able to exercise what remains of our freedoms.
I’m sure the timing of the introduction of the tax in the academic mid-year is deliberate.
Parents will be more reluctant to make their kids change schools mid-year.
If families find they can just about cope with the additional costs during the winter-summer terms the government hopes more will dig that bit deeper and so continue to contribute to the fantasy £
1.71.5bn (and falling) tax takeBy creating the additional obstacle of changing schools mid-year the government hopes to phase in the increase in demand for state school places over a longer period.
Also holding out the possibility of punishing families (which can’t or won’t pay increased fees) for taking the kids away from independent school with no state school place allocated the government again hopes to manage the increase in demand.
In Bristol there at least 5000 children in Private schools. If they all went to the state system it would instantly collapse. It is already almost dead, with poor results. How would he fix this? I suppose a wave of a wand would build 3 new schools in 6 weeks! Dream on…
I find it difficult to understand why one man is being allowed to destroy an entire country? How is this possible in this day and age in a “democracy”?