
On many issues – lockdowns, Net Zero, free speech, wokery, to name a few – the Daily Sceptic and Spiked are usually on the same page. Links to its articles frequently appear in our bulletins. However, one area where, since early 2021, we have diverged sharply is on Covid vaccines. At TDS we have maintained a sceptical guard against the often overhyped claims of safety and efficacy put out by Government and other sources. Articles questioning them – often by experts in the field – have become part of our standard fare. Spiked, on the other hand, has stuck firmly to its pro-vaccine position. Not a single article questioning the Government line on vaccine safety and efficacy has ever, to my knowledge, graced its pages – though despite this, to its credit, it has (mostly) maintained a firm line against vaccine coercion.
Rarely has this difference been so apparent as in a piece this week by Deputy Editor Fraser Myers that can only be described as a brutal polemic against Andrew Bridgen, the U.K. Member of Parliament who has been vocal in his criticism of the Covid vaccines and was last month kicked out of the Conservative Party.
The article, titled ‘The delusions of Andrew Bridgen‘ and setting the dismissive tone with its opening line, “It can be tempting to ignore the antivax conspiracy theorists”, contains many errors of fact, as well as misrepresentations. Many readers, I imagine, will be left wondering why a website that they read for viewpoints not found in the mainstream seems unwilling to countenance the possibility that the Government’s line on the vaccines might – just might – be skewed by the vested interest it has in claiming the vaccine rollout as a big success, or that all the independent experts who have stuck their heads above the parapet to urge caution might – just might – be saying something worth listening to.
Well, be that as it may, what we have instead is Myers’ attack on one of the few MPs raising these issues that are clearly of some concern to a number of his constituents and the medical experts he’s in contact with. Perhaps it would have been better if Myers had ignored him. But seeing as he didn’t, and in the spirit of rational debate rather than name-calling, I will endeavour to respond to Myers’s characterisation of him as an “antivax conspiracy theorist”.
One of the difficulties in responding, though, is that not all of Myers’s claims are backed up with sources or evidence. This makes it hard to know what he’s basing his statements on, or even at times what he’s referring to. For instance, he mentions a “now-infamous Westminster Hall debate last December” in which Bridgen “reeled off a list of academic papers, citations and statistics, all purporting to show that the vaccines are doing more harm than good (much of it based on misinterpretations or perhaps misrepresentations of the data)”.
But there was no Westminster Hall debate on vaccines in December 2022 (though there had been several in previous months). Rather, on December 13th there was a House of Commons debate on vaccine harms, led by Andrew Bridgen, and presumably it is this that Myers is referring to. Exactly why he deems this debate to be “now-infamous” is unclear, as is why he describes Bridgen’s citations as being “based on misinterpretations or perhaps misrepresentations of the data”.
Myers clearly regards Bridgen’s claim that the mRNA vaccines may be doing more harm than good to be nonsense, but in fact it is well-supported by evidence. For instance, British Medical Journal Editor Dr. Peter Doshi along with Dr. Joseph Fraiman and colleagues examined the data from the vaccine clinical trials and found that, compared to controls, the Pfizer and Moderna mRNA COVID-19 vaccines were associated with an increased risk of serious adverse events of 10.1 events per 10,000 vaccinated for Pfizer and 15.1 events per 10,000 vaccinated for Moderna. When combined, the mRNA vaccines were associated with an increased risk of serious adverse events of 12.5 per 10,000 vaccinated, or 1 in 800. The authors note that these adverse event rates were considerably higher than the observed reductions in COVID-19-related hospitalisation rates, meaning the findings imply that among trial participants the vaccines were doing more harm than good.
Similarly, Dr. Kevin Bardosh and colleagues – hailing from the Universities of Harvard, Oxford, Johns Hopkins, Edinburgh and Washington, among others – found that for every COVID-19 hospitalisation prevented by boosters in previously uninfected young adults, 18 to 98 serious adverse events occurred, including 1.5 to 4.6 cases of booster-associated myocarditis in males. That’s more harm than good, at least for healthy young adults.
Does Myers deem Bridgen to be misinterpreting or misrepresenting these studies, or does he think these studies are themselves misinterpreting or misrepresenting the data? He doesn’t tell us.
Myers’s next objection is to Bridgen calling the vaccines “experimental gene therapy”. He writes:
Bridgen refers to the Pfizer-BioNTech mRNA jab as “experimental gene therapy”. This technology is certainly novel. Rather than using a neutralised version of an infection or a close cousin, the mRNA vaccines deliver instructions to human cells which induce an immune response. The successful deployment of mRNA in the Pfizer and Moderna Covid vaccines marked a major scientific breakthrough. But these vaccines are not ‘experimental’, as they have gone through clinical trials. Nor are they ‘gene therapy’, as they make no changes whatsoever to a patient’s DNA.
What Myers is overlooking here is that while the vaccines were approved for use under an emergency provision, the Phase 3 trials were still some years from completion. An open letter from more than 60 doctors and scientists to the MHRA in May 2021 spelled this out. They wrote:
All Phase 3 COVID-19 vaccine trials are ongoing and not due to conclude until late 2022/early 2023. The vaccines are, therefore, currently experimental with only limited short-term and no long-term adult safety data available. (emphasis added)
It is also of significance that the products were tested only under the less-stringent safety protocols for vaccines, not under the more-stringent requirements for novel genetic products, as the HART group explained in October 2022:
The U.K. drug regulator, the MHRA, did not carry out the toxicity, biodistribution and pharmacokinetics studies that are required of new drugs because of the political pressure to approve. However, nearly two years have passed since then and the MHRA has not set a deadline for the pharmaceutical companies to provide these data. The MHRA allowed the treatments to be presented as vaccines like any other when they are a novel class of agents, never before approved for human use despite the technology being around for decades (mostly because they have been dangerous and ineffective in previous human trials).
Myers’s claim that the vaccines are not ‘gene therapy’ because “they make no changes whatsoever to a patient’s DNA” misses the fact that from a regulatory point of view gene therapy products include not only those which alter DNA but also those which “alter the biological properties of living cells“.
This is why Moderna’s November 2018 Securities and Exchange Commission (SEC) registration statement says that its “mRNA [technology] is considered a gene therapy product by the FDA”.
Likewise, the September 2019 BioNTech SEC Registration notes that “[In] the United States, and in the European Union, mRNA therapies have been classified as gene therapy medicinal products”.
Myers is wrong: mRNA vaccines are classed as gene therapy products.
A particularly odd point in Myers’s article is when he says that Bridgen is “inconsistent” because he claims not to be opposed to vaccines in general, “only the ‘experimental gene therapy’ mRNA variety”. Myers notes that Bridgen regrets taking two doses of the AstraZeneca jab, which he points out “is not an mRNA vaccine (it uses a chimpanzee adenovirus to induce immunity to Covid)”. He adds: “When a BBC employee reportedly died following complications from the AstraZeneca vaccine, Bridgen blamed it on ‘experimental treatments‘.”
Leaving aside the reference to the BBC employee (presumably Lisa Shaw) “reportedly” dying from the AstraZeneca vaccine (Shaw’s death wasn’t merely “reported” as such, it was found by the coroner to be so), Myers here appears to be oblivious to the fact that the adenovirus vector vaccines also involve using genetic material (in their case DNA) to ‘reprogramme’ cells to make SARS-CoV-2 spike protein. His description implies that the chimpanzee adenovirus induces immunity to Covid directly. But in fact the adenovirus is just a vector or carrier, like a box, into which has been inserted the DNA encoding for the spike protein. The adenovirus vector is the vaccine’s way of getting the genetic code into the cells. This is no less “altering the biological properties of living cells” and thus a gene therapy product than the mRNA vaccines, and Bridgen is right to place them under the same umbrella.
Lastly, Myers gets onto the frequency of vaccine injuries. “Potential” vaccine harms like myocarditis and blood-clotting are “incredibly rare”, he says, quoting ONS data showing that by December 2022 “just 47 deaths in England and Wales where the underlying cause was a Covid vaccine” were recorded. Gotcha! Except, of course, in the censorious climate that prevailed during the pandemic doctors registering deaths would be very reluctant to identify a vaccine as the underlying cause of death without some strong grounds for certainty such as an autopsy. Much safer just to write the condition that was responsible for the death, rather than speculating on the role of the vaccine in inducing it. A more realistic estimate of reported vaccine deaths comes from the MHRA’s Yellow Card adverse event reporting scheme, which has logged around 2,500 U.K. deaths. These are all deaths which those who filed the report (mostly medics and healthcare practitioners) suspect were due to the vaccine that the deceased had recently received.
Myers has a few words to say about the Yellow Card scheme. He accepts that by November 2022 “the MHRA had received and analysed nearly 178,000 such cards for the Pfizer vaccines, 247,000 for the AstraZeneca jab and 47,000 linked to Moderna”. But while these “may sound like large numbers”, he says, “we shouldn’t forget the size of the vaccinated cohort – the U.K. has handed out more than 151 million doses of vaccine and has double-vaccinated almost nine in 10 residents”. Let’s leave aside whether 90% of the population has really been vaccinated (more realistic estimates from polls and the NIMS database suggest it’s more like 75% of adults who’ve had at least one dose). The key point is that Myers doesn’t offer any comparison data to tell us whether 472,000 Yellow Cards for 151 million doses is high or low, worrying or normal. Similar figures for the U.S. indicate that the reported vaccine fatality rate is still over 20 times higher for Covid vaccines than it is for flu vaccines, even taking into account the total number of doses distributed. The same data also indicate there has not been any great degree of over-reporting during the pandemic as there was no increase in death reports linked to other (non-Covid) vaccines. In the U.K., the reporting rate for non-COVID-19 Yellow Cards actually fell by 16% from 2020 to 2021.
Myers states that “the overwhelming majority of these reports relate to reactions at the injection site or include things like sore arms, dizziness, nausea, headaches and fatigues”. This is true, and I don’t believe anyone claims otherwise, although Myers writes that “for Bridgen every Yellow Card is to be taken as evidence of serious vaccine injury”, though, again, no source is provided for this. He then quotes Bridgen saying that Yellow Card reporting represents “only 10% of the true rate of serious adverse events”, which seems to contradict his claim as Bridgen refers here to serious adverse events, suggesting he is distinguishing serious and non-serious events and not, as Myers implies, conflating them.
Myers does not dispute the claim about 90% under-reporting, which may be because it is on the MHRA website. It states: “It is estimated that only 10% of serious reactions and between 2-4% of non-serious reactions are reported.” However, it’s worth noting that MHRA has argued that this 10% estimate doesn’t apply to the Covid vaccines owing to the increased awareness of the scheme, though we have seen that that is not borne out in the reporting rate for other vaccines.
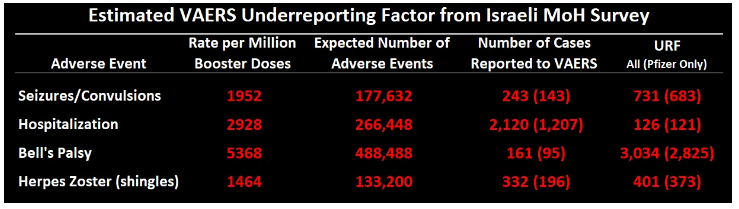
But we don’t really need to guess about this stuff as many governments carry out active monitoring via surveys of vaccinated people. The Israeli Government’s survey, for instance, found that 0.3% of vaccinated people (1 in 333) reported being hospitalised as a result of their first Covid booster, while a U.S. CDC survey found 0.9% of vaccinated people (1 in 111) reported seeking medical care as a result of their vaccination. A vaccine monitoring app in Germany found that 0.3% of vaccine recipients reported at least one serious adverse reaction to the first dose of the vaccine. The MHRA has never published the U.K. version of these data. A comparison of the Israeli active monitoring rate (from the survey) to the passive monitoring rate (from VAERS) showed that the true number of people hospitalised following their vaccination was 126 times higher than the number who reported it to VAERS, i.e., less than 1% of those who according to the survey were hospitalised following their vaccine reported it to VAERS. Other under-reporting rates in the Israeli survey (see examples in table below) were even higher, making Bridgen’s (and the MHRA’s) 10% estimate look very conservative. Note that these figures don’t have a control group for comparison to allow for incidental events.
If 0.3% of people who receive each dose of a Covid vaccine are hospitalised with a serious adverse reaction, as per the Government surveys, then after 151 million doses there would be around 450,000 hospitalisations following vaccination. It really is that many, because 0.3% of 151 million is still a big number.
Myers concludes: “[Anti-vax] conspiracy theories corrode reason, democracy and humanism. We cannot allow them to fester unchallenged.”
I think it’s fair to say, if Myers is worried about the corrosion of reason, he needs to start somewhere closer to home.












To join in with the discussion please make a donation to The Daily Sceptic.
Profanity and abuse will be removed and may lead to a permanent ban.